
Abstract
This study explores how context-specific behavioral economic principles could be employed to tailor interventions to support patients’ efforts to modify day-to-day routines. Using adapted geo-ethnography techniques, interviews collected in-depth descriptions about facilitators and barriers to physical activity (PA), and contexts influencing decisions about day-to-day activities. Data were analyzed using the Capability, Opportunity, and Motivation - Behaviour (COM-B) model for behavior change and MINDSPACE behavioral economic principles as coding frameworks. Twenty-nine patients (19 men, 10 women) aged 50–79 participated. Findings indicate patients were motivated and capable of increasing PA but were challenged to identify opportunities to adapt day-to-day routines for increasing PA. Patients described disrupting default routines, increasing commitments, changing the messenger, and introducing incentives as potentially useful behavioral economic principles to improve day-to-day decisions about increasing PA. Patients had insight into potential behavioral economic principles, although they were not previously educated, and were valuable partners in developing research and clinic-based behavioral economic intervention strategies.
Keywords
Introduction
Cardiovascular diseases (CVD) are the leading cause of death worldwide, accounting for more than 17 million deaths annually (World Health Organization, 2021a), and one-fifth of all deaths in Canada (Statistics Canada, 2020). These deaths are largely preventable through modification of lifestyle risk factors such as smoking, physical inactivity, obesity, poor nutrition, high blood pressure, and excessive consumption of alcohol (Roth et al., 2020; World Health Organization, 2021b). Behavioral interventions for modifying risk factors are critical for reducing risk of CVD or a repeat event.
The effectiveness of interventions to reduce risk of CVD is hindered by poor maintenance of behaviors after an intervention (Graham et al., 2020; McQuoid et al., 2017) when patients no longer have regular contact with healthcare professionals and peers (Bray et al., 2006). Digital tools have been shown to improve intervention effectiveness by sustaining interaction between patients and clinicians, through individualized monitoring and feedback, and by tailoring interventions to acknowledge the unique requirements of patients to maintain behavior change in real-world settings (Inglis et al., 2010; Santo and Redfern, 2020; Schorr et al., 2021). However, the success of these digital tools can be limited when they do not adequately consider the spatiotemporal contexts within which patient health behaviors occur. This additional knowledge is critical to ensure intervention strategies are tailored to incorporate the timing and location that seemingly automatic decisions patients make as part of their daily routines.
Spatiotemporal contexts play an important role in promoting or inhibiting health behaviors (Macintyre et al., 2002). Identifying the unique social and environmental contexts that influence the timing and location of individual health-related activities is critical for tailoring intervention strategies (Barber et al., 2024a). This is especially important considering the powerful influence of associative learning, where environmental cues become conditioned stimuli that elicit behavior (Havermans, 2013). Spatiotemporal contexts of day-to-day health behaviors previously explored by our research team identify when and where routine health activities can be disrupted to increase physical activity (PA) within a clinic-based intervention for CVD (Barber et al., 2024b). We adapted geo-ethnography mixed-method techniques (Matthews et al., 2005; Milton et al., 2015) to develop a data collection and communication tool for collecting geospatial and temporal contexts of patient PA behaviors. This study identified the context and timing of health promoting activities (i.e. walking in neighborhood in morning or early evening) as well as opportunities for disrupting health inhibiting sedentary activities (i.e. watching television in evening; Barber et al., 2024b). Time-use patterns provide a visualization of patients’ unique spatiotemporal sequencing of day-to-day activities and understanding of when and where interventions can be tailored for disrupting routines and modifying behavior change. This research aims to serve as a critical intermediary step in advancing the development of more effective interventions by exploring how context-specific strategies can be tailored to improve decision-making processes, ultimately making the adaptation of day-to-day routines easier and more automatic.
Limitations of behavioral interventions
Behavioral interventions are often designed with a theoretical framework that emphasizes individual motivation, capability, and cognitive restraint for behavior change (Jacob et al., 2018; Liu et al., 2021; Room et al., 2017; Winter et al., 2016). For example, interventions using cognitive-behavioral strategies for weight management often target underlying motivation, beliefs, and emotions through cognitive restraint training that encourages slow and deliberate decision-making processes toward modifying eating behaviors (Amiri et al., 2020; Jacob et al., 2018). The Capability, Opportunity, and Motivation - Behaviour (COM-B) model is one approach used to inform the design of interventions by explaining how decisions about behaviors are driven by individual capability, opportunity, and motivation (Michie et al., 2011). Yet routine health behaviors are influenced by seemingly automatic decisions about day-to-day activities under constraints of limited time and resources (Betsch et al., 1998; Marteau et al., 2012). These automatic decisions are known as fast thinking and result in health behavior choices that are made unconsciously (Kahneman and Tversky, 1984). Health behaviors are not solely driven by intrinsic, reflective thought processes, and when executive functions are compromised from factors like fatigue, individuals commonly default to automatic decision-making processes that are influenced by environmental contexts and unconscious habits (Kahneman, 2003; Marteau et al., 2012).
Understanding the contexts that influence automatic decision-making processes is critical for tailoring intervention strategies so that behavior change techniques are individualized to the contexts in which patients make choices about their health activities. Strategies from other disciplines like behavioral economics provide insight into cognitive biases that influence automatic decision-making processes and strategies to improve decisions about engaging in health promoting activities.
