
Abstract
Retaining persons with HIV (PWH) in HIV care and ensuring access to antiretroviral therapy are crucial for reducing HIV transmission and enhancing health outcomes. HIV care engagement rates in the United States have plateaued over the last decade, indicating the need for innovative re-engagement strategies. We developed an automated electronic health record-based alert system to identify out-of-care (OOC) PWH presenting to any emergency department (ED) within the Duke University Health System. OOC was defined as no HIV care clinical visit in over 12 months. Automated alerts were processed by the HIV Rapid Response Re-engagement Team (H3RT), which connected with disengaged PWH by phone after an alert was triggered by an ED visit. Re-engagement was defined as a completed HIV clinic visit after H3RT outreach. The alert system identified 217 PWH, of whom 117 (54%) had transferred care to another health system. Among the 71 truly OOC PWH, 63% were male, 82% Black, and 34% uninsured. Median ED utilization while OOC was 1.30 ED visits/year [interquartile range (IQR): 0.66–2.37], compared with 1.05 ED visits/year [IQR: 0.33–1.85] when engaged in care. H3RT successfully re-engaged 46 (64.8%) of the 71 OOC PWH. The H3RT cohort had a higher proportion of persons assigned female sex at birth, uninsured, and Black compared with the overall engaged HIV clinic population. This low-cost, informatics-driven approach successfully re-engaged OOC PWH from priority populations within a large, multi-facility health system. Higher ED utilization rates among PWH while OOC support the integration of HIV care re-engagement efforts into these points of health care access. H3RT represents a scalable approach to HIV care re-engagement in Southern health care systems.
Introduction
The Southern United States accounts for more than half (52%) of new HIV diagnoses in the United States. 1 The Centers for Disease Control and Prevention estimates that 62% of HIV transmission occurs from persons with HIV (PWH) who are aware of their HIV status and who are either not virally suppressed or not optimally engaged in HIV care. 2 Disengagement from HIV care leads to increased morbidity and mortality for PWH3–5 and also increases the risk of HIV transmission to others.2,6,7
Despite the importance of regular HIV care engagement and sustained use of life-saving antiretroviral therapy (ART), national data suggest that at least 50% of PWH are not optimally engaged in HIV care. 8 Southern states tend to have lower rates of care engagement compared with other regions, which likely contributes to the South leading the United States in HIV transmission.9,10 Within North Carolina (NC), greater than a third of PWH were not virally suppressed in 2020. 11 The NC Department of Health and Human Services has had limited success re-engaging these out-of-care (OOC) PWH, with only 27% returned to care through state-based re-engagement programs. 12 Novel approaches are needed to identify OOC individuals and successfully link them back into HIV care. We aimed to use informatics to prioritize re-engagement for PWH with recent emergency department (ED) visits, with real-time alerts, to focus what we know are resource-intensive re-engagement efforts on this particular population, who may only interface with the health system for an acute medical or social service need.
ED visits or hospitalizations offer an opportunity to re-engage PWH who are OOC. PWH who are poorly engaged in care often have high ED utilization.13,14 In addition, ED utilization has been shown to be associated with risk factors for poor care engagement, such as substance use, unstable housing, and lack of insurance, and cohort studies have shown that PWH with ED use are less likely to be receiving ART or have a suppressed viral load.15–17 The post-ED encounter period may present an opportunity for a re-engagement team to engage a PWH who recently sought out medical care due to an acute medical or social service need. Systems that integrate HIV clinic team members into re-engagement care efforts at the point of care have shown promise in the published literature.13,18,19 Health system-wide re-engagement notification systems are likely to be more impactful in the South, where in many jurisdictions, health care is rendered by relatively few large health care systems (often with multiple facilities in the same jurisdiction). Few reports to date have explored the prospective impact of an electronic health record (EHR)-algorithm-informed notification system for HIV care re-engagement in the South.
We report findings from the first 3 years of the Duke Health HIV Rapid Response Re-engagement Team (H3RT), a clinical initiative that combines an EHR-algorithm-informed notification system for OOC PWH who presented for ED encounters with rapidly deployed re-engagement efforts to integrate these individuals back into HIV care.
Methods
Study design and setting
We created an EHR-based algorithm to identify individuals who presented to a Duke University Health System (DUHS) ED who had previously accessed care at a Duke HIV Clinic but had since disengaged from HIV care. Our algorithm was developed by the Duke Innovation and Scientific Enterprises Research Network (DISCERN), which combines both retrospective warehouse data and clinical events contained in prospective Health Level 7 (HL7) messages to provide a real-time alert to study personnel as individuals become eligible. 20 We leveraged this pre-existing system, an open-source, data-driven cohort recruitment system, typically used to alert study personnel of individuals who become eligible for a research study or clinical trial, for an HIV care re-engagement program. The trigger for the algorithm was a visit to the ED. The algorithm identified individuals who met the following criteria at the time of the ED visit: (1) HIV diagnosis by International Classification of Diseases, Tenth Revision (ICD-10) code (B20, B97.35, 098.7, R75, Z21); (2) at least one prior encounter in the Duke Infectious Disease HIV Clinic; (3) no HIV Clinic visit within the prior 12 months; (4) at least 18 years old at the time of alert. The DISCERN algorithm was deployed with technical assistance from the Duke Analytics Center of Excellence.
