
Abstract
Objective
This review comprehensively examines interventions which sought to improve the occupational safety and/or health of construction workers. Factors that explain the (in)effectiveness of interventions were also summarized.
Data Source
This review consisted of a search using two electronic databases, PubMed and Web of Science.
Study Inclusion and Exclusion Criteria
Targeted workers in the construction industry; had at least one primary outcome that aimed to improve occupational safety and/or health; were published between January 01, 1990 and December 01, 2019; and were written in English.
Data Extraction and Synthesis
Two researchers independently carried out the process of reviewing the titles, abstracts and full texts, and extracted all data. If there were differences, discussions were held until a consensus was reached.
Results
A total of 1297 articles were retrieved and 24 were selected for final evaluation. Seventeen studies reported significant intervention effects, while 7 found their primary outcome not significantly improved.
Conclusion
Future research should place more effort on interventions aimed at improving both occupational safety and health outcomes in an integrated manner, with environmental interventions that accompany behavioral interventions at the individual level. Besides, additional effort is also needed to ensure the involvement of relevant stakeholders in designing the intervention, avoiding contamination effects (through cluster randomization), optimizing the “dosage” of intervention, and improving measurement of outcomes.
Indexing Key Words
1. Manuscript format: literature review 2. Researchpurpose: intervention testing/program evaluation 3. Study design: randomized trial/quasi-experimental 4. Outcome measure: morbidity/mortality 5. Setting: workplace 6. Health focus: fitness/physical activity, nutrition, smoking control, social health, spiritual health, weight control 7. Strategy: education, skill building/behavior change, incentives, culture change, built environment 8. Target population age: adults 9. Target population circumstances (specify all that apply): education/income level, geographic location
Objective
Construction is considered one of the most dangerous industries due to its high injury and mortality rates. In 2005, the International Labor Organization (ILO) estimated that more than 60 000 people lose their lives on the job in the construction industry each year globally. 1 In developed countries, 25-40% of occupational deaths take place at construction sites, despite the fact that the construction industry employs only around 6-10% of all workers. 1
Besides occupational safety, construction is also a high-risk industry in terms of the burden of chronic diseases. Studies suggest that construction workers have higher prevalence of behavioral risk factors, including alcohol use, 2 smoking, 3 and unhealthy diet, 4 compared with those in other industries. These unhealthy behaviors increase the risk for chronic diseases such as cancer, heart disease, cerebrovascular disease, and pneumonia, accounting for 66.5% of male and 69.6% of female mortality among construction workers according to a report by the Ministry of Health, Labour and Welfare in Japan. 5 Mortality from chronic diseases can be even higher than that due to accidents. For example, among the 818 deaths in a cohort consisting of 19 943 male German construction workers who were followed for 10 years, 299 died of cancer and 138 died of heart disease, whereas only 36 died of non-transport related accidents (mainly falls and being struck by falling objects). 6
The concept of workplace health promotion was proposed by Sorensen and Barbeau to better integrate occupational safety with health promotion. Evidence shows that an intervention that simultaneously targets both occupational safety and health could achieve higher uptake and effectiveness. 7 This perspective derives from the complementarity principle articulated by Dow, Philipson, and Sala-i-Martin. 8 The principle refers to the idea that intervening to reduce threats to health in one domain (e.g. reducing hazards for occupational injury) simultaneously increases the marginal benefit of investing in an unrelated domain (e.g. smoking cessation). For example, in the WellWorks 2 Trial, blue collar manufacturing workers were reluctant to change their smoking behavior following a health education program because, as they told researchers, they were already exposed to the same chemicals (present in cigarette smoke) in their workplaces, which reduced their motivation to quit smoking. 9 Motivations to change behavior can be affected by socio-environmental factors, and hence interventions need to be comprehensive, and address multiple levels of influence. Indeed, an intervention that combined individual education efforts with a work-site level occupational health and safety intervention to reduce chemical hazards in the workplace resulted in twice the smoking cessation effect compared to the individual education-only intervention.9,10
This brief review suggests that a multi-level intervention (MLI) design, 11 promoting a combination of behavior change at the individual level and occupational safety at the workplace level, would be more effective in improving both safety and health among construction workers.
