
Abstract
Purpose
The present study identified the vulnerable IPV cohorts of South Asian women, and the prevalence of and predictors of the women’s IPV acceptance.
Design
Cross-sectional survey - the United Nations Children’s Fund multiple index cluster survey.
Setting
Many South Asian women are accepting of IPV. Studies mostly focus on individual countries.
Subject
103 139 ever-married women from Bangladesh, Laos and Nepal.
Measures
Women’s attitudes toward IPV were measured using a set of five, fixed, binary responses.
Analysis
Following bivariate analysis, complex survey weight adjusted logistic regression models were fitted for individual country data, and the pooled sample.
Results
Of the sampled South Asian women 27.8% accepted IPV, and no major variation among countries in IPV acceptance. Education was the most reliable protector against IPV acceptance whereby, higher educational attainment systematically reduced IPV acceptance (OR = .61 [.56-.83]). Other significant protective factors were being un-married (Married OR = 1.34 [1.28-1.42]), having increased wealth (OR = .71 [.56-.83]), and being over 24 years old (OR = .88 [.83-.97]).
Conclusion
Only education produced absolute consistency at the country and region level; there seems to be no blanket solution for regionally reducing women’s IPV acceptance rates in Southern Asia. Focus on the least educated women and making education more accessible should be prioritised. Future IPV studies can consider measurement methods for women’s direct exposure to patriarchal standards and within community interaction.
Keywords
Introduction
Intimate partner violence (IPV) is defined as any act of brutality committed against an individual by an intimate or romantic partner 1 . Behaviours considered as IPV include those which result in harm, or the threat of harm through psychological, neglectful, physical, or sexual means. 2 Due to the exceedingly negative health and wellbeing implications associated with this brutality, including long-term physical and mental trauma, or even death, IPV is a recognised global health concern.2-4 A major concern encompassing intimate partner violence against women (IPVAW) is that many women hold supportive attitudes about spousal violence,5,6 and in some cases are even more accepting of IPV than men; a finding especially common in low- and middle-income countries (LMICs)7-9 and regionally in Southern Asia (SA).8,10
Investigations concerning heightened IPV acceptance rates have shown that women exposed to certain IPV prevalence risk-factors, including low education level, poverty, being married, lower age of marriage and exposure to childhood violence,2,4-6,8,11-16 as well as certain cultural and social norms such as living in a patriarchal society, are more likely to accept such violence inflicted upon them5,17, as cited in9,10. Critically, because greater IPV acceptance is associated with higher IPVAW occurrence2,6, with IPV effecting 29% of women globally in 2021, and between 35% and 41% of women in SA between 2019 and 20211,18,19; in order to reduce IPVAW prevalence, investigation into the factors which increase the likelihood women will condone IPV is an important area of inquiry. It is expected that by understanding the differences between the groups of women most likely to accept IPV, an improved understanding about the women at increased risk of IPVAW occurrence can be established
Nevertheless, recent, large-scale population-based studies investigating women’s justification attitudinal associations with IPV related risk-factors, together with social factors are limited, especially in the context of SA. Moreover, literature which considers both married and unmarried women is also lacking, thus limiting population application for a number of findings.
Accordingly, the current study aimed to investigate the proportion of women in selected LMICs of SA who hold attitudes of condoning IPVAW, as well as establish whether previously documented IPV risk indicators influence IPV acceptance. Accordingly, a SA applicable model which included Bangladesh, Laos PDR and Nepal was established for regionally predicting women’s likelihood of accepting IPV, with associations found between IPV risk indicators and women’s IPV acceptance then utilised for the purpose of identifying the most IPVAW vulnerable groups within these LMICs of SA. Insights gained from the study expected to provide a valuable contribution toward contemplating actionable approaches for policy makers in improving IPVAW, and therefore contributing to achieving United Nation’s (UN) sustainable development goal (SGD) 5.2 20 to end all violence against women.
Method
Design and Sample
The present study utilised nationally representative data of three Southern Asian countries from round six of the United Nations Children’s Fund (UNICEF) multiple index cluster survey (MICS; 21 wherein, applicability of nations was deemed if the sampled countries were in SA, shared the inclusion of the variables of interest, as well as synthesizable measurement styles of those variables. The samples therefore having been acquired between 2017 and 2019, containing female participants aged 15-49 from Bangladesh, Lao People’s Democratic Republic (PDR) and Nepal.