We included all three DUHS EDs located in the Durham/Raleigh metropolitan area, which combined account for nearly 185,000 patient encounters annually. The Duke Infectious Disease Clinic serves over 2,000 PWH annually at two sites in Durham, NC. We defined an ED visit as checking into one of the three EDs in the DUHS and defined having accessed care in our HIV Clinic as having evidence of a prior clinician visit at a Duke Infectious Disease Clinic since the inception of the DUHS EHR in 2013. We defined disengaged from care as no clinic visit for HIV care in the 12 months prior to the ED visit.
H3RT members consisted of three HIV clinicians and two social workers following the H3RT process map outlined in Figure 1. An alert generated by the DISCERN system arrived to H3RT as a page and email to each team member; however, after hours and on weekends, only an email was generated by the alert. Once an alert was generated, H3RT members manually reviewed the chart to confirm eligibility. Team member would determine if individuals were being seen by another provider outside the DUHS based on documentation of engagement with a provider responsible for their HIV care in the EHR (EPIC, https://www.epic.com), including review of the Care Everywhere Health Information Exchange platform (EPIC, https://www.epic.com/careeverywhere/) embedded in the EHR, which provides medical documentation from other health systems. Individuals who had evidence in the medical record or Care Everywhere of being established with another provider or facility for HIV care since being seen in our clinic were excluded from H3RT re-engagement.
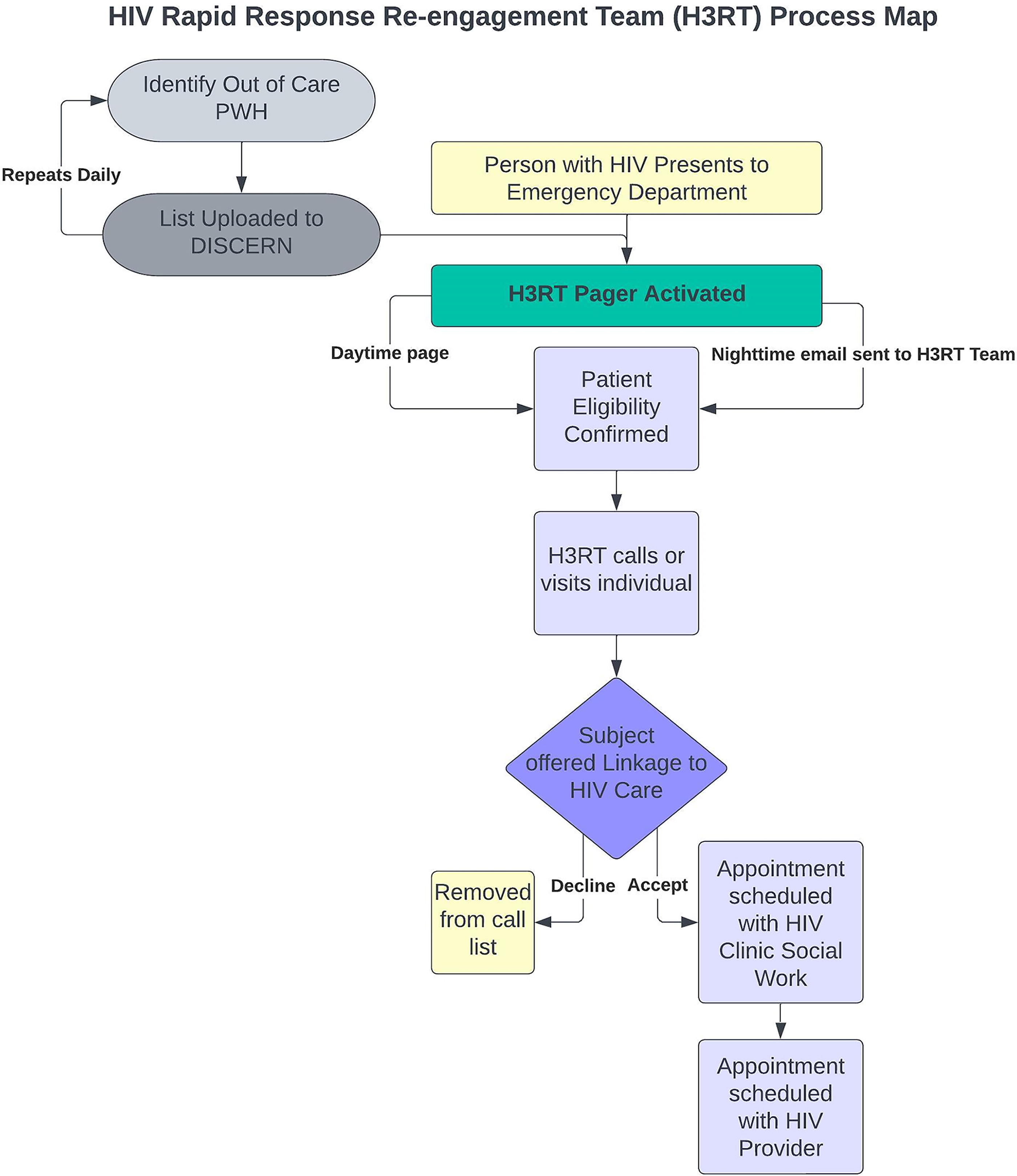
HIV Rapid Response Re-engagement Team (H3RT) process map combining automatic alert system with re-engagement team.
