
Abstract
Purpose
This study assesses the association between SUD, economic hardship, gender, and related risk and protective factors on serious psychological distress (SPD) during the COVID-19 pandemic.
Design
Quantitative cross-sectional design.
Setting
National Survey on Drug Use and Health (NSDUH).
Sample
Data were from the NSDUH (2020) N = 25,746, representing 238,677,123 US adults, who identified as 18 or older and either male or female.
Measures
SPD measured as scoring a 13 or more on the Kessler (K6) distress scale. SUDs were determined using DSM5 criteria. Sociodemographic and socioeconomic variables included in analyses.
Analysis
Logistic regressions evaluated the association between gender, protective, and risk factors on SPD.
Results
After controlling for sociodemographic and related factors of SPD, having a SUD was the strongest correlate of SPD. Other significant correlates of SPD included female gender and an income level at or below the federal poverty threshold. Gender stratified regressions illustrated that religiosity, self-identifying as Black, and high levels of education were protective against SPD for women but not men. Poverty level was more associated with SPD for women than men.
Conclusion
In the United States, individuals with SUDs were nearly four times more likely to report SPD than those without SUDs, controlling for economic hardship and markers of social support during 2020. Effective social interventions to reduce SPD among individuals with SUDs are needed.
Keywords
Introduction
The COVID-19 pandemic significantly impacted many individuals’ physical and mental health, evidenced by increasing substance use and overdose deaths.1,2 In addition, stress associated with home, work, finances, fear, anxiety, and loss increased during the pandemic.1,3,4 These psychological factors have been linked with substance use initiation during the pandemic for those with no prior substance use history 3 and increasing use or relapse among those who used drugs or achieved abstinence before the pandemic,2,4 which is attributed to maladaptive coping mechanisms to manage the pandemic’s psychological impact. 5 The increase in emotional distress and substance use have increased the risk for COVID-19 among those with substance use disorders (SUDs). 6 The increased risk of physical and mental health issues is complicated by decreased access to health care during the pandemic. 2 The supply of licit and illicit substances was disrupted due to shutdowns and barriers in regulation and manufacturing.2,7 Additionally, access to harm reduction programs, such as needle exchange programs and programs that distribute opioid overdose reversal drugs, was limited.2,8 Other substance use treatment programs were limited in the services provided during the pandemic due to reduced revenue and resources. 9
Serious psychological distress (SPD), a frequent impairment in functioning due to multiple mental health symptoms, 10 is particularly important to evaluate during the pandemic. Before the COVID-19 pandemic, experiencing SPD was associated with behavioral and social determinants of health, 11 lower quality of life, chronic medical conditions, 12 and mortality. 13 Gender differences and social factors are also salient factors in the understanding and reporting of SPD 14 and as it relates to COVID-19. 15 There is evidence that men and women are impacted by the COVID-19 pandemic differently, with women reporting less severe short-term symptoms associated with COVID-19 than men, but greater longer-term complications, including depression. 16
Due to the closure of schools, childcare facilities, and female-dominated industries during the pandemic, childcare challenges and financial hardship greatly impacted working mothers.17,18 These stressors may be especially pronounced among women from minoritized racial/ethnic groups. 19 Individuals with intersecting marginalized identities may also be at elevated risk for substance use and reduced access to treatment.20,21 Stressful life events and SPD increase the odds of the onset or continuation of alcohol use with a much greater effect for women than for men.22,23 Substance use during the COVID-19 pandemic has also been associated with experiencing a lack of identity with a religious community, which may impact women more than men.6,24 The severity of COVID-19 symptoms did not predict symptoms of depression; social support was most important in reducing symptoms of depression, and symptoms of depression were more frequently reported by women. 25 This suggests factors, such as support, isolation, and the impact of gender, may influence women’s substance use and psychological distress during the COVID-19 pandemic, indicating a need for further research in this area.
Methods
Design
This study assessed the association between SUD, economic hardship, gender, and related risk and protective factors on SPD during the COVID-19 pandemic. Data for this study were derived from the 2020 National Survey on Drug Use and Health (NSDUH), a nationally representative cross-sectional survey on drug use, mental health, and other health issues administered by the Substance Abuse and Mental Health Services Administration (SAMHSA). 26 All items on the NSDUH are measured via a self-report survey.
