
Abstract
Exposure to potentially traumatic events (PTEs) is common in students and might lead to post-traumatic stress disorder (PTSD). Nevertheless, population-based information about PTSD in students is lacking in the Netherlands. Therefore, we aimed to determine the prevalence of PTEs, PTSD, help-seeking behavior, treatment history, and help-seeking barriers in a population-based sample of Dutch students. A total of 270 students (Mage = 20.7 years, SDage = 3.5 years) completed online self-report questionnaires, including the Life Events Checklist for DSM-5 (LEC-5), the PTSD checklist for DSM-5 (PCL-5), and the International Trauma Questionnaire (ITQ). The lifetime prevalence of any PTE was 79.3%. Bullying and an unwanted sexual experience were the most frequent self-experienced PTEs during the study years. The prevalence of probable lifetime Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) PTSD was 22.2%, current DSM-5 PTSD was 2.6%, and current complex PTSD (CPTSD) was 4.1%. Of the students with probable lifetime PTSD, only one-quarter received first-line trauma-focused treatment. Common reasons for not seeking help included avoidance, shame, and lack of knowledge. In conclusion, PTSD prevalence is high in Dutch students compared to the general population. The treatment gap and the discovered barriers underline the importance of education about PTSD and treatment options, to raise awareness and increase access to treatment.
Introduction
Exposure to potentially traumatic events (PTEs) can lead to stress symptoms that in most cases remit within the first month after onset (American Psychiatric Association [APA], 2013; Kessler et al., 2017). However, for some individuals these symptoms persist and develop into disorders such as post-traumatic stress disorder (PTSD; Kessler et al., 2017) or complex PTSD (CPTSD; World Health Organization, 2019).
Exposure to PTEs is common in late adolescence and, specifically, during the student years (Benjet et al., 2016, Breslau et al., 1998). Moreover, the risk of developing PTSD is elevated during this stage of life (Breslau et al., 1998). The transition to student life introduces challenges such as distance from the previous social support network, financial strain, and academic pressure, all of which may increase PTSD risk following exposure to a PTE (Brown, 2018; Conley et al., 2018; Sheldon et al., 2021). A recent population-based study in the Netherlands found that young adults are at increased risk of developing PTSD (Hoeboer et al., 2025). 1
PTEs and PTSD in Students
Research on PTEs and PTSD in students is essential, as PTSD has been associated with comorbid mental health conditions, school dropout, and adverse health outcomes (APA, 2013; Boyraz et al., 2016; Cusack et al., 2019; Tripp et al., 2015). However, few studies investigated exposure to PTEs and consequent PTSD prevalence in population-based student samples according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)/International Classification of Diseases 11th Revision (ICD-11). Regarding PTSD, previous studies in student samples reported DSM-5 (probable) current and lifetime PTSD estimates of 9.2% and 34.4%, as well as ICD-11 PTSD and CPTSD estimates of 4.6% and 3.4%, respectively (Cusack et al., 2019; Elhai et al., 2012; Truskauskaite et al., 2023). In addition, following the outbreak of COVID-19 pandemic, an increase in PTSD rates has been registered, with an estimated pooled prevalence of coronavirus-related PTSD in university students of 23% (Idoiaga et al., 2022). Moreover, the rise of the “MeToo” movement could reveal higher levels of PTSD associated with sexual assault (Boskovic et al., 2023; van Berlo, 2022; Wellum et al., 2023).
Regarding PTE exposure, a study on Australian students showed that approximately 64% of the students had experienced at least one PTE in their life (Walters et al., 2025), and a Brazilian study found that 93% of first-year college students had experienced a PTE (Pereira et al., 2018). Furthermore, recent studies in the Netherlands and Belgium reported a wide range of prevalences of inappropriate behavior and sexual assault, ranging from 4% to 56% (Boskovic et al., 2023; Ministry of Education Culture and Science, 2022; Wellum et al., 2023). Regarding inappropriate behavior, 58% of the students indicated that perpetrators included university staff (Ministry of Education Culture and Science, 2022).
Additionally, research findings showed that a majority of students experienced some form of interpersonal violence in the past year, with sexual harassment, peer victimization, and psychological partner abuse reported most frequently. Moreover, affiliations with groups such as athletics, fraternities, student government, and student unions were risk factors for heightened exposure to violence (Swan et al., 2021). Intimate partner violence among college students has also been linked to poorer physical and mental health outcomes (Seon et al., 2022). In the Netherlands, it was found that physical and sexual violence are common among young people (Hoeboer et al., 2025). Taken together, these findings highlight the urgent need for research on trauma and PTSD within student populations.
PTSD Treatment and Help-Seeking Barriers in Students
There is ample evidence on the effectiveness of trauma-focused cognitive behavioral therapy (TF-CBT) and eye movement desensitization and reprocessing (EMDR) to treat PTSD in young adults (John-Baptiste Bastien et al., 2020). These two treatments are first choice treatments according to the guidelines (National Institute for Health and Care Excellence, 2018). Nonetheless, in the Netherlands it is estimated that more than 75% of people with PTSD do not receive any professional mental health support, and that among those who receive treatment for PTSD, only 40% receive trauma-focused interventions (Zorginstituut Nederland, 2020).
