
Abstract
Purpose
To identify reasons for burnout, characterize the effect of lifestyle medicine (LM) practice on burnout, and assess the risk of burnout in relation to the proportion of LM practice.
Design
Analysis of mixed methods data from a large, cross-sectional survey on LM practice.
Setting
Web-based survey platform.
Participants
Members of an LM medical professional society at the time of survey administration.
Methods
Practitioner members of a medical professional society were recruited to a cross-sectional, online survey. Data were collected on LM practice and experiences with burnout. Free-text data were thematically grouped and counted, and the association of burnout with the proportion of lifestyle-based medical practice was analyzed using logistic regression.
Results
Of 482 respondents, 58% reported currently feeling burned out, 28% used to feel burned out but no longer do, and 90% reported LM had positively impacted their professional satisfaction. Among LM practitioners surveyed, practicing more LM was associated with a 43% decrease (0.569; 95% CI: 0.384, 0.845; P = 0.0051) in the odds of experiencing burnout. Top reasons for positive impact included professional satisfaction, sense of accomplishment, and meaningfulness (44%); improved patient outcomes and patient satisfaction (26%); enjoyment of teaching/coaching and engaging in relationships (22%); and helps me personally: quality of life and stress (22%).
Conclusion
Implementing LM as a greater proportion of medical practice was associated with lower likelihood of burnout among LM practitioners. Results suggest that increased feelings of accomplishment due to improved patient outcomes and reduced depersonalization contribute to reduced burnout.
Keywords
Background
Burnout among healthcare practitioners has been well-documented.1–3 Prior to the COVID-19 pandemic, an estimated one in three physicians was experiencing burnout;1–3 by 2022, this increased to 63%. 1 Practitioner well-being has been studied using the Maslach Burnout questionnaire which evaluates burnout based on three measures: emotional exhaustion, depersonalization, and reduced sense of personal accomplishment.4–6 Stress from workload and work environment are most associated with burnout.7-12 Women8,13 and younger practitioners with less developed coping capabilities face greater burnout,7,13,14 and balancing heavy work and personal life is reported as a challenge. 13
Attempted solutions to practitioner burnout have typically addressed organizational factors or personal behaviors.11,15-18 Organizational or systemic solutions focus on work procedures to reduce hours and workload, reduce time spent on completing medical and insurance records, increase co-worker and administrative support, and improve control of job or career. 19 Individual solutions target job skills training, stress management, self-care, relationships, and depression.20,21 Such solutions have resulted in modest improvements in burnout. 22 Organizational and systemic interventions may not address the root causes of burnout related to a reduced sense of success and satisfaction in helping patients overcome disease.10,11,22,23 Research indicates that lack of work satisfaction is a primary cause of burnout.7,10,24
Lifestyle medicine (LM) is an emerging field of medicine in which practitioners use evidence-based lifestyle interventions, incorporating behavioral medicine across six domains of health behavior, a whole-food, plant-predominant eating pattern, physical activity, restorative sleep, stress management, risky substance avoidance, and positive social connections, to treat chronic conditions. However, barriers to LM practice exist, with the foremost being that an LM approach is not taught as a part of conventional medical training. Thus, medical practitioners often need to seek out training in LM on their own and/or in the form of continuing medical education. Additionally, a previous analysis of the survey data presented here found that LM treatment is poorly aligned with current reimbursement pathways. 25 Thus, while some LM practitioners exclusively practice LM, others incorporate LM into their practice to varying degrees. Those able to integrate a greater degree of LM bring more health behavior education and behavior change into their patient encounters, which may occur in the form of one-on-one counseling during an appointment, referral to a dietitian or health coach, or deployment of shared medical appointments (SMAs) for health education. These kinds of interventions to support healthy lifestyle changes are compatible with primary care and specialty practices in multiple specialties such as cardiology or endocrinology. Practitioners of LM can include physicians (MD, DO), nurses, advance practice nurses, dietitians, and physical and occupational therapists. Membership of the medical professional society surveyed in this study is composed of slightly more than half MD/DOs, with the remainder of other members being clinicians and other health professionals. Rapid improvements in patient health compared to non-LM practitioners, including cardiometabolic improvements, 26 diabetes remission, 27 weight loss 28 and reductions or cessation of need for medications are well-documented. 29 Some have speculated about the potential of LM to address burnout by supporting self-care of practitioners;30-32 however, the potential impact of improved patient outcomes on burnout and professional satisfaction has not been evaluated.
