
Abstract
Objective
Faith leaders often serve as health-related role models yet many struggle with obesity and self-care engagement. The purpose of this scoping review was to examine how the faith leader literature has defined self-care and examined obesity and obesity-related chronic disease.
Data Source
Studies were identified through database (eg, PubMed, CINAHL, PsycINFO), backward, and grey literature (eg, dissertations) searches.
Inclusion/Exclusion Criteria
Studies published in English with participants who were 18 years or older and examined leaders across all faiths. Studies also included an examination of self-care behaviors among faith leaders within the context of obesity or obesity-related chronic diseases.
Data Extraction/Synthesis
Data synthesis was qualitative and informed by the six-step framework developed by Arksey and O’Malley (2005) as well as updated recommendations by Daudt et al (2013). Of the 418 studies identified and screened, 20 met the eligibility criteria.
Results
Studies were primarily cross-sectional and participants Christian faith-leaders in the US. Most studies did not define self-care or incorporate theory, but focused on vegetarian diets and physical activity engagement. Other self-care related behaviors (eg, sleep, days off), some unique to faith leaders (eg, sabbatical), were included but not systematically.
Conclusions
Research with more diverse faith leaders and that uses theory is needed to guide development of strategies for engaging this population in self-care to reduce obesity and related chronic diseases.
Objective
The prevalence of obesity among United States (US) adults is approximately 42%. 1 Individuals classified as obese are at an increased risk of developing obesity-related chronic diseases (eg, diabetes, high blood pressure, high cholesterol).2,3 However, both obesity and obesity-related chronic diseases can be prevented or reduced through lifestyle behaviors such as physical activity and diet.4,5 These and other lifestyle behaviors (eg, taking time off, sleep) are often included in a broader range of behaviors known as self-care behaviors.6,7
The World Health Organization defines self-care as “the ability of individuals, families and communities to promote health, prevent disease, maintain health, and to cope with illness and disability with or without the support of a health-care provider.” 8 The enactment of self-care may be dependent on one’s view of caring for self – an important construct that enhances health outcomes and aids in the development of positive self-care behaviors.9,10 Within the nursing profession, for example, caring for self and its role in optimizing personal health is acknowledged as important for job performance (eg, fewer sick days, reduced turnover) 10 and reduced burnout. 11
Faith leaders (eg, Christian clergy, Buddhist Priests, Catholic nuns) are another group where caring for self and the incorporation of self-care behaviors is important in reducing burnout. In addition, enacting self-care behaviors may reduce the high prevalence of obesity and chronic disease in this population.7,12,13 Data from studies with Christian clergy indicate obesity may range from 32 to 60% depending on the geographic location, gender, and race/ethnicity of the sample.7,12,14-19 These faith leaders also report having high blood pressure (20-68%), high cholesterol (14-41%), diabetes (10-20%), and arthritis (14-34%).12,14-17,19 Data on other faith leaders is more limited. In studies with Buddhist priests, while their body mass indexes (BMIs) fall within the normal range (20-24.99 kg/m2), they often report having metabolic syndrome (19-30%)20-22 or high blood pressure (20%). 21
The health behaviors of faith leaders also play an important role in the way they discuss health and their willingness to serve as health-related role models for their congregations.23,24 Given faith leaders are influential figures in the communities and congregations they serve, 25 their ability to engage in self-care behaviors have important implications not only for their health, but for the health of those they serve. Reviews of the literature on faith leaders have focused on factors influencing their health (eg, physical, mental) or the prevalence of health outcomes (eg, depression, anxiety, and obesity).26-29 Interventions with faith leaders have also focused on helping them engage in self-care.30,31 However, literature aimed at understanding how self-care is defined within the context of faith leaders health or how self-care influences obesity and obesity-related outcomes among faith leaders is limited. In addition, most research to-date has focused on Christian clergy, with few studies examining the health and behaviors of faith leaders from other religious traditions (eg, Buddhism, Islam, Judaism, Hinduism).20-22,32 Therefore, a scoping review was conducted to broaden our understanding of how self-care has been researched across faith traditions. We aimed to answer two research questions: How does the literature define self-care within the context of faith leaders? And, What research exists examining self-care behaviors within the context of obesity or obesity-related chronic disease outcomes among faith leaders?