There is no information on barriers toward help-seeking for PTSD specifically in students, but international research suggests that stigma, lack of awareness about the gravity of one’s traumatization, lack of knowledge about treatment, and underestimation of the symptoms act as barriers for general help-seeking (Ameral et al., 2020; Nobiling & Maykrantz, 2017; Robinson et al., 2016; Vanheusden et al., 2009). In contrast, a recent study revealed that Dutch students experienced little stigma, and this was not a predictor of disclosure or help-seeking; sex was also not found as a predictor of help-seeking (Dopmeijer et al., 2020). Hence, more research is needed into help-seeking behavior, barriers, and treatment gap in Dutch students.
Aim of the Study
The Netherlands lacks up-to-date population-based information regarding exposure to PTEs and PTSD in Dutch students. All the presented Dutch studies were based on self-selected groups (Boskovic et al., 2023; Ministry of Education Culture and Science, 2022; Wellum et al., 2023), or on a population-based sample of the Dutch society (Hoeboer et al., 2025). Hence, the aim of the present paper is to determine the probable lifetime and current (C)PTSD prevalence in a population-based sample of Dutch students, together with exposure to PTEs, help-seeking behavior, treatment history, and help-seeking barriers.
Material and Methods
Design and Participants
A cross-sectional study was performed in Dutch students. The recruitment was realized through the Longitudinal Internet studies for the Social Sciences (LISS) panel, an online household panel administered by Centerdata (Tilburg University, the Netherlands), based on a true probability sample of households and representative of the Dutch population (Centerdata, 2024). The panel operates on an invitation-only basis. Inclusion criteria of the panel are being 16 years or older and speaking Dutch. The panel members can decide which study they want to participate in, and they receive financial compensation after completing a survey.
For the current study, an additional inclusion criterion “being a student” was applied, which required the responders to be subscribed to a secondary vocational education, higher vocational education, or to a university. Before the start of the questionnaires, responders received detailed information about the current research. The study design was exempted from formal review by the Medical Ethics Review Committee of Amsterdam University Medical Centers (Ref.: 2023.0370).
Procedure and Sample Size
All students in the LISS database were invited to the survey. A total of 490 students were invited to take part in the study between September 1 and November 1, 2023. Of those, 373 members responded to the survey (response rate = 76.1%). In total, 93 responders were excluded because they were not students. Of the 280 remaining students, 10 dropped out at the start of the survey and were omitted. Therefore, the final dataset included 270 participants of which the majority (n = 268) completed all questionnaires.
Measures
Participants’ demographic information was retrieved from the LISS panel database. This included sex (“male,” “female,” “other”), gender (“man,” “woman,” “non-binary,” “intersex,” “in another way,” “I don’t know”), age (in years), cultural background (“Dutch,” “first generation foreign western,” “first generation foreign non-western,” “second generation foreign western,” “second generation foreign non-western”), and educational level (“secondary vocational education,” “higher vocational education,” “university”).
Exposure to PTEs
Lifetime exposure to PTEs was measured with the Dutch Standard Self-Report version of the Life Events Checklist for DSM-5 (LEC-5; Weathers et al., 2013), a 16-item self-report checklist of PTEs. For every PTE, participants were asked to indicate in which way they experienced it: self-experienced, experienced as witness, having heard of the event happening to a family member or a close friend, or being exposed as part of their job. In addition to the 16 items, a new item was added, regarding violence in the context of organized crime. This first part of the questions was used to determine lifetime PTE exposure (for participants reporting any kind of exposure to a PTE) and lifetime self-experienced PTE exposure (for participants reporting only self-experiencing a PTE).
Participants were asked to answer a second list of only interpersonal PTEs related specifically to the years of vocational or higher education (from here on referred to as “study years”). This second list contained four items of the LEC-5 (physical assault, assault with a weapon, sexual assault, and other unwanted or uncomfortable sexual experience) and three additional school-related PTEs (online inappropriate behavior, bullying, and other inappropriate behavior). Participants had to report whether they self-experienced those PTEs, and the answers were used to determine PTE exposure during the study years. Participants were also asked in which situation the PTEs happened (school, internship, place of residence, while going out, or somewhere else). Moreover, information about the perpetrators was asked in case of endorsement of interpersonal PTE during the study years (e.g., a teacher, another student, family members, an acquaintance, and a former partner). The PTEs that happened during the study years, and that took place at a school or a stage location, or that had a student or a teacher as perpetrators, were defined as “study-related PTEs.” Responses to the traumatic event (e.g., filling a complaint) were also investigated. When students declared not having taken any action, the possible reasons were explored. See Supplemental Appendix A for a complete overview of the questions and possible answers.
DSM-5 Post-Traumatic Stress Disorder
The Dutch version of the PTSD checklist for DSM-5 (PCL-5; Boeschoten et al., 2014) was used to measure probable current and lifetime PTSD according to the DSM-5 criteria. It contains 20 questions on 5-point Likert scales concerning complaints in the past month and during the lifetime. Total scores were calculated by summing all items (range 0–80 with higher scores reflecting higher symptom severity). Good internal consistency and convergent validity were reported in the Dutch version of the PCL-5 (Hoeboer et al., 2024). A previous study established a cutoff of 29 to be optimal for probable lifetime PTSD diagnosis, and a cutoff of 49 to be optimal for probable current PTSD diagnosis in the general Dutch population (Hoeboer et al., 2025). In the current study, Cronbach’s alphas for both current and lifetime scales were calculated and revealed high internal consistency (.958; .961).