Contexts of decision-making processes
Behavioral economics is an evolving field, rooted in psychology and economics, that offers insights about cognitive biases that influence decision-making processes (Möllenkamp et al., 2019; Tversky and Kahneman, 1974; Vlaev et al., 2016). Behavioral economic principles have become widely applied within interventions and are distinct from behavioral science techniques (Gilovich et al., 2002; Kahneman and Tversky, 1984). Behavioral economic principles identify that individuals commonly default to heuristics, known as fast-thinking processes, that are automatic and emotionally charged and less commonly use slow, deliberate, and analytic thinking processes to make decisions day-to-day (Kahneman, 2003; Korteling et al., 2018). Nine of the most common cognitive principles that have been used to improve the design of behavioral interventions are outlined by the MINDSPACE framework including messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego (Dolan et al., 2015; Vlaev and Makki, 2018). A more detailed description of each principle within the MINDSPACE framework is outlined within Table 1.
Description of MINDSPACE principles (Dolan et al., 2015; Vlaev and Makki, 2018).
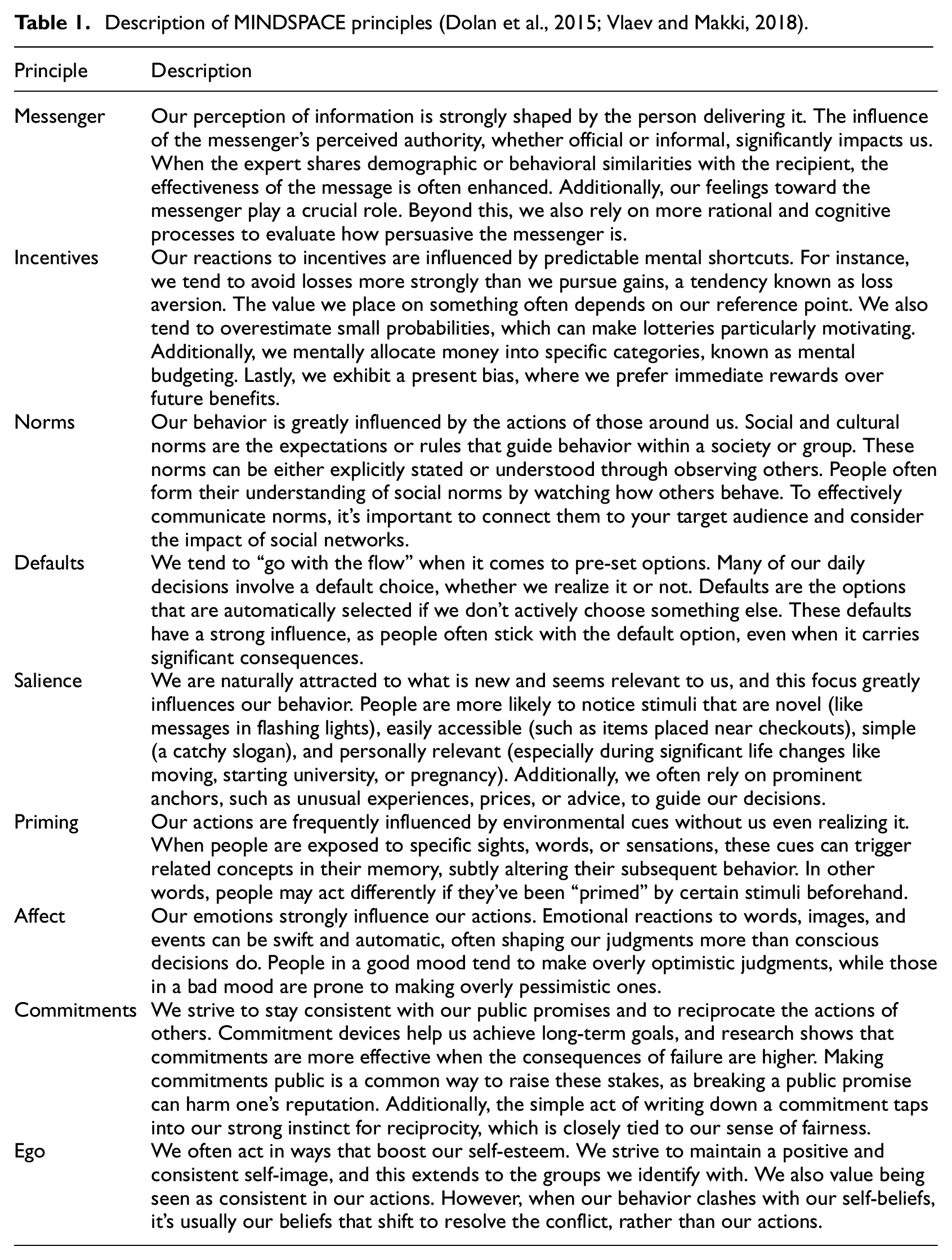
Changing default settings, peer comparison, and introducing incentives are the most widely applied behavioral economic principles that have shown to improve the effectiveness of behavioral interventions targeting healthcare professional and patient behaviors. Incentives are the most widely adopted behavioral economic principle used to target patient PA behaviors (Hare et al., 2021; Waddell et al., 2020). For example, patients who received a FitBit watch for monitoring PA and cash-based financial incentives engaged in significantly more minutes (29 minutes per week) of moderate to vigorous PA compared to patients that received a FitBit watch and charity-based financial incentive, or a FitBit watch alone (Finkelstein et al., 2016).
Interventions tailored to individual needs of patients (Santo and Redfern, 2020) and underlying motivation and cognitive restraint for behavior change (Jacob et al., 2018) do not adequately account for fast thinking and automatic habits that influence decisions about day-to-day health behaviors. Behavioral economic principles provide insight of contexts influencing automatic and fast thinking decisions however, the timing and location of patients’ day-to-day routines are critical for tailoring interventions by identifying opportunities to disrupt routines based on knowledge of when and where health activities occur. It is not evident how behavioral economic principles can be applied to tailor intervention strategies based on contexts of patients’ day-to-day routines and automatic decision-making processes for modifying behaviors.