Methods
Data Sources
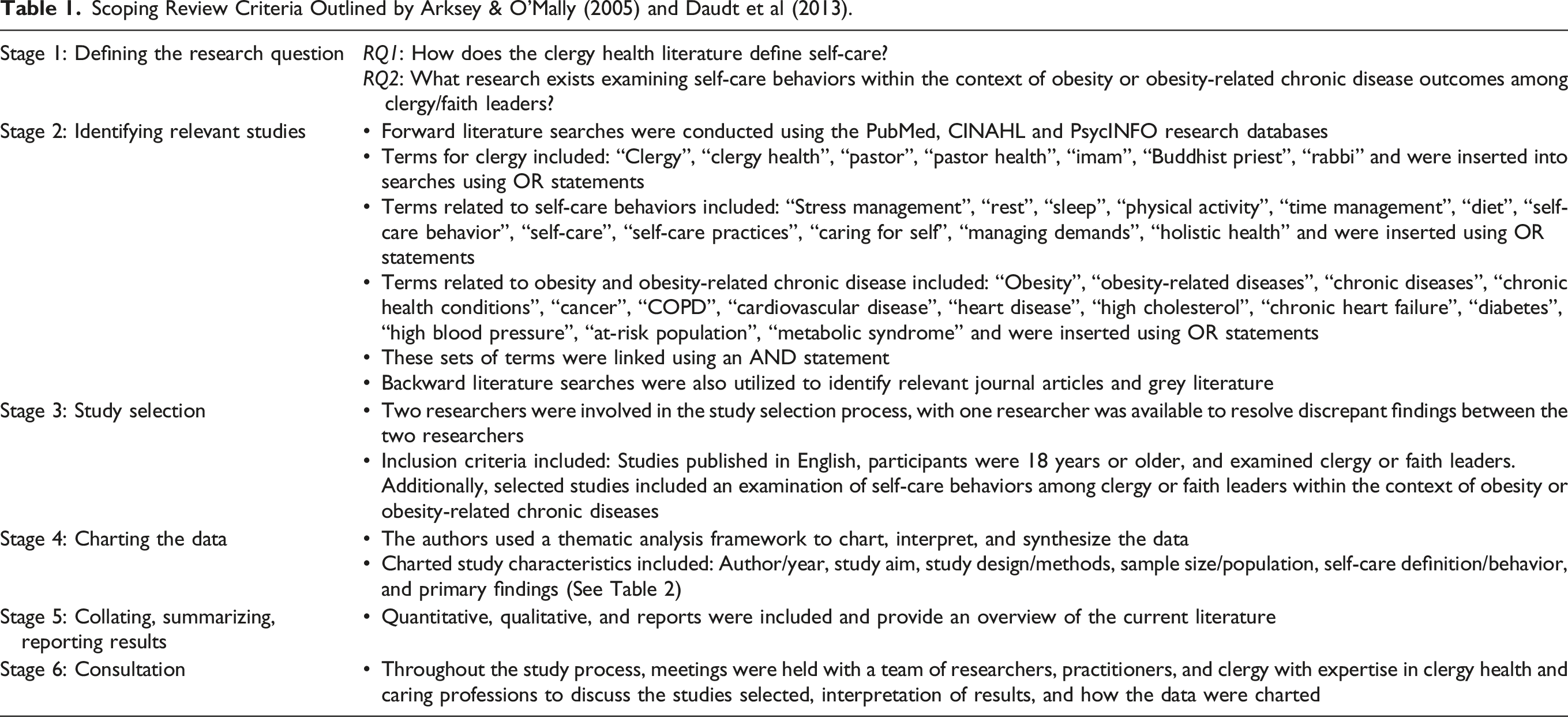
Scoping Review Criteria Outlined by Arksey & O’Mally (2005) and Daudt et al (2013).