ICD-11 (Complex) PTSD
The Dutch version of the International Trauma Questionnaire (ITQ; Cloitre et al., 2018) was used to measure probable current PTSD and CPTSD according to the ICD-11 criteria. The ITQ contains 18 items on 5-point Likert scales concerning complaints in the past month. It is divided in two major subscales, PTSD and disturbances in self-organization (DSO). Additionally, a last cluster of items assesses functional impairment associated with PTSD and DSO symptoms. For ICD-11 current PTSD, at least one item per symptom cluster in the PTSD subscale has to be scored “moderate” or more severe, and at least one item has to indicate functional impairment due to PTSD symptoms. The diagnosis of probable current CPTSD additionally requires a score of “moderate” or more severe at least in one item per symptom cluster in the DSO subscale, and at least one item has to indicate functional impairment related to DSO. Note that the two ICD-11 diagnoses of PTSD and CPTSD are non-overlapping groups, so those with probable CPTSD are not included in the probable PTSD group. Good internal consistency and convergent validity were reported in the Dutch ITQ (Gerrmann et al., 2023).
Help-Seeking Behavior, Treatment History, and Help-Seeking Barriers
Treatment history, help-seeking barriers, and help-seeking behavior were investigated in participants that reported at least one PTE, using multiple choice questions. Firstly, participants were asked whether they suffered from mental complaints related to a PTE. Secondly, those endorsing the first question were asked if they had sought professional help and what kind of treatment they received. Thirdly, if the participants reported not having sought help, potential reasons were explored. Fourthly, we explored attitude toward future help-seeking in all participants. The reasons for not seeking help in the future were also investigated. See Supplemental Appendix B for a complete overview of the questions.
Statistical Analyses
A detailed preregistration of the analyses can be found at the Open Science Framework (Hoeboer et al., 2023). The prevalence of current and lifetime PTSD, CPTSD, exposure to PTEs, treatment history, help-seeking, and barriers to help-seeking were described using descriptive statistics. T-tests and χ²-tests were calculated to compare demographic, trauma, and help-seeking behavior variables between groups, giving importance specifically to the role of sex. For all analyses, alpha was set at .05 (two-tailed). Analyses were performed with IBM SPSS Statistics Version 28.0.
Results
Demographic Characteristics
