
Abstract
Purpose
To examine how health care providers’ knowledge, attitudes, and practices affect their referrals to the National Diabetes Prevention Program.
Design
Cross-sectional, self-report data from DocStyles—a web-based survey
Setting
USA
Sample
Practicing family practitioners, nurse practitioners, pharmacists, and internists, n = 1,503.
Measures
Questions regarding health care providers’ knowledge, attitudes, and practices and their referrals to the National Diabetes Prevention Program.
Analysis
Bivariate and multivariate analyses were used to calculate predictive margins and the average marginal effect.
Results
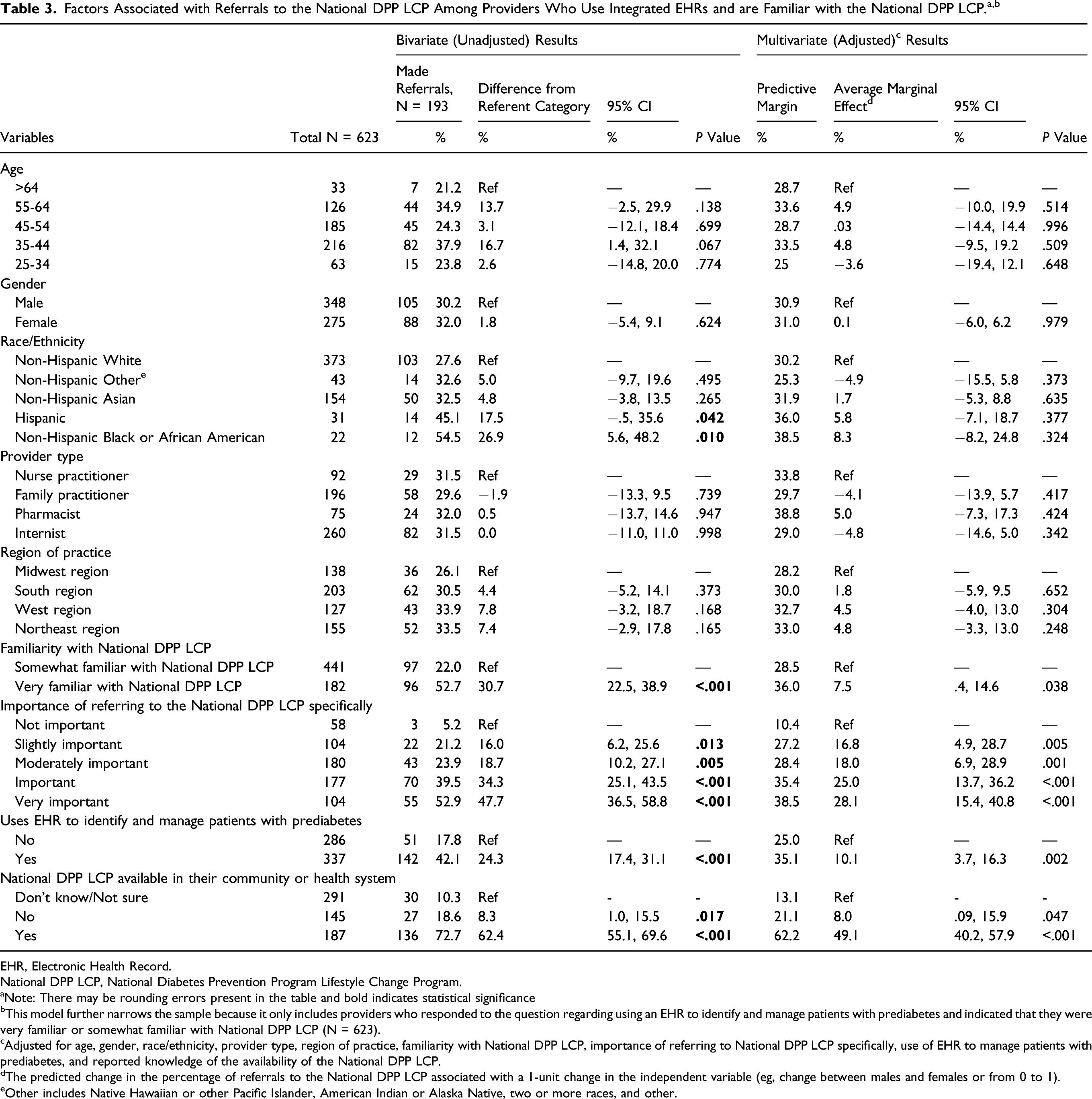
Overall, 15.2% of health care providers (n = 1,503) reported making a referral to the National Diabetes Prevention Program. Health care providers were more likely to make referrals if they were familiar with the program (average marginal effect = 36.0%, 95% CI: 29.1%, 42.8%), reported knowledge of its availability (average marginal effect=49.1%, 95% CI: 40.2%, 57.9%), believed it was important to make referrals to the program (average marginal effect = 20.7%, 95% CI: 14.4%, 27.0%), and used electronic health records to manage patients with prediabetes (average marginal effect = 9.1%, 95% CI: 5.4%, 12.7%). Health care providers’ demographic characteristics had little to no association with making referrals.