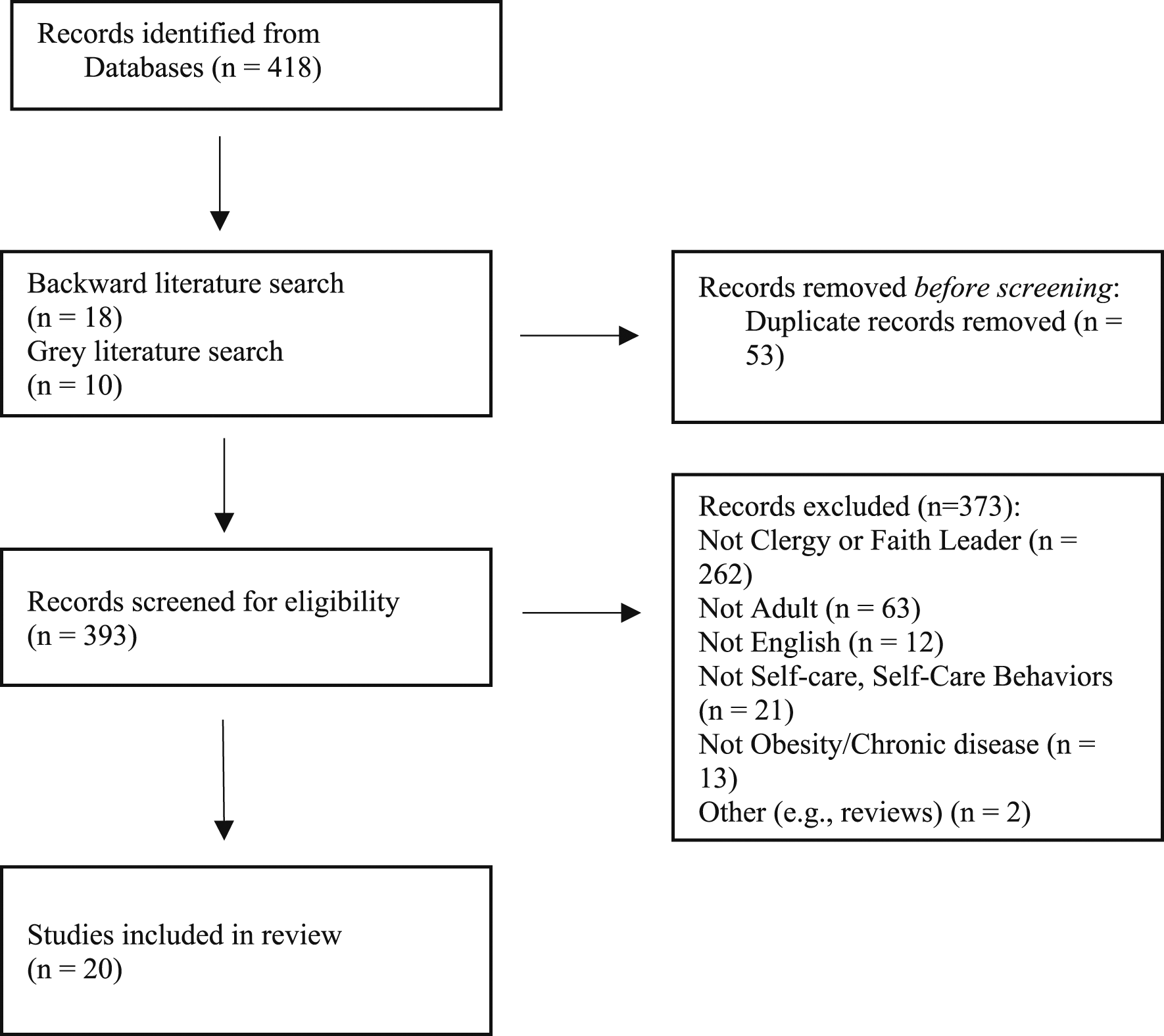
Identification of studies via databases and registries.
Inclusion/Exclusion Criteria
Three researchers (NTW, MH, TC) independently screened and selected titles and abstracts based on the a priori eligibility criteria and research questions (See Table 1). A fourth researcher (BEH) was consulted if any discrepancies were found throughout the screening process. After reaching consensus on articles to screen out, the researchers independently completed a full review of each study. Before screening commenced, 53 duplicate articles were removed. Articles were excluded if they did not focus on clergy or faith leaders (n = 262), self-care or self-care behaviors (n = 21), obesity or chronic diseases (n = 13), adults (18 years or older) (n = 63), were not in English (n = 12), and were review articles (n = 2).