Survey Objectives
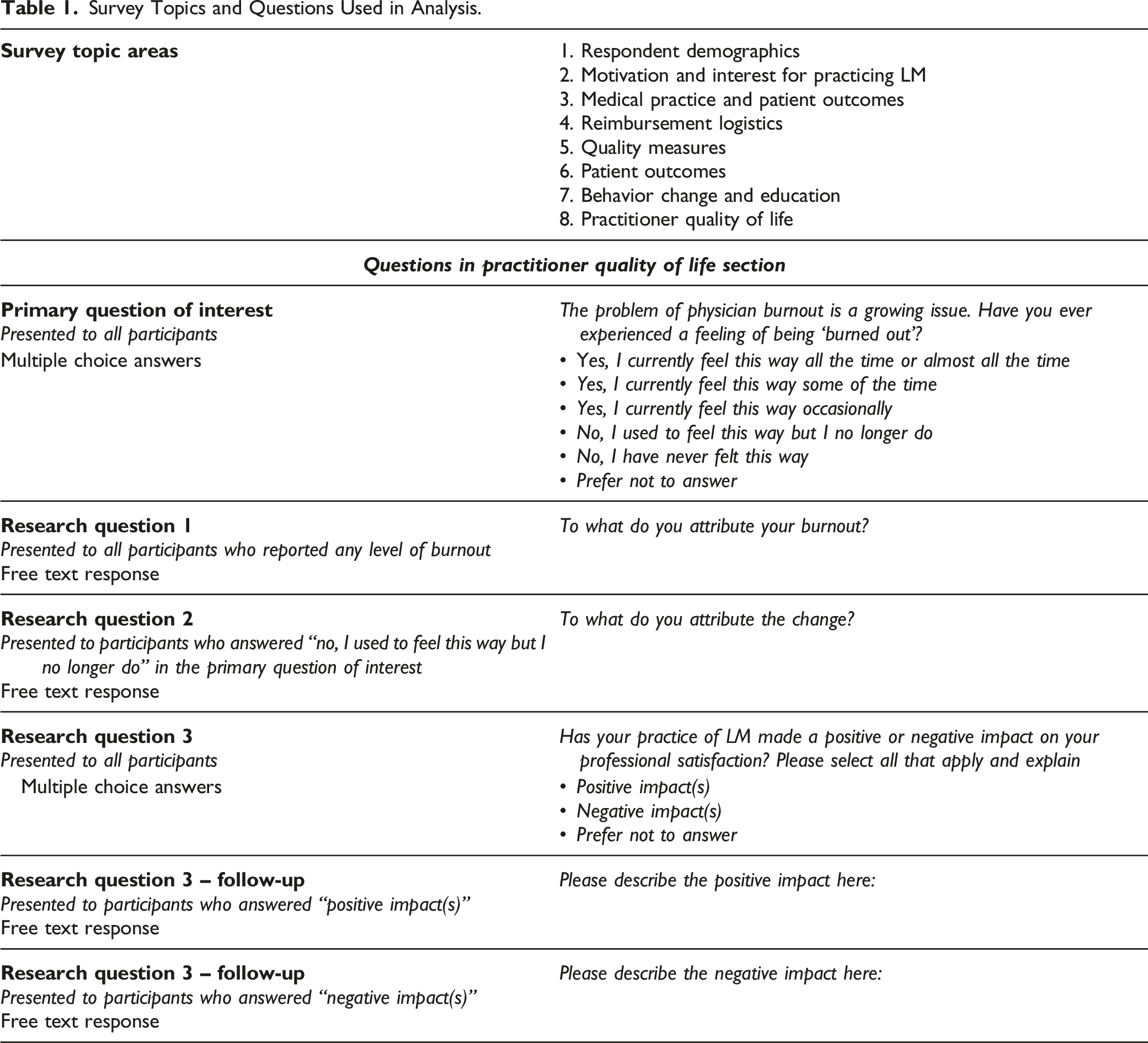
The overall objective of the survey was to characterize the professional experiences of LM practitioners with respect to motivation, practice, and barriers/facilitators to incorporating LM into their treatment. This study uses data collected as part of a large, cross-sectional survey aimed at examining LM practice, including practitioner quality of life and, subsequently, burnout among LM practitioners. Specifically, we address the following research questions: 1. Is the degree of LM practice quantitatively associated with reduced burnout? 2. Which components of medical practice are perceived by LM practitioners as contributing to burnout? 3. How do LM practitioners describe experiences with reductions in burnout and to what do they attribute the change? 4. How do LM practitioners perceive the impact of LM practice on their professional satisfaction?
Participants
In 2019, the American College of Lifestyle Medicine conducted an online, closed, cross-sectional survey of LM practitioners using a total population sampling frame, defined by their active membership status in the organization at the time of survey administration (N = 3182 surveys distributed). No remuneration was offered, though participants who completed the survey were entered into a drawing for a complimentary registration to a related medical professional conference.
This study was reviewed by the Institutional Review Board (IRB) of the University of New England, and informed consent was obtained from survey participants.
Design
The survey was iteratively designed using a collaborative process, incorporating input from key staff and members of the medical professional society first and then utilizing a pilot test to assess respondent burden and make revisions prior to administration. A full explanation of survey development and administration using the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) is available in Supplemental Table S1. 33
Survey Topics and Questions Used in Analysis.