To ensure valid representation of these populations, using two-stage clustering with consideration of enumeration areas (EAs), MICS (version 6) participants were proportionately selected from the countries’ national population and housing census’ of previous years (2011, 2011 and 2015 respectively). At stage two, systematic random sampling of EA produced clusters of 20-25 households and lead to surveying of potential participants from Bangladesh, Laos PDR and Nepal.
For the purposes of the current study, restrictions were applied to the initial MICS national samples wherein, women were removed listwise from analysis if they did not respond to at least one of the violence against women items (the variable of interest), or at least one of the media exposure items (frequency of watching television, reading newspaper or magazine, listening to radio). As were women who did not respond to any one of the sociodemographic or additional non-sociodemographic predictors. Furthermore, as marital status for Laos included one more category (living with a partner) than marital status for Bangladesh and Nepal, for consistency, those women from Laos PDR were removed. The final sample comprised of 64 105, 24 425, and 14 609 women from Bangladesh, Laos PDR, and Nepal, respectively.
Measures
Outcome Variable
In order to establish the prevalence of women’s attitudinal acceptance of IPV, and its associations with additional explanatory factors, the outcome variable was women’s attitudes toward domestic violence. Women’s attitudes toward IPV were measured using a set of five, fixed, binary response (yes/no) questions which asked women whether a husband is justified for beating his wife if: (1) she goes out without telling him, (2) if she neglects the children, (3) if she argues/quarrels with the husband, (4) if she refuses sex with the husband, and (5) if she burns the food. In order to support informative post-study discussion, in line with previous similarly focussed studies7,8,22, IPV was measured dichotomously - if the respondent answered yes to any of the justifications for a husband hitting or beating his wife she was classified as presenting IPV attitudinal acceptance (Yes = 1), and if she did not respond yes to any of the five items she was classified as not presenting IPV attitudinal acceptance (No = 0).
Independent Variables
To gain insights about sociodemographic associations with women’s attitudes toward IPV, five consistently documented IPV risk indicator, population-based, demographic explanatory variables were considered: wealth index, age, education level, marital status, and area of residence2,4-6,8,11,12,14. Wealth index, which was constructed via confirmatory factor analysis by the data custodians (as per the Demographic and Health Survey; 23 was as measured by the data custodians using five categories (poorest/poor/middle/wealthy/richest). Similarly, women’s marital status was considered as either ‘yes currently married’ or ‘no not in union,’ and area as ‘rural’ or ‘urban.’ For all three countries, education was measured as ‘none,’ ‘primary,’ ‘secondary’ or ‘higher.’ For Laos PDR, rural with road and rural without road were combined to represent rural; and ‘lower secondary’ and ‘upper secondary’ were merged as ‘secondary’ education, and ‘post-secondary/non-tertiary’ was collapsed with ‘higher’ to represent post-secondary education. Similar to past studies6,11,14,24,25, respondent’s age was ordinally measured (15-24, 25-34, 35-44, 45-49 years).
To understand the effects of access to media and mobile phone use on women’s IPV acceptance, four additional variables were selected. To measure exposure to media, frequency of watching television, reading the newspaper or a magazine, and listening to the radio (measured as not at all/less than once a week/at least once a week/almost every day) were extracted. Each was then collapsed dichotomously so that responses to any of the media items of at least once a week or more reflected ‘yes exposed’ and responses of less than once a week ‘not exposed.’ Ownership of mobile phone (yes/no) was included in its original format. Finally, data from each of the countries was combined, allowing for a single, nominal country variable to be included in the final analysis for comparison. For modelling purposes, information on survey weights and clusters were retained.
Statistical analyses
In order to investigate primary associations between the predictors with women’s IPV acceptance, alongside enable introductory insights into the differences between the predictive factors and the prevalence of women’s IPV acceptance for the populations, using SPSS version 27, frequency distributions for each country against each variable were produced. Additionally, using weight and cluster adjusted Chi-square
Due to the clarity of interpretation using odds ratios and robustness to violations of multivariate normality and equal variance-covariance 26 , for comparisons across countries to be made, a complex survey weight- and cluster-adjusted binary logistic regression model was fitted to the pooled sample of the selected LMICs with women’s IPV acceptance as the outcome variable.