To our knowledge, there has not been a review of interventions targeted to construction workers from the above-mentioned theoretical viewpoints. Therefore, we sought to (1) summarize the findings of past interventions aimed at occupational safety and/or health among construction workers, (2) assess whether the interventions adopted a MLI design, and (3) provide suggestions for future studies and worksite practices.
Methods
Protocol
The review was conducted based on the PRISMA extension for scoping reviews (PRISMA-ScR), 12 which is described below.
Data Sources and Search Strategy
This scoping review was conducted in December 2019 through a search of the electronic databases PubMed and Web of Science. The following key word search strategy was applied to both the PubMed and Web of Science databases: (“program” or “prevention” or “intervention” or “measure” or “training” or “effect” or “implement” or “tool” or “preventing”) AND (“civil engineer” or “construction” or “green job” or “green building” or “brick layer”) AND (“trial”). For the search on PubMed, the following filters were used: Article types: Clinical trial; Randomized Controlled Trial; Species: Human; Language: English. For Web of Science, the filters were: Language: English; Document type: Article. The search was conducted in English. The search strategy described above was the final version, used in order to ensure maximum inclusion and determined after a series of pilot searches in which the formula was modified based on the resulting papers. Specifically, “civil engineer”, “green job” and “green building” were found to be important terms to help target studies that placed an emphasis on workers’ safety and health. In addition, specific construction work types were not included in the formula in order to keep our focus at the industry level rather than on specific occupations. For example, our concern was with the safety environment (i.e., industrial safety practices) of carpenters employed at construction sites (as opposed to a self-employed carpenter working on his/her own. However, “brick layer” was included based on informal interviews with individuals in the construction industry, who indicated that brick layers may face unique occupational safety and health challenges compared to other occupations in the field. By including “brick layer” in our search terms, we are not excluding other important occupations or aspects of the construction industry, but rather providing a more targeted lens through which to view the issues and interventions related to occupational safety and health in this field.
Inclusion and Exclusion Criteria