Methods
Quantitative analysis was performed using SAS software, version 9.4 (SAS System for Windows, SAS Institute Inc, 2013, Cary, NC, USA). Descriptive statistics were generated to describe the sample, including medians and interquartile ranges for continuous variables and percentages for categorical variables. To address research question 1, crude and adjusted logistic regression models (total n = 439; n = 43 missing due to missing values) were performed to assess the likelihood of reporting any level of burnout by practitioners who reported that a greater proportion of their practice is LM [all (n = 127) or most (n = 131) is LM] as compared to practitioners reporting less or none of their practice is LM [ half (n = 46), some (n = 145), or none (n = 10) is LM]. Responses of prefer not to answer were removed from this analysis. To maximize the sample size for each group of the outcome variable, a binary variable was created to compare no burnout vs any burnout [never (n = 43) or no longer burned out (n = 136) vs currently burned out all or almost all (n = 51), some of the time (n = 100), or occasionally (n = 125)].
Multicollinearity was checked using simple linear regression. Age, years in practice, and length of time practicing LM were highly collinear with the exposure of interest while gender was found to be highly collinear with the primary covariate, physician status. The model was adjusted for physician status (binary; physician (n = 307) vs non-physician (n = 174) with n = 1 missing). Additional adjustment for gender did not attenuate the association between the proportion of medical practice that is LM and burnout (data not shown). To assess the possibility that the proportion of medical practice that is LM was a proxy for age or years in practice, mean values of these continuous variables were calculated for all original categories of the proportion of medical practice that is LM, and results did not suggest meaningful differences, thus, statistical tests were not conducted (data not shown).
To address research questions 2–4, free-text data were reviewed and thematically coded by a single researcher who reviewed and collapsed codes to achieve a parsimonious category set with no less than 5% of responses in a single category (KP). Most responses were assigned more than one code. Data were reviewed by the same researcher (KP) and two additional researchers (MK and KS) to discuss final coding and achieve consensus. Key quotes were extracted to illustrate consistent themes.
Results
Respondents
Of n = 3182 medical professional society members emailed an invitation to participate, n = 1271 began the survey. A total of n = 857 remained after excluding the following: those who completed the survey outside of the US, were not age 18 yrs or older, did not report being a healthcare practitioner, and declined to participate. After further restricting to those who finished the survey and answered the last required question, a total of n = 482 were included in this analysis.
Characteristics of Lifestyle Medicine Practitioner Sample, N = 482.
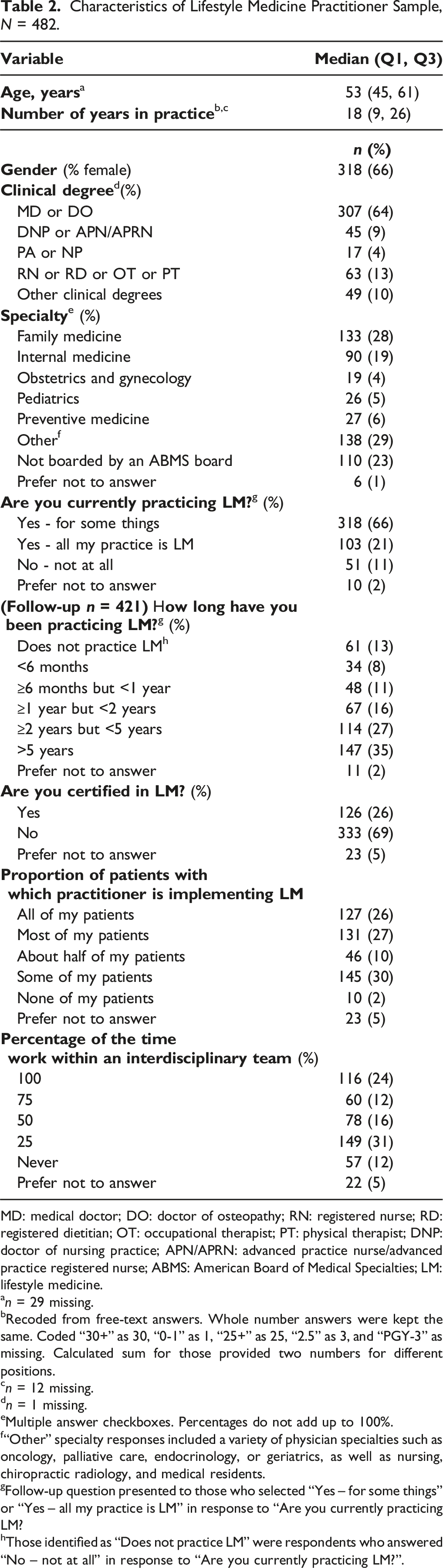
MD: medical doctor; DO: doctor of osteopathy; RN: registered nurse; RD: registered dietitian; OT: occupational therapist; PT: physical therapist; DNP: doctor of nursing practice; APN/APRN: advanced practice nurse/advanced practice registered nurse; ABMS: American Board of Medical Specialties; LM: lifestyle medicine.
an = 29 missing.
bRecoded from free-text answers. Whole number answers were kept the same. Coded “30+” as 30, “0-1” as 1, “25+” as 25, “2.5” as 3, and “PGY-3” as missing. Calculated sum for those provided two numbers for different positions.
cn = 12 missing.
dn = 1 missing.
eMultiple answer checkboxes. Percentages do not add up to 100%.
f“Other” specialty responses included a variety of physician specialties such as oncology, palliative care, endocrinology, or geriatrics, as well as nursing, chiropractic radiology, and medical residents.
gFollow-up question presented to those who selected “Yes – for some things” or “Yes – all my practice is LM” in response to “Are you currently practicing LM?
hThose identified as “Does not practice LM” were respondents who answered “No – not at all” in response to “Are you currently practicing LM?”.
