
Abstract
Sexual and gender minority (SGM) adults in South Africa face high levels of violence and poor mental health outcomes. Interventions to prevent these negative health implications are hampered by a lack of representative data among this population. This study aims to quantify the associations between three forms of violent victimization and depressive symptoms in a sub-sample of SGM drawn from a population-based cross-sectional study in Gauteng, South Africa. Data come from the sixth Quality of Life survey conducted in South Africa’s Gauteng province. Brief screeners assessed childhood sexual abuse (CSA), past-year intimate partner violence (IPV), non-partner violence, and depressive symptoms. Three survey-weighted logistic regression analyses were fit to model associations between elevated depressive symptoms and CSA, past-year IPV, and past-year non-partner violence, controlling for socio-demographics (age, race, sex, area of residence, education, socioeconomic status, and recent employment). N = 1,328 SGM respondents were included. Over 40% (n = 537) reported depressive symptoms, while 17% (n = 222) reported CSA, 5% (n = 67) reported IPV, and 16% (n = 208) reported non-partner violence. CSA and non-partner violence were associated with significantly higher odds of reporting depressive symptoms (aOR: 1.51, 95% CI [1.03, 2.23]; aOR: 1.84, [1.24, 2.73], respectively). IPV was not associated with elevated depressive symptoms (aOR: 1.17, [0.64, 2.16]). In all models, employment in the past 7 days was associated with significantly lower odds of reporting depressive symptoms. Recent and childhood violence is a major burden that is associated with elevated symptoms of depression among SGM in urban South Africa. Community-tailored interventions and policy-related advocacy related to employment and violence prevention may alleviate depressive symptoms in SGM adults in Gauteng.
Introduction
There is broad scientific consensus that sexual and gender minority (SGM) communities, especially those consisting of lesbian, gay, bisexual, transgender, queer, and intersex individuals, face worse mental health outcomes than cisgender and heterosexual communities (American Psychiatric Association, 2017; Semlyen et al., 2016; The Trevor Project, 2021; World Health Organization, 2023). Broadly speaking, SGM individuals are more than twice as likely as cisgender, heterosexual men, and women to experience a diagnosed mental health disorder in their lifetimes (American Psychiatric Association, 2017; Semlyen et al., 2016). Too often, undiagnosed and untreated mental illness leads SGM individuals to consider ending their lives, with recent evidence suggesting that 42% of SGM youth (and over half of transgender youth) in the United States considered suicide in the past year (The Trevor Project, 2021). While its effect is beyond the scope of this paper, the COVID-19 pandemic worsened these disparities (Hawke et al., 2021; Salerno et al., 2020, 2023; The Trevor Project, 2021) and reduced access to critical mental health care for this population, compounding the negative impacts of poor mental health effect (Ormiston & Williams, 2022; The Trevor Project, 2021).
Depression is the most common mental illness and is the 13th largest contributor to morbidity worldwide (Ferrari et al., 2022). Within the broader constellation of mental illness, SGM people experience a disproportionate burden of depressive symptoms when compared to their cisgender and heterosexual counterparts (McNeil et al., 2017; Plöderl & Tremblay, 2015; Su et al., 2016). The large global burden of depression and its disproportionate effect on SGM people makes understanding the drivers of the increased rates of depression among SGM people especially important to uncover, as these can lead to points of intervention to reduce its burden in this population.
The prevailing theoretical explanation for disparities in depressive symptoms among SGM individuals is the Minority Stress Theory (Meyer, 1995, 2003). Minority Stress Theory maintains that specific and unique stressors arise from experiences of discrimination, prejudice, and stigma related to identifying with a sexual and/or gender identity in a heterosexist society. These stressors have consistently been associated with higher rates of depression among all categories of sexual and gender minorities (Bowleg et al., 2003; Jefferson et al., 2013; Lattanner et al., 2022; Lytle et al., 2016; Newcomb et al., 2012; Norcini Pala et al., 2015; Sarno et al., 2020; Testa et al., 2017). The mechanisms uncovered by these studies and others find that persistent challenges faced by these individuals, including social rejection, internalized heterosexism, enacted discrimination (e.g., hate crimes, violence, individual and societal prejudice), and identity concealment, can contribute to chronic stress that significantly impacts mental health. However, the majority of this literature uses samples from the Global North, with a paucity of studies examining how these constructs may affect SGM in the Global South differently. For example, due in part to the availability of affirming mental health service providers, minority stressors are thought to lead to poorer mental health outcomes and increased mental health service utilization among SGM compared to non-SGM individuals in many high-income contexts (McNamara & Wilson, 2020; Ormiston & Williams, 2022). However, these same drivers lead to significantly lower mental health services use among SGM in the Global South, due largely to the fear of even more discrimination from health care providers (World Health Organization, 2023).