Conclusion
Making referrals to the National Diabetes Prevention Program was associated with health care providers’ knowledge of the program and its reported availability, their attitudes, and their use of the electronic health record system to manage patients with prediabetes.
Keywords
Purpose
There are 88 million adults in the United States who have prediabetes, a condition characterized by blood glucose levels that are high but not high enough to be diagnosed as diabetes. 1 If left untreated, prediabetes can lead to type 2 diabetes, a devastating chronic disease that affects millions of people in the United States. 1 Diabetes is the seventh leading cause of death in the United States, and contributes to over $320 billion dollars in direct health care expenses and reduced productivity costs.1,2
Several landmark studies, including the Diabetes Prevention Program (DPP) trial, have demonstrated that a structured lifestyle change program is an effective way to prevent or delay progression to type 2 diabetes for those at risk.3-7 Subsequently, Congress authorized the Centers for Disease Control and Prevention (CDC) to establish the National Diabetes Prevention Program (National DPP), a partnership between public and private organizations to deliver its lifestyle change program (LCP) nationwide.8,9
A vital piece of the National DPP is health care providers’ referrals of their at-risk patients to the LCP. 3 Providers who promote the National Diabetes Prevention Program and make referrals to it can be enormously influential because they are often a trusted source for their patients and potentially influence their health behaviors.10-13 The American Diabetes Association, along with other professional organizations, has recommended that providers refer their at-risk patients to a lifestyle change program, such as the one offered through the National DPP.7,14-16 Evidence has shown that patients who receive a referral from their provider for a lifestyle change program are more likely to participate in such a program. However, only 15% of individuals with prediabetes have been informed that they have the condition. 1 Additionally, less than 5% of patients with prediabetes or at risk for type 2 diabetes are reported to have received a referral to a lifestyle change program.13,17 Also, many providers have confirmed that they had not made referrals to a lifestyle change program,18-22 a result that may be linked to the large number of providers reporting that they are not familiar with the program.19,22 It is also unclear if providers are aware of the availability of the lifestyle change program. 22 Studies show that providers’ attitudes toward managing prediabetes are positive,18,21,23-25 but it is unclear if that same attitude extends to making referrals to the National DPP LCP. Therefore, the researchers sought to better understand providers’ knowledge, attitudes, and practices that may be associated with their decision to refer to the National DPP LCP.
Methods
Design
The researchers used data from the web-based survey DocStyles, 1 administered between June and August 2018. DocStyles was commissioned by Porter Novelli Public Services, 26 a public relations firm, and conducted by SERMO 27 to solicit responses from providers regarding various health conditions. Participants from SERMO’s Global Medical Panel of health care providers were sent a link to the survey and were paid an honorarium of $40-$90 for completing it.
Sample
SERMO set quotas to reach a certain number of family practitioners and internists (1,000), obstetrician/gynecologists (OB/GYNs) (250), pediatricians (250), oncologists (250), nurse practitioners (250), and pharmacists (250). To meet this quota, 3,465 providers were invited to participate in the survey. Only providers who practice in the United States; who actively see patients; who work in an individual, group, or hospital practice; and who have been practicing for at least three years were selected to participate in the survey. There were 2,256 providers who met those criteria and completed the entire survey, representing a 65.1% response rate. The remaining 34.9% either did not complete the entire survey (43), were excluded based on the screener questions (99), were excluded due to filled quotas (78), or did not respond to the invitation or tried to respond after the survey closed (989). Of the 2,256 respondents, diabetes-specific questions were only given to family practitioners and internists, nurse practitioners, and pharmacists, so the final sample for the current study consisted of 1,503 providers. No individual identifying information was included in the survey dataset and therefore this analysis was deemed exempt from [details omitted for double-anonymized peer review] Institutional Review Board approval process.
Measures
Demographic variables, including age, gender, race, ethnicity, region of practice, and provider type were collected in the survey and included in the current study. The researchers recoded the race and ethnicity variables to represent five categories: non-Hispanic white, non-Hispanic black or African American, non-Hispanic Asian, Hispanic, and non-Hispanic other (includes Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, two or more races, and “other” race). The researchers recoded the continuous age variable into five categories: 25–34, 35–44, 45–54, 55–64, and 65+ years.