For eligible PWH who were not engaged in care, a physician team member attempted to contact the individual who triggered the alert, ideally within 72 hours by telephone after their ED visit. If a PWH was unable to be reached by two phone calls to contact information in the EHR, they were considered unable to contact. If a new alert occurred for a PWH who was not previously able to be contacted, a new set of phone calls was placed to the individual. Contact was attempted for up to a week after an alert was generated. For individuals that could be reached, H3RT performed a brief needs assessment and a screening for mental health and/or substance use needs via the Substance Abuse and Mental Illness Symptoms Screener (SAMISS). 21 The SAMISS was reviewed by the social worker at the time of re-engagement to inform the needs of PWH. Afterward, the team member scheduled an appointment with an HIV clinician and clinical social worker. Appointments were only scheduled after we contacted the individual directly. Individuals were offered an appointment with a social worker at the point of re-engagement to perform a more in-depth needs assessment and provide referrals for additional supportive services as necessary (e.g., housing, case management, and behavioral health). Re-engagement was defined as completed clinic visit after H3RT contact. PWH were followed from the time of their medical encounter until they were successfully re-engaged in care, or until the end of the study period. The intervention period was 34 months, from October 2020 to August 2023.
Primary outcome and statistical analysis
The primary outcome was completion of a scheduled follow-up HIV clinical appointment after H3RT alert. Re-engagement in care was defined as attending an appointment with an HIV clinician after contact by the H3RT. Demographic information collected for this project included age, sex assigned at birth, self-reported race, self-reported ethnicity, primary language, and insurance status at the time of disengagement. Public insurance included persons with Medicaid and Medicare. Uninsured PWH had no insurance at the time of last HIV care visit prior to disengagement. All uninsured, including uninsured PWH enrolled in the North Carolina HIV Medication Assistance Program (HMAP), were included in this group. The clinic attempts to enroll all eligible uninsured PWH in HMAP, the AIDS Drug Assistance Program that uses state and federal (Ryan White Part B) funds to provide medications for the treatment of HIV, related conditions, other comorbidities, and related opportunistic infections. We collected clinical information such as smoking status, mental health disorder, substance abuse disorder, ED use, and last HIV viral load prior to disengagement from HIV care using the Duke Enterprise Data Unified Content Explorer interface. 22 Viral suppression was defined as viral load less than 200 copies/mL. Continuous characteristics were presented as median with interquartile range (IQR), and categorical variables were presented as count (percent). Due to the low number of eligible persons, logistic regression was not performed to compare factors associated with likelihood to re-engage. We compared demographic characteristics of our OOC persons identified by H3RT (n = 71) to the engaged PWH Duke Infectious Disease Clinic population between 2021 and 2022 (n = 2,066). The clinic cohort included for this comparison was a snapshot of our clinic population that included PWH ≥18 years old with at least one HIV care visit with a physician or advanced practice provider in the Duke HIV Clinic between 2021 and 2022. Fisher’s exact test was used to compare proportions of PWH identified by H3RT compared with the composition of the Duke Infectious Disease Clinic. Statistical significance was set at α < 0.05.
To evaluate ED utilization rates for engaged period and OOC period, we calculated the median rate of visits per year for each time period. Engaged period was defined as period of continuous engagement (at least 1 HIV care visit every 12 months). Disengaged period was counted from the last HIV clinic visit to either re-engagement in care through H3RT or the end of the study period for those who never re-engaged. Two individuals were excluded from this part of the analysis because they had no time in the engaged period (they only had one HIV clinic visit before they disengaged). R version 4.0.0 (R Core Team), with the RStudio interface was used for statistical analysis.
The Duke University Institutional Review Board determined the study was exempt (Pro00104825), and informed consent was not required or obtained, in accordance with Title 45 CFR§46.