Aim and objectives
The aim of this study was to explore opportunities for incorporating context specific behavioral economic principles into patients’ PA routines. To achieve this aim, this study answers two more specific research objectives: (1) to identify contexts of facilitators and barriers influencing patients’ capability, opportunity and motivation to increasing PA; (2) to identify potential context specific behavioral economic principles that could be used to tailor secondary interventions for CVD.
Methods
Research setting
This study took place in the context of a voluntary cardiac prevention and rehabilitation intervention program for patients presenting risk factors for CVD, or patients that have recently experienced a cardiac event. A more detailed description of the research setting can be found in a previous publication (Barber et al., 2024b).
Study design
This study used a qualitative descriptive approach to gather detailed information about patients’ day-to-day PA routines, including perceptions about factors that influence decisions about activities. Qualitative description is a particularly useful design to gather patients’ experiences and allows first person accounts to be described directly from those experiencing the phenomenon (Bradshaw et al., 2017; Kim et al., 2017; Neergaard et al., 2009).
Patient recruitment and data collection
Purposeful recruitment of potential patients was conducted with patient cohorts enrolled in the cardiac program. Cohorts of 8–10 patients were purposively selected for recruitment if they were in week 2 or 3 of the 6-week program. Recruitment was carried out by a healthcare professional at the cardiac program by first approaching patients with information about the purpose of the study and what would be required to participate. The recruitment process was repeated with 5 different patient cohorts, with 6 patients agreeing to participate from each cohort, to generate a sample size sufficient for qualitative saturation (Hennink and Kaiser, 2022). To acknowledge the time commitment required for patients to be interviewed, every patient was offered an honorarium of a 25-dollar (CAD) gift certificate to a grocery store.
Interviews were conducted in-person by the first author at the cardiac program between June to September 2021. Interviews were structured to gather contextual information about patients’ activities, including what, where, and when routine activities occur, why they occur, relationships that influence activities, and perceptions about adapting routine activities. Patients were also asked to discuss their health goals and factors that support or prevent them from reaching health goals. Interview questions included, “How would you describe your typical activities on a given day?” “What sorts of activities do you do in your neighborhood?” “What are some of your health goals you are working toward?” “Are there times during the day you find it difficult to stay on track with your goals?” “How might your activities be influenced by who you are with?”
Ethics approval
This study obtained ethics approval from Nova Scotia Health Research Ethics Board (REB#1026722). All patients provided informed consent for their de-identified and anonymous personal health information and direct quotes to be included in research results.
Analysis
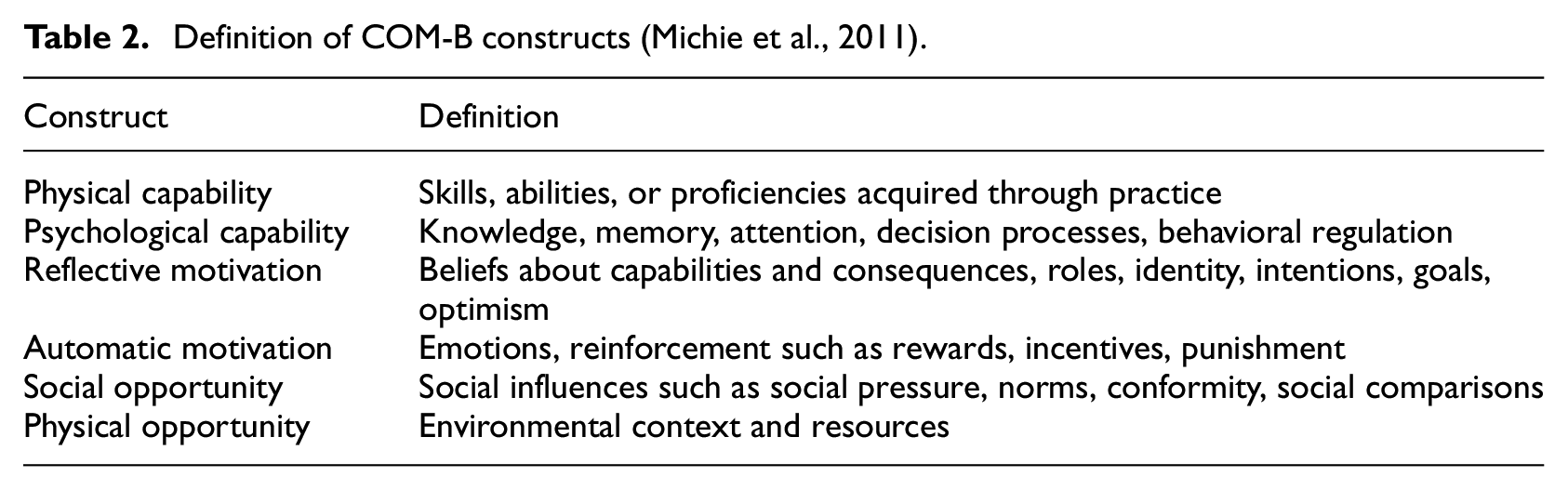
Interviews were audio-recorded, transcribed verbatim, and then coded by the first author with the aid of QSR NVivo12.6.1 qualitative data analysis software (QSR International, 2020). Deductive thematic analysis was employed (Fereday and Muir-Cochrane, 2006), guided by the COM-B model (Michie et al., 2011) and the MINDSPACE framework (Dolan et al., 2015; Vlaev and Makki, 2018) as coding frameworks to address the study’s research objectives. For the first objective, the COM-B model was applied to identify facilitators and barriers to increasing PA (Michie et al., 2011). A more detailed definition of each principle within the COM-B framework is provided in Table 2.
Definition of COM-B constructs (Michie et al., 2011).