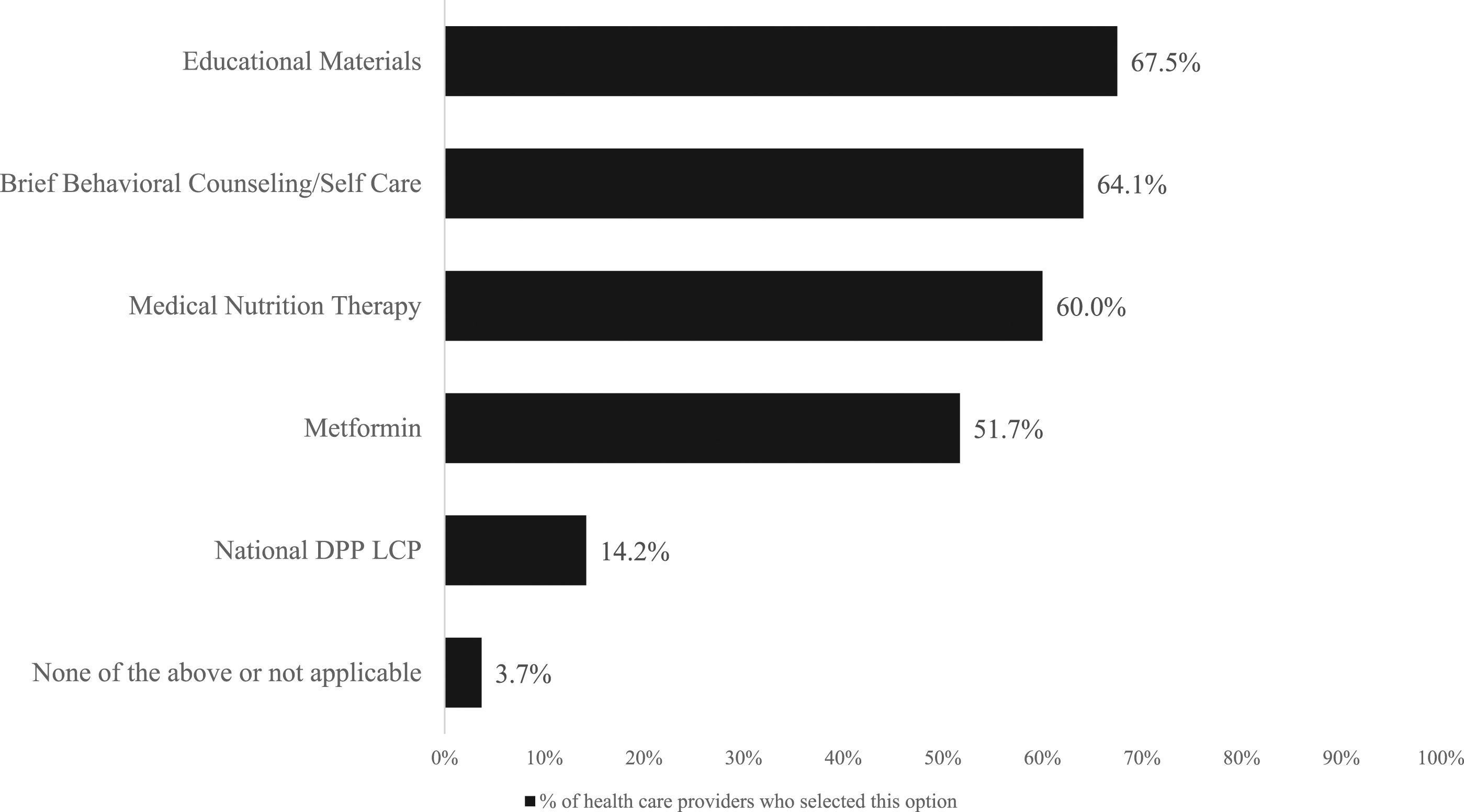
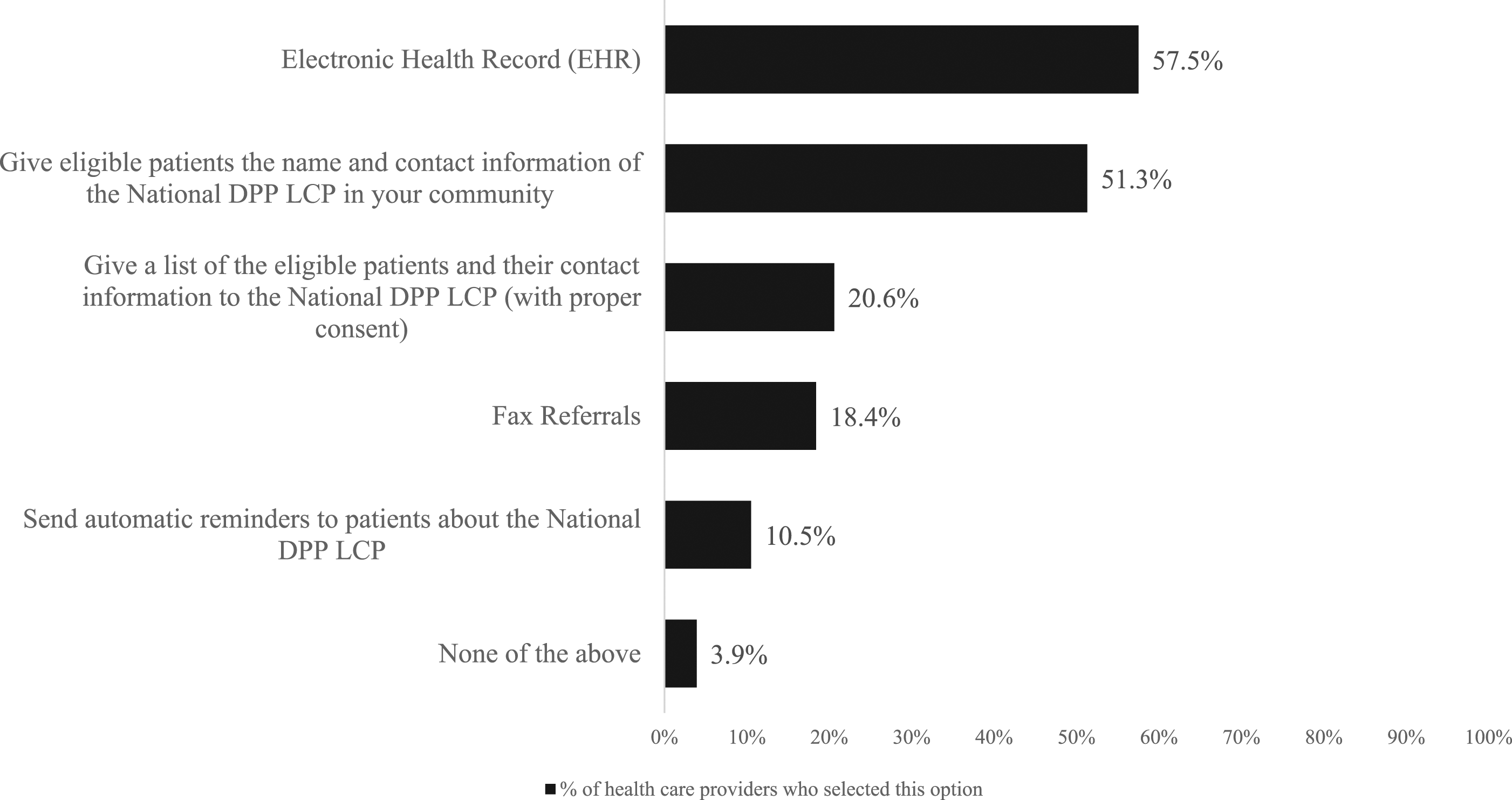
Providers’ familiarity with the program was assessed through the question, “How familiar are you with the National Diabetes Prevention Program lifestyle change program (National DPP LCP), a yearlong structured program, offered in person or online, aimed at preventing or delaying the onset of type 2 diabetes for individuals with prediabetes?”. Answer choices were very familiar, somewhat familiar, or not familiar. Their reported knowledge of the program availability was assessed through the question, “Is the National DPP LCP available in your community or health system?” with answer choices being yes, no, or don’t know/not sure. Skip patterns were used so that only providers who previously indicated that they were either very familiar or somewhat familiar with the National DPP LCP could respond to the second question. The main variable of interest was provider referral practices, which was addressed through the question, “Have you referred your patients with prediabetes to the in-person or online National DPP LCP to prevent or delay type 2 diabetes?”. The response categories for this variable were yes, no, and don’t know/not sure. Due to there being a small number of providers (N = 187) who selected the don’t know/not sure option, they were included with those who answered no. Providers’ attitudes toward the National DPP LCP were examined through the question, “How important is referring patients with prediabetes to the National DPP LCP, specifically?”. Answers were provided on a five-point Likert scale, from very important to not important. Providers were asked about whether they used an integrated electronic health record (EHR) in their practice or pharmacy. For those who did, they were then asked, “Do you use the capabilities of your integrated EHR system to identify and manage your patients with prediabetes?” Answer choices were yes, my EHR does not have this capability, don’t know/not sure, and no. Since the number of providers who selected my EHR does not have this capability and don’t know/not sure were too small to change the results of the analysis, they were included with those who said no. Two additional questions were asked (Figures 1 and Figure 2) to further understand providers’ treatment preferences for their patients with prediabetes and referral practices. Health care provider-recommended prediabetes treatment/management choices, DocStyles 2018. Description: Results from the question, “Which of the following are you most likely to recommend to your patients to prevent type 2 diabetes? (Select all that apply)”.