Sample
Our sample was limited to individuals 18 or older who identified as either male or female, N = 25,746. We restrict our study to NSDUH 2020 as methodological differences in data collection render pre- and post-pandemic comparisons inappropriate. 27 This study used publicly available de-identified data and therefore no ethical review was required.
Measures
Serious Psychological Distress
The Kessler-6 distress scale (K6) was used to define SPD. This scale assessed past 30-day feelings of nervousness, hopelessness, restlessness, depression, worthlessness, and everything feeling like an effort. 28 Responses were recorded on a 5-point Likert scale (all of the time, most of the time, some of the time, a little of the time, none of the time), with “all of the time” coded as 4 and “none of the time” coded as 0. A combined score of 13 or above in response to these six items was categorized by the NSDUH as SPD. Example item measuring hopelessness, “During the past 30 days, how often did you feel hopeless?”. A study evaluating the psychometrics of the K6 for individuals with mental health diagnoses reported good reliability (Cronbach’s α = 0.87 for panic disorder and G.A.D. 0.86 for bipolar disorder schizophrenia) and validity (significant analyses for concurrent and incremental validity). 11
Gender
The 2020 NSDUH instructs the interviewer to “record respondent’s gender” with either “male” or “female” response to obtain gender identity. Responses for gender identity are limited to either male or female. Terms male and female will be used to be consistent when specifically referencing NSDUH data, otherwise the terms women and men will be used when describing gender groups.
Substance Use Disorder
The 2020 NSDUH determined the presence of SUDs based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria. An example of the 11 criteria used is “inability to cut down or stop using [the substance] every time tried or wanted to”. A mild SUD was identified if two or three criteria were met, a moderate SUD if four or five criteria were met, and a severe SUD if six or more criteria were met. Respondents reporting a past year alcohol, marijuana, cocaine, heroin, hallucinogen, inhalant, methamphetamine, pain reliever, tranquilizer, or stimulant use disorder that at least met the threshold of “mild” were included in this study. This study included the presence of a SUD regardless of severity to include all possible individuals experiencing substance use.
Sociodemographic Characteristics
Were included to assess how social differences influenced SPD for individuals during the COVID-19 pandemic. Sociodemographic factors included in this study include age, race/ethnicity (non-Hispanic Black/African American, Asian, Native Hawaiian/Pacific Islander, Native American/Alaskan, White, Mixed or Multiracial, Hispanic/Latino), education level (high school, some college, college or more), household income (at poverty threshold, up to two times poverty threshold, more than two times poverty threshold), employment, criminal justice involvement (CJI), religious importance and involvement, self-help group attendance, and rural or urban community environment (large metro, small metro, non-metro as defined by the Office of Management and Budget). 29
Analysis
Logistic regressions were used to assess correlates of SPD, with adjusted odds ratios and corresponding 95% confidence intervals. Predictors included age, race/ethnicity, education level, household income, employment, criminal justice involvement, religiosity, self-help group attendance, marital status, and rural or urban environment. Gender stratified regressions assessed the role of risk and protective social factors for SPD separately for men and women. Analyses were conducted using S.A.S. 9.4.