For the second research objective, the MINDSPACE framework (Dolan et al., 2015; Vlaev and Makki, 2018) was used to explore patients’ cognitive biases and the potential application of context-specific behavioral economic techniques to improve decision-making processes toward increasing PA. Definitions of MINDSPACE principles are outlined in Table 1.
Data analysis followed a rigorous process of generating initial codes, searching for themes, reviewing themes, and defining and naming themes that represented patient responses (Braun and Clarke, 2006; Fereday and Muir-Cochrane, 2006). The COM-B model served as the coding structure for categorizing emergent themes as facilitators or barriers under each construct of capability, opportunity, and motivation. Similarly, the MINDSPACE framework guided the coding and thematic analysis of patient responses, linking emergent themes to specific behavioral economic principles. The first author (BVB) conducted the initial coding, and themes were collaboratively reviewed and refined with another research team member (MV). This iterative process ensured consistency and credibility in aligning patient responses with the theoretical frameworks, enabling a nuanced understanding of the factors influencing PA behaviors and opportunities for targeted intervention design.
Results
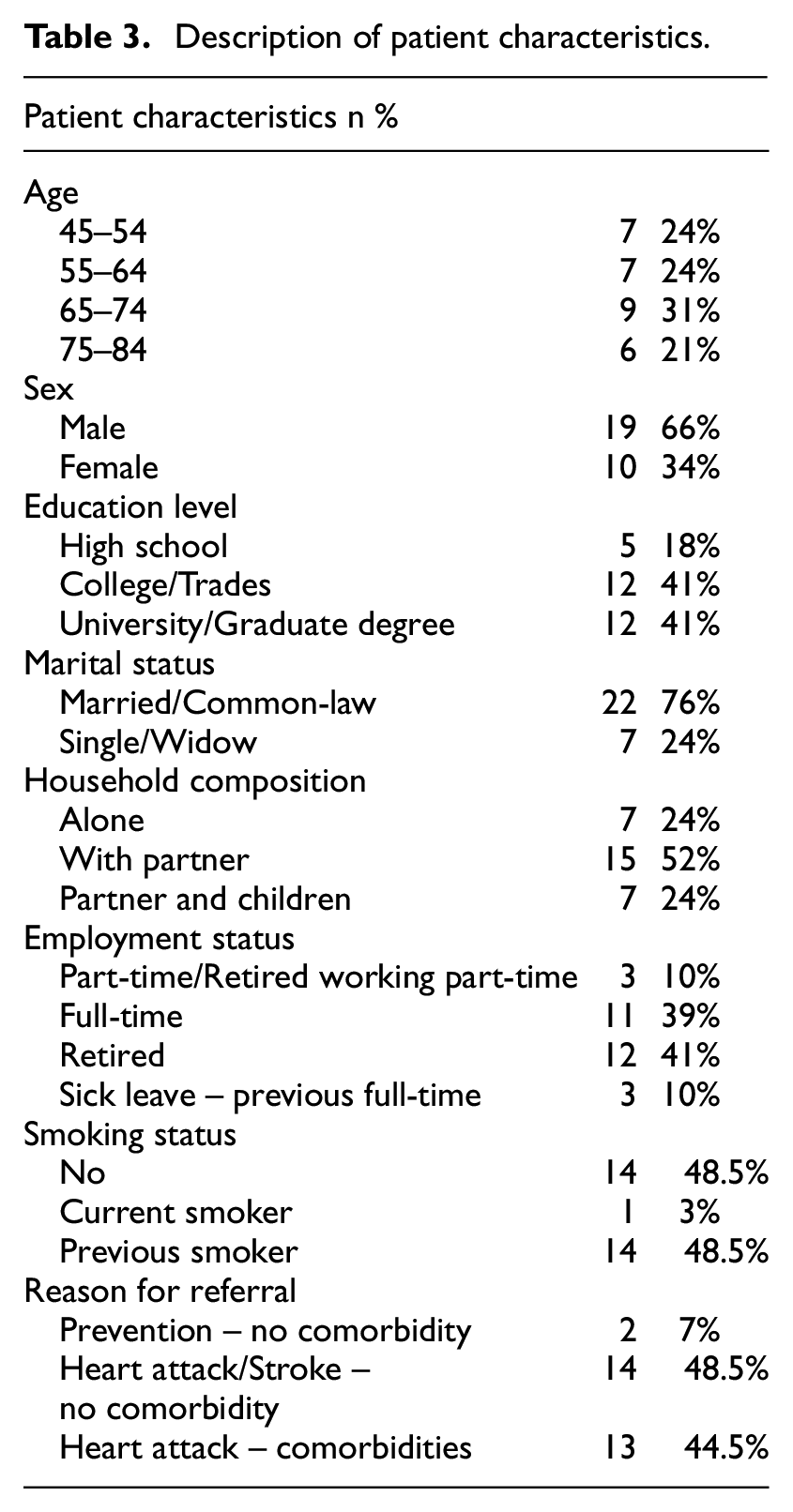
A total of 58 interviews were conducted with 29 patients (19 men and 10 women). Two interviews were conducted with each patient, lasting on average 71 minutes (range 37–110 minutes). A total of 31 individuals were recruited to participate in this study, however, 2 dropped out of the study before the first interview due to lack of time to participate. A detailed description of patient characteristics has been previously published (Barber et al., 2024b) and a summary provided within Table 3.
Description of patient characteristics.
The findings are presented by drawing from patient accounts to describe: (1) facilitators and barriers to increasing PA, and (2) context specific behavioral economic principles for tailoring secondary interventions. Using deductive content analysis, patient-reported barriers and facilitators were categorized according to the constructs of capability, opportunity, and motivation within the COM-B model. A summary of these findings is presented in Figures 1 and 2. Themes aligned with behavioral economic principles from the MINDSPACE framework emerged during analysis, including disrupting default routines, increasing commitments, changing the messenger, and introducing incentives. The interconnections between COM-B-identified barriers to PA and the corresponding behavioral economic principles are visually represented in Figure 3.