Demographic characteristics of the sample are shown in Table 1. The majority (60.0%) of the participants were female. For most of the students of which information about gender was available, sex corresponded with their gender (97.3%). The majority (56.7%) identified as women, 37.4% as men, and 3.0% identified with other genders. Only 3 participants (1.1%) declared to have an “other” sex than female or male and not all the gender categories were sufficiently represented (see Table 1). Therefore, to ensure adequate power of the analyses, only sex differences (i.e., between females and males) were examined. More than half of the participants had a Dutch cultural background (67.8%). The mean age of the sample was 20.74 years (SD = 3.48), and the participants were enrolled at a university (31.1%), higher vocational education (28.5%), or secondary vocational education (17.0%).
Sociodemographic Characteristics of Participants.
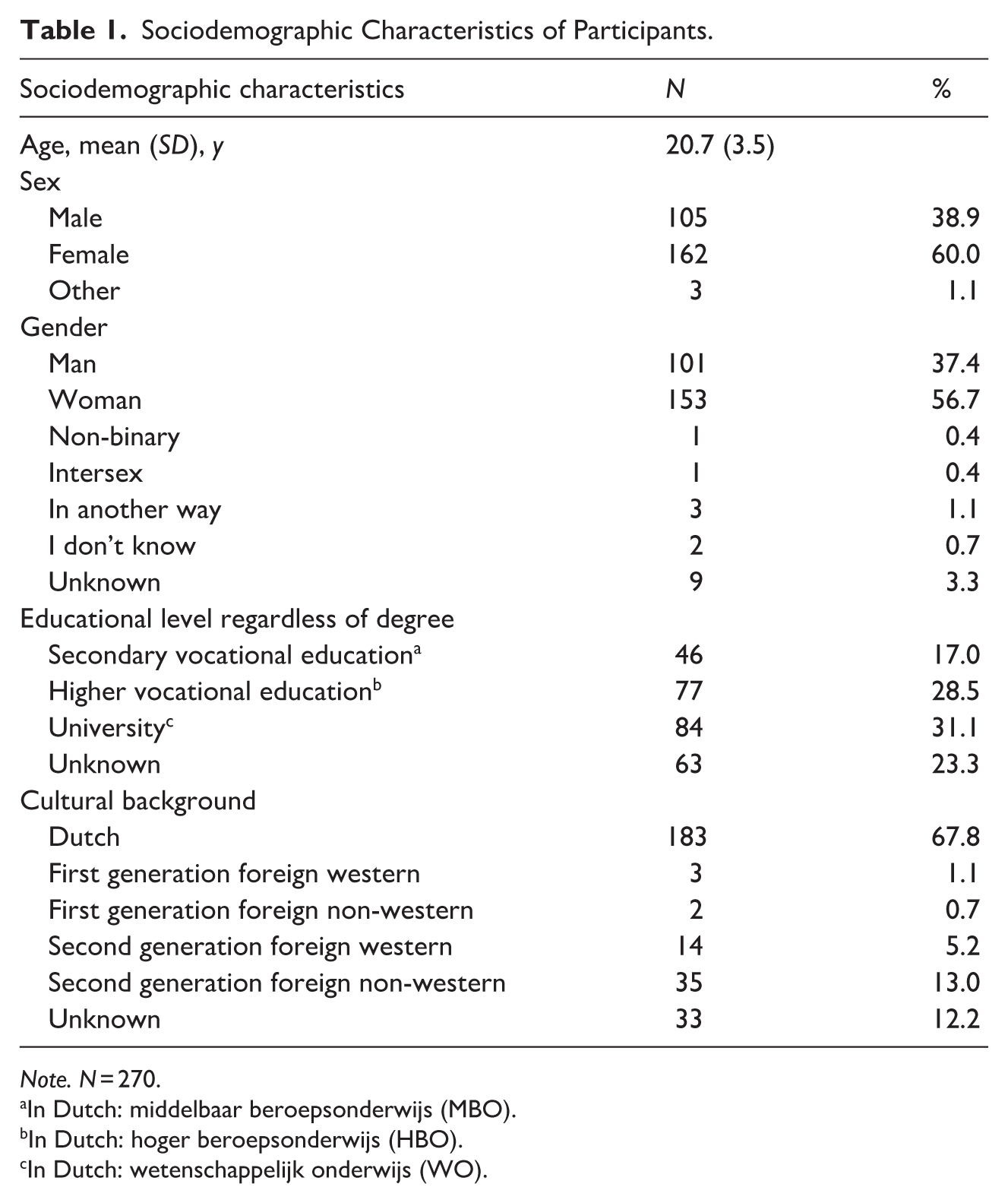
Note. N = 270.
In Dutch: middelbaar beroepsonderwijs (MBO).
In Dutch: hoger beroepsonderwijs (HBO).
In Dutch: wetenschappelijk onderwijs (WO).
Potentially Traumatic Events
The lifetime prevalence of exposure to any PTE was 79.3%. Across all types of exposure, the mean number of types of PTEs endorsed was 5.7 (95% CI [5.1, 6.3]). The most prevalent PTE was a transportation accident (58.5%), followed by life-threatening illness or injury (53.7%), and physical assault (50.0%). No sex difference was found in the number of types of PTEs experienced (t(265) = −0.247, p = .805); however, females (48.1%) were more often exposed to an unwanted or uncomfortable sexual experience than males (35.2%; X2(1, N = 267) = 4.330, p = .037). See Supplemental Appendix C for a complete overview of the lifetime exposure to PTEs in females and males.
The lifetime prevalence of self-experienced PTEs was 51.1%. The mean number of self-experienced PTEs was 1.0 (95% CI [0.8, 1.2]). The most prevalent self-experienced PTE was an unwanted or uncomfortable sexual experience (20.7%), followed by transportation accident (15.9%), and physical assault (13.7%). No sex difference was found in the amount of self-experienced PTEs (t(255.095) = −1.540, p = .125). Males (10.5%) more often experienced a serious accident than females (3.1%; X2(1, N = 267) = 6.176, p = .013), while females more often experienced an unwanted or uncomfortable sexual experience (30.9%; X2(1, N = 267) = 26.538, p < .001) and sexual assault (8.6%; X2(1, N = 267) = 5.133, p = .023) than males (4.8% and 1.9% respectively). Figure 1 shows the lifetime prevalence of any self-experienced PTE in the sample and the sex distribution of self-experienced PTEs.
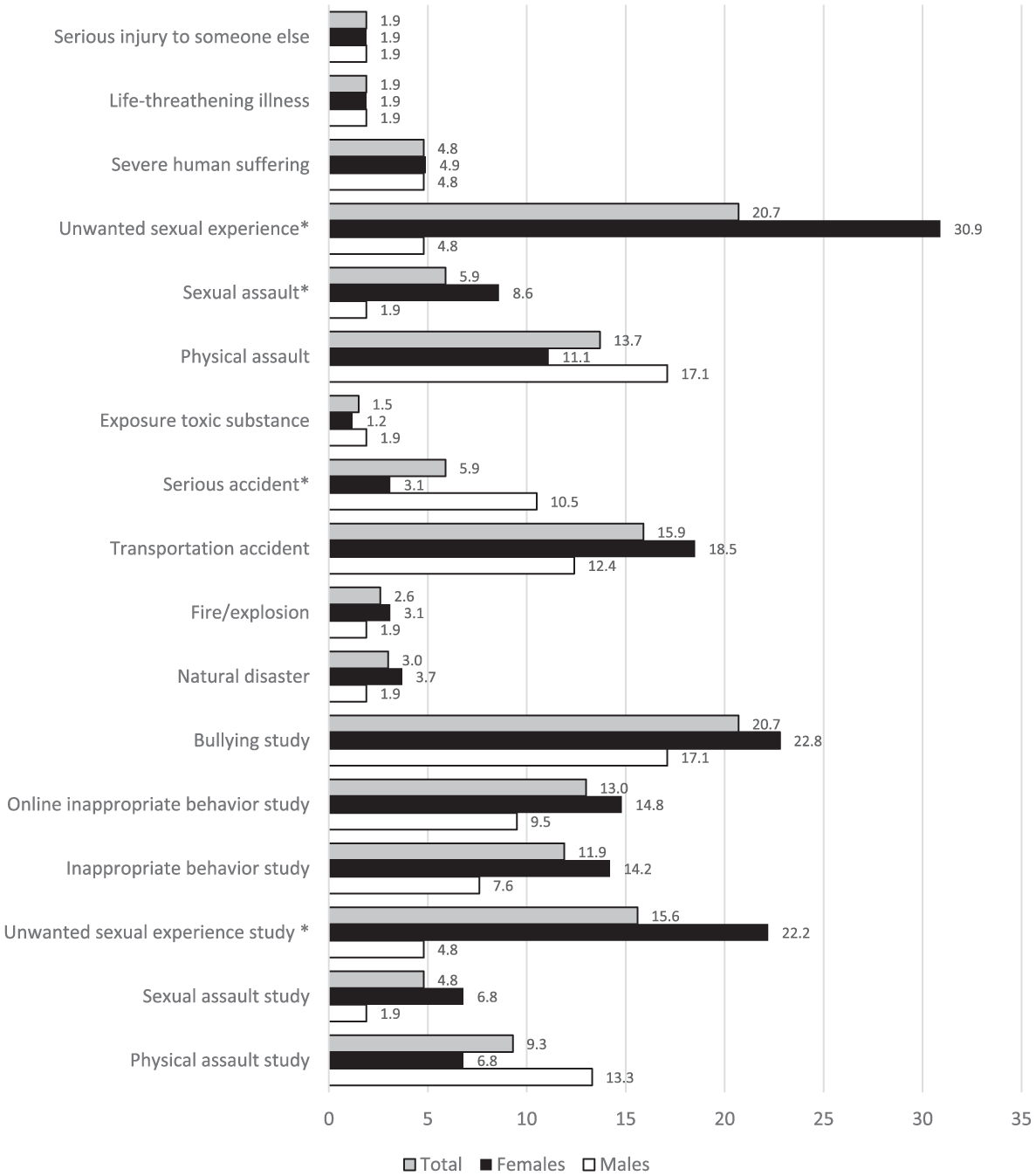
Lifetime exposure (%) of self-experienced PTEs in females and males. For PTEs during the study years, the word “study” is added.
PTEs During the Study Years