In response to unequal sizes between groups for some of the variables, and insufficient previous literature to credibly compare the results of the present study against, to ensure replicability and reduction of type 1 errors, a P-value threshold for significance of .005 was imposed 27 .
Results
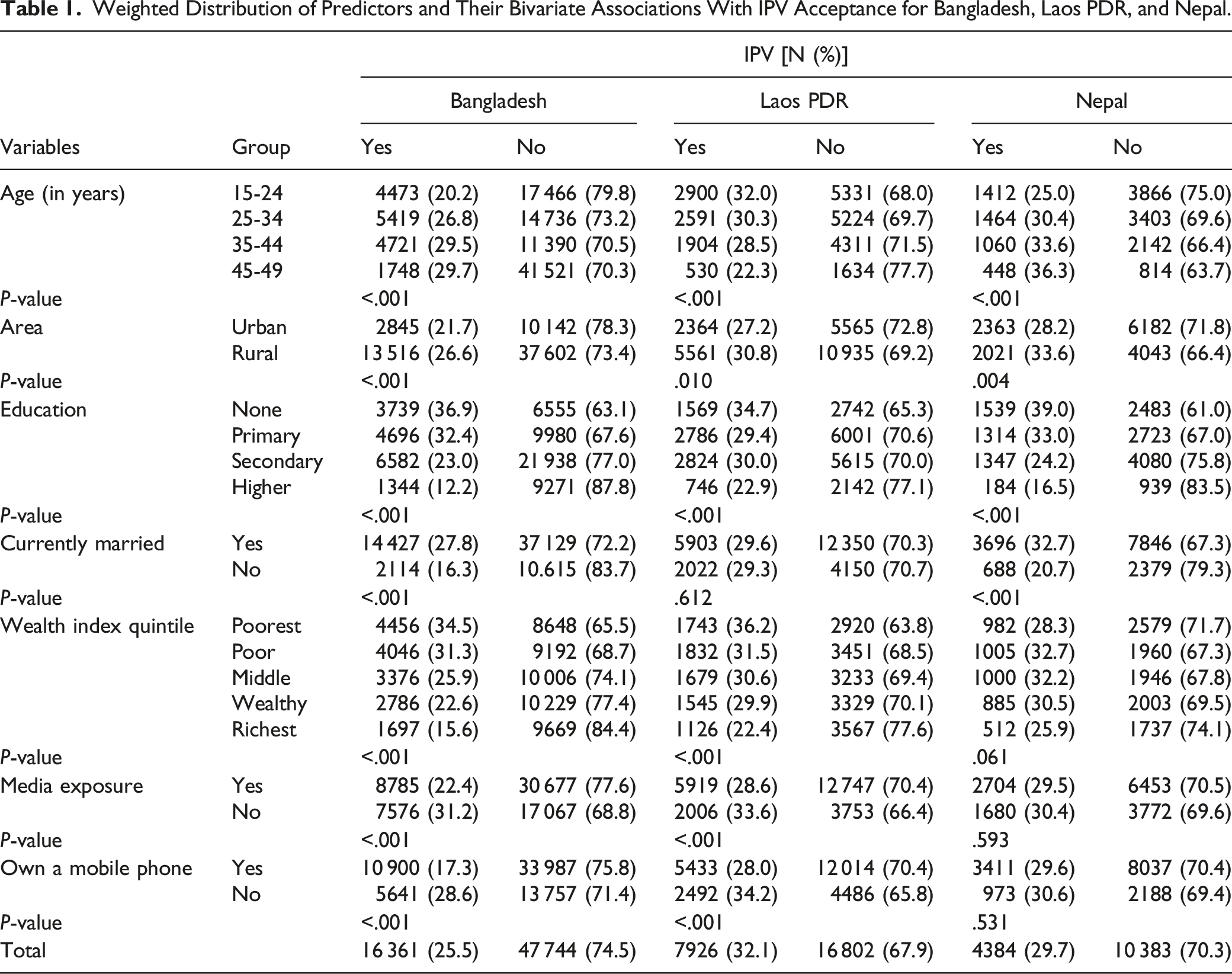
For the combined sample of 103 139 SA women, the highest proportion of participants were aged between 15 and 24 years (34.4%), married (78.7%) and living in rural areas (71.4%); and participants’ highest level of reported education was most commonly secondary education (41.1%) with the least participants having attended post-secondary school education (14.2%). There was an approximately equal proportion of women within each of the five wealth index groups, with only slightly fewer being classified as the richest (17.8%). Regarding exposure to media and ownership of a mobile phone, just over two thirds of respondents reported being exposed to media in some form (65.2%), and a slightly larger proportion reported that they owned a mobile phone (71.5%) (detailed breakdown in).