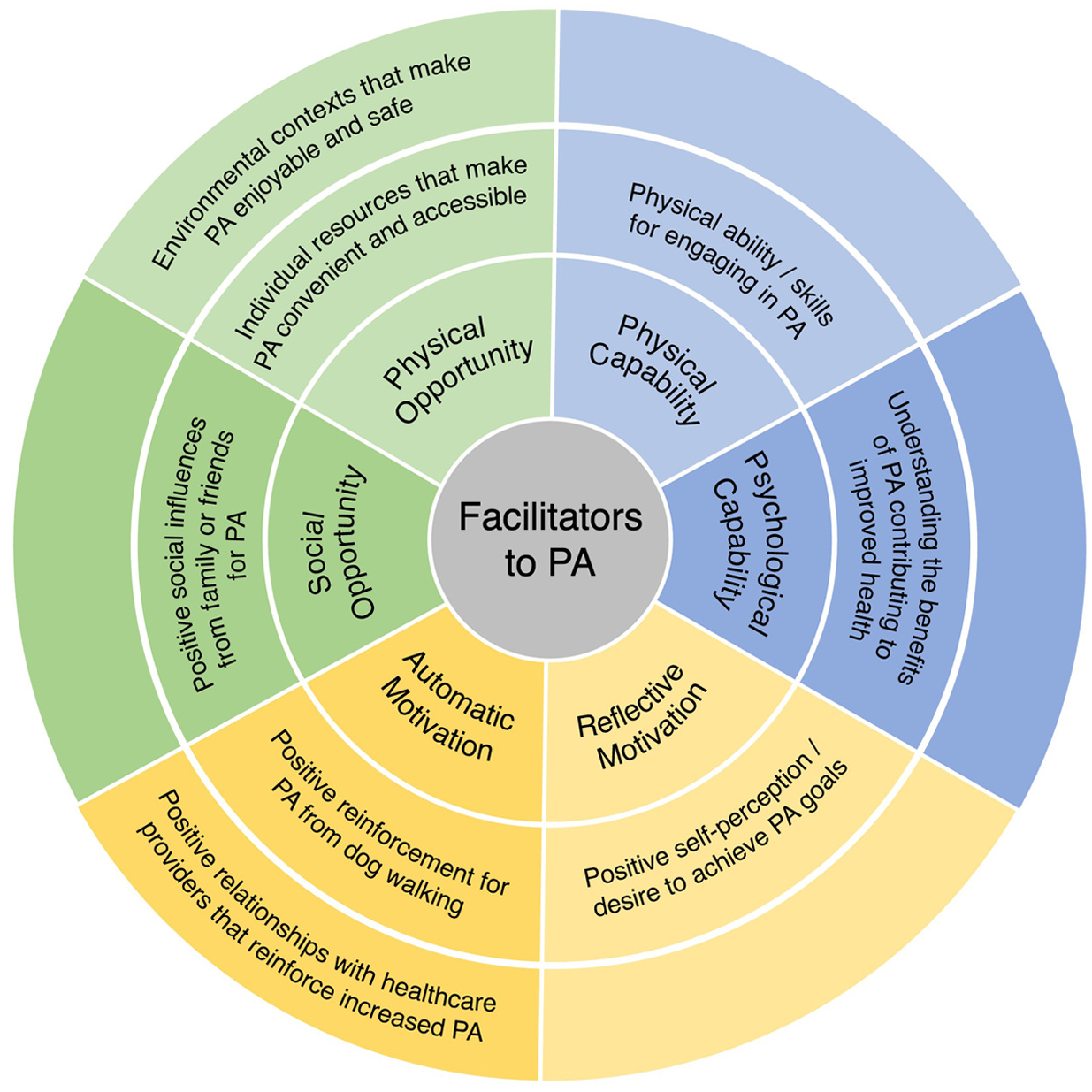
Facilitators to physical activity.