Results
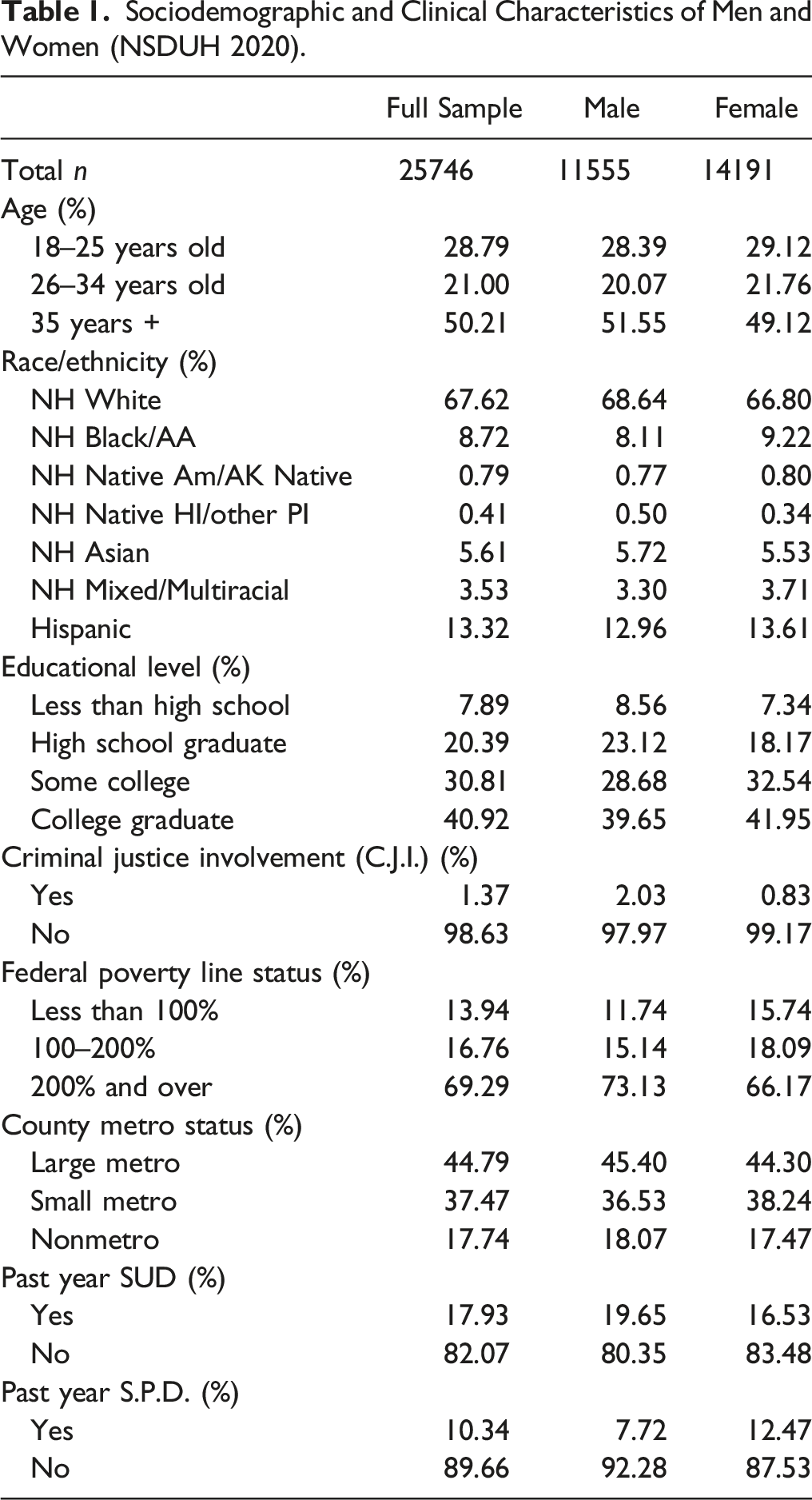
Sociodemographic and Clinical Characteristics of Men and Women (NSDUH 2020).
Logistic Regression Analysis of Predictors of SPD.