Association of Degree of LM Practice With Experience of Less Burnout
Association of Reporting Less Burnout With Proportion of Medical Practice That Is Lifestyle Medicine.
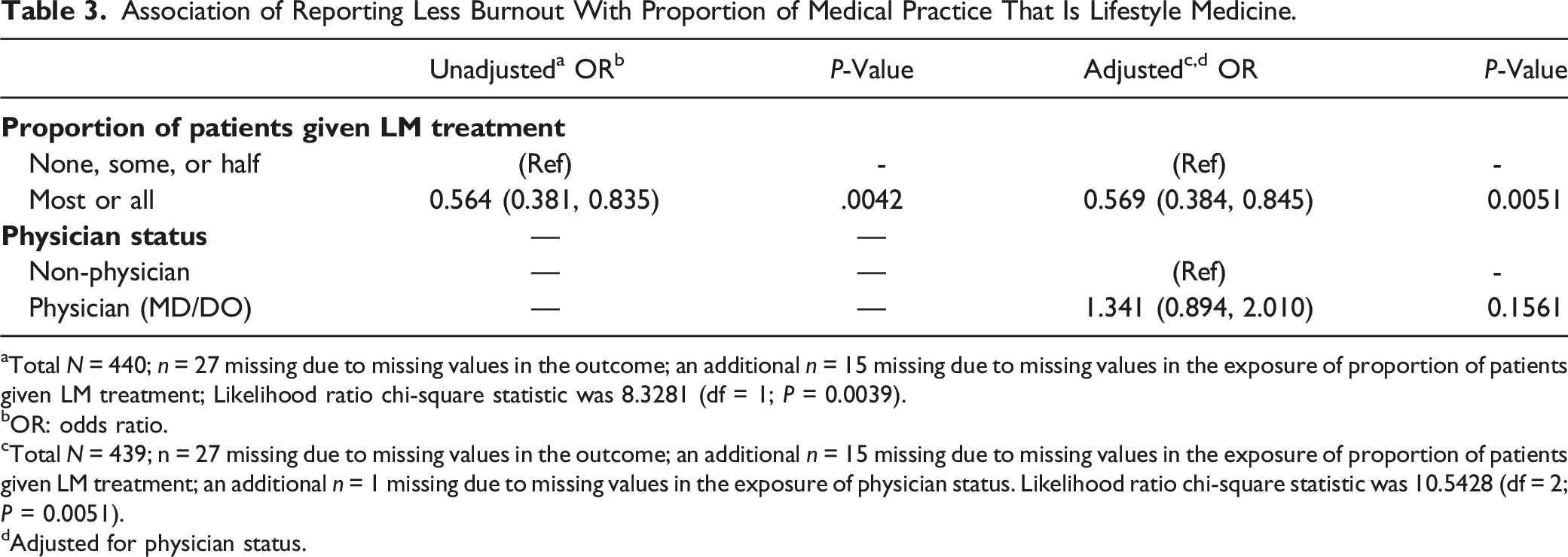
aTotal N = 440; n = 27 missing due to missing values in the outcome; an additional n = 15 missing due to missing values in the exposure of proportion of patients given LM treatment; Likelihood ratio chi-square statistic was 8.3281 (df = 1; P = 0.0039).
bOR: odds ratio.
cTotal N = 439; n = 27 missing due to missing values in the outcome; an additional n = 15 missing due to missing values in the exposure of proportion of patients given LM treatment; an additional n = 1 missing due to missing values in the exposure of physician status. Likelihood ratio chi-square statistic was 10.5428 (df = 2; P = 0.0051).
dAdjusted for physician status.
Self-Reported Practitioner Experiences With Burnout in the Context of Medical Practice (N = 482).