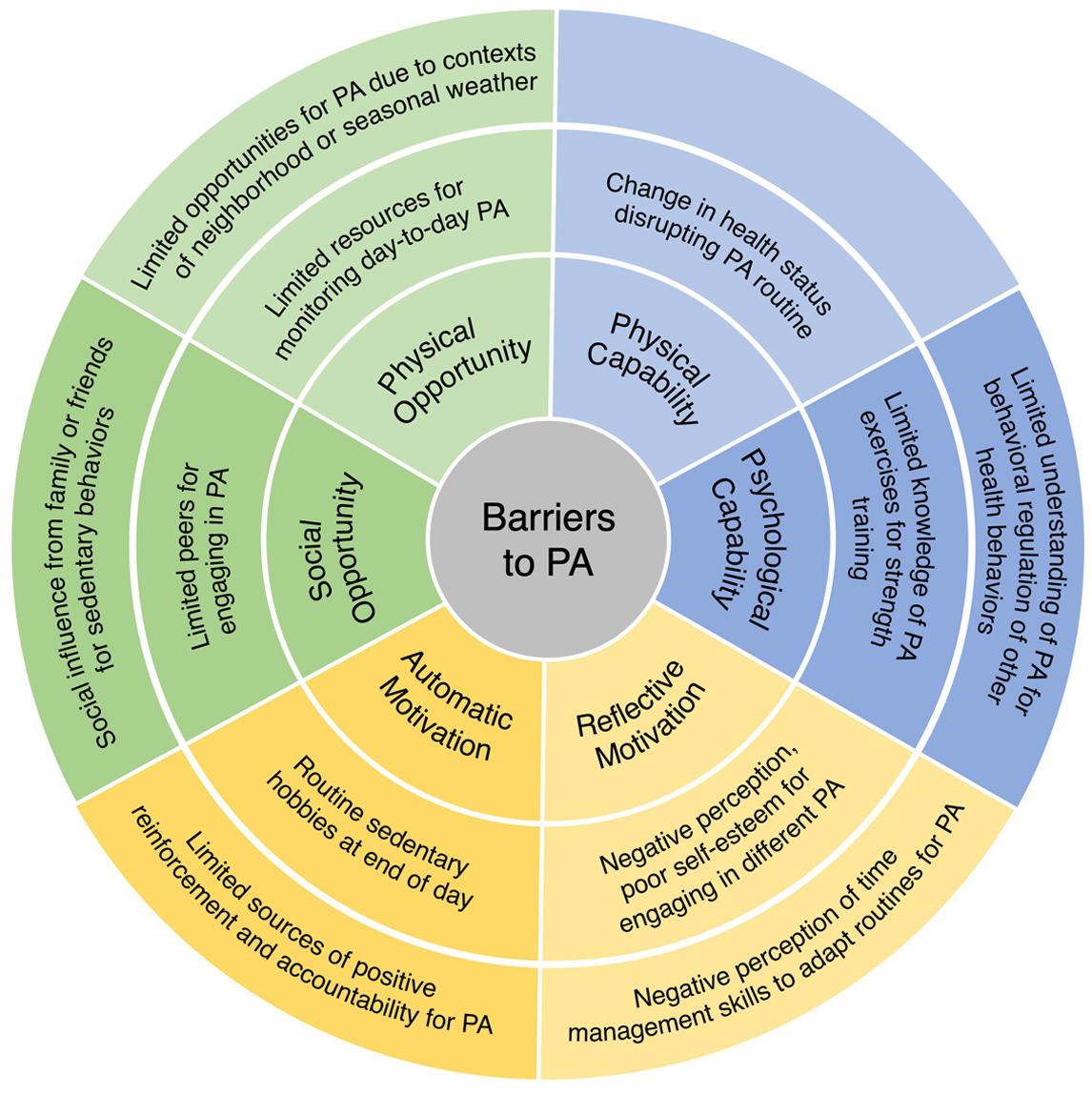
Barriers to physical activity.
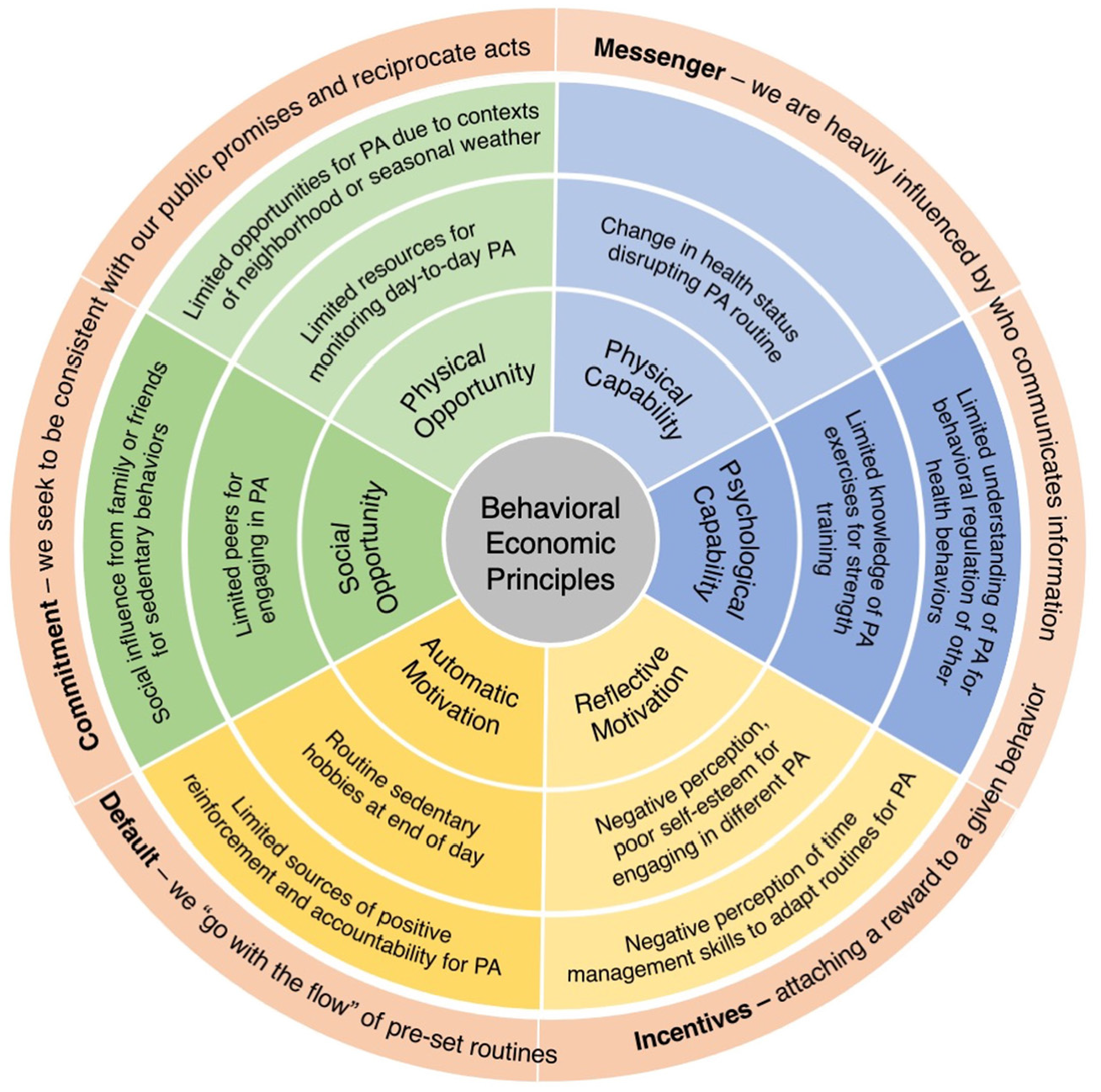
Behavioral economic principles.