Data Extraction and Synthesis
After initial inclusion/exclusion screening, 38 studies were included in the analysis. Descriptive data were charted from each study including: author, year published, study aim, study design/methods, sample size/population, self-care definition/behavior, and primary findings. Data were charted using an iterative process by NTW and BEH. A draft of the charting form and data were presented to experts in clergy health and the caring professions. After consulting the research team, 18 studies were removed for not meeting the criteria of applying to clergy or faith leaders, self-care or self-care behaviors, or obesity or chronic diseases. Therefore, 20 studies were included in the final analysis.
To collate and summarize findings (Stage 5), qualitative methods were used.33-35 These methods adhered to Braun and Clarke’s (2006) six-step thematic analysis framework including: (1) Becoming familiar with the data from each article, (2) Developing initial codes from charted data, (3) Searching for and identifying themes related to each research question, (4) Assessing identified themes, (5) Naming each theme, and (6) Writing the report. 36 The analysis was conducted by NTW in consultation with BEH and reviewed by the research team. Charted data were organized into three major themes: self-care definition, associations between self-care behaviors and obesity-related outcomes, and self-care as the dependent variable.
Results
Studies included in this review were published between 1982 and 2021. Most studies (n = 15) were published in 2013 or later. The majority of studies were published in the United States (n = 13),7,12,14,15,17,30,31,37-42 with the remaining studies published in South Korea (n = 4),20-22,43 Sri Lanka (n = 1), 32 Canada (n = 1) 44 and Britain (n = 1). 45
Study Design and Characteristics
Summary of Charted Data (N = 20).
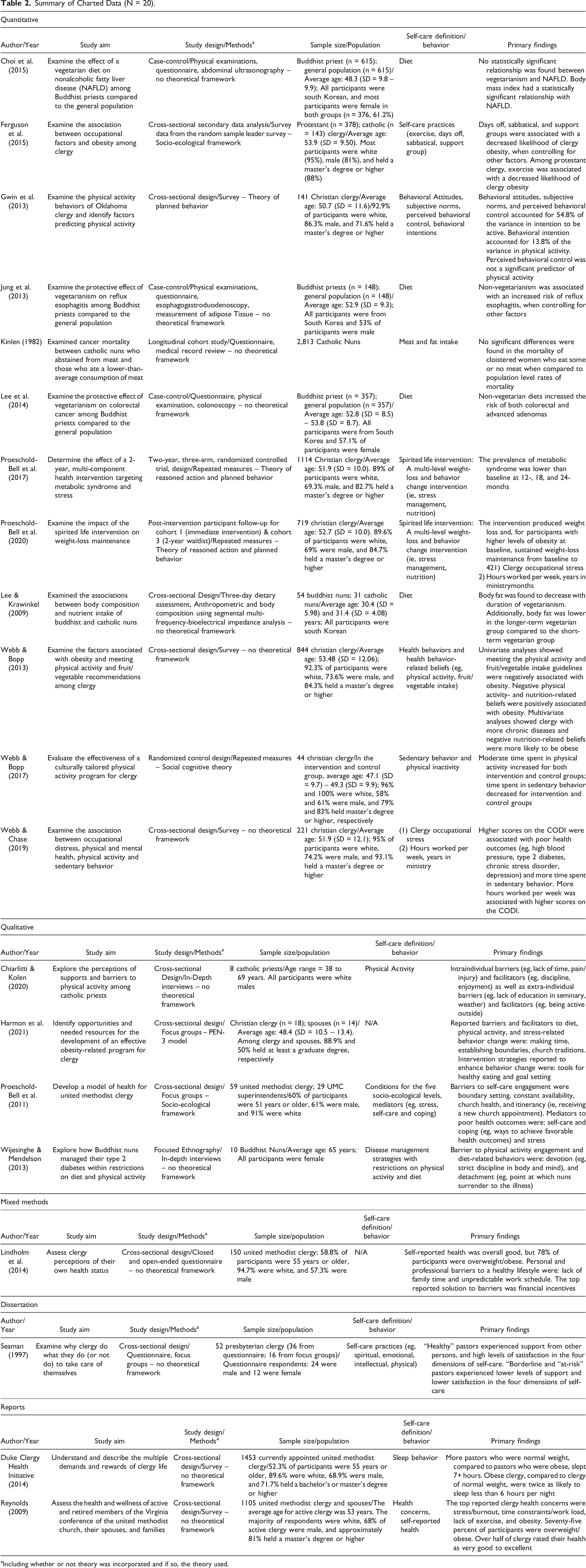
aIncluding whether or not theory was incorporated and if so, the theory used.