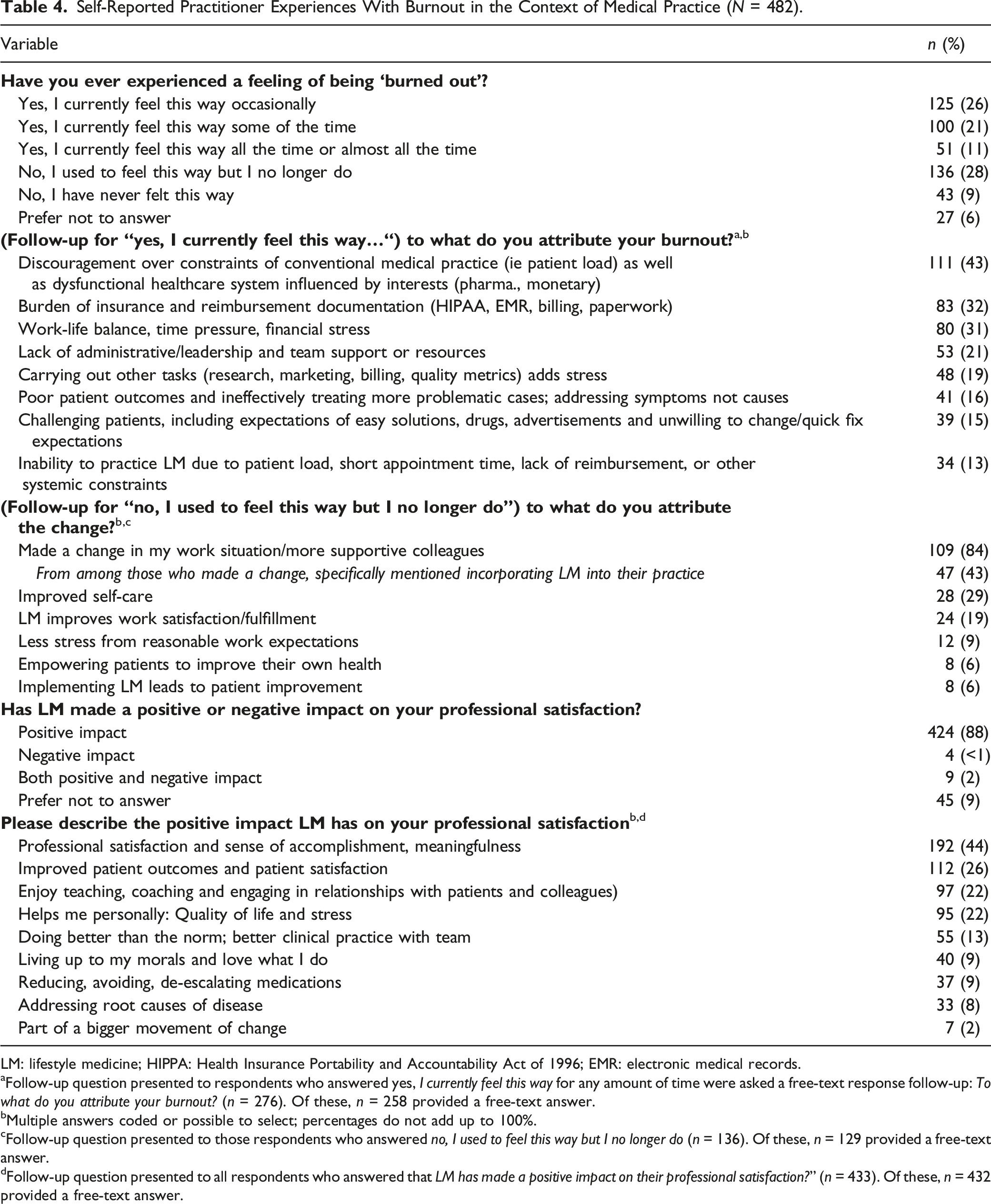
LM: lifestyle medicine; HIPPA: Health Insurance Portability and Accountability Act of 1996; EMR: electronic medical records.
aFollow-up question presented to respondents who answered yes, I currently feel this way for any amount of time were asked a free-text response follow-up: To what do you attribute your burnout? (n = 276). Of these, n = 258 provided a free-text answer.
bMultiple answers coded or possible to select; percentages do not add up to 100%.
cFollow-up question presented to those respondents who answered no, I used to feel this way but I no longer do (n = 136). Of these, n = 129 provided a free-text answer.
dFollow-up question presented to all respondents who answered that LM has made a positive impact on their professional satisfaction?” (n = 433). Of these, n = 432 provided a free-text answer.
Components of Medical Practice Perceived by LM Practitioners to Be Contributing to Burnout (n = 276)
Among those who reported any of the three levels of burnout (n = 276), the top-reported reason (43%) reflected discouragement over the constraints of conventional medical practice, such as overwhelming patient load as well as a feeling that the medical system itself is ineffective and/or dysfunctional: “A big part of it is our disease based/pharmaceutical-driven medical system with its emphasis on production, not helping patients; did not really mesh with my philosophy of medical care,” and “Systemic flaw in the system which rewards bad/quick fix medicine rather than addressing the root cause”. Other systemic constraints in this category included the burden of a heavy patient load, along with lack of reimbursement, and other systemic constraints exemplified in “Working currently in retail medicine so it is all about volume; they are trying to incorporate chronic care but not enough emphasis on lifestyle.” With respect to lack of appropriate reimbursement for work: “Organizations asking physicians to see more patients and not pay more…”
Among respondents who reported any level of burnout, the burden of insurance and reimbursement documentation was the second-most frequently mentioned response, 32%, consistent with the national trend of burnout components among physicians, 34 as in, “my practice has become more bogged down by data entry. I enjoy patient care but am frustrated by the demands of the EMR.” Also, “Overwhelming regulations, incredible documentation requirements, onerous pre-authorization requirements for everyday procedures, totally dysfunctional EMRs. 80% of my day is in front of a computer…”
Further, work-life balance and overwork accounted for almost a third of the burnout expressed (31%), as in the comment, “Working too many hours,” and “Not enough hours in the day to do what needs to be done for work and infringes on self-care and home life.” The lack of support was reported as an important reason for burnout (21%). This lack of support was sometimes, but not always, specifically related to the practice of LM. Comments include “lack of support in practicing lifestyle medicine” and “Admin always asking more of providers but not providing more compensation, in fact taking away benefits each year. Lack of autonomy.”