Facilitators to increasing physical activity
The following facilitators to PA are presented as health promoting abilities and knowledge, supportive social and environmental influences, and positive beliefs about capabilities and reinforcement (Table 4).
Facilitators to physical activity.

Barriers to increasing physical activity
The following barriers to PA are presented as limiting abilities and knowledge, restricting social and environmental influences, and negative perceptions and accountability (Table 5).
Barriers to physical activity.

Behavioral economic principles
The following behavioral economic principles are presented as strategies to support automatic decisions toward increasing PA like disrupting default routines, increasing commitments, changing the messenger, and introducing incentives (Table 6).
Behavioral economic principles.

Discussion
Contexts that influence patients day-to-day decision-making processes provide important insight for identifying potential behavioral economic principles that could be used to influence seemingly automatic decisions about increasing PA. Results from this study highlight patients had capability and were motivated for increasing PA, but were challenged with identifying opportunities, such as when, where, and how they could adapt day-to-day routines to increase PA. Facilitators to PA are important for understanding patient capability for PA, such as where patients are at along different stages of readiness to change (Mauriello et al., 2017). Barriers to PA provide insight of contextual factors influencing decisions about PA, such as patients’ perceptions of intrinsic and extrinsic constraints influencing opportunities for increasing PA. Although the COM-B model is useful for understanding individual drivers of behavior, the COM-B model is not useful for identifying factors that influence common automatic decisions about day-to-day activities. The integration of behavioral economic principles is critical for understanding patients’ cognitive biases and identifying potential strategies that can support automatic decisions toward increasing PA like disrupting default routines of watching television, increasing commitments by signing up for exercise classes, changing the messenger with texts from healthcare professionals, and introducing incentives to reach daily step count goals. The use of behavioral economic principles as a coding framework provides useful information about tailoring strategies to the spatiotemporal contexts of patients’ automatic decision-making processes. For example, timing and location sequences of patient routine activities provide import information of when and where patients are challenged with task-switching, such as disrupting automatic sedentary routines of watching television after dinner. Future research should continue to explore suitability and efficacy of behavioral economic principles before they are integrated into an intervention to ensure strategies are tailored to the contexts of barriers influencing patients’ cognitive biases and resources and opportunities of different patient populations for reaching behavioral goals.
This study represents a crucial first step in enhancing behavioral interventions by identifying context specific opportunities that make decisions for adapting routines easier and more automatic. Behavioral economic principles are one example of intervention strategies that target fast-paced decision-making processes, such as adding environmental cues to support development of routines that are habitual and automatic (Marteau et al., 2012). Framing, incentives, and social norms are some of the most applied behavioral economic principles within interventions for PA (Blaga et al., 2018; Hare et al., 2021; Waddell et al., 2020). For example, a Nintendo Wii video game using threat-framed messages has shown to improve positive PA attitudes, self-efficacy, and perceived behavioral control among adolescents (Lwin and Malik, 2014). Furthermore, the use of incentives has shown to increase population-wide PA for users of the Carrot Rewards mobile app in British Columbia and Newfoundland and Labrador, Canada (Mitchell et al., 2018, 2020). Our study strengthens the evidence base supporting incentives as an appealing intervention strategy for achieving daily PA goals. However, more than half of patients (n = 16) described their intrinsic motivation for PA and did not perceive that an incentive was necessary to initiate a change in behavior. Although patients had positive perceptions of their motivation and capability for PA, our study patients did not reflect on how their motivation and capability for PA fluctuated throughout the day, such as when they were more likely to default to sedentary activities. When executive functions are fatigued, and patients have diminished self-regulating control for making goal-directed decisions about their behaviors; incentives may be critical for encouraging automatic decisions about adapting routines to reach an individualized goal for PA before the end of the day. Incentives have shown to positively influence PA (Barte and Wendel-Vos, 2017); however, it is less evident whether incentives have been tailored using information about the timing and location of behaviors, such as incentivizing increased PA during times when patients are prone to defaulting to sedentary activities.
Tailoring individualized interventions
The significance of applying behavioral economic principles within this study was to understand the contexts influencing decision-making processes and identify what potential strategies could be applied to tailor interventions to the individual needs and health goals of patients. Results from this study provide insight of the importance of tailoring digital tools to the common decisions patients make as part of their daily routines. For example, information that patients are challenged by limited knowledge of PA exercises for strength training provides an opportunity for healthcare professionals to work with patients to develop their own intervention strategies like scheduling calendar notifications with instructions of different strength training exercises. Calendar notifications could be tailored and delivered at the most opportune time and place based on patients’ existing day-to-day routines, access to equipment, and capability for engaging in different strength training exercises.