Results
Over the 34-month study period, the DISCERN algorithm triggered 507 alerts (approximately 15 alerts/month), with 45% occurring during the business hours of 9:00 AM to 5:00 PM, Monday to Friday, and 54% occurring on evenings and weekends. The 507 alerts were generated from 217 unique individuals (some with multiple ED visits) classified as disengaged from HIV care at the time of presentation to a DUHS ED. Manual chart review of these 217 individuals revealed that 54% (117/217) had transferred care to another health system since last being seen at the Duke Infectious Disease Clinic. Over half of these individuals (64/117, 55%) transferred care to one of two other HIV clinics in the Durham–Chapel Hill area: a nearby federally qualified health center and a neighboring academic institution. Nine of the 217 individuals that triggered an alert were considered ineligible, given that they had an HIV clinic appointment already scheduled within 30 days of the alert (9/217, 4%). Twenty individuals that triggered the alert (20/217, 9%) were currently engaged in HIV care in the Duke Transplant Center, in which infectious disease providers see PWH under the umbrella of the transplant clinic, a designation that was not included in our alert algorithm. In total, 71 individuals were determined to be eligible for re-engagement after manual chart review.
Of the 71 OOC PWH, 63% (45/71) were assig!ned male sex at birth, and 82% (58/71) identified as Black or African American. Thirty-four percent were uninsured, and 42% (30/71) had Medicaid or Medicare insurance. Viral suppression (HIV polymerase chain reaction viral load <200 copies/mL) was seen in 63% (45/71) at last HIV clinic visit prior to disengaging from care. Furthermore, 62% (44/71) had a mental health diagnosis such as an anxiety disorder, depression, schizophrenia, bipolar disorder, or adjustment disorder, and 45% (32/71) had a diagnosis of a substance use disorder (Table 1). The median time of continuous engagement at the Duke HIV Clinic prior to falling OOC was 4.46 years (IQR: 2.13–6.17). For PWH who were re-engaged in HIV care by H3RT, the median time OOC prior to re-engagement was 1.89 years (IQR: 1.40–2.96). For persons who were not re-engaged by H3RT by the end of the study period, the median observation time OOC was 2.78 years (IQR: 1.77–4.49). During the intervention period, the 71 OOC persons identified by the alert algorithm had a total of 449 ED visits, 20% of which resulted in a hospital admission (90/449). The median rate of ED visits per year was greater during the OOC period [1.30 ED visits/year, (IQR: 0.66–2.37)] compared with the period when the PWH was engaged in HIV care [1.05 ED visits/year, (IQR: 0.33–1.85)].
Clinical and Demographic Features of Eligible Out-of-Care Persons with HIV Identified by H3RT Alert System
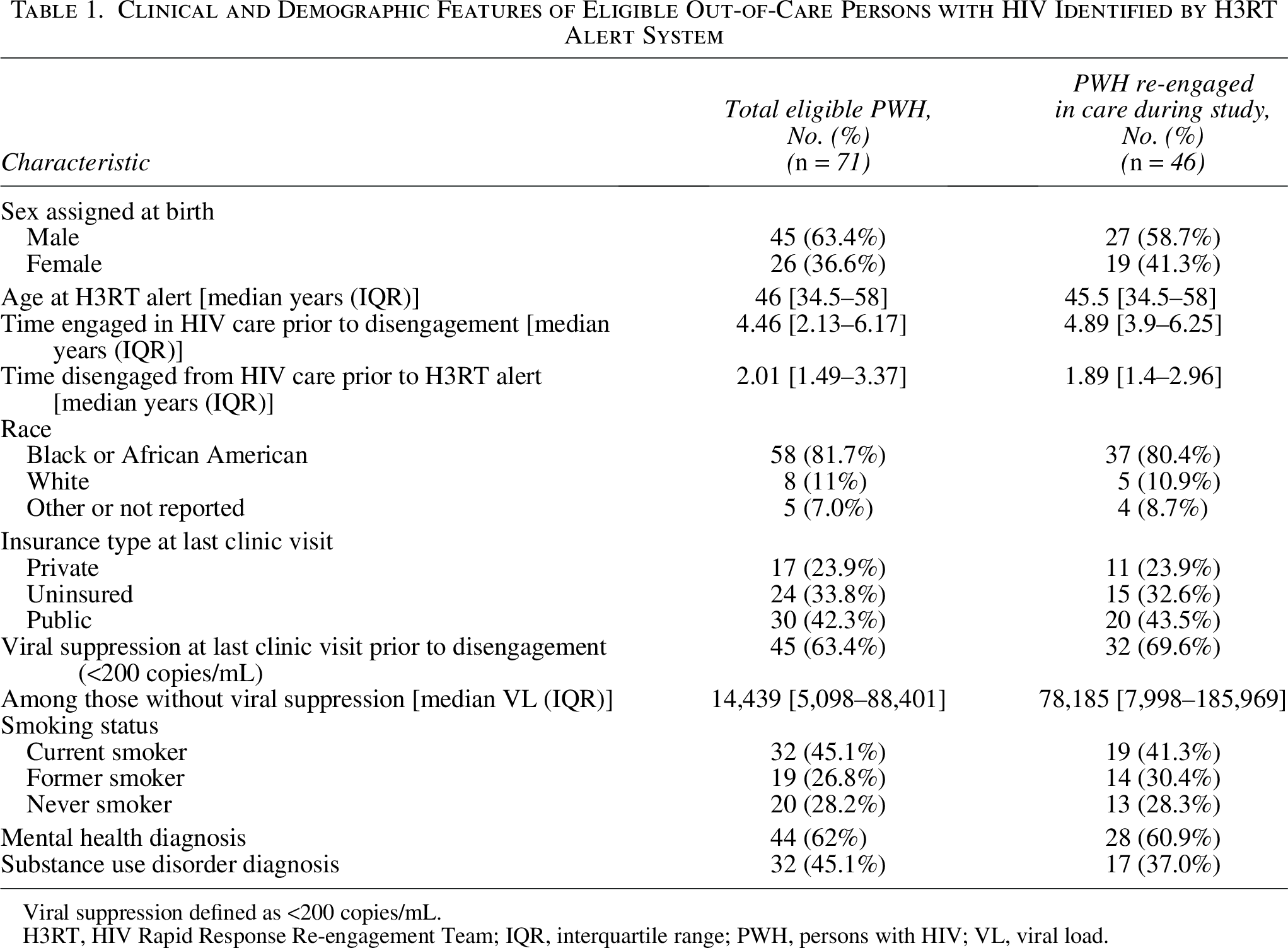
Viral suppression defined as <200 copies/mL.