South Africa is the only country in Africa to legalize same-sex marriage, provide full employment discrimination protections for SGM, and have a National Strategy for SGM people (South African National AIDS Council, 2016). Despite these progressive policies and an increasing social acceptance of those identifying as SGM, the enforcement and implementation of these laws can vary across the country (Williams Institute, 2021). Moreover, persistent negative social norms regarding homosexuality and gender diversity are pervasive among many South Africans and often lead to poor mental health (McAdams-Mahmoud et al., 2014; Stephenson et al., 2021). In a 2018 report using a representative sample, 70% of South Africans reported that homosexual sex and breaking gender dressing norms is simply “wrong” and “disgusting” (The Other Foundation & Human Sciences Research Council of South Africa, 2018). This illustrates the underlying and deeply entrenched social norms regarding SGM communities in South Africa. In addition, South Africa also exhibited one of the world’s highest rates of violence against SGM people (Statistics of South Africa, 2020) and witnessed a rash of high-profile violence against SGM people in late 2021 (Reid, 2022). Three specific forms of violence against SGM people: childhood sexual abuse (CSA; Balsam et al., 2010; Xu & Zheng, 2015) intimate partner violence (IPV; Bukowski et al., 2019; Miltz et al., 2019; Reuter et al., 2017) and violence experienced by non-partners (Almeida et al., 2009; Nadal, 2019) have all been found to be associated with elevated depressive symptoms in SGM samples outside South Africa. However, despite a clear need for a better understanding of how these forms of violence affect mental health outcomes in SGM South Africans, little is known about how different forms of violent victimization are associated with elevated depressive symptoms among SGM populations within South Africa.
One reason for the lack of robust data is that most research among SGM populations in South Africa has so far focused on convenience or venue-based samples of men who have sex with men (Chard et al., 2017; Cloete et al., 2008; Lane et al., 2014; McAdams-Mahmoud et al., 2014; Metheny et al., 2022; Stephenson et al., 2020, 2021). These studies find that the prevalence of IPV is high in these communities (Stephenson et al., 2020) and that these experiences of violence are associated with depressive symptomatology (Metheny et al., 2022) and sexual risk-taking behaviors (Lane et al., 2014). Despite these findings, critical gaps remain in understanding the health disparities regarding this population and research on associations between violence and mental health in the broader SGM community in South Africa is lacking and requires further exploration. Moreover, convenience sampling is likely to overrepresent participants who feel safe and comfortable participating in research targeting SGM populations or have the time, literacy, or means to participate (Owens et al., 2020). However, existing population-based studies such as the South African Demographic and Health Surveys and other surveys conducted by Statistics South Africa do not include sexual orientation and gender identity (SOGI) variables, precluding the ability to analyze this data in SGM sub-samples (Mkhize et al., 2023)
In this analysis, we extend the evidence based on the associations between enacted discrimination (as measured by violent victimization) in South Africa by using SGM-identified participants from a representative sample and population-based survey in the Gauteng Province of South Africa. This study proposes to explore cross-sectional associations between three forms of violence (CSA, IPV, and non-partner violence) and elevated depressive symptoms among SGM respondents. Drawing on previous literature, we hypothesize that all three forms of violence will be independently associated with greater odds of depressive symptoms. Understanding whether (and how) these experiences are associated with depressive symptoms may illuminate specific points of intervention to improve mental health in SGM South African communities.
Methods
Data
Data for this analysis comes from the self-identified SGM respondents of the 2020–2021 Quality of Life Survey, a population-representative survey led by the Gauteng City-Region Observatory (GCRO; de Kadt et al., 2021). The Quality of Life survey has been conducted every 2 years since 2009 and includes all administrative units (i.e., wards) within Gauteng Province. In addition to being home to the country’s largest urban centers of Johannesburg and Pretoria, Gauteng is the most densely populated South African province and comprises inner-city, suburban, and industrial areas as well as rapidly growing informal and peri-urban settlements (Statistics South Africa, 2023).
The sixth edition of the Quality of Life survey interviewed 13,616 adults aged 18 years and older across all 529 wards in Gauteng between October 2020 and May 2021 using multistage stratified cluster sampling. In total, at least 20 interviews were conducted in each ward. Data collected was weighted by population size, race, and sex to ensure representative estimates at the ward, municipal, and provincial levels. Full methodological and sampling strategies for the Quality of Life survey are published elsewhere (de Kadt et al., 2021).
All study materials were translated into nine local languages, and respondents were interviewed in the language of their choice. Interviews were conducted in person by trained enumerators following verbal informed consent. An additional self-complete section on gender identity, sexual/romantic attraction, and experiences of violence was included for the first time in the sixth edition of the Quality of Life survey. The SOGI-related questions were included as part of advocating for the recognition of SGM individuals and ultimately quantify instances of othering encountered by members of the SGM community. The analysis is limited to those who participated in the self-complete section and indicated they identified as an SGM by answering two questions regarding (a) their own gender (male, female, gender-diverse) and (b) the gender of those to whom they are attracted. While n = 25 respondents identified as “gender diverse,” this small sample size precluded inclusion as its own category. Therefore, those responding as gender diverse or with same-sex attraction were considered SGM respondents. This resulted in N = 1,328 SGM respondents or 9.75% of the total sample that participated in the self-complete section. Ethical approval for the Quality of Life survey was secured from the Human Research Ethics Committee of the University of the Witwatersrand, Johannesburg.
Measures
Measures were chosen in consultation with the Queering Social Survey Research team at GCRO and reflect the constructs of interest and those indicated in the literature to be associated with violence and depressive symptoms in SGM populations.