For PTEs during the study years, only self-experienced PTEs were investigated. In total 38.9% of the students experienced at least one type of PTE during the study years (M = 0.8; 95% CI [0.6, 0.9]). The most prevalent PTEs were bullying (20.7%) and an unwanted or uncomfortable sexual experience (15.6%). Females (M = 0.9, SD = 1.3) endorsed on average more self-experienced PTEs during the study years than males (M = 0.5, SD = 1.0; t(259.021) = −2.313, p = .022). Females (22.2%) were more often exposed than males (4.8%) to an unwanted or uncomfortable sexual experience during the study years (X2(1, N = 267) = 14.943, p < .001). Figure 1 shows the prevalence of self-experienced PTE during the study years and the sex distribution. A total of 65 students (24.1%) reported experiencing at least one study-related PTE.
Perpetrators
During the study years, bullying (n = 56) was often committed by another student (67.9%), followed by a family member (25.0%), a teacher or a tutor (19.6%), an acquaintance (14.3%), an ex-partner (7.1%), and an unknown offender (7.1%). The remaining investigated PTEs during the study years (n = 147; other unwanted or uncomfortable sexual experience, (online) inappropriate behavior, physical assault, and sexual assault) were most often committed by people unknown to the victim (42.9%), followed by an acquaintance (21.1%), another student (18.4%), a family member (8.1%), an ex-partner (7.5%), a teacher or a tutor (6.8%), a date (6.1%), and someone else (4.1%).
Response After a Study-Related PTE
Among the students who reported at least one study-related PTE (n = 65), 69.2% (n = 45) took action for at least one PTE. These study-related PTEs were grouped into two categories, to ensure adequate sample size for the analyses: study-related bullying (n = 48), and other study-related PTEs (n = 36), including physical assault, sexual assault, other unwanted or uncomfortable sexual experience, and (online) inappropriate behavior.
Of the students that reported experiencing study-related bullying (n = 48), 27 (56.2%) took action. The most common actions were talking to someone outside the institution, confronting the perpetrator, and talking to someone inside the institution. Of the students that reported not taking any action, the most common reasons were not believing that action would be useful, believing that the complaint was not that important, and experiencing a barrier to discuss the complaint. See Supplemental Appendix D for a detailed description of responses and reasons regarding study-related bullying.
A total of 36 students reported experiencing other study-related PTEs, with a total of 42 PTEs reported in these categories. For only 38.1% (n = 16) of the other study-related PTEs, an action was taken. The most common action was facing the perpetrators, followed by talking to someone inside the institution, and reporting the incident to the police. The most common reasons for not reporting the event (n = 26) were believing that nothing would be done, thinking that the complaint was not important, and experiencing a barrier to file or discuss the complaint. See Supplemental Appendix E for a full description of responses and reasons regarding other study-related PTEs.