H3RT, HIV Rapid Response Re-engagement Team; IQR, interquartile range; PWH, persons with HIV; VL, viral load.
Among the OOC PWH identified by H3RT in a Duke Health ED, there was a higher proportion of individuals who self-reported as Black/African American (81.7% vs. 59.7%), assigned female sex at birth (36.6% vs. 26.0%), and uninsured (33.8% vs. 14.9%) compared with the composition of the population of PWH engaged in care within the Duke Infectious Disease Clinic (Fig. 2).
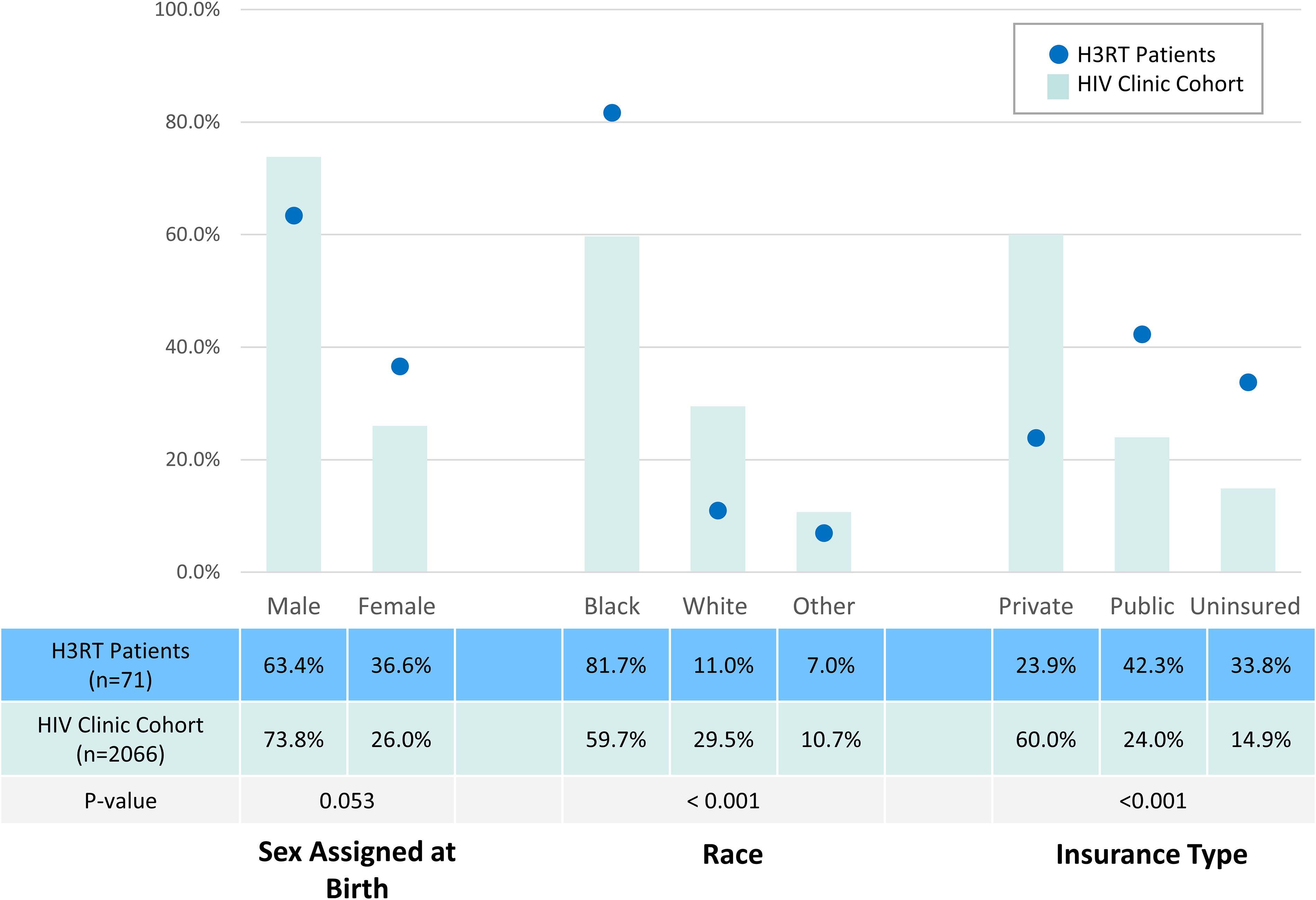
Proportion of patients identified by H3RT alert system compared with the general HIV clinic composition. H3RT, HIV Rapid Response Re-engagement Team.