The inclusion criteria for this review led to the selection of intervention studies that: targeted workers in the construction industry; had at least one primary outcome that aimed to improve occupational safety and/or health; were published between January 01, 1990 and December 01, 2019; and were written in English. Studies from any continent, country or area were included regardless of geographical borders. For exclusion criteria, we excluded protocol studies and process evaluation studies.
Data Extraction and Data Synthesis
HH and YL independently carried out the process of reviewing the titles, abstracts and full texts, and extracted all data. If there were differences in the studies extracted by the authors, discussions were held until a consensus was reached.
Results
Study Selection
A total of 1297 citations were retrieved upon searching the selected two electronic databases. 416 records came from PubMed and 881 records were from Web of Science. 1159 records remained after removing duplicates. Then, after screening of titles and abstracts, 131 records were selected for full-text evaluation. Finally, 24 studies met the inclusion criteria and remained for final qualitative evaluation, all with acceptable level of quality.13-36 The PRISMA flowchart of this screening process is depicted in Figure 1. PRISMA flow chart of the selection process.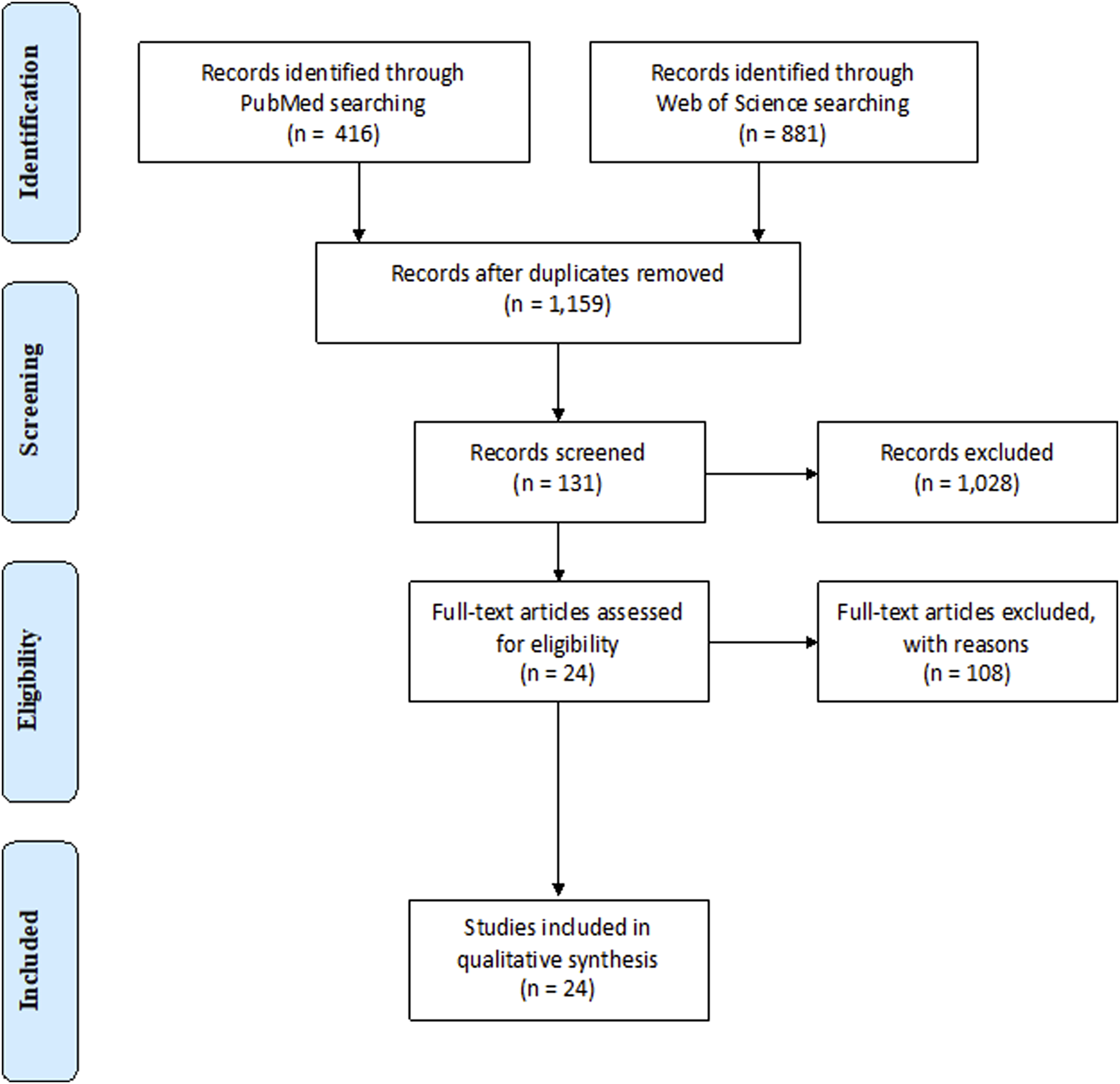
Study Characteristics
General Characteristics
General characteristics for each study are summarized in Supplemental Table 1. Among included studies, two by Viester et al. were found to have the same intervention, but with different outcome measurements.15,27 Two more pairs of studies by Oude Hengel et al.,29,30 and Gram et al.,25,28 applied the same approach. Therefore, the 24 included publications correspond to 21 individual studies. Each of the 24 publications was published between 2003 and 2019, with 20 of them published between 2010 and 2019. In terms of the countries where the 21 studies were conducted, 8 took place in the Netherlands, 8 in the US, 2 in Denmark, 1 in China, 1 in Australia, and 1 in the UK.
Intervention Method
The methods by which the interventions were implemented included personnel-dependent methods such as training, counseling, education, coaching, discussion and inspection, and also non-personnel-dependent methods including video, pamphlets, and text messages. Most of the studies targeted construction workers, but a few targeted on-site managers or supervisors. Although some the studies intended to target participants regardless of their sex, due to the fact that gender distribution is highly uneven in the construction industry, many eventually targeted only male workers.
Intervention Aims
The aims and targeted outcomes of each study were categorized according to whether they focused on safety or health (or both). Though safety and health are highly connected, we define safety-related interventions as those seeking to reduce workplace injuries or damages, while health-related interventions target workers’ health including lifestyle changes and chronic disease prevention.