Prevalence and Risk Factors of (C)PTSD
The estimated lifetime prevalence of DSM-5 PTSD was 22.2%. The estimated current DSM-5 PTSD prevalence was 2.6%. The estimated current prevalence of ICD-11 PTSD was 1.5%. The estimated current prevalence of CPTSD was 4.1%. No significant difference was found in the average age of people with lifetime PTSD (M = 21.2, SD = 3.8) and without lifetime PTSD (M = 20.6, SD = 3.4) (t(268) = −1.1, p = .261). Sex (X2(1, N = 267) = 1.610, p = .204), cultural background (X2(2, N = 270) = .730, p = .694), and educational level (X2(3, N = 270) = 4.380, p = .230) did not emerge as predictors of the diagnosis of lifetime PTSD.
Help-Seeking Behavior, Treatment History, and Help-Seeking Barriers
Of the students with probable lifetime PTSD (n = 60), 61.7% reported complaints related to their index trauma, and 62.2% of those sought help. The most common type of support received was first-line trauma-focused treatment (EMDR, Prolonged Exposure [PE], or CBT; 65.2%), followed by therapy or medication by a psychiatrist (43.5%), support from a coach (39.1%), support from an expert by experience (39.1%), mindfulness or yoga (30.4%), support by a student psychologist (30.4%), medication (26.1%), cognitive therapy (26.1%), support by nurse practitioner (26.1%), therapy that involved movement (8.7%), alternative medicine (8.7%), another treatment (8.7%), treatment from a sexologist (4.3%), stabilization therapies (4.3%), and animal-assisted therapy (4.3%). Two people declared seeking help but not receiving it (8.7%).
Among those who declared not having sought help for their index trauma (n = 14), the most common reasons were wanting to forget about the event (35.7%), being ashamed (28.6%), believing help is not needed (28.6%), preferring informal help (21.4%), not being able to afford help (21.4%), not believing that it would help (21.4%), being too scared (21.4%), feeling that one does not deserve help (21.4%), and not knowing that help was available (14.3%).
The majority (n = 195; 72.2%) of the students indicated that they would seek help in the future when they would develop mental health complaints after exposure to a PTE. Females (77.8%) more often reported the intention to seek help in the future compared to males (63.8%; X2 (1, N = 267) = 6.205, p = .013). The most frequently indicated reason for not seeking help in the future (n = 75) was thinking that they would not need help (52.0%), followed by preferring informal support (30.7%), not believing that it would help them (13.3%), not being able to afford treatment (10.7%), being ashamed to seek help (10.7%), thinking to not deserve help (8.0%), having bad experience in the past (6.7%), and other reasons (4.0%).
Discussion
The aim of the present study was to estimate the prevalences of current and lifetime PTSD and current CPTSD in a population-based sample of Dutch students, their exposure to PTEs, help-seeking behavior, treatment history, and help-seeking barriers.
PTEs and PTSD in Students
We found that 22.2% of the students in our sample had probable DSM-5 lifetime PTSD, 2.6% DSM-5 current PTSD, 1.5% ICD-11 current PTSD, and 4.1% current CPTSD. The estimated prevalences are similar to the findings of other Western studies (Cusack et al., 2019; Elhai et al., 2012; Truskauskaite et al., 2023). Compared with the results of Cusack et al. (2019) concerning DSM-5 probable lifetime PTSD (24.1%), our rates were slightly lower; however, the findings of Cusack et al. (2019) could overestimate the probable prevalence, since the assessment tool used was a 4-item PTSD screener. Conversely, we found slightly higher rates of DSM-5 current PTSD compared to another American study (Elhai et al., 2012), and of ICD-11 PTSD (1.5%) and CPTSD (4.1%) compared to a recent study in Lithuania (4.6%; 3.4%; Truskauskaite et al., 2023). Compared with the general Dutch population (estimated DSM-5 current prevalence 1.3%; estimated DSM-5 lifetime prevalence 11.1%, estimated CPTSD prevalence 1.6%), we found that the estimated prevalences of PTSD and CPTSD in students are substantially higher (Hoeboer et al., 2025).
We found that 79% of the students experienced at least one type of PTE, 51% self-experienced at least one PTE, and 39% of the students self-experienced at least one PTE during the study years. These rates are slightly lower compared to recent findings in the Dutch general population regarding all types of exposure (81.5%) and self-experienced PTEs (55.9%). Note that this study included an additional question for those not endorsing any PTEs, verifying whether they did not experience any stressful event in their life. Compared with other student studies, our findings suggest higher PTE exposure rates than reported in the United States and Lithuania (Cusack et al., 2019; Truskauskaite et al., 2023). We found that transportation accident, life-threatening illness, and physical assault were the most commonly reported PTEs, and the most prevalent self-experienced PTEs were unwanted or uncomfortable sexual experience, transportation accident, and physical assault. During the study years, the most prevalent self-experienced PTEs were bullying and unwanted or uncomfortable sexual experiences. Thus, our findings suggest that the prevalence of probable PTSD and CPTSD is higher in students than the general population, despite similar overall exposure to PTEs.
Unknown perpetrators, other students, and acquaintances were the most frequently reported offenders across the groups of PTEs. We found that 24% of the students experienced at least one study-related PTE, and 69% of these students undertook action. Among those who reported experiencing study-related PTEs, three-quarters were exposed to bullying, and over half were exposed to other PTEs. For only less than half of those PTEs, an action was taken. This proportion is higher than what was found in Dutch universities, where 25% to 35% of students reported taking no action after exposure to sexual assault (Wellum et al., 2023). The most common actions across study-related PTEs were facing the perpetrators themselves and talking to someone inside or outside the institution. These results partially align with previous findings on Dutch students: Consistently with our findings, talking about the PTE with friends was reported by 28% to 57% of the participants; conversely, confronting the perpetrators was reported only by 14% to 21% of the students, which is lower than what we found (Wellum et al., 2023). Across study-related PTEs, people who did not report the event most commonly believed that nothing would be done or thought that the complaint was not important. This is in line with the latest findings of Ameral et al. (2020).