Age was categorized into 5-year groups, and gender was based on the respondent’s gender identity as indicated in the SOGI questionnaire. Race was categorized into common South African census categories as Black African, White, Colored, Indian/Asian, or Other. Due to limited sample sizes of the latter three categories, these were combined for analyses. Education was dichotomized, measuring whether the respondent completed secondary school. Secondary school was chosen as the cutoff, given previous evidence that this is the amount of schooling that usually confers more egalitarian gender norms (Karam, 2013). Given the high rate of unemployment and underemployment in Gauteng (32.7%; Statistics South Africa, 2023) and its demonstrated effect on depressive symptoms (Amiri, 2022) and violence via financial strain (Umukoro & Okurame, 2023), Employment was measured via a dichotomous variable indicating whether respondents had been paid for any type of work in the past 7 days. Immigration status was dichotomized depending on whether the respondent was born in South Africa and is pertinent given the influx of refugees currently facing South Africa (United Nations High Commission on Refugees, 2023). Socioeconomic status was assessed using a weighted measure of coverage by medical insurance, highest level of education completed, working internet access in the home, employment status, and household income that ranged from 1 to 10 on a continuous scale. This was categorized into tertiles (low [<3.34], medium [3.34–6.77], and high [>6.77]). Since sample size limitations at the administrative unit level precluded the consideration of neighborhood as a random effect, municipality (Ekurhuleni, Johannesburg, Tshwane, Sedibeng, West Rand) was included as a fixed effect to account for the clustered nature of the data.
CSA was assessed using two items from the four-factor Childhood Trauma Questionnaire (Bernstein et al., 1997). Respondents were asked behaviorally specific questions about whether, before the age of 18, anyone forced them to touch genitals (“Someone touched my genitals or made me touch their genitals when I did not want them to” characterized as molestation), or physically forced or threatened them into to having sexual intercourse (“Someone had sex with me because I was frightened, threatened or forced.” characterized as rape). IPV was measured using items from the World Health Organization’s (WHO) Multi-Country Study Instrument (Garcia-Moreno et al., 2005). IPV included reports of physical violence (hitting, kicking, threats, or use of a weapon to intimidate) and/or sexual violence (forced sex by a current or former partner). Low prevalence of sexual violence in this sample precluded the separate analyses of these forms of violence. Non-partner violence was assessed using the same items as IPV but changed slightly to refer to anyone except an intimate partner. Physical and sexual violence were again combined for consistency and due to low sample size for non-partner sexual violence.
Depressive symptoms were assessed using the two-item shortened version of the Patient Health Questionnaire-2 (PHQ-2), which has been validated in South Africa (Bhana et al., 2015) and elsewhere (Löwe et al., 2005). This brief screening tool asks about the frequency of two symptoms over the past 2 weeks ((a) feeling down, depressed, and hopeless and (b) losing pleasure or interest in doing things) with responses ranging on a Likert scale of 0 (not at all), 1 (a few days), 2 (more than half the days), and 3 (nearly every day). With combined scores for the two questions ranging from 0 to 6, the PHQ-2 score of two or more has been shown to have good sensitivity and adequate specificity that suggests probable depression (Levis et al., 2020; Mkhize & Hamann, 2022). Although PHQ-2 is not a diagnostic measure of clinical depression, it is appropriate as a screening tool for population-based evidence of depressive symptoms.
Analysis
After data cleaning and categorization as described above, descriptive statistics were tallied, and correlation analyses were run on Stata 16 to gauge potential for multicollinearity. Given high levels of correlation between the types of violence experienced by respondents, it was determined that separate regression models examining the associations between each type of violence and depressive symptoms were warranted. Therefore, three logistic regression analyses with depressive symptoms as a binary outcome (i.e., PHQ-2 ≥ 2) were fit. All three models used the survey (svy:) commands to adjust for data clustering by ward and to account for differentiation in sampling strategies. Each of the three models included all covariates mentioned above (age, race, education, unemployment, socioeconomic status, employment status, and immigration status). All three models were identical except for the form of violence (CSA, IPV, or non-partner violence) assessed.
Results
A total of 1,328 SGM respondents were included in the analyses and ranged in age from 18 to 90 years old (Mean [M] = 38.21, SD = 13.66). While the full Quality of Life survey is representative of the Gauteng population, the SGM sub-sample merely excises the SGM-identifying respondents from this survey. This resulted in Black Africans and those of lower socioeconomic status being slightly overrepresented, comprising nearly 91% (n = 1,207) and 70% (n = 929) of the sample, respectively, compared to 81% and 55% (x2 < 0.000) in the full sample. Half of the SGM respondents (50%, n = 662) completed secondary school compared to 60% (n = 5,985) of non-SGM respondents (x2 < 0.000). Nearly 1 in 10 SGM and non-SGM respondents (9%, n = 125; 9%, n = 990, respectively) were born outside South Africa. More than 40% of SGM respondents (n = 537) indicated depressive symptoms, which was not significantly different from non-SGM respondents (38%, n = 3,806; x2 = 0.127). Significantly larger percentages of SGM respondents reported CSA (17%, n = 222 SGM; 10%, n = 983 non-SGM; x2 < 0.000), past-year IPV (5%, n = 67 SGM; 3%, n = 299; x2 < 0.000), and past-year non-partner violence (16%, n = 208 SGM, 12%, n = 1,207 non-SGM, x2 < 0.000) compared to non-SGM respondents. Full descriptive results are shown in Table 1.
Sample Characteristics.