Based on these classification criteria, five studies were categorized as safety-related, covering topics including avoiding chemical and physical hazards associated with construction work like silica dust exposure, noise, ultraviolet radiation, as well as fall prevention and general safety planning. Seventeen studies were health-related, and covered a much broader range of topics. These included modifying lifestyle behaviors, contraceptive use, aerobic capacity, muscle strength, work ability, musculoskeletal pain reduction and also mental health. For lifestyle interventions specifically, research topics included contraception, tobacco cessation, consumption of fruits and vegetables, recreational physical activity, consumption of snacks and sugar-sweetened beverages, sickness absence and work-related vitality. Mental health-related interventions were only studied in three of the included publications, and topics included self-stigma (self-blame, shame, and help-seeking inhibition), work engagement and organizational context (mainly social support from supervisors and the teams). Two studies implemented an integrated intervention with both safety and health components.14,32
Study Designs
There were 19 RCT studies, and among them 9 were cluster RCTs that randomized at company, site or group level, while 5 were pre/post or longitudinal non-randomized studies.
Intervention Content, Dose, and Duration
The duration of interventions could be classified into two groups, one where they lasted minutes or hours and which could be considered as one-time interventions, and the other usually on the scale of weeks, months or even years. Three studies were considered as one-time interventions.23,34,36 The content delivered to control groups was mostly no intervention or usual care. Some of the control groups were given a brief lecture, brochures, and/or handouts, which were considered to have minimal effect on the outcomes as compared to the intervention.18,20,23,28 Milner et al. (2018) adopted waitlist control which gave the control group the same material delivered to the intervention group at the end of the study. 26 Details are listed in Supplemental Table 2.
Outcome Assessment
Outcome assessment can be subjective (e.g., safety knowledge, fruit and vegetable consumption) or objective (e.g., body weight, BMI, heart rate). Subjective outcome data were usually collected through self-reporting using previously validated questionnaires or questionnaires designed by the researchers themselves, while objective measurements were usually assessed using devices, observation records, or diagnoses. Some studies were mixed, with both subjective and objective outcomes. Eight studies included at least one outcome that was measured objectively.15,16,18,19,24,25,27,29
Results of Individual Studies
Among the 24 included studies, 17 reported significant effectiveness of their intervention,13-25,33-36 while 7 found their primary outcome not significantly improved as compared to the control group or pre-intervention stage.26-32 Details are listed in Supplemental Table 3.
All seven studies with non-significant improvement in their primary outcome were occupational health-related studies. Among them, three examined mental health outcomes and 5 targeted work ability or muscle strength. All five studies related to occupational safety reported significant results. Potential reasons for lack of effectiveness that study authors mentioned in their reflections included the ceiling effect (limited room left for improvement due to inappropriate baseline outcomes), insufficient intervention exposure (“dose”) and duration, inadequate outcome measurement, unresolved external variables, contamination, insufficient statistical power, additional stress exerted by the interventions, key parties not being involved in interventions, and failing to adopt MLIs. Further explanation of these reasons will be illustrated in the discussion section.
Risk of Bias Within Studies
Two characteristics of construction workers that may potentially introduce bias to intervention studies are that they (1) sometimes keep moving from site to site, even on a daily basis; and (2) work together as a team. Mobility is more likely as the duration of interventions get longer, which introduces contamination into the intervention or control group or causes loss to follow-up.29,30 On the other hand, workers working together as a team can influence each other’s behavior, which might also introduce contamination if randomization took place at the individual level.27,36 This is one reason why a cluster RCT design is preferable in order to minimize contamination bias. However, the number of clusters needs to be sufficient to avoid imperfect randomization or heterogeneity of baseline characteristics of participants between the intervention group and the control group. We found that baseline differences between sites did not seem to decrease as the site number increases, which means a study with 20 sites might still be susceptible to imperfect randomization. Based on an understanding of the local construction industry, Sparer et al. assumed that there was more variability between sites of different contractors than within sites of the same contractor. 33 Therefore, the researcher paired two sites together within the same contractor if they were of similar size and trade make-up and block randomized within this pair.
In the context of a safety and health intervention for construction workers, it is not feasible to blind participants. However, blinding of the outcome, from the perspective of both investigators and participants, is feasible and crucial in this setting in order to avoid bias. The adoption of self-reported outcome measurements might introduce bias due to socially desirable responses since the unblinded participants, due to their higher involvement in the intervention, could have a tendency to report improved outcomes in order to meet the expectations of the researcher. Another way in which subjectivity affects outcome assessments occurred in Oude Hengel’s study, 24 where participants might have felt sensitive about filling out questionnaires related to work ability.