Weighted Distribution of Predictors and Their Bivariate Associations With IPV Acceptance for Bangladesh, Laos PDR, and Nepal.
Complex Survey Adjusted Binary Logistic Regression Model Fitted to IPV Acceptance With Listed Factors for the Pooled Southern Asian Sample of Three Countries Namely Bangladesh, Laos PDR, and Nepal.
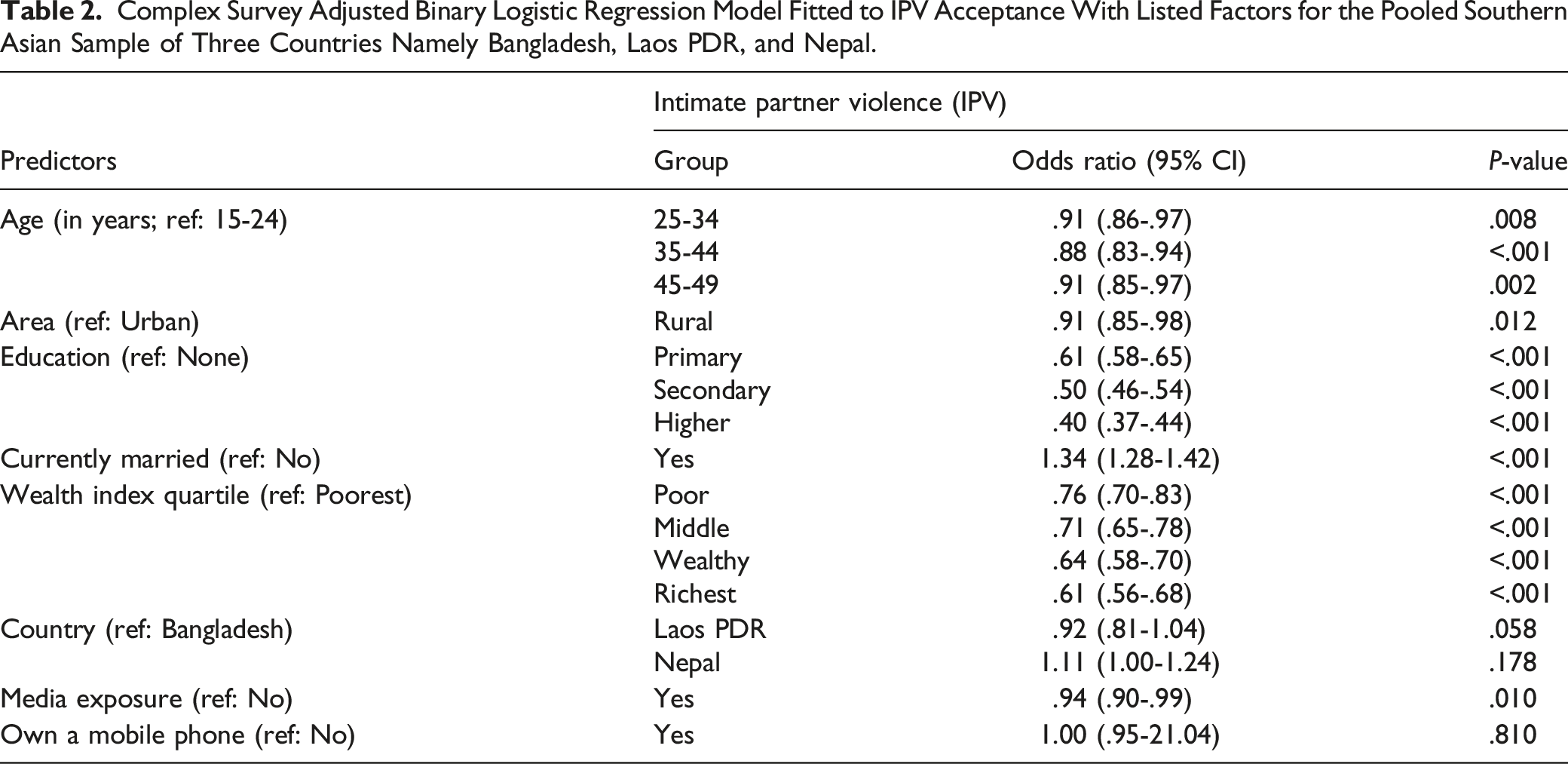
Results presented in Table 2 indicate that married women were 34% (OR: 1.34, 95% CI: 1.28-1.42) more likely to be accepting of IPV than unmarried women, and those who were the least educated were up to 60% more likely to accept IPV than the most educated. Specifically, compared with those who had no education, women with primary, secondary, and higher education were 39% (OR: .61, 95% CI: .58-.65), 50% (OR: .50, 95% CI: .46-.54), and 60% (OR: .40, 95% CI: .37-.44) less likely to be accepting of IPV, respectively.
Wealth index also presented significant systematic differences in women’s IPV acceptance whereby, women’s IPV acceptance decreased as wealth index increased. Specifically, when compared with those who were the poorest, poor women were 24% (OR: .76-95% CI: .70-.83) less likely to be condoning of IPV, middle class women 29% (OR: .71, 95% CI: .65-.78) less likely, the wealthy 36% (OR: .64, 95% CI: .58-.70) less likely, and the richest 39% (OR: .61, 95% CI: .56-.68) less likely to be condoning of IPV. For differences between age groups, when compared with the youngest group of women (aged 15-24), only those who were aged between 35-44 (OR: .88, 95% CI: .83-.94), and those aged between 45-49 (OR: .91, 95% CI: .85-.97) presented significant decreases in IPV acceptance.
Area of living, media exposure and owning a mobile phone indicated no change in women’s IPV acceptance at the .005% level, and consequently, did not influence women’s IPV acceptance for the pooled sample. As reported in Supplementary Tables 2S-4S of the supplementary section though; area, media exposure and mobile phone ownership was found to be associated in Bangladesh; media exposure in Laos PDR; as well as area and media verging on significant for Nepal.
Discussion
In order to identify IPV vulnerable cohorts of women, the present study investigated women’s acceptance of IPV in SA, and several risk factors associated with such acceptance, but no differences in women’s IPV acceptance across the SA countries was found - suggesting that significant associations of the predictive factors with IPV acceptance within the pooled sample could be considered as applicable to SA as a region.