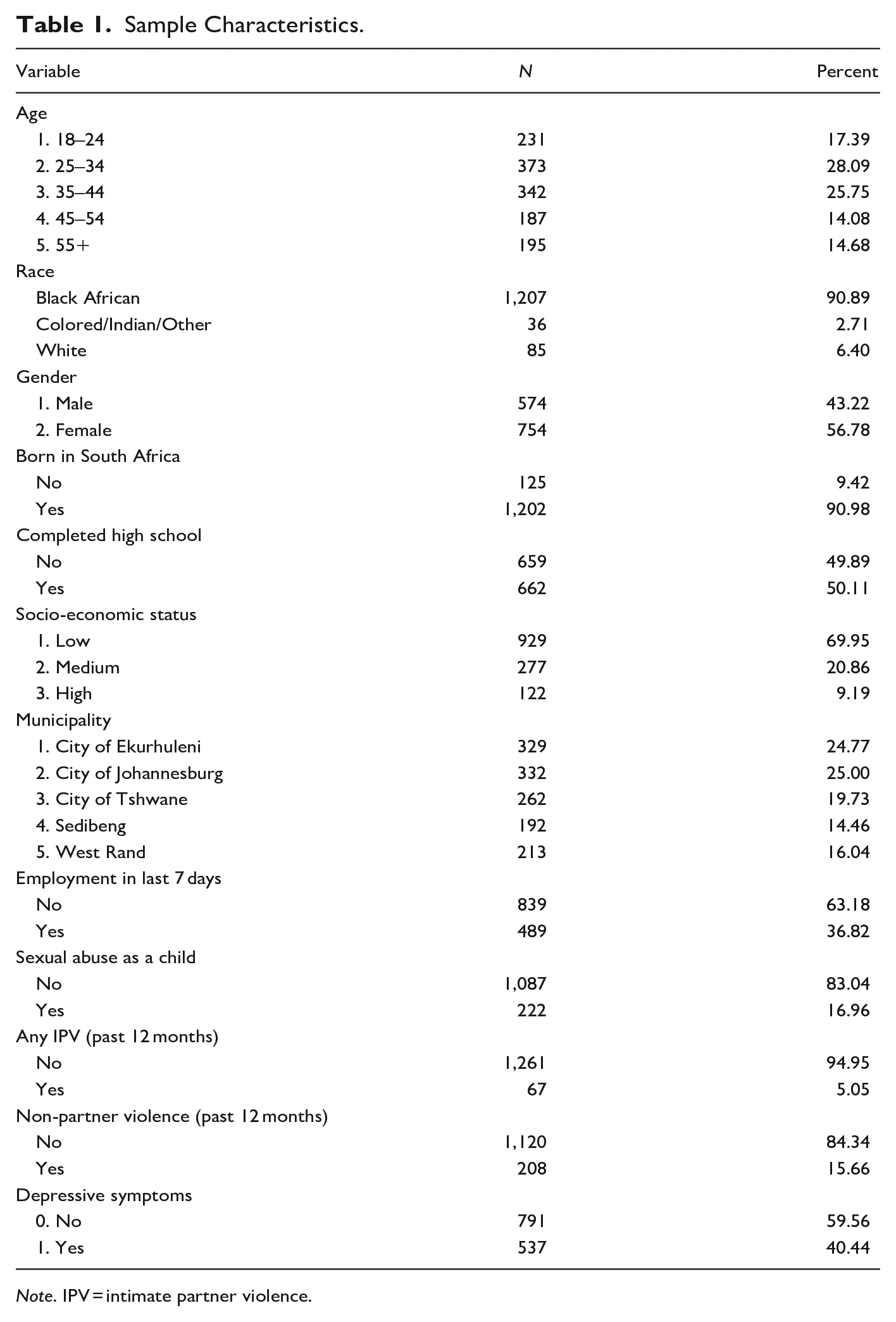
Note. IPV = intimate partner violence.
Model 1: CSA: A total of 222 (17%) reported one or both forms of CSA measured in the survey. Respondents aged 35 to 44 and those aged 55+ had 1.662 (95% confidence interval [CI] [1.049, 2.632], p-value [p] = .03) and 2.292 ([1.355, 3.878], p < .000) times the odds of reporting depressive symptoms compared to those aged 18 to 24, respectively (see Table 2). Those who indicated paid work in the past 7 days (adjusted odds ratio [aOR]: 0.667, [0.479, 0.928], p = .016) had significantly lower odds of depressive symptoms. Controlling for all other variables, experiencing CSA was associated with significantly higher odds of depressive symptoms (aOR: 1.513, [1.028, 2.228], p = .036). Odds ratios for other covariates were not statistically significant when adjusted for all other variables.
Associations Between Childhood Sexual Abuse and Depressive Symptomatology.