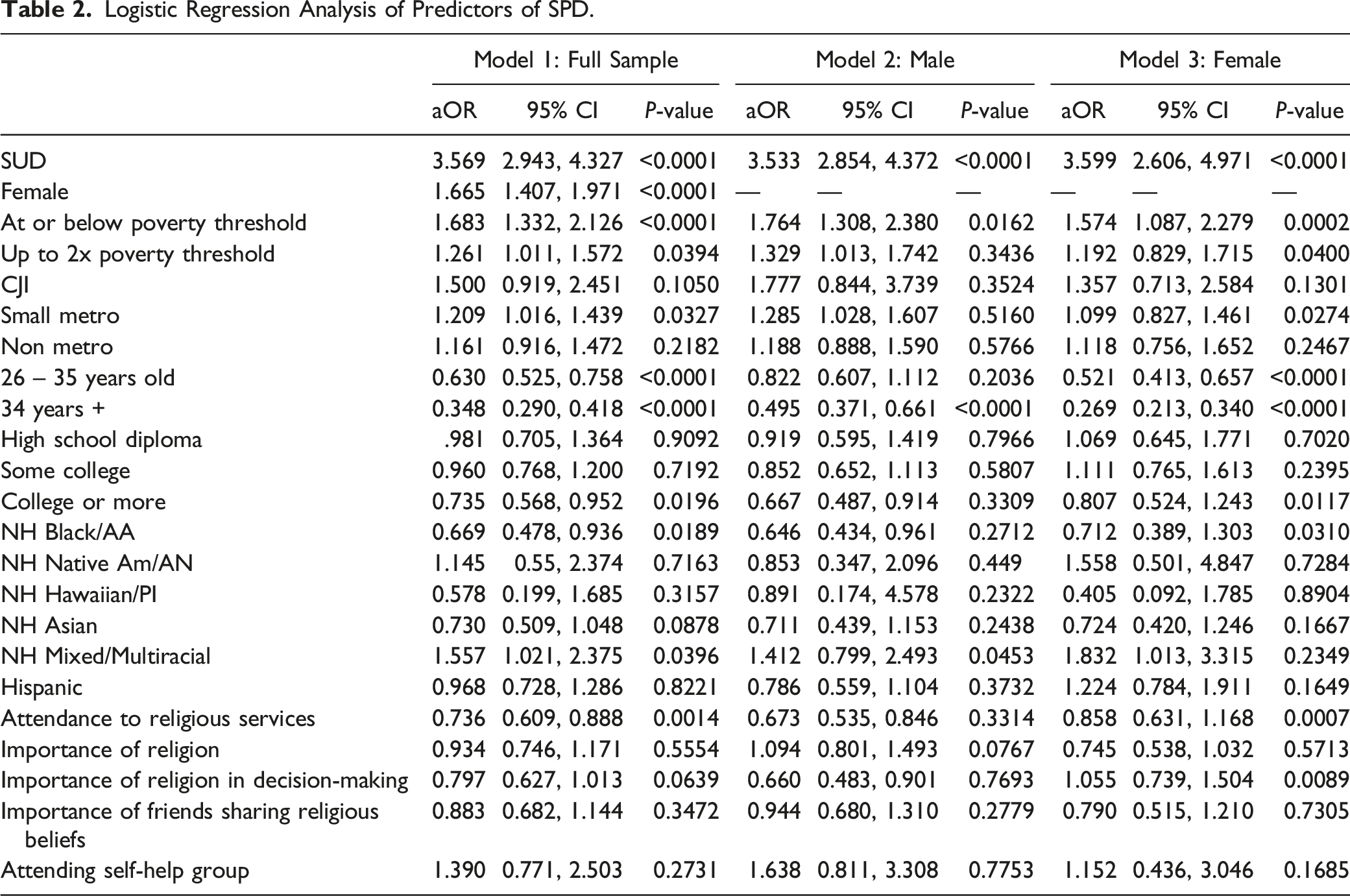
When we examined stratified regressions by gender, we found that some factors were protective against SPD for women but not for men. For women, reporting high levels of religiosity via attendance to religious services (aOR = 0.86, 95% CI = 0.63, 1.17), self-identifying as Black (aOR = 0.71, 95% CI = 0.39, 1.30), and high levels of education (aOR = 0.80, 95% CI = 0.52, 1.24) reduced the likelihood of SPD. While reporting a household income level two times or more above the poverty level was associated with a greater likelihood of experiencing SPD in the full sample, this correlation was only statistically significant for women in the gender stratified models (P = .04 and P = .34 respectively). For men, self-identifying as Mixed or Multiracial was significantly associated with SPD (aOR = 1.41, 95% CI = 0.80, 2.50) as compared with men who self-identified as White, which was not the case for women who identified as Mixed or Multiracial.
Discussion
This study assessed substance use and related correlates of SPD in the pandemic year 2020, particularly delving into gender differences. Our findings suggest that having at least one SUD was the strongest correlate of SPD for both men and women in 2020, even when controlling for sociodemographic and contextual factors. Previous research provides evidence for the significant increase in stressors during the COVID-19 pandemic that may contribute to initiating or increasing substance use or relapsing in substance use recovery.1,2,5,6 Though data cannot be statistically analyzed with previous years’ NSDUH data, our finding that 10.34% of individuals reported experiencing SPD within the past year is consistent with a gradual increase in SPD from previous NSDUH data, which was 8.4% in 2018 and 9.7% in 2019.