There are two ways to blind outcomes, by either selecting objective measures of the outcomes, or blinding those who are evaluating the outcomes so that they do not know whether the individual received the intervention or not. Outcome measurements through external observation can overcome biases caused by self-reporting. For example, Deurssen et al. assessed the use of a silica dust protection device via external observation. 19 However, observers need to be blinded and the result may still be biased if workers are aware they are being observed, as in the Hawthorne effect. 37 Brandt et al. used technical measurements to quantify the workload rather than relying on self-reports or observations. 23 Viester et al., Groeneveld et al. and Gram et al. used laboratory tests for objective parameters such as blood pressure, blood cholesterol, and BMI.15,16,25 For non-randomized studies, a single-arm design without the use a control group was considered an important issue that may influence the validity of the study. The research by Dian et al. and the investigation by Marín and Roelofs failed to set up a control group in their study designs.20,34 Moreover, an absence of randomization is more likely to result in lack of balance in participants’ baseline characteristics, as found in the study by de Boer et al. 31
Discussion
This review provided a comprehensive evaluation of the effects of different kinds of interventions aiming to promote different aspects of occupational safety and health promotion for construction workers. Results showed that most of the interventions tested had a positive effect on the participants.17 out of the 24 studies (70.8%) showed statistical significance in the intervention effect. Some important lessons can be drawn from the results of our scoping review.
First, the complementarity principle suggests that in order to motivate individuals to take up a behavior in one domain (e.g., stopping smoking), it may be necessary to intervene simultaneously in another domain (e.g., mitigating chemical hazards in the workplace). 8 That is, when a risk from one source is reduced, the marginal benefit of reducing other sources of risk is simultaneously increased. This theory may explain why many health promotion interventions in blue collar workplaces often fail. The reason is because workers may perceive a negligible benefit from avoiding one health risk (e.g. by stopping smoking) when they continue to be exposed to the same carcinogens in their workplace.
Hence, without addressing safety issues in the workplace through actions by management, workers may feel disempowered to engage in health promotion efforts through behavioral changes.38,39 Therefore, occupational safety interventions need to be delivered in an integrated manner with health promotion interventions in order to maximize impact. If safety interventions are unaccompanied by health promotion interventions, the threat of chronic disease is overlooked, and this poses a greater burden on health care costs and lost productivity in addition to the risk of occupational injuries. Thus, it is highly recommended that future interventions combine both health promotion and occupational safety. 11 The following are the main findings from this scoping review:
Need for Multi-Level Intervention Designs
The importance of MLIs has long been demonstrated in public health. Among the included studies, Sorensen et al. suggested that lifestyle interventions like smoking cessation that promote the health of construction workers should be integrated with workplace safety interventions. 21 Also, Viester et al. suggested that exercise or training interventions would have been more effective if combined with components addressing environmental and organizational issues. 27 Specifically, health and lifestyle promotion could be combined with workload and working condition improvements; physical risk reduction could be combined with psychosocial environmental change through enhancing social support. 27 Nevertheless, only two studies (Peter et al. and Hammer et al.) in this review actually applied this consideration in their intervention design.
There has been limited use of MLIs, mainly because of the difficulty of operationalization (e.g., cost and feasibility, among others). 40 This barrier can be overcome by using parsimonious models focusing on several important factors based on a review of those which most affect targets. 40 For example, the WellWorks Study by Sorensen et al. demonstrates the importance of MLIs held in the jewelry industry (provision of smoking cessation at the individual level, and managerial interventions at the worksite level). Although this is an example from a different industry, since targets (e.g., blue collar workers) are similar, it provides learnings that the construction industry can consider.
Key Stakeholders Were Not Involved in the Design of Interventions
Previous studies demonstrated that interventions involving multiple stakeholders work better in reducing the use of disability pensions and sick leave.41,42 In the study by Oude Hengel et al., the middle-management of the construction company and supervisors were not engaged in the intervention. Involving them in the intervention could give autonomy to workers so that they can make behavioral changes, including taking additional rest breaks to alleviate musculoskeletal symptoms. For outcomes such as social support and work engagement, it would be even more difficult for the intervention to take effect if supervisors were not receiving the intervention content. 30 The study by de Boer et al. adopted the Swedish Galaxen model, which involved representatives from the employers, trade union, regional employment office, and an assigned personal case manager to the employee. 31 The structure of the construction industry poses a challenge to identifying relevant stakeholders, as workers tend to be from different companies (e.g., subcontractors or vendors supplying the general contractors). Therefore, this kind of structural issue may exacerbate the difficulty of seeking the input of all stakeholders.