Among persons eligible for re-engagement in HIV care, 59 of 71 (83%) were able to be reached by telephone. We were unable to contact 12 people. Of those contacted, two declined follow-up for their HIV care: one was previously noted to be an elite controller and declined additional follow-up, and the other individual did not wish to engage with H3RT. Three individuals that were contacted reported transfer to another facility for HIV care. The remaining 54 that engaged with the H3RT team agreed to schedule an HIV care appointment, of which 46 persons completed an HIV care appointment. Overall, 46 of 71 (64.8%) PWH identified by the H3RT alert re-engaged in care during the study period. Forty-one percent of these individuals (19/46) were re-engaged within 30 days of the ED visit that generated the OOC alert. Of the 52 people who agreed to be scheduled for an HIV follow-up appointment, 40 showed up to the initial appointment, and an additional 6 who missed the first appointment ultimately re-engaged during the study period (Fig. 3). Of the 46 patients who re-engaged in care during the study period, 58.7% were assigned male sex at birth (27/46), 41.3% were assigned female sex at birth (19/46), 80.4% were Black (37/46), 10.9% were White (5/46), and 8.7% were other or had no racial classification documented (4/46). Forty-three percent successfully re-engaged in HIV care had public insurance (20/46), 32.6% were uninsured (15/46), and 23.9% had private insurance (11/46) (Table 1). Four PWH died during the study period and all four had re-engaged in care prior to their death.
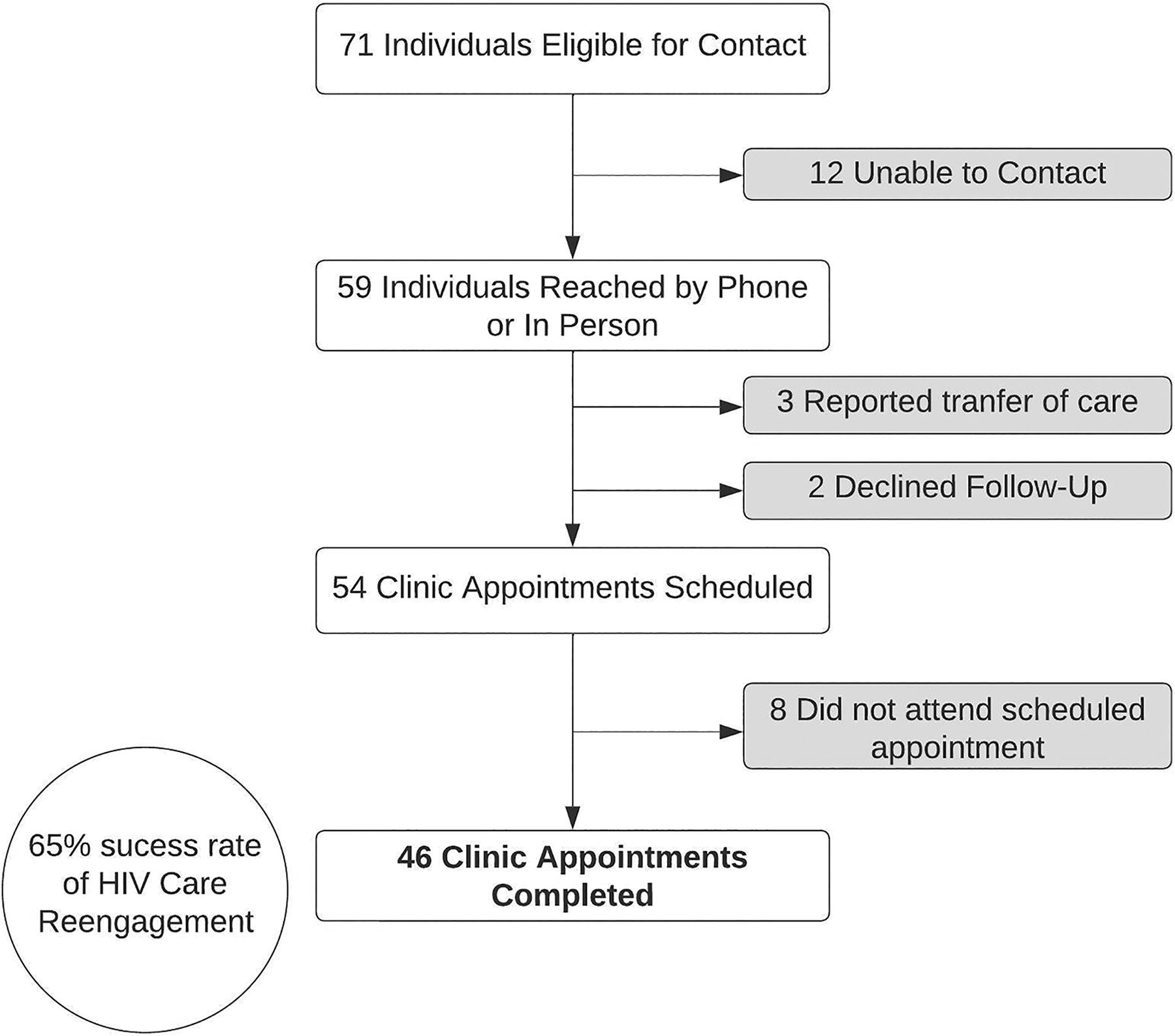
HIV care re-engagement flowchart for out-of-care persons with HIV identified by the HIV Rapid Response Re-engagement Team (H3RT) alert system.