Self-Care Definition
Of the 20 studies examined, one study explicitly defined self-care as, “Behaviors and practices intended to promote physical health, mental/emotional health, spiritual well-being, or a combination of all the three” (pg. 705) and this was within the context of United Methodist clergy. 38 Two studies used the term “self-care practices” when introducing the independent variables of their study including: (1) Exercise, support groups, sabbaticals, and days off 7 ; and (2) multi-dimensional self-care practices (eg, intellectual, spiritual, emotional, physical). 42 Most studies (n = 17) made no mention of self-care, rather they examined the influence of specific behaviors on obesity, obesity-related outcomes, or obesity-related behaviors.7,12,14,15,17,20-22,30-32,37,39,40,43-45 These behaviors included: vegetarian diet, physical activity, occupational distress, sleep, boundary setting, and barrier reduction.
Associations between Self-Care Behaviors and Obesity-Related Outcomes
There were four studies that examined the relationship between self-care or self-care practices (eg, physical activity, diet, days off, sabbatical, support group, sleep) within the context of obesity.7,12,17,43 Two studies found inverse associations between engaging in physical activity and obesity.7,12 One study found days off, taking a sabbatical, and attending a support group were negatively associated with obesity. 7 One other study identified participants of normal weight, when compared to participants who were obese, were more likely to sleep seven or more hours/night. 17 One study found that a long-term vegetarian diet produced lower body fat when compared to a shorter duration vegetarian diet. 43 Two studies examining vegetarian diets found a positive association between non-vegetarian diets and obesity-related outcomes (eg, colorectal adenoma, reflux esophagitis).21,22 In contrast, two studies found no protective effects of reduced meat/fat consumption on NAFLD 20 or cancer mortality. 45 One study found positive associations between participant occupational distress and poor health outcomes (eg, high blood pressure, type 2 diabetes). 14 A multiple behavior-change intervention (eg, stress management, nutrition) produced long-term reductions in metabolic syndrome and weight outcomes.30,37
Self-Care as the Dependent Variable
Most studies (n = 4) of self-care within the context of obesity identified factors influencing an obesity-related behavior15,41,42 or ways to reduce barriers and increase self-care engagement. 31 Studies (qualitative: n = 3; mixed-method: n = 1) also identified themes describing barriers to and facilitators of self-care engagement (eg, physical activity, diet, boundaries) among faith leaders. One study described both participant detachment (eg, surrendering to illness) and personal devotion to their faith tradition as barriers to diabetes self-management. 32 Studies (n = 3) found some consistently reported barriers (eg, lack of time, boundary setting, constant availability) to participant self-care engagement (eg, physical activity, diet, healthy lifestyle).38-40
Conclusions
The purpose of this review was 2-fold: (1) explore how the faith leader health literature has defined self-care, and (2) examine obesity and obesity-related chronic disease in the context of self-care among faith leaders. Based on our findings, the literature defining self-care among faith leaders is sparse with most studies focusing on some aspect of physical activity or a vegetarian diet, but without a comprehensive framework of self-care behaviors that may be important to include when working with faith leaders.
Current study findings suggest physical activity engagement and a vegetarian diet were associated with positive outcomes related to obesity and obesity-related chronic disease among faith leaders. Given the numerous health benefits received from physical activity and vegetarian diets4,5 as well as the poor health outcomes seen among faith leaders,7,12,13 it is no surprise most research among faith leaders has examined self-care through this lens. However, considering the challenges faith leaders experience (eg, burnout, complex time demands),26,28,39 additional forms of self-care are likely necessary to help faith leaders find the time and/or be able to prioritize these behaviors. Unfortunately, in the literature reviewed there was no consensus on what these other forms of self-care are or how they align with promoting healthy diet and physical activity behaviors or achieving positive health outcomes. 6 A small sample of studies did find evidence of positive health outcomes (eg, negative association with obesity, improved functioning) when faith leaders spent time in rest, on a sabbatical, and getting adequate sleep.7,17 Moreover, some studies highlighted how faith leaders struggle with a lack of time or setting boundaries with their congregations, which may influence their time spent in self-care behaviors.38-40 Thus, there is a need for future research examining associations with obesity-related outcomes and various self-care behaviors beyond diet and physical activity (eg, sabbatical) as well as associations with these other forms of self-care and engagement in diet and physical activity.