We did not identify demographic variables predicting probable lifetime PTSD in our sample. These results are in contrast with previous studies which found that sex and cultural background were risk factors for PTSD (Hoeboer et al., 2025; Truskauskaite et al., 2023). However, we observed some sex differences in the amount of self-experienced PTEs: Females self-experienced almost twice as many PTEs during study years compared to males (0.9 vs. 0.5). Moreover, males were more often self-exposed to serious accidents; females were more often (self-)exposed to unwanted sexual experiences (during study years and overall) and sexual assault. These sex differences are in line with the previous studies, where sexual violence was more often reported by females and serious accidents by males (de Vries & Olff, 2009; Hoeboer et al., 2025). Finally, specifically considering unwanted sexual experiences and sexual violence, our results are consistent with recent studies and reports in the Netherlands which showed that, in students, females are more often exposed to sexual assault and sexual inappropriate behaviors than males (van Berlo, 2022; Wellum et al., 2023). Thus, probable lifetime PTSD diagnosis does not seem to be influenced by sex in Dutch students, while in the Dutch general population female sex is a risk factor (Hoeboer et al., 2025). A possible explanation could be that in older generations, stigma about mental health is stronger in males. A recent scoping review examined men’s experiences of stigma across the lifetime, and found different themes associated with stigma experiences in men (McKenzie et al., 2022). Alternatively, we might have lacked sufficient power in the current study to identify sex differences.
Help-Seeking, Treatment History, and Barriers in Students
More than half of the students with probable lifetime PTSD and complaints reported that they sought professional help at least once. The most common type of treatment received was first-line trauma-focused treatment, followed by therapy or medication by a psychiatrist. The guidelines for the treatment of PTSD in adolescents suggest TF-CBT as first-line treatment, followed by EMDR therapy (National Institute for Health and Care Excellence, 2018). According to our results, 75% of students with probable lifetime PTSD did not receive these treatments. Among those who developed symptoms and declared not having sought help, wanting to forget about the event, being ashamed, and believing one does not need help were the most frequently reported reasons. These results are in line with recent studies in students identifying avoidance, stigma, and lack of awareness and knowledge about treatment as barriers influencing help-seeking (Dopmeijer et al., 2020; Dunley & Papadopoulos, 2019; Nobiling & Maykrantz, 2017; Robinson et al., 2016).
We have not found sex differences in help-seeking behavior in students with lifetime PTSD, in contrast with previous results (Li et al., 2016). An explanation is that sex-related stigma may have weakened in recent years (Dopmeijer et al., 2020). Nevertheless, we found that females more often reported the intention to seek help in the future compared to men. This confirms results on non-clinical student samples (Li et al., 2016). Reported reasons for refraining from seeking professional help in the future included believing to not need help, preferring informal support, and a disbelief that professional help is effective. Once again, lack of awareness and knowledge about mental health disorders and wrong beliefs about treatment played a role in determining the help-seeking attitude, confirming the literature findings (Dopmeijer et al., 2020; Vanheusden et al., 2009). These results suggest that even though students tend to seek help, some of them still experience significant barriers. According to our results, there is still a lack of knowledge about PTSD, available treatments, and treatment outcomes.
Limitations
Our study has several limitations. Firstly, retrospective self-report questionnaires were used to measure PTEs and PTSD, so results may be influenced by social desirability or recall bias (Althubaiti, 2016; Van de Mortel, 2008). Secondly, although our sample was representative of the Dutch student population respecting sex, age, and cultural background (CBS, 2022, 2023), educational level appeared to be less well represented: While the proportion of students in higher vocational education (37%) was comparable to the data from the Ministry of Education (36%), students in secondary vocational education were underrepresented (22% vs. 37%), and university students were overrepresented (41% vs. 27%; Ministry of Education Culture and Science, 2023). Thirdly, information about reports, treatment received, and barriers was collected via closed-ended answers, while open-ended qualitative data would have helped to give a better representation of the treatment gap and the barriers toward help-seeking. Fourthly, we were unable to compare different kinds of PTEs that happened during the study years because of sample size reasons.
Despite the limitations, our research is the first prevalence study in Dutch students using a population-based sample, providing a first indication of the prevalence of probable DSM-5 and ICD-11 PTSD and CPTSD in this population, together with information about treatment gap, treatment history, help-seeking behavior, and help-seeking barriers. Unlike previous studies which usually focused on a specific student subgroups, usually college students or University students (Ameral et al., 2020; Cusack et al., 2019; Dopmeijer et al., 2020; Idoiaga et al., 2022), we included a diverse sample of students in terms of sex, cultural background, and type of higher education. Hence, our results generalize well to the general student population. We also tested whether diversity-related variables predicted higher risk of PTEs and PTSD, which appeared to be the case for females. This is important information for targeted (preventive) interventions.