2
Analysis
Cross tabulations were used to conduct bivariate analyses to determine the association between providers’ referrals to the National DPP LCP and providers’ demographics, knowledge, attitudes, and practices; Wald test was used to obtain P-values.
Multiple logistic regression was used to generate predictive margins and 95% confidence intervals (CI) to estimate the probability of making referrals based on provider characteristics, knowledge, attitudes, and EHR use.28,29 The first adjusted model included only providers who responded to the question regarding using the EHR to manage their patients with prediabetes (N = 1,239 of 1,503). The second adjusted model further narrowed the sample because the addition of the question regarding reported program availability only included providers from the first model who were very familiar or somewhat familiar with the National DPP LCP (N = 623 of 1,239). For both models, additional covariates were included that had the potential to influence provider referrals, that is, age, race, gender, region of practice, and provider type. The analyses were carried out in 2020 using SAS Enterprise Guide, version 6.1 and Stata/IC, version 11.2.
Results
Health Care Provider Demographic Characteristics, Knowledge, Attitudes, and Practices: DocStyles 2018 Survey Respondents.
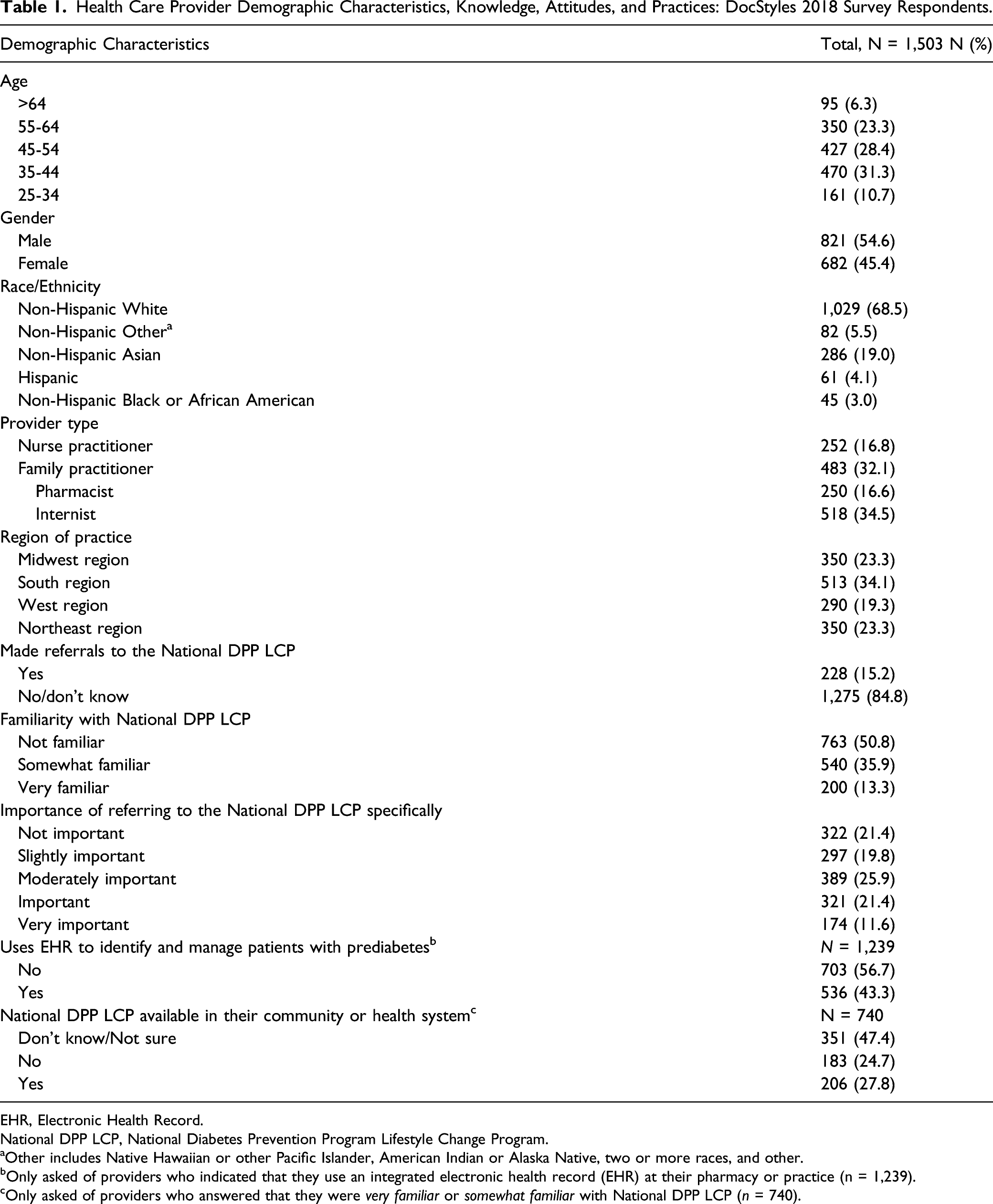
EHR, Electronic Health Record.