Poor patient outcomes from addressing symptoms instead of the root causes of disease, and ineffectively treating complex, multi-causative cases brought frustration (16%), expressed as “…medical model of treating illness rather than the root cause…” and “Allopathic pressures to treat symptoms rather than causes.” Additionally, dealing with challenging patients unwilling to change behavior who have expectations of easy solutions like medications and are influenced by advertisements (15%) and barriers to practicing LM (13%) were noted.
Reasons for Reductions in Burnout (n = 136)
Among those who reported they no longer felt burned out (28% of n = 482), the majority attributed the change to altering their work situation (84%), as noted by one participant: “Leaving a job that did not have a good grasp on provider well-being and team-based care. Pursuing a more flexible work schedule. Improving my own diet and physical activity regimen.” Within this group who changed their work situation, 43% reported that incorporating LM into their practice was a reason for this change, as explained: “It is aligned with my purpose, so provides satisfaction. I get time with patients and can address emotional/spiritual issues in addition to physical complaints, thus addressing the whole person,” and “Being able to offer a way to avoid or reverse chronic disease rather than simply ‘moving chairs around on the deck of the Titanic’,” as well as “Lifestyle medicine has revived my love of medicine. I enjoy seeing patients get healthier and happier using simple principles and without medications,” and “Finding Lifestyle Medicine - adopting it myself and a new found love for medicine now that I can share it (and truly heal!) my patients.”
Improved self-care was another top reason reported for no longer feeling burned out (29%), described by one participant as: “…I also implemented my own LM changes - increased physical activity, switched to plant-based diet, managed stress better.” Practicing LM resulted in greater work satisfaction/fulfillment, and mentioned as a reason for no longer feeling burned out (19%), for example, “LM practice has brought joy and meaning to my professional work.”
Six percent reported that empowering patients to improve their health outcomes improved burnout, for instance, “guiding the patient instead of shouldering all the pressure to heal the patient” and “…seeing patients transforming their lives daily and being very grateful.” Another 6% reported that implementing LM reduced burnout as it led to patient improvement, such as “Lifestyle medicine: I was burned out by the constant feeling that I wasn’t getting anywhere with patient health using pills and procedures. Now my patients actually get well! Gamechanger!!”
Perceived Impact of LM on Professional Satisfaction (n = 433)
A total of 90% (n = 433) of participants reported that LM had positively impacted their professional satisfaction, with n = 424 reporting only positive effects and n = 9 reporting both positive and negative effects. Among those who reported LM had a positive effect on their professional satisfaction, top reasons included professional satisfaction, sense of accomplishment, and meaningfulness (44%), with comments such as “Truly helping patients with the root cause of their health issues, more rewarding than any other care that I have provided patients.” Also, “To have a truck driver normalize his Hba1c from 11[%] in 3 months, it’s the biggest reward a primary care MD can get,” and “It’s satisfying and empowering to improve my health and others’ health.” Improved patient outcomes and satisfaction (26%) was depicted as “My patient outcomes have improved, and I have a greater confidence in being able to cure my patients” and “It gives me satisfaction to see patient’s locus of control when provided with the right information and tools.”
Also, enjoyment of teaching/coaching (22%) was mentioned as: “It has allowed me to provide evidence-based interventions that I not only teach to my students and clients but live in my own life,” “I really like having the opportunity to sit down with my clients to educate, monitor, and coach them to optimal health….,” “I feel it is my job to be a role model and walk the walk” and “joy in medicine again and educating patients.” Another 22% reported feelings that LM has helped personally with quality of life and less stress, expressed as “improvement in my personal life, encouragement that this will make a difference in disease treatment/reversal.”
For those who responded that they had never experienced burnout n = 43, the common themes were experiencing a sense of meaning in their work, having control over their work, having a stimulating and challenging work life, and having a strong self-care practice (data not shown). Of those who reported that LM had a negative impact on their professional satisfaction (n = 13), their reported frustration was universally over the inability to practice LM because of reimbursement, systemic challenges, or lack of resources or support to practice LM (data not shown).