Overall, education was found to be the most influential predictive factor of women’s IPV acceptance at both regional and national levels. Thus, as women’s literacy and education has been consistently identified as the most consistent protector against women’s IPV acceptance within a number of studies5,6,9,22, education appears to be the most reliable preventative measure in SA, and perhaps universally. This is likely because women’s educational attainment provides more opportunities to be less reliant upon abusive partners18,22, improves the cognitive and social skills required to understand they need not be subjected to violence 18 ; and schools often participate in public health campaigns which provide young women with the support they need to adjust their attitudes toward IPV. Additionally, education acts as a protective factor against young-age marriage (ie, girls are busy with school, so marry later), which in turn reduces both IPV prevalence and acceptance. 22
Accordingly, as women’s education attainment is least common amongst the poorest households of LMICs, 5 the result that increased wealth index is, like education, systematically associated with decreased IPV acceptance for SA is understandable (in line with.5,6,8,11,22 Additionally, and independent from education, as wealth index decreases so do household stressors (ie, financial stress), in turn increasing violent partnership disputes and consequently women’s feelings of suppression and therefore, IPV acceptance. 28
Importantly too, within the pooled sample, older individuals being more accepting of IPV was only evident when a generational gap was present whereby, both the youngest and the oldest women are most likely to be accepting of IPV. As also reported for IPV prevalence in 25 study, results from the present study therefore supportive of a U-shape in IPV acceptance across age groups for SA. And so, as marriage for the pooled sample lead to increased IPV acceptance, but not at the country-level for Laos PDR - with consideration that in Laos PDR age of first marriage is on average 3 years older than in Nepal, and up to 5 years older than in Bangladesh28-30 - because increased strength of patriarchal societal values is associated with younger marriage, and increased patriarchal values are associated with heightened IPV acceptance5,22,31, the effects of both marital status and age on women’s IPV acceptance could in fact be moderated by women’s age of first marriage (see 7 ).