National DPP LCP, National Diabetes Prevention Program Lifestyle Change Program.
aOther includes Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, two or more races, and other.
bOnly asked of providers who indicated that they use an integrated electronic health record (EHR) at their pharmacy or practice (n = 1,239).
cOnly asked of providers who answered that they were very familiar or somewhat familiar with National DPP LCP (n = 740).
Factors Associated With Referrals to the National DPP LCP Among Health Care Providers Who Use Integrated EHRs in their Practice/Pharmacy. a,b
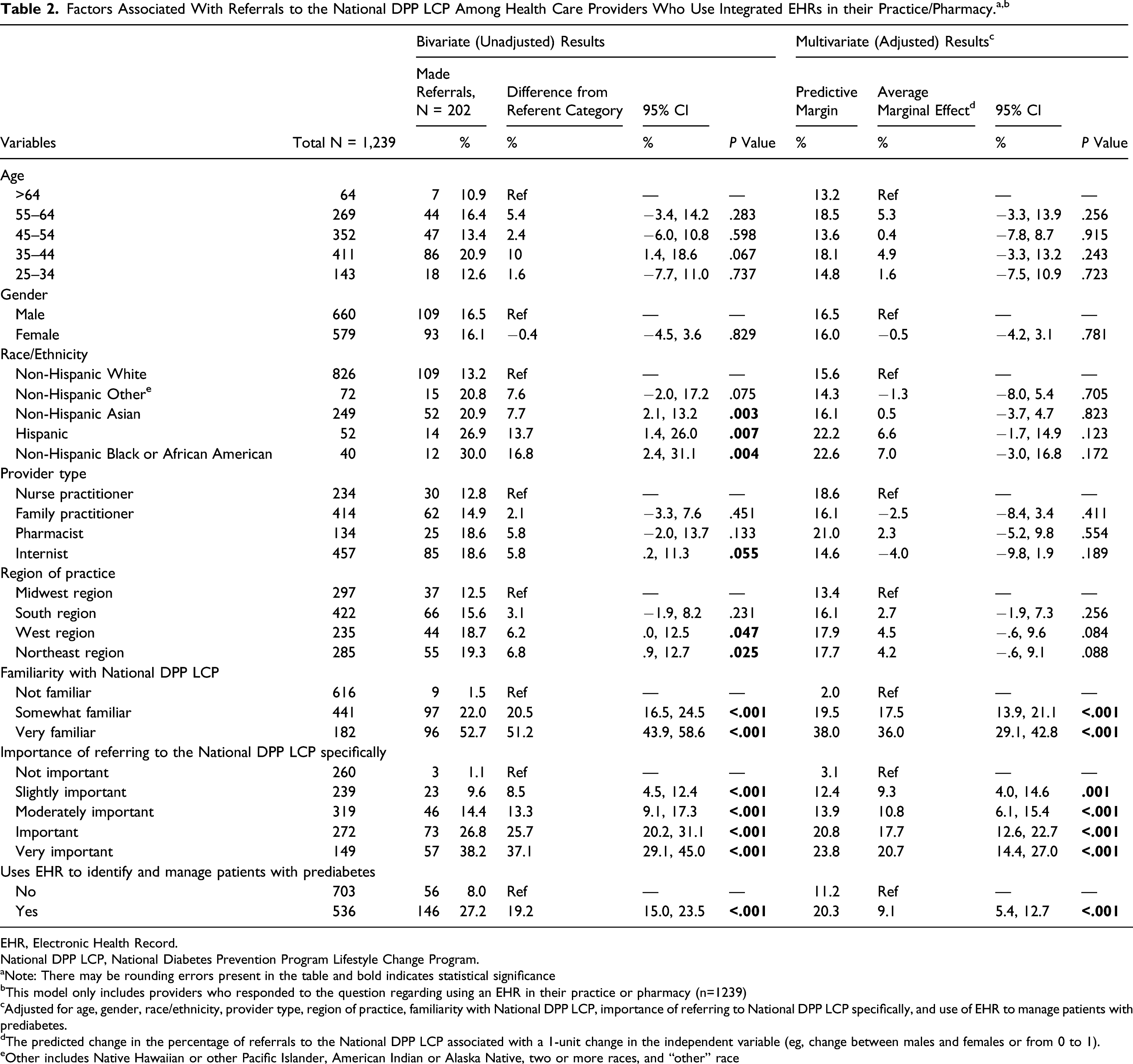
EHR, Electronic Health Record.