Avoiding the Challenge of Contamination (Through Cluster Randomization)
Due to the fluidity of participants’ worksites and the phenomenon of imitation or sharing between participants in the intervention group and control group, intervention content often cannot be concealed. In particular, construction workers tend to work at different construction sites on a daily basis, which makes it challenging to rule out contamination effects. This is the reason why cluster randomization is usually preferred over randomization at the individual level.
Determining the Correct “Dose” of Treatment
In terms of intervention design, insufficient frequency, duration, intensity, follow-up times, and imperfect implementation were common causes mentioned in the discussion sections of the seven studies with insignificant intervention effects.26-31 In the study by Oude Hengel et al., 30 the physical therapist did not deliver all training sessions individually and trainers did not always involve supervisors in the training session. Gram et al. used a mix of aerobic and muscle strength training interventions, which might be a reason why they did not have the same positive effect as previously reported in separate interventions. 28 In another study by Oude Hengel et al., 29 the intervention with the aim of improving work ability failed because the concept of work ability was too broad, and the “dose” might have been insufficient to result in a significant effect. The intervention content in the study by Milner et al.’s intervention content was six text messages delivered across six weeks, which was also thought to be weak in intensity. 26
From the perspective of the participants, low compliance (or adherence, fidelity) and low satisfaction were commonly found in these studies.26,27,29,30 In Viester’s study, although the majority of workers had done the exercises, only a few exercised regularly while strictly following the intervention content. 27 Also, a proportion of the program was tailored to the participant’s need, based on their self-selected physical activity goal. However, allowing flexibility in the treatment might have resulted in insufficient “dosage”, resulting in non-significant reduction in musculoskeletal symptoms. 27 To account for these issues, future research could adopt techniques to quantify participants’ individual intervention exposures, which will increase the precision of the exposure assessment and achieve a better understanding of the optimal “dosage” of interventions. Such an approach could have been easily integrated into the study by Milner et al., since the intervention content was delivered through smart phones. 26 Also, as proposed in the study by Oude Hengel et al., 29 knowing what specific actions from the intervention content were taken by participants will produce further knowledge on the optimal type, duration, and intensity of the interventions.
Inadequate Outcome Measurement
Since many questionnaires for outcome assessment were designed for patients in a clinical setting, they might not have been suitable for measuring health outcomes for population studies targeting construction workers.26,31 Optimally, the target population that the questionnaire is designed for needs to match the actual study population. Otherwise, validation is recommended if no suitable metric is available.
Also, selected scales may fail to detect intended or pertinent aspects of outcomes. Milner et al. reported that self-stigma is a complex process and their research used the Self-Stigma of Depression Scale (SSDS), which was designed for measuring self-blame, shame, and help-seeking inhibition. However, it may be that perceived stigma and stereotype endorsement are particularly important to investigate, since they were included in other scales as crucial components. 26 Hammer et al. stated that the outcomes measured were not comprehensive enough to assess all that could be measured about team effectiveness and supervisor support. 32 Qualitative methods could have been used to discover more about the boundary conditions of intervention effects beyond the selected quantitative measures. 32 It is encouraged to make a comparison of the different highlights of questionnaires to find the one that best matches the underlying theory.
Besides the tools used for outcome assessments, the follow-up time when the assessment takes place also influences the observed results of intervention’s effectiveness. Viester et al. noted that although their intervention failed in the short term, it could have had long-run effects by lowering systemic and metabolic risk factors. 27 An adequate time interval should be set between the end of intervention and the outcome assessment, depending on the outcome.
In addition, various techniques can be adopted to increase the accuracy and precision of outcome measurement. External observation is a good choice if the observers are blinded. Using objective measures can also reduce bias in measurement. These include biomarkers in blood or urine or data from health records, 21 real-time recording of the use of hearing protection devices, 35 and sick leave records.27,29 However, it is worth noting that one limitation of records for sick leave is that their causes are usually not specified (in the data for total sickness absence. Therefore, using sick leave data as a proxy of health status or the outcome of interests in these studies like musculoskeletal pain may introduce noise.