Contradictory to some previous literature, living area was not a predictor of women’s IPV acceptance for SA in this study; and in line with Biswas et al. 22 and Serrano et al. 6 findings, if it had been, rural living woman tended to be less accepting of IPV than their urban living counterparts. Thus, as sense of community is believed to be higher within rural areas, which has in turn been connected to improved positive attitude adoption and consequently reduced IPV prevalence 15 , it is possible that higher occurrence of social interactions of rural living women might blunt the direct effects of living area on women’s IPV acceptance - or simply that previously identified predictors of IPV acceptance and prevalence have changed with time.
One possible explanation for such a change over time could be women’s increased access to media and mobile phone use. Contradictory to this though (and contrary to5,10, neither exposure to media nor ownership of a mobile phone were significant predictors of women’s IPV acceptance for the pooled SA sample. Consequently, although media exposure and mobile phone ownership generally promote awareness and women’s support networks subsequently reducing IPV acceptance 31 ; given that at least one form of the technologies resulted in reductions of women’s IPV acceptance for Bangladesh and Laos PDR, the interchanging national effects of media exposure and mobile phone ownership on women’s IPV acceptance is likely the result of underlying cultural differences, suggesting implications for technologically based IPV acceptance prevention strategies across borders.
Thus, with consideration of the potential effects things such as age of first marriage, and patriarchal exposure on women’s IPV acceptance; alongside that women’s IPV acceptance was not found to differ across countries - in order to best expand research concerning women’s IPV acceptance, especially for region level investigations, additional variables which better take into account inter-nation cultural differences require inclusion in future studies. Hence why, finding means of accurately measuring women’s direct exposure to patriarchal values, as well as social and community level interactions would be necessary. Additionally, and in line with the limitations of the present study, future inclusion of men’s IPV acceptance attitudes would allow comparisons between men and women; and measurement of attitudes concerning additional IPV types (ie, emotional and mental) would improve understanding of IPV as a whole. Lastly, the addition of qualitative questions would enable subjective assessment and therefore deeper understanding of the intricacies of results such as these. Note though, as the present study was cross-sectional, causal interpretation of the results must be done so with caution.
Conclusion
The present study revealed that for Bangladesh, Laos PDR, Nepal and SA as a whole, women’s education should be considered as the primary driver of prevention when it comes to understanding and reducing their IPV acceptance. Not only has education presented consistent results across a number of regions and countries within a number of IPV acceptance studies but has now also displayed stability at the individual country-level as well as regionally in SA. Consequently, and in working toward achieving goal 5.2 of the Agenda for Sustainable Development
20
to end all violence against women, as IPV vulnerable groups need to first be identified and subsequently prioritised, for SA, education would be the best starting point. Specifically, policy makers should find ways to improve SA women’s access to education, and also focus IPV prevention programs at those who are the least educated. Many South Asian women are accepting of IPV. In working toward improving IPV against women of the region, the present study identified the vulnerable IPV cohorts of South Asian women and how education provides the strongest evidence for a possible social intervention. Policy makers should implement strategies on a country-by-country basis, focussing on the least educated women, and by making education more accessible.So What
What Is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgments
The authors would like to acknowledge the United Nations Children’s Fund (UNICEF), who conducted the nationwide survey and made their data freely accessible.
Author Contributions
LA Pettitt conducted literature review, performed formal analysis, and drafted the manuscript. RK Biswas conceptualized the study, synthesized the analysis plan, and edited the manuscript. J Bhowmik structured the manuscript, aided in variable selection, and drafted the manuscript. The final manuscript was read and approved by all the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.