Although digital health tools provide a means of delivering behavior change techniques, it is unclear whether technology-based strategies would have the same effectiveness for all patients. For example, 13 patients within this study were using digital tools, including watches or mobile applications for self-monitoring PA, and 16 patients were not using any technology for self-monitoring PA. It is unlikely digital tools used to deliver behavioral economic intervention strategies would have the same impact on patients that regularly interact with technology-based stimuli versus patients that do not use technology. For example, a meta-analysis of interventions using prompts to increase patient engagement with technology-based interventions found small-to-moderate positive effects that prompting reminders increased patient engagement in technology-based interventions in comparison to no prompting strategy (Alkhaldi et al., 2016). To increase effectiveness of interventions using digital tools it is critical interventions are flexible enough to adapt behavior change techniques, so they are specific to individual needs and preferences. For example, interventions could be tailored by delivering individualized counseling via mobile text messages with patients that have high engagement with using technology tools versus offering counseling via phone calls with patients that have low engagement with using technology tools. CVD interventions using mobile text messages to send motivational and educational information that encourage specific PA goals have shown to significantly increase peak aerobic capacity from baseline after 24 weeks post-intervention (Frederix et al., 2015) and increase moderate to vigorous PA minutes (>105 minutes/week) from baseline after 2 weeks post intervention (Legler et al., 2020). Additional research is required to assess long-term effectiveness of digital health tools such as identifying whether digital health tools lose novelty when patients are exposed to the same stimuli over time (Mobekk et al., 2020).
Individualizing digital health tools is also critical for tailoring interventions across diverse patient populations that experience unique facilitators and barriers to behavior change, including chronic time deficits and limited knowledge of self-management strategies (McQuoid et al., 2017; Stuart-Shor et al., 2012). CVD disproportionately affects marginalized populations (Mensah, 2018), including African Nova Scotian populations within communities where this study took place (Kisely et al., 2008). It is not evident how behavioral interventions are adapted to target recruitment of diverse populations and what contextually relevant strategies are used to meet the needs of diverse and marginalized populations (Stuart-Shor et al., 2012). Research methods used in this study could be applied to advance equity, diversity, and inclusion goals by adapting the design of interventions specific to the contexts of diverse populations and community settings. For example, patient populations that experience chronic time deficits are unlikely to participate in a clinic-based intervention (Stuart-Shor et al., 2012), however, digital technologies provide a means of delivering interventions remotely using individualized health education and counseling strategies. By integrating geo-ethnographic techniques (Barber et al., 2024a, 2024b), interventions could gather information of patients’ time-use patterns and tailor strategies to the unique social and environmental contexts influencing opportunities for adapting health behaviors. For example, patients challenged by lack of transportation may be encouraged to participate in an intervention using incentives for daily PA goals, such as encouraging patients to walk to a public transportation stop further away from home. Incentive strategies could also be tailored to encourage patients to watch educational health videos during opportune times when commuting on public transportation.
Integrating strategies from other disciplines
Improving the effectiveness of behavioral interventions to prevent chronic disease and associated risk factors will require evidence from other disciplines and methodologies (Bacon et al., 2020; Nieuwlaat et al., 2013). This study explored why behavioral economic principles are important for understanding contexts influencing decision-making processes and what strategies are potentially useful for improving automatic decisions toward increasing PA. Behavioral economic principles have not yet, to our knowledge, been integrated with geo-spatial contexts to identify the most opportune time and place to deliver behavioral economic principles. When geo-ethnographic techniques and behavioral economic principles are combined, the effectiveness of behavioral interventions can be strengthened by identifying where, when, and how to disrupt routine activities with context specific strategies that improve automatic decisions to increase PA. The sustainability of intervention strategies will depend upon using information about the timing and place of existing routines to support decisions about adapting health activities that are easy and automatic.
Limitations
A limitation of this study was gathering patient perceptions about their decision-making processes without testing whether the identified behavioral economic principles are effective for increasing PA. Future research should consider integrating the APEASE framework to assess implementation of behavioral economic principles and factors influencing uptake of intervention strategies within the contexts of clinic-based interventions (Michie et al., 2011). The APEASE criteria outline important context-based decisions that need to be considered when adapting interventions including: (1) affordability, (2) practicality, (3) effectiveness and cost-effectiveness, (4) acceptability, (5) side-effects/safety, and (6) equity (Michie et al., 2011). Many behavioral economic principles are cost-effective, however, without considering the contexts of existing health interventions, including human and financial resources available, the feasibility of implementing novel intervention strategies may be overlooked.
Conclusion
Coupling behavioral economic principles with spatiotemporal contexts of patient day-to-day routines provides critical information of what behavioral economic principles can be tailored based on knowledge of when and where patients’ health activities occur. This study explores facilitators and barriers to increasing PA and how behavioral economic principles could potentially be used to tailor secondary interventions for CVD. Results indicate patients were capable and motivated for PA, but were challenged with identifying opportunities for adapting routines to increase PA. Disrupting default routines, increasing commitments, changing the messenger, and introducing incentives were identified as potential behavioral economic principles that could be applied to influence patient decision-making processes for increasing PA. Further research is required to implement and test the use of behavioral economic principles identified in this study to explore whether the identified methods are effective at improving the design of CVD interventions.
Footnotes
Acknowledgements
The authors would like to acknowledge the time and effort of all research participants and the cardiac prevention and rehabilitation intervention program in Nova Scotia where this study took place. This research would not have been made possible without the support and guidance of the program director and team of healthcare professionals that supported recruitment and data collection.
Author’s contributions
The authors confirm contribution to the paper as follows: study conception and design: BVB, GK, MV, RM, DR; data collection: BVB; analysis and interpretation of results: BVB, GK, MV, RM, DR; draft manuscript preparation: BVB, GK, MV, RM, DR. All authors read and approved the final version of the manuscript.
Data sharing statement
The data that support the findings of this study are not publicly available to ensure the privacy and protection of the participants’ identities. Anonymized and de-identified data may be made available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Maritime SPOR Support Unit (#2420)
Ethics approval
Ethics approval for this study was obtained from Nova Scotia Health Research Ethics Board (REB#1026722).
Informed consent
All patients provided informed consent for their de-identified and anonymous personal health information and direct quotes to be included in research results.