Discussion
To the authors’ knowledge, this is the first study examining self-reported burnout among a sample of LM practitioners, 78% (n = 421) of whom reported practicing LM for one year or more. We found that greater reported implementation of LM in medical practice was associated with a reduced risk of burnout in this sample, and practitioners attributed their reductions to adoption of LM practice in their free text responses. Many respondents reported that LM positively affected professional satisfaction (90%). This high satisfaction rate is in stark contrast to one of the key components of burnout as identified in the accepted definition – the reduced sense of personal accomplishment,4–6 which has been reported in other settings such as oncology 35 and mixed specialty healthcare providers. 36 This study provides meaningful insight into potential solutions addressing the root causes of burnout among healthcare practitioners.
Previous attempts to reduce burnout have typically targeted organizational changes (i.e. adding staff, reducing rotations, reducing paperwork). These initiatives produced modest results, as one systematic review and meta-analysis revealed, indicating that implementing such organizational changes along with individually-focused interventions such as communication skills training and stress management resulted in an overall decrease in burnout from 54% to 44%. 22 In that study, emotional exhaustion score decreased 2.65 points out of a total score range of 0–30. 22 While meaningful, these interventions did not appear to address root causes of burnout such as lack of professional satisfaction.
Practitioners may be ill-equipped to overcome a sense of failure or lack of accomplishment if their patients' conditions progress unresolved,37,38 and, in our analysis, survey respondents shared in their own words that poor patient outcomes and treatment focused on symptoms rather than causes contribute to their experience of burnout, leading to a sense of “moral injury.”39,40 This inability to heal3,38 can lead to a feeling of powerlessness within a system that repeats moral distress 41 and further adds to burnout (depression, fatigue, depersonalization, and relationship stress).37,38 Among those practitioners who previously experienced burnout but no longer do in the current study (28%), the majority attributed their reduction to a change in work, with 43% of these having changed their practice to incorporate LM.
Of this same group reporting that they previously experienced burnout but no longer do, 6% reported their reduction in burnout was due to implementing LM leading to patient improvement, and another 6% reported that this change was directly due to empowering patients to improve their own health outcomes. A total of 22% of respondents who shared their positive impacts of LM noted enjoyment of teaching and coaching patients and engaging in relationships with patients and colleagues, thus suggesting a renewed sense of purpose and accomplishment. LM practitioners may experience increased feelings of accomplishment by empowering patients to take control of their health, as most chronic conditions are related to lifestyle. 42
Since LM focuses on a team-based approach, the fact that only 24% of practitioners surveyed reported working within an interdisciplinary team 100% of the time may indicate an added responsibility of carrying out LM implementation tasks that could be more effectively delegated to other team members, such as nutritional counseling, cooking demonstrations, physical activity interventions, emotional support, therapy, and substance use programming. While most clinical guidelines for chronic disease management point to lifestyle modification as first-line treatment in primary and chronic condition care, such as in guidelines from the American Diabetes Association, American Heart Association, and American Cancer Society,43-45 more work is needed to facilitate the integration of LM into the standard of care. Lack of support from staff, co-workers, and administrators to incorporate lifestyle approaches, reported by 21% of respondents experiencing burnout, may add a sense of lost opportunities to heal and support patients. This approach lays the foundation for a culture supporting whole person health46,47 for all stakeholders. More research is needed to quantify this experience. 48
Our sample of LM practitioners reported many frustrations similar to the general practitioner population, including a high workload, clerical burdens including medical record upkeep, other tasks unrelated to patient care, lack of control over work, short appointment times, and the constant task of work-life balance. These frustrations align with national trends.10,13,14,24,49,50 Specific to this sample, our previous analysis of this same survey data indicates that 55% of LM practitioners reported frustration at not being able to receive reimbursement for utilizing LM in their practice, as well a lack of support for LM practice from colleagues and administrators. 51 The results of this analysis suggest that the team approach of LM, incorporating dietitians, coaches, exercise physiologists, health educators and others,52-55 may address feelings of isolation within an ineffective system that respondents in this survey describe as rewarding volume over value.12,46
Our results support conclusions made by other researchers on burnout. Previous work has shown that implementing lifestyle changes can help avoid practitioners’ emotional exhaustion through effective treatment tools, self-care, and reduced depersonalization, based on a closer connection to patients and their healthcare team. 56 Furthermore, as LM includes the utilization of many behaviors that may strengthen one’s own ability to respond to stress, such as ensuring adequate sleep, having positive social connections, and optimizing stress management, it may further benefit practitioners.