Discussion
Poor retention in HIV care remains a significant public health issue, with no improvement in HIV care retention rates seen across the United States over the past decade. 23 We leveraged clinical informatics to create an alert algorithm to identify OOC PWH seen at a DUHS ED and successfully re-engaged 65% back into HIV care. When considering re-engagement rates among the 54 PWH who spoke directly with an H3RT team member and agreed to schedule an appointment, 85% (46/54) re-engaged in HIV care. Only 8 of 54 individuals who agreed to schedule an appointment remained OOC at the end of the study period. Our study found that we achieved high rates of re-engagement among disengaged PWH, with even higher rates of engagement among those who were able to engage directly with the H3RT by phone within 72 hours of the ED encounter.
The success of our program, which focuses on re-engagement of OOC PWH immediately after seeking health care in the ED, supports the hypothesis that interaction with the health care system for emergency care may be an important touch point when re-engagement efforts may be more successful.13,24 Our OOC PWH had higher rates of ED use once they fell OOC, suggesting the ED is a high-yield setting for identifying individuals who have fallen OOC or may otherwise infrequently interact with the health care system. The high proportion of OOC PWH identified by this intervention who were assigned female sex at birth, who identified as Black or African American, or who were uninsured supports the use of the ED visit as a unique and important way to identify priority populations, including those with an increased risk for advanced HIV/AIDS and non-AIDS-related morbidity and mortality.25,26 In addition, keeping PWH engaged in care may be an incentive for health systems, as it can reduce costly ED visits and potential hospital admissions, particularly for underinsured or uninsured persons. An ED-based approach to HIV care re-engagement also focuses resources on PWH who are likely to be in the area, whereas some statewide programs for re-engagement involve tracking down PWH generated from data, which may not be real-time or reflective of where they currently reside.
Health systems in other regions of the United States have had success in implementing re-engagement teams in the ED setting. In an academic health system in Chicago, Illinois, OOC PWH were identified by an EHR-based algorithm when they accessed care in the health system’s ED. 18 The alert system identified every PWH presenting to the ED, and a team manually determined if they were OOC. While manual chart review was essential to confirm if a PWH transferred HIV care to another center in our study, our algorithm only identified PWH with no recent HIV care visit in our health system to improve the accuracy of the alert system. The alert system in Chicago achieved a re-engagement rate of 66% among eligible individuals, similar to the results of our alert system. In Seattle, Washington, an academic center partnered with the health department to add precision to their identification of OOC PWH with the use of real-time data exchange to identify virally unsuppressed PWH presenting to the ED or inpatient admission (ED/IP). 13 Once an alert was generated by the data exchange, an HIV care relinkage team linked the PWH to follow-up care. This team defined care re-engagement as a viral load test within 3 months of ED/IP-generated alert and did not see a significant increase in care re-engagement during their intervention; however, they found improved viral suppression by 6 months after an ED/IP-generated alert. While health centers have had success implementing re-engagement teams in the ED setting, such efforts have not been studied in the U.S. South. A health system-wide strategy that leverages health care utilization data from HIV clinic visits, admissions, and ED visits from across the health system would likely be high impact in the South, where large health care systems dominate the health care landscape.