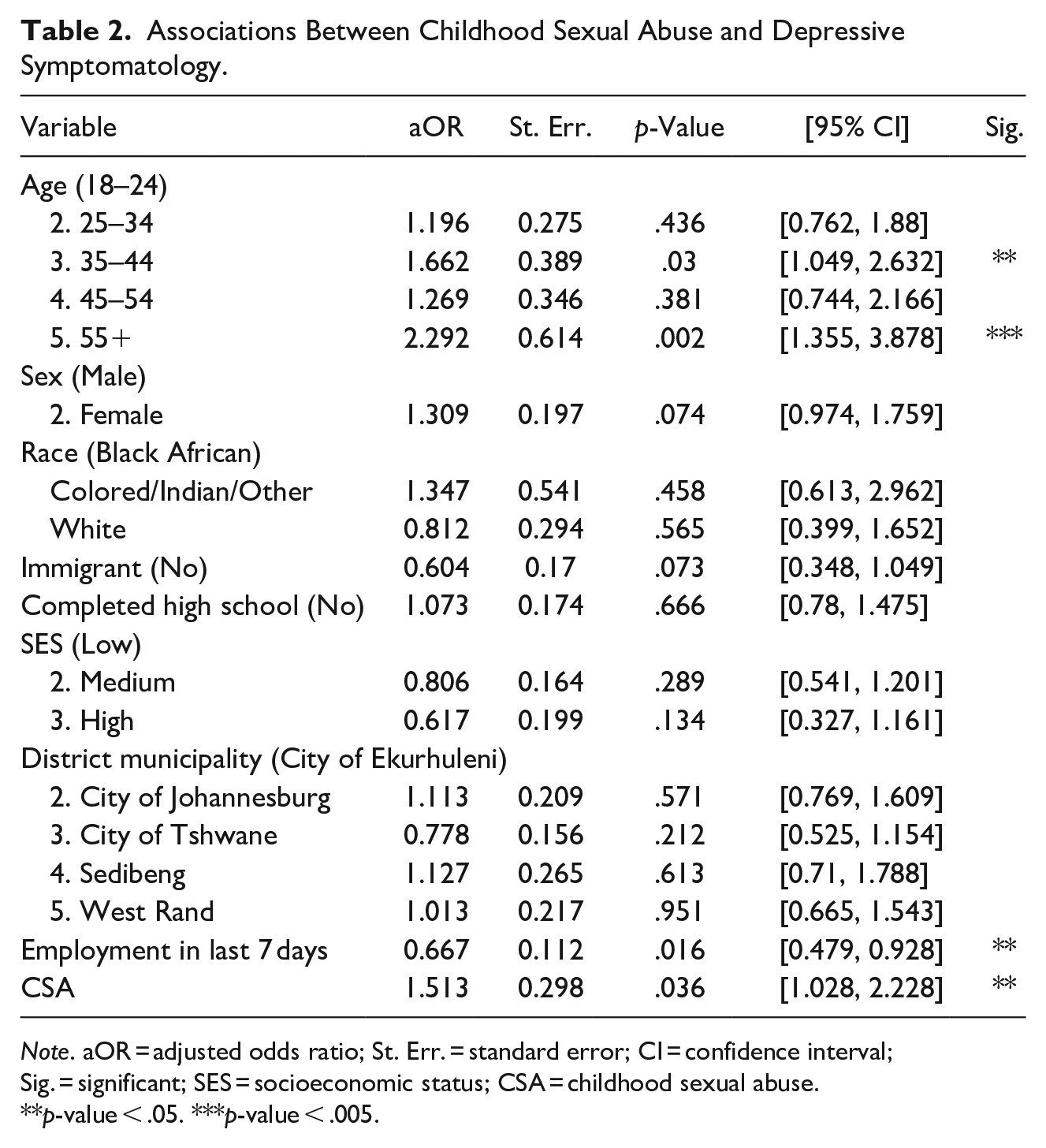
Note. aOR = adjusted odds ratio; St. Err. = standard error; CI = confidence interval; Sig. = significant; SES = socioeconomic status; CSA = childhood sexual abuse.
p-value < .05. ***p-value < .005.
Model 2: Past-year IPV: Among all SGM respondents, 5% (n = 67) reported IPV in the past 12 months. Like Model 1 (CSA), respondents aged 35 to 44 and those aged 55+ had significantly higher odds of depressive symptoms compared to those aged 18 to 24 (35–44: aOR: 1.609, 95% CI [1.023, 2.53], p = .039; 55+: aOR: 2.46, [2.156, 3.608], p = .003; see Table 3). Those employed in the past 7 days had significantly lower odds of reporting depressive symptoms (aOR: 0.686, [0.495, 0.95], p = .024). The adjusted association between past-year IPV and elevated depressive symptoms was directionally congruent with the other forms of violence but did not reach statistical significance at α = .05 (aOR: 1.17, [0.64, 2.16], p = .599). Odds ratios for other covariates were not statistically significant when adjusted for all other variables.
Associations Between Past-Year Intimate Partner Violence and Depressive Symptomatology.