National DPP LCP, National Diabetes Prevention Program Lifestyle Change Program.
aNote: There may be rounding errors present in the table and bold indicates statistical significance
bThis model only includes providers who responded to the question regarding using an EHR in their practice or pharmacy (n=1239)
cAdjusted for age, gender, race/ethnicity, provider type, region of practice, familiarity with National DPP LCP, importance of referring to National DPP LCP specifically, and use of EHR to manage patients with prediabetes.
dThe predicted change in the percentage of referrals to the National DPP LCP associated with a 1-unit change in the independent variable (eg, change between males and females or from 0 to 1).
eOther includes Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, two or more races, and “other” race
Factors Associated with Referrals to the National DPP LCP Among Providers Who Use Integrated EHRs and are Familiar with the National DPP LCP. a,b
EHR, Electronic Health Record.
National DPP LCP, National Diabetes Prevention Program Lifestyle Change Program.
aNote: There may be rounding errors present in the table and bold indicates statistical significance
bThis model further narrows the sample because it only includes providers who responded to the question regarding using an EHR to identify and manage patients with prediabetes and indicated that they were very familiar or somewhat familiar with National DPP LCP (N = 623).
cAdjusted for age, gender, race/ethnicity, provider type, region of practice, familiarity with National DPP LCP, importance of referring to National DPP LCP specifically, use of EHR to manage patients with prediabetes, and reported knowledge of the availability of the National DPP LCP.
dThe predicted change in the percentage of referrals to the National DPP LCP associated with a 1-unit change in the independent variable (eg, change between males and females or from 0 to 1).
eOther includes Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, two or more races, and other.
Discussion
The results indicate that making referrals to the National DPP LCP was strongly and independently associated with providers’ knowledge of the program and its reported availability, their attitudes, and their use of the EHR system to manage patients with prediabetes. In contrast, making referrals had little or no association with providers’ demographic characteristics. These findings are encouraging because they suggest that referrals might be increased by addressing changeable factors such as knowledge, attitudes, and practices. This study had several strengths, including a high response rate (65.1%) which was consistent with previous analyses of DocStyles.19,30 Also, the current study builds upon a previous analysis 19 by adding pharmacists to the sample, asking providers specifically about the National DPP LCP, and including new variables to assess providers’ attitudes toward the program and its reported availability. Finally, because provider demographics, knowledge, attitudes, and EHR use were included in the models, the relative importance of all these factors could be shown, thus providing valuable insight into where to focus new approaches to provider engagement. These factors will now be explored in more depth.
Providers’ familiarity with the National DPP LCP and the reported the availability of the program were both shown to be highly associated with making referrals. To our knowledge, this is the first study to show the association between providers’ reported knowledge of the availability of the National DPP LCP and making referrals to the program. In fact, this variable had the strongest association with referrals of all the variables examined. Other studies have found similar evidence showing that providers who had heard of a LCP 19 or reported knowledge of the availability of one 30 were more likely to make referrals. Despite these promising results, the additional analysis showed that when given the opportunity to select their preferred treatment choice for patients with prediabetes, few providers chose National DPP LCP. In addition, 50% of the sample reported not being familiar with the National DPP LCP and over 70% reported that the program was either not available or they were not sure if it was, results which are consistent with another study that assessed providers’ awareness of the National DPP LCP. 22 Of note, although the multivariate results demonstrated a strong association between familiarity with the program and referrals, the predicted probability of referrals for those who were familiar was less than 40% when holding all other factors constant, indicating that it may be valuable to explore additional factors beyond familiarity with the program. Suggested strategies for increasing providers’ referrals to health-related programs include providing professional development/training about the program that explains the referral process, the benefits of referring their patients, and reinforces clinical guidelines31-34; encouraging positive referral behaviors through audit and feedback31,35; and increasing providers’ awareness of locally available programs.33,35,36 These results suggest that future marketing and engagement efforts may be beneficial if they include increasing providers’ familiarity with the National DPP LCP in addition to increasing their awareness of the program’s availability in their community or health system.