As a 2022 survey of U.S. physicians found social determinants of health have a significant impact on patient outcomes, with 61% of respondents (N = 1502) feeling unable to address their patients’ social determinants and 87% wanting more time and flexibility to do so. 57 This is something that practitioners who have the opportunity to implement LM may be better positioned to address. As one respiratory therapist states, “The primary concern for burnout is not being able to emotionally take care of each patient individually or uniquely.” 58 Practitioner discontent may result from utilizing standardized medical practices that do not address the root cause of disease but rather manage symptoms (sick-care).30,31 An inability to resolve chronic disease using pharmaceuticals and other standard treatments may impede a practitioner’s ability to feel a sense of accomplishment,40,59,60 yet there is not much research addressing this concern.10,60
Strengths and Limitations
Although burnout has been widely studied in the context of standard care, this is the first study describing factors of healthcare practitioner burnout among a sample of predominately LM practitioners. Thus, the results offer a unique perspective on LM utilization and practice. Additionally, the mixed-method approach allowed for data capturing the practitioners’ own words, creating a deeper, richer view into the experiences of burnout and reasons for changes in burnout. The context and detail captured in the free-text answers provide a contextual explanation for results presented in the cross-sectional regression analysis. Additionally, the analysis includes a relatively large proportion of the target population, given that the total population of LM practitioners was targeted for this survey, as there is no other directly relevant professional society from which to draw LM practitioners.
At the same time, the membership of the medical professional society for LM has tripled since data collection, 61 thus, the sample size may now represent a smaller proportion of LM practitioners. Our survey results also may not be representative of healthcare practitioners nationally. It is important to note that this was a lengthy survey (approximately 30–40 min) targeted at busy healthcare practitioners, thus a high dropout rate is not surprising. The survey did not ask respondents about what setting they practice in, nor did it ask what enabled them to transition towards more LM practice; thus, we do not know if other factors that reduce burnout concurrently enabled them to practice more LM. Finally, this study was a cross-sectional survey among LM practitioners only, and therefore does not directly compare burnout among LM practitioners and non-LM practitioners. Future research should prospectively examine experiences of burnout among LM practitioners in comparison to similar groups of non-LM practitioners. A final limitation is that our survey and data collection were conducted prior to the COVID-19 pandemic, thus practitioner experiences may now be further affected by factors including different hospital patient-caregiver ratios, higher nurse and staff turnover rates, retention issues, staff shortages, politicization of illness, and higher death rates.
Conclusion
LM practitioners in this survey who practice a greater proportion of LM were significantly less likely to report burnout, suggesting that incorporating more LM into practice may potentially reduce burnout among healthcare practitioners interested in LM. Participant free-text responses further support this finding, as participants reported that incorporating more LM into their work promoted feelings of accomplishment due to improved patient outcomes and greater human connection (reduced depersonalization), addressing two defining components of burnout. Future research should examine experiences of burnout among LM practitioners in comparison to similar groups of non-LM practitioners. Additionally, future research should prospectively evaluate changes in burnout among physicians who begin practicing LM and explore how LM may support physicians and other practitioners to counter common causes of burnout. Burnout among healthcare practitioners has serious implications for quality of care, retention, and well-being, and burnout continues to increase. Two key contributors to burnout are depersonalization and a reduced sense of personal accomplishment. This study is the first to explore the experiences of burnout and reduced burnout among LM practitioners, adding new knowledge to our understanding of the root causes of burnout and how it can be ameliorated in this population. The outcomes from this study are highly encouraging for healthcare practitioners, indicating that greater practice of LM may help alleviate frustration as a foundational tool to manage and even reduce burnout in a time of demanding workload.SO WHAT?
What is already known?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - Lifestyle Medicine Practitioners Implementing a Greater Proportion of Lifestyle Medicine Experience Less Burnout
Supplemental Material for Lifestyle Medicine Practitioners Implementing a Greater Proportion of Lifestyle Medicine Experience Less Burnout by Kathryn J. Pollard, Joel Gittelsohn, Padmaja Patel, Liana Lianov, Kelly Freeman, Kara L. Staffier, Kaitlyn R. Pauly, and Micaela C. Karlsen in American Journal of Health Promotion.
Footnotes
Acknowledgments
The authors wish to thank Gail Rogers and Dr. Mika Matsuzaki for their assistance with statistical analysis.
Author Contributions
Dr. Karlsen was responsible for the study concept, design, and administration; acquisition, analysis, and interpretation of data; and drafting of the manuscript. Ms. Pollard led the writing and contributed to the acquisition, analysis, and interpretation of data. Ms. Staffier contributed to the analysis and interpretation of data. Drs. Karlsen and Gittelsohn provided oversight and supervision of the project. All authors contributed to the manuscript by providing critical revisions and intellectual content with respect to the interpretation of the data. Ms. Pollard and Dr. Karlsen had full access to all data and take responsibility for the integrity of the data and accuracy of data analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Pollard, Freeman, Staffier, Pauly, and Karlsen are employed by the American College of Lifestyle Medicine (ACLM). Lianov reports consulting payments and payments for attending meetings from ACLM and payments or honoraria from University of California Davis, Drexel University, Wellcoaches, and the American College of Preventive Medicine (ACPM). Gittlesohn reports consulting payments from ACLM. Patel declares no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was internally funded by the American College of Lifestyle Medicine (ACLM). ACLM staff engaged in the study design, analysis, and interpretation of results.
Ethical Approval
This study was reviewed by the University of New England Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.