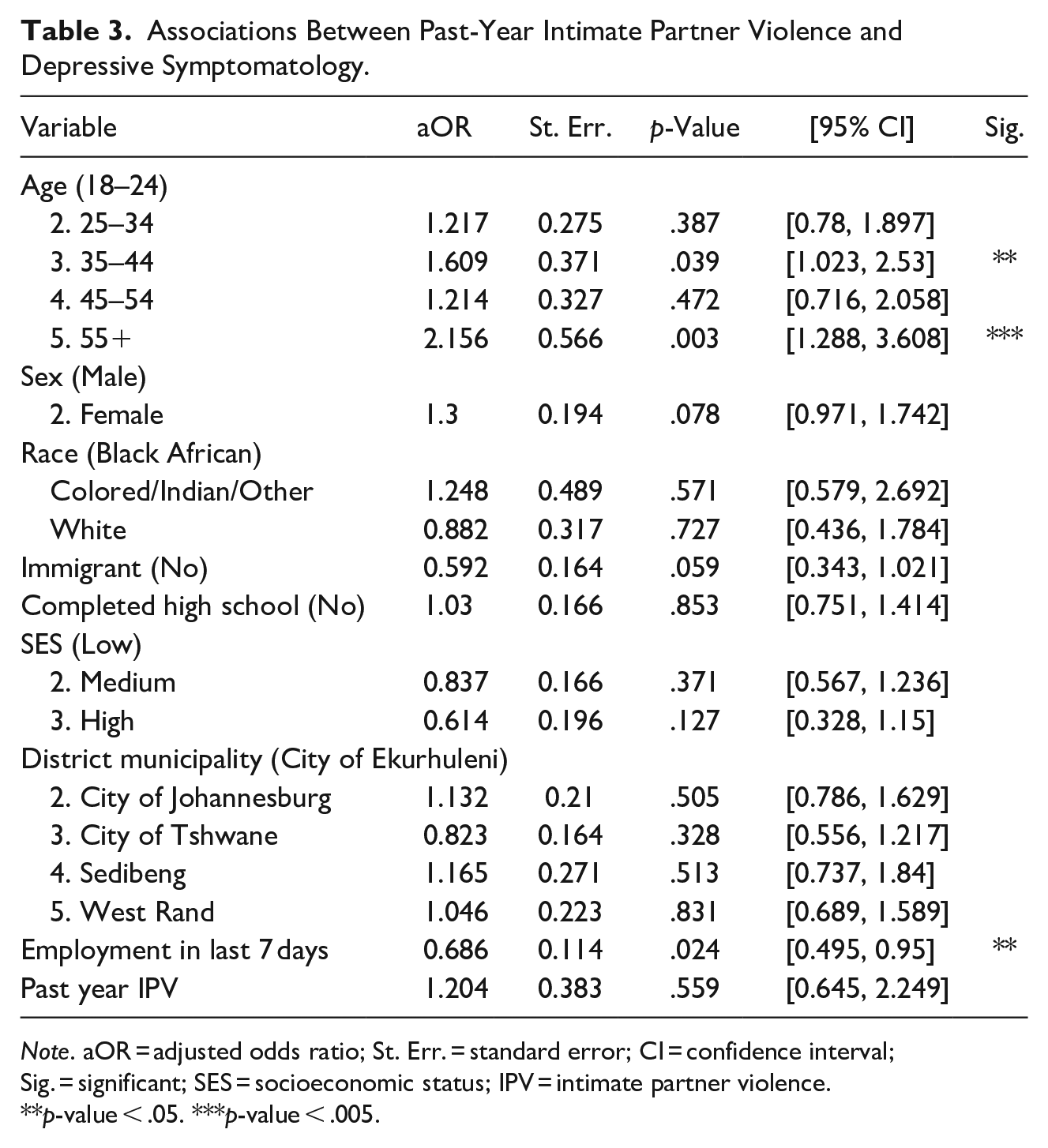
Note. aOR = adjusted odds ratio; St. Err. = standard error; CI = confidence interval; Sig. = significant; SES = socioeconomic status; IPV = intimate partner violence.
p-value < .05. ***p-value < .005.
Model 3: Non-partner violence: A total of 208 participants (16%) experienced past-year non-partner violence. Respondents aged 35 to 44 and those aged 55+ again had significantly greater odds of reporting depressive symptoms (35–44: aOR: 1.712, 95% CI [1.085, 2.702], p = .021; 55+ aOR: 2.323, [1.391, 3.878], p = .001; see Table 4). SGM females who experienced non-partner physical and/or sexual violence also had significantly higher odds of reporting depressive symptoms in this model (aOR: 1.403, [1.039, 1.895], p = .027). Those employed in the past 7 days had significantly lower odds of reporting depressive symptoms (aOR: 0.67, [0.481, 0.932], p = .017). Experiencing non-partner physical and/or sexual violence in the past 12 months was associated with significantly greater odds of reporting depressive symptoms (aOR: 1.842, [1.243, 2.73], p = .002). Odds ratios for other covariates were not statistically significant when adjusted for all other variables.
Associations Between Non-Partner Violence and Depressive Symptomatology.
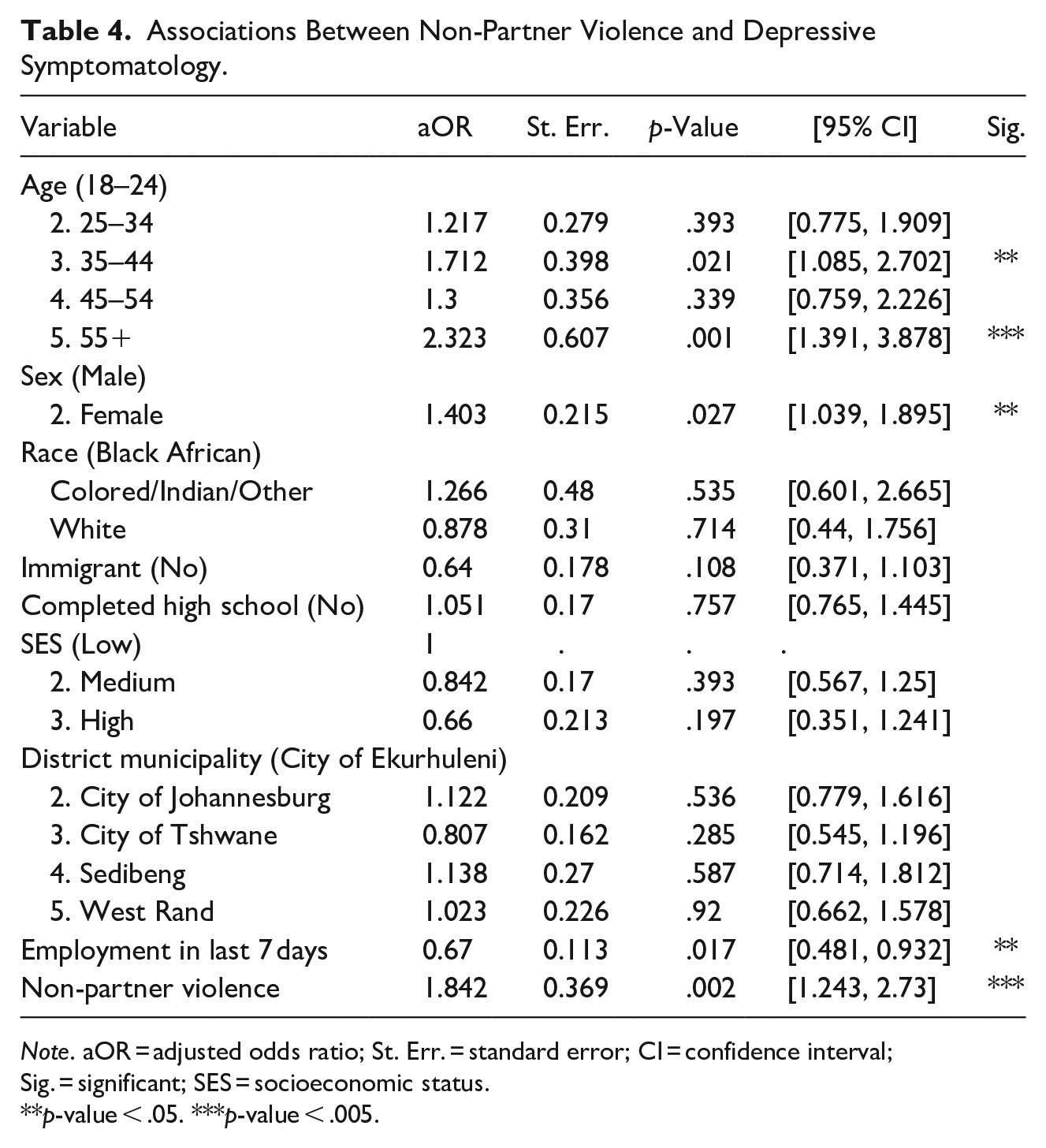
Note. aOR = adjusted odds ratio; St. Err. = standard error; CI = confidence interval; Sig. = significant; SES = socioeconomic status.
p-value < .05. ***p-value < .005.
Discussion
This study highlights the significant relationship between discrete forms of enacted discrimination as measured by violence exposure and elevated depressive symptoms among a population-based and representative sample of SGM adults in Gauteng, South Africa. Of note, 40% of the sample reported depressive symptoms. While prevalence rates of CSA (17%) and past-year non-partner violence (16%) were high, the prevalence of past-year IPV was surprisingly low (5%).
CSA was associated with a nearly 50% increase in the odds of reporting elevated depressive symptoms, corroborating previous research associating CSA and poor mental health in SGM populations (Balsam et al., 2010; Friedman et al., 2011; Xu & Zheng, 2015). This has relevance for mental and physical health since childhood abuse and neglect are linked to stress-response behaviors, such as substance misuse (Fletcher, 2021) that can also increase the likelihood of victimization and perpetration of IPV and other forms of violence (Spencer et al., 2019). While affirming services for SGM people who have experienced CSA in South Africa exist, they are often under-resourced, which limits the ability of individuals feeling safe enough to access them (Mkhize & Maharaj, 2023). Trauma-informed services that are built into existing spaces, such as schools and non-SGM-specific organizations, may provide additional access to more discreet services for those who feel unable to access them in spaces that cater specifically to SGM groups.