Implications
Our results have four main implications. Firstly, the priority should be to increase knowledge and thus to educate students about PTEs, PTSD, and treatment; students should be informed through media and through preventive interventions at school about treatment options and outcomes, mental health, PTEs, and consequences of PTSD on both daily and student life. Social media has been demonstrated to be a powerful source of information and education on mental health in adolescents (O’Reilly et al., 2019). Students should become aware of professional help and how to access it. For example, given the high prevalence of unwanted sexual experiences, students should be made aware of the existence of specific centers for sexual violence (e.g., “Centrum Seksueel Geweld in the Netherlands”), with an emergency number to call in case of need and an online chat service. Psychosocial education on these topics can be given in schools to achieve this goal. Psychoeducation has been shown to increase access to care and symptom awareness (Savell et al., 2024).
Secondly, school staff should enhance awareness and attention to mental health disorders to reduce stigma and discuss negative treatment beliefs; to reach this goal, they should also receive training and instruction on the topic of interpersonal violence at school and how to intervene in problematic situations (Wichmann et al., 2023). Furthermore, it should be ensured that students are well-informed about how to file a complaint (e.g., inside or outside the study institution), who are the involved subjects, what are the options inside and outside the school institutions (e.g., formal complaint, police report), what the process of filing a complaint entails, and what are the consequences for the perpetrators.
Thirdly, the focus should also be on preventing unwanted sexual experiences and bullying in the study environment, since they seem to be highly prevalent PTEs during the study years. Literature has shown that various preventive interventions can reduce sexual violence and sexual victimization: for example, using an ecological framing of sexual violence and training the school staff to provide institutional-level prevention and guidance to students, teaching positive models of consent and respect, and increasing collective awareness (Basile, 2015; Sales & Krause, 2017). Moreover, prevention should begin at home, in the media, and in the society, teaching children rules of respect and safety (van Berlo, 2022). Prevention should start early, before youngsters engage in sexual relationships (van Berlo, 2022). Finally, unwanted and uncomfortable sexual experiences are more common in females: This should be taken into account when formulating health policies.
Regarding bullying, research has presented different successful programs and interventions for its prevention, ranging from school policies to tools and resources such as advisors (Cismaru & Cismaru, 2018). Specifically in the Netherlands, several programs are available and effective, including the PRIMA program and the KiVa program (Huitsing et al., 2020; van Verseveld et al., 2019). The PRIMA program consists of lessons for all year groups, an e-learning and training program for school staff, a monitoring tool to keep track of cases of bullying and students at risk, and action protocols for various bullying situations (van Verseveld et al., 2019). The KiVa program is composed of a prevention part, with lessons delivered by teachers and targeted at all students, and an intervention part, with actions targeted at ongoing bullying by a specialized KiVa team (Huitsing et al., 2020). Nevertheless, schools require support and guidance in following and starting these programs, to avoid a decrease of participation in the long term (Nationaal Regieorgaan Onderwijsonderzoek, 2018; Sainio et al., 2020). Overall, these results highlight the importance of programs aimed at preventing interpersonal violence to reduce the impact of the otherwise long-lasting victimization (Graham et al., 2019; Mengo & Black, 2016).
Fourthly, students’ advisors and psychologists should be trained in screening instruments and guidelines for PTSD and related symptomatology, in order to recognize PTSD early.
Conclusion
Our results indicate that PTSD is more common in Dutch students than in the general population (Hoeboer et al., 2025). Only about 38% of students sought help, and 65% of them received first-line trauma treatment. Thus, the treatment gap is substantial. Barriers toward help-seeking were related to avoidance, stigma, lack of knowledge, and disbeliefs about therapy. After exposure to study-related PTEs, some students did not take any action. The main reasons for not reporting the event were related to the disbelief that the complaint would have a consequence, thinking that the complaint was not important, or experiencing a barrier in submitting the complaint. Our results underscore the importance of preventive interventions aimed at increasing knowledge in students about PTSD, providing information, support, and indications about treatment options, preventing exposure to PTEs, and recognizing early PTSD symptoms, to raise awareness and reduce the treatment gap.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251414109 – Supplemental material for Higher Education Students and Trauma: PTSD, Treatment Gap and Help-Seeking Challenges
Supplemental material, sj-docx-1-jiv-10.1177_08862605251414109 for Higher Education Students and Trauma: PTSD, Treatment Gap and Help-Seeking Challenges by Federica Nava, Chris M. Hoeboer, Joris F. G. Haagen and Miranda Olff in Journal of Interpersonal Violence
Footnotes
Ethical Considerations
The study design was exempted from formal review by the Medical Ethics Review Committee of Amsterdam University Medical Centers (Ref.: 2023.0370).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
Federica Nava: Data curation, Formal analysis, Writing original draft. Chris M. Hoeboer: Conceptualization, Funding acquisition, Methodology, Supervision, Writing review & editing. Joris F. G. Haagen: Conceptualization, Funding acquisition, Methodology, Writing review & editing. Miranda Olff: Conceptualization, Funding acquisition, Methodology, Writing review & editing.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The research was made possible in part by a grant from the Spinoza Fonds, part of the Amsterdams Universiteitsfonds. This study was also funded by ARQ National Psychotrauma Centre.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Data Availability Statement
All pseudo anonymous data will be available via the LISS Panel Data Archive.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.