Alongside SUDs, self-identifying as female and a family income at or below the poverty threshold increased the likelihood of SPD. These results align with research indicating that financial factors are greatly associated with stress for women. During the COVID-19 pandemic, the increase in families living below poverty thresholds was greater for families with a female householder and no spouse compared to families with a male householder and no spouse. 30 The strength of the association between poverty and SPD was not seen in the male-only analyses.
Our results build on previous research documenting that women with life event stress and SPD are at much greater risk to initiate alcohol use than men.22,23 Studies have also identified that women report poorer psychological adjustment to the stressors of the pandemic, which was related to issues that disproportionately affect women.17,31 Results also indicated a significant association of self-identifying as Multi or Mixed race for men with SPD. Literature has indicated that identifying as biracial may be associated with higher anxiety and depression symptoms. 32
For individuals self-identifying as female, some protective factors were identified. High levels of religiosity and education were associated with lower levels of psychological distress for women only. Religiosity has been identified in previous studies as protective against stress; 33 however, our results suggest a gender difference in the effects. Women who self-identified as Black were less likely to report SPD; however, this was not seen for men who self-identified as Black. One study indicated that Black adults were 72% more likely to report high levels of resilience against mental distress than White adults during 2020, potentially due to the trait-level resilience Black adults may develop in response to experiences of systemic racism. 34
There are limitations to this study. First, due to the nature of the cross-sectional design, causal relationships between independent variables and covariates and SPD cannot be established. Second, the NSDUH data is obtained from participants in the U.S.A., so findings may not be generalizable to populations of other countries. Third, responses of gender were recorded as male or female. Nonbinary and non-gender-conforming individuals were not represented in this study. Fourth, all responses collected by the NSDUH are made by self-report, which may not be comparative to datasets that assess SUD and SPD through clinician assessment. This study does not differentiate between SPD resulting directly from the COVID-19 pandemic, SPD resulting from other stressors, or symptoms of a specific mental illness.
In this study, CJI was not significantly correlated with SPD, deviating from research supporting the link between SPD and involvement with the criminal justice system. 35 NSDUH data measured CJI by current engagement with a parole or probation system and may not have captured the impact of involvement with justice systems. Likewise, educational attainment was not associated with SPD whilst studies on educational attainment and SPD have reported mixed results. 36 The mechanisms through which educational attainment impacts psychological distress may not have been fully assessed in COVID-19 research.
Conclusion
In the United States during the pandemic year of 2020, individuals with SUDs were nearly four times more likely to report SPD than those without SUDs when controlling for economic hardship and markers of social support. Effective social interventions to reduce symptoms of SPD among individuals with SUDs are needed, highlighting considerations for religiosity and financial security for women, as well as and understanding of the intersection between race and gender in experience of SPD. The COVID-19 pandemic increased psychological distress, substance use, and economic challenges for populations across the globe. Our results suggest that in the United States gender may play a role in protective and risk factors for psychological distress, including substance use, income level, religiosity, and racial identity in relation to stressors associated with the COVID-19 pandemic. This study highlights gender differences in substance use, SPD, and the need for individualized and systemic approaches to treatment that consider the impact of gender and race on an individual and their environment. Interventions that address the personal and social factors that serve as risk and protective factors, such as income level and religiosity, are needed to reduce psychological distress among individuals with SUDs. Understanding the role of substance use, gender, race, and other social issues is critical in effectively treating psychological distress.So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this article add?
What are the implications for health promotion practices or research?
Footnotes
Author Contributions
All authors contributed to the study’s design, draft revisions, and final approval. The conception and first draft of the manuscript was written by Joy Gray, and all authors substantially revised the manuscript. Alexis Santos-Lozada and Hannah Apsley performed data analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health grant K01DA051715 (P.I.: A. A. Jones) and National Institute on Drug Abuse T32DA017629 (Trainee: H.B. Apsley).