Model 2 did not support our hypothesis that past-year IPV would be significantly associated with increased odds of reporting depressive symptoms. While previous literature supports this hypothesis (Bacchus et al., 2018; Miltz et al., 2019) there may be methodological reasons this association was not found in the Quality of Life survey. First, the scope of IPV measurement was brief due to the logistical constraints of conducting population-based surveys with large samples. We limited the exposure to three types of physical violence, two forms of sexual abuse, and being threatened with a weapon by a current or former partner. By not including an exhaustive list of specific IPV behaviors, we may misclassify respondents. Model 3 found that non-partner violence was significantly associated with greater odds of reporting elevated depressive symptoms. Non-partner violence is a normative phenomenon among all populations in South Africa, but our data suggest SGM adults bear a disproportionately higher burden. Respondent status as an SGM person can make victimization more frequent and severe and can limit opportunities for recourse after the violent episode (Judge & Nel, 2008; Wells & Polders, 2006). This is consistent across forms of gender-based violence, where the same individuals who are marginalized and targeted for abuse are systematically precluded from accessing justice. In South Africa, recentering SGM individuals in violence prevention and response is paramount and urgent, particularly as the country enacts a raft of three new pieces of legislation to improve the identification of and response to gender-based violence (Republic of South Africa Department of Justice and Constitutional Development, 2023)
Across all three models, two age groups (35–45 and 55+) had significantly higher odds of reporting elevated depressive symptoms. Previous studies of sexual minority men and transgender women in South Africa found elevated levels of enacted discrimination and anticipated stigma in respondents in their 30s and 40s (Metheny et al., 2022), while older SGM adults have reported the highest levels of discrimination (Nyeck et al., 2019). Since enacted and anticipated, stigma is closely related to poor mental health outcomes (Almeida et al., 2009; Hatzenbuehler, 2016), entrenched social norms in less accepting segments of South African society may lead to greater odds of depressive symptoms in this sample as well.