The informatics-driven H3RT intervention was shown to be a low-cost means to identify and re-engage OOC PWH within a large health system using clinical informatics and a small re-engagement team. These features are particularly attractive because such a low-cost and labor-efficient model is more likely to be adopted in Southern health systems, where resources dedicated to PWH re-engagement efforts may be limited. The total cost to the informatics team to set up the EHR-based algorithm was a one-time fee of $250. The re-engagement team of three physicians rotated time as lead on the H3RT pager every month, with approximately 4 hours of effort per month. The success of the program was also linked to our ability to utilize pre-existing systems within the health system, such as EPIC and DISCERN, for real-time alerts generated from up-to-date data. With the growth of health information technology and informatics capacity within health systems and public health departments, many centers have access to similar programs that integrate warehoused data within their system with time-sensitive criteria and automatic alerts. Using these pre-established systems, often used for clinical trial recruitment or surveillance alerts, to identify OOC individuals when they interact with the health care system is a promising and feasible approach for Southern health care systems.
Although we achieved a high rate of HIV care re-engagement, our EHR-based alert system had some limitations. Over half of the PWH generating alerts appeared OOC based on health system data (54%) but had actually transferred care to another facility, often referred to as “silent transfer.” A prior report highlighted high rates of silent transfer within a multisite HIV clinic in Tennessee. In this setting, misclassification of OOC PWH was improved with integration of a statewide database into their OOC classification. 27 Still, many health systems and community clinics do not have a direct and dynamic relationship with statewide data, which may better be able to identify PWH who are OOC. Challenges in accurately identifying OOC PWH to prioritize for care re-engagement have been well documented. An OOC surveillance pilot study conducted by the Massachusetts Department of Public Health found that 75% of the persons characterized as OOC were erroneously classified (the majority had moved or were engaged in care elsewhere). 28 In Washington state, a clinic-based surveillance intervention found 79% of the individuals classified as OOC had moved, transferred care, or were in a correctional facility. 29 A large collaborative analysis in six Northwestern states likewise found 72% of PWH described as OOC had rather moved, died, or were erroneously identified as OOC. 30 The data silos between major health care organizations in the same jurisdiction represent a major structural barrier to fully harnessing the power of data science to address the gaps in the Southern HIV care continuum. Structured data elements in the EHR, such as encounter data and viral load, fail to recognize transfer of care to another facility, institution, or out of state. The use of automatic alerts to identify OOC PWH could be greatly improved by incorporation of nonstructured data elements, which may provide better indicators for transfer of care. Advancements in the use of machine learning and natural language processing to correctly define PWH disposition are needed to focus our efforts on those who are truly lost to care. We aim to refine our algorithm with machine learning to exclude individuals who have evidence of transfer to another facility in clinical notes.
Additional limitations in the study structure include the lack of a control group. Some individuals may return to care voluntarily, and we do not present a control group that evaluates pre-intervention rate of return to care after disengagement. A prior study in our health system, however, evaluating care engagement between 2008 and 2012 suggested around 20.8% of OOC PWH voluntarily re-engaged with the clinic each year. 24 Furthermore, individuals who triggered H3RT alerts near the end of the study may not have had time to complete their re-engagement prior to the study conclusion. Finally, although we achieved high rates of HIV care re-engagement through our alert system, we will need to follow the individuals who returned to care longitudinally to monitor long-term engagement, viral suppression, and health care utilization among this group. The reach of H3RT is currently limited to PWH who visit a Duke Health ED during their OOC period. There may be other valuable health care interactions that can be harnessed for re-engagement, such as urgent care visits. Further, to have a larger impact on eliminating the HIV epidemic in the United States, it will be important to assess the ability of H3RT to expand its benefits beyond a single health system.
H3RT is an innovative approach that integrates EHR-informed algorithms for the identification of OOC PWH with responsive clinical care teams committed to supporting people’s return back into HIV care. This strategy is low cost, and given the low personnel requirements, we believe that it is also highly scalable to health care systems in the Southern United States, the epicenter of the nation’s HIV epidemic, and beyond. A formal cost-effectiveness analysis of this ED-utilization HIV care re-engagement approach would be a valuable area for future research. We seek to continue to refine our algorithm’s data input pathways, in an effort to improve the precision of our notification system and further decrease the burden of work on H3RT team members. If successful, we will expand implementation to urgent care facilities throughout Duke Health, leveraging the broad reach of the health system in our region and offering a potential model to inform similar strategies across Southern health systems. Overall, H3RT presents a promising example of how health system-based clinical informatics can help optimize the HIV care continuum and ultimately impact the trajectory of the Southern HIV epidemic.
Authors’ Contributions
Conception and design: C.M.B., N.L.O., D.P., and J.P.; Data collection: N.A., C.M.B., D.P., and N.L.O.; Analysis and interpretation of results: N.A., C.M.B., J.D.J., F.H., R.B., and N.L.O.; Writing—original draft: N.A.; Review and editing: N.A., C.M.B., J.D.J., F.H., R.B., D.P., J.P., and N.L.O. All authors reviewed the results and approved the final version of the article.
Footnotes
Acknowledgments
The authors acknowledge the collaborative efforts of the Clinical Social Workers at the Duke Infectious Disease Clinic, including Sarah Schmidt, Amy Carmen, and Scotty Elliott, and the Duke Center for AIDS Research (5P30 AI064518).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Duke University Center for AIDS Research (CFAR; 5P30 AI064518).