The current study showed that providers’ attitudes about the importance of making referrals to the National DPP LCP was associated with making referrals. As providers’ opinions of the importance of referral became more positive, the likelihood of referring increased, even after adjusting for other factors. To our knowledge, this is the first study to address providers’ attitudes toward making referrals to the National DPP LCP specifically, whereas other studies have assessed attitudes toward prediabetes screening and treatment.21-25 Although the multivariate results demonstrated that attitudes regarding the importance of making a referral was associated with the outcome, the majority of providers did not make a referral, even those who thought it was at least important to refer. This suggests that it may be valuable to explore additional factors that might influence providers referral behaviors. Another study found that providers’ attitudes and beliefs are significant barriers to making referrals to intensive behavioral counseling programs, and recommended strategies that reinforce the importance and effectiveness of the program to overcome any potentially negative attitudes. 37 Strategies to engage providers in the National DPP LCP referral process could include methods to bolster positive attitudes toward referring such as reinforcing the importance and effectiveness of the program, in addition to identifying any other attitudes that could be influencing referral behaviors.
Health care providers who used the EHR system to identify and manage their patients with prediabetes were more likely to make a referral to the National DPP LCP than those who did not. These results are in line with other studies where an increase in referrals was observed once providers were trained on using an integrated EHR system to do so.32,34 The additional analysis revealed that for providers who made referrals to the program, using the capabilities of the EHR system was their most common method of carrying out the referral. This indicates the potential benefits of encouraging the use of the EHR system to manage patients with prediabetes. Future strategies to increase provider referrals could consider promoting the use of the EHR system to manage patients,31,32 ensuring referring providers are confident in their ability to use the EHR system, 25 using opt-out vs opt-in referral pathways, 38 and promoting a seamless automated referral process to prevent disruption of current workflow.32-34 Doing so could increase the number of providers who use the EHR system to identify and manage their patients with prediabetes and subsequently make referrals to the National DPP LCP.
This study had several limitations. DocStyles consists of self-reported survey data, so recall bias could have affected the accuracy of the answers. Also, geographical bias could have influenced responses since approximately a third of the providers in the sample were practicing in the South region. In addition, social desirability bias may have led to providers responding that they were familiar with the program or made referrals even when those answers may not have been accurate. However, this seems unlikely to be highly prevalent since many providers indicated that they were not familiar with the program and had not made referrals. Also, because this was a cross-sectional survey, associations could only be viewed at a single point in time and the researchers cannot be sure that knowledge or attitudes predict future referral behaviors. Finally, selection bias could have occurred because the survey set a quota for number of provider types eligible to respond, so the responses collected may not reflect a generalizable sample of relevant health care providers. Research has been done to understand primary care providers’ knowledge, attitudes, and practices as they relate to prediabetes and lifestyle change programs. Health care providers’ familiarity with and reported knowledge of the National Diabetes Prevention Program (National DPP), as well as their attitude about the importance of referrals to the program, and their use of the EHR system to identify and manage their patients with prediabetes were independently associated with making referrals to the National DPP. This analysis gives credence to the need for provider engagement strategies that increase health care providers’ knowledge of the National DPP and its availability, that promote both the importance and effectiveness of making referrals to the program, and the use of the EHR system to manage patients with prediabetes. Addressing these malleable factors could not only increase referrals but may also influence the uptake of the National DPP. This could ultimately lead to a reduction in the incidence rate of type 2 diabetes because of the integral role that providers play in managing their patients’ health.So What?
What is already known on this topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgments
The authors would like to thank Shannon Michael for her assistance with data analysis, and the Synthesis, Translation, and Applied Research Team of the Division of Diabetes Translation, Centers for Disease Control and Prevention, for their assistance with designing the survey questions.
Author Contributions
LH contributed to the development of the scope and design of the analysis, contributed to the analysis and interpretation of the data, drafted the manuscript, critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.XZ contributed to the development of the scope and design of the analysis, the interpretation of the data, critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.BN contributed to the analysis of the data, the interpretation of the results, critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.KN contributed to the design of the survey, the scope of the analysis, interpretation of data, and critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.TK contributed to the design of the survey, the scope of analysis, interpretation of data, and critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.MC contributed to the development of the scope and design of the analysis, interpretation of the data, critically revised the manuscript for important intellectual content, read and approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, CyberData Technologies Inc., University of Central Florida, or the American Medical Association.
Ethical Approval
No individual identifying information was included in the survey dataset and therefore this analysis was deemed exempt from CDC’s Institutional Review Board approval process.