The finding that recent employment was consistently associated with significantly lower odds of depressive symptoms is consistent with longitudinal data showing that unemployment negatively impacts mental health in South Africans (Burger et al., 2017). This is even more pronounced in SGM South Africans, where significant wage differentials exist between SGM and non-SGM South Africans, especially for those working part-time, casually, or in an informal sector (Nyeck et al., 2019). In a country where more than one-third of people are unemployed (a rate that rises to nearly two-thirds among those 25–34; Nyeck et al., 2019; Statistics of South Africa, Republic of South Africa, 2022), employment is a key social determinant of mental health. Structural interventions that provide meaningful skills training and employment to SGM South Africans may, therefore, be advantageous in reducing the mental health impacts of the minority and other social stressors that affect SGM people in a multiplicative way. Moreover, given the results of this study, there is likely an effect of being unemployed and experiencing one or more forms of violence and their combined effect on depressive symptoms. Though these have been individually determined to add to the risk of developing depressive symptoms (as mentioned above), there are no studies of SGM people that look at the intersection of these factors and their effect on mental health outcomes in this community. Future studies using Quality of Life survey data may be able to understand these complex drivers of depression.
Approaches to reduce the negative mental health effects of violence against SGM people in urban South Africa must also consider the broader context of South African society (Baranyi et al., 2021). First, SGM people in South Africa are often placed at the intersection of several social determinants of health (e.g., poverty, unemployment, homonegative stigma) that place them at higher risk for violence and, therefore, poorer mental health. Second, individual-level interventions to improve mental health (e.g., talk therapy) can be less effective in the context of high levels of violent crime (Finegan et al., 2020). Given that Johannesburg, which occupies a large segment of the Gauteng Province from which this sample was drawn, is the most violent African city per capita (Statistics South Africa, 2023), it is recommended to implement structural interventions aimed at addressing CSA, IPV, and non-partner violence against SGM individuals. Employing structural and social determinants of health approaches is essential to mitigate the negative associations between violence and depressive symptoms in the urban context of SGM South African individuals.
Strengths: This study has numerous strengths, including its large-for-context sample size, rigorous sampling methodology, and multiple measures of violence that provide new knowledge regarding the implications of enacted discrimination via violence victimization on the mental health of an urban South African SGM population.
Limitations: There are, however, important limitations that should be noted. First, the study is cross-sectional, which precludes any measure of causality or temporality. Second, the survey measures of violence, specifically IPV, may not account for SGM-specific forms of violence and, therefore, provide an undercount of the true prevalence of all three forms of violence in the SGM population. This is likely one reason for the low prevalence of IPV found in this study and likely contributed to the inability to disaggregate by typology. The scope of IPV measurement was brief due to the logistical constraints of conducting population-based surveys with large samples. For example, IPV may be distinct among SGM (e.g., through forms of “outing” someone or via higher levels of psychological abuse vs. physical abuse), yet the vast majority of IPV measures were developed for heterosexual women (Lejbowicz & Jacobs-Colas, 2022; Reuter et al., 2017). These limitations may lead to underreporting of the prevalence of past-year IPV among SGM individuals in our data and an attenuated association with depressive symptoms. To understand IPV more holistically in this context, adapting standardized measures of IPV to the needs and experiences of SGM people is essential to accurately account for the prevalence and impacts of IPV in this community. Third, we were unable to pinpoint whether the respondent’s SGM status was a contributing factor in the victimization or whether it was merely a coincidence. That is, we do not know if the violence occurred because the person is SGM. However, minority stress theory maintains that identifying as a sexual and/or gender minority automatically places many SGM individuals at an elevated risk of experiencing numerous negative health outcomes due to their vulnerabilities related to their physical, psychological, and social factors (Frost et al., 2015; Kertzner et al., 2009; Meyer, 2016). Still, a more precise understanding of the motivation for violence could further inform interventions. Finally, while we were able to disaggregate by sex, sample size, and survey limitations precluded the ability to fully disaggregate by SGM status, requiring the collapsing of these distinct communities into a single SGM category. While this complicates important differences between SGM groups, understanding how this community experiences violence and mental health disparities is important for policy-related advocacy to lay audiences and an appropriate starting point for more nuanced data collection efforts and analyses.
Conclusion
This analysis represents the first use of sexual and gender orientation variables within a population-based African study. The inclusion of SGM-specific data in representative samples provides an opportunity to evaluate population trends, identify community-based needs, and uncover potential points of intervention specific to urban South African SGM people. Future research should continue examining the physical and mental health outcomes of urban SGM people living in South Africa, as well as the intricate relationships between different forms of violence and health in this marginalized population.
A significantly greater burden of depressive symptoms and social stressors versus non-SGM respondents in the Quality of Life survey underpins the need for additional resources and interventions for SGM adults across South Africa. These should aim to both prevent and treat violence victimization and its associated mental health implications in this population. New and better measures that respond to the unique stressors and forms of violence seen in these communities, and rigorous longitudinal data may highlight specific points of behavioral, structural, and policy intervention to improve the quality of life for urban South African SGM.
Footnotes
Authors Note
Nicholas Metheny is also affiliated to University of Cape Town, Cape Town, South Africa.
Declaration of Conflicting Interests
The author(s) declared a potential conflict of interest (e.g., a financial relationship with the commercial organizations or products discussed in this article) as follows: Dr. Metheny received compensation as a consultant from the Gauteng Region City Observatory.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Metheny received funding from GCRO to lead this research as an outside consultant. No other authors received financial support for the research and/or authorship of this article.