Research was identified related to faith leader self-care, but not within the context of obesity, obesity-related chronic disease, or obesity-related behaviors and thus beyond the scope of this review.24,46-49 These studies, for example, explored pastoral eating and role identities, knowledge of obesity, nutrition and physical activity, spirituality and health, and self-care and job demands in other contexts (eg, mental health). Researchers focusing on obesity and chronic disease may need to explore this self-care literature to identify cross-cutting concepts that can be applied in obesity-related research.
Most studies in this review lacked a theoretical framework, making interpretations of findings and implications for future research difficult at times. It is suggested theory helps explain the meaning of predictions and findings, particularly in the context of health behavior research. 50 A subset of studies did use holistic health models or common health behavior theories to better explain the relationship between self-care and faith leader health,15,30,31,38,39 but the models and theories were examined in a limited context (eg, United Methodist clergy) or did not fully account for the various factors influencing faith leader health. Therefore, investigators should continue applying and adapting theory to enhance the methodological rigor of faith-based research and provide better insight into how faith leaders conceptualize and enact self-care behaviors.
This review also identified a lack of diversity across studies examining self-care among faith leaders. For example, findings show most studies reviewed were cross-sectional with samples consisting of mostly white, male, Christian clergy. This highlights the need for examining self-care and its associations with obesity with more diverse samples and across religious traditions to better understand how self-care is practiced among a variety of faith leaders. Future investigators should use different study designs and more diverse samples (eg, rural/urban clergy, race/ethnicity, gender, and denominations) as well as following participant self-care behaviors, beliefs, and attitudes longitudinally to help determine causal associations with obesity-related outcomes.
Strengths and Limitations
This scoping review has several strengths. (1) To our knowledge, this is the first scoping review to be conducted exploring self-care and health outcomes among faith leaders. (2) Peer-reviewed methodology, developed by Arksey & O’Mally (2005) and Daudt et al (2013), guided this study. (3) A rigorous multi-disciplinary approach (eg, public health, kinesiology, psychology, and theology) was used to develop the research questions and interpret findings. (4) Multiple team members analyzed and coded studies included in this review, further enhancing the accuracy of findings,
Despite the novelty and strengths of this review, there were limitations. (1) While data extraction provided an in-depth insight into each study, quality assessments of studies were not conducted. (2) The research focus was on obesity due to this being a primary focus in clergy-related research to date, but there is growing research in mental health with other outcomes yet to be explored. The review’s focus allowed for statements to be made about self-care within the context of obesity, but limited the ability to examine self-care definitions and behaviors in the context of other health outcomes among faith leaders (eg, mental health, well-being). Faith leaders have reported a high prevalence of obesity and obesity-related chronic disease. Given the role of faith leaders, self-care engagement has important implications for their own health and the communities they serve. It is unclear how self-care has been defined in research conducted with faith leaders as well as associations between self-care variables and obesity-related outcomes among faith leaders. Findings from this review show literature defining self-care among faith leaders is sparse with most studies focusing on a few behaviors (eg, physical activity, vegetarian diet). Moreover, study findings show much of the literature examining self-care and its association with obesity-related outcomes among faith leaders has rarely incorporated theory, is primarily cross-sectional and includes mostly White and Christian faith leaders. This study reinforces the importance of physical activity and diet when working with faith leaders on obesity and chronic disease prevention efforts. However, these are not the only self-care behaviors that may need to be addressed. Working with faith leaders to help them take time off and make room for rest and sleep may enhance health promotion efforts. Findings from this review also suggest future research is needed with more diverse faith leaders and study designs guided by theory to inform the development of evidence-based strategies for engaging this population in self-care to reduce obesity and related chronic diseases. Furthermore, faith leaders’ behaviors and behavior change, including those related to self-care, should be contextualized within their environmental settings and the social determinants of health, and thus health promotion practitioners should work to support their healthy behaviors through collaborative work on these external factors.So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Authors’ Contribution
BEH, NTW conceived of the study and assisted with analysis and manuscript writing; TC, MH analyzed the data and assisted with manuscript writing and editing; BLW, JN, KHW, TAW, CHL assisted with manuscript writing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.