Ceiling Effect (Inappropriate Baseline Outcomes)
In most of the studies targeting improvement in health or safety outcomes, a high level of health and safety at baseline is a major reason explaining the null effect of the intervention. A higher pre-intervention level of health or safety means the room left for improvement is limited (i.e., a ceiling effect). Consequently, the likelihood of observing a significant difference in changes in outcomes decreases.27,28 Also, due to the high intensity of workload in the construction industry, workers with severe musculoskeletal symptoms were less likely to remain in the workforce for longer periods of time (a healthy worker effect), which was thought to be a cause of the reason that most participants reported only modest pain. 28
Conversely, de Boer’s et al. included only workers at high risk of developing a work disability, but the study still resulted in insignificant intervention effects. 31 It was thought that the threshold level for inclusion might have been set too high, i.e., workers who already showed advanced stages of symptoms. 31
Unresolved External Variables
External socioeconomic context, such as an economic recession, were thought to exacerbate a worker’s stress and workload in the study by Viester et al. and Oude Hengel et al.’s research.27,30 In such a situation, participants could only focus on behaviors that directly and obviously contributed to productivity, and were less committed to other interventions, due to fear of job loss. Conversely, positive support at the management level may facilitate the implementation of the intervention. For example, in the study by Peter et al., a major contributor to the effectiveness of the intervention was that it aligned with companies’ current practices on the worksite and could be easily integrated into the companies’ business structures. 14 Furthermore, factors including leadership, high mental work demands, lack of autonomy, poor physical work environment, and high physical workload were all found to be associated with work ability but were not accounted for in Gram et al.’s study. 28 Viester et al. also noted that not all sickness absence can be explained by illness. Socioeconomic factors, organizational features, job content and attitudes towards work are all associated with sickness absence, which may not be reflected in sickness records. 27
There are some limitations to this review. One is that the databases used to search for articles included only PubMed and Web of Science. We saw an overlap in the records at the first level of screening, but this overlap was a rather small portion, indicating that some other studies satisfying the search criteria might have been overlooked and could have been found through different databases. Another limitation is that the language of the search was only English, so there may have been other relevant articles that were not included. In addition, due to the variety of topics and aims that the interventions covered, it was not possible to perform a quantitative analysis. Nevertheless, this review could serve as a good reference for future intervention studies in this field, as well as for recommendations to current practices in the construction industry.
Conclusions
A variety of effective interventions were examined, covering different aspects of occupational safety and health for construction workers. Future research should place more effort on interventions aimed at improving both occupational safety and health outcomes in an integrated manner, with environmental interventions that accompany behavioral interventions at the individual level. Besides adopting a MLI design, additional effort is also needed to ensure the involvement of relevant stakeholders in designing the intervention, avoiding contamination effects (through cluster randomization), optimizing the “dosage” of intervention, and improving measurement of outcomes. Construction is a high-risk industry in terms of occupational safety and health issues. Various interventions have been implemented, and while some of the intervention effects were significant, others were not. This review comprehensively examines interventions which sought to improve the occupational safety and/or health of construction workers. Factors that explain the ineffectiveness of interventions were also summarized. This review provides a reference for future research and practice to improve their intervention design and implementation process. Multi-level interventions that integrate occupational safety and health are recommended.SO WHAT?
What is Already Known on this Topic?
What Does this Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - A Scoping Review of Interventions to Improve Occupational Safety and Health of Construction Workers
Supplemental Material for A Scoping Review of Interventions to Improve Occupational Safety and Health of Construction Workers by Hana Hayashi, Yue Li, David D. Sussman, Sakurako Okuzono, Kasisomayajula Viswanath and Ichiro Kawachi in American Journal of Health Promotion
Footnotes
Acknowledgements
We would like to thank Ryoichi Togashi, program director, office of chief technology officer of Komatsu Ltd., for his great support throughout the project and useful discussions. The authors are also grateful to Yasumasa Yamamoto for collaboration on the early stages of this work. We also thank Akihiro Shimoda to help manage the entire project.
Author Contributions
HH, YL and KI contributed to the concept or design of the study. All authors contributed to the acquisition, analysis, or interpretation of data for the work. HH, YL, and DS drafted the manuscript. DS, SO, KV and KI critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of the work, thus ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Komatsu Ltd. [grant number N/A].
Correction (August 2023)
This article was corrected to update the placeholder symbols “## and $$” with the authors’ initials “HH and YL” respectively on page 3, under section “Data Extraction and Data Synthesis”.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.