
Abstract
This study examined the associations between violence victimization, homelessness, and severe mental illness (SMI) among people who use opioids (PWUOs) in three U.S. cities. We analyzed data from a cross-sectional survey conducted from May 2019 to February 2020 across three study sites: Los Angeles, CA; Las Vegas, NV; and Atlanta, GA. We used multivariable regressions to examine how multiple victimizations and housing situation are associated with SMI. Based on K-6 scale, nearly half (44.2%) were screened positive for SMI. Meanwhile, 69.7% of the participants reported experiencing some kind of violence in their lifetime, and more than half (51.9%) reported experiencing recent violence (in the past 6 months). The most common form of lifetime violence was emotional (59.5%), followed by physical and intimate partner violence (IPV) (56.1 and 34.9%, respectively), and 34.9% of all participants reported experiencing multiple forms of victimization in the past 6 months. Participants who reported homelessness were more likely to report having experienced recent violence victimization (p < .001). In multivariable models, experiencing recent victimization was significantly associated with SMI (adjusted odds ratio (AOR) = 1.85, 95% confidence interval [CI] [1.46, 2.38]), as was homelessness (AOR = 1.57, 95% CI [1.15, 2.14]), after adjusting for study covariates. Among those with moderate and SMI (n = 927), only 22% were currently receiving mental health services, and those who reported having experienced any forms of violence in the past 6 months were more likely to utilize mental health services than those who had not experienced any recent violence victimization (25 vs. 17.9%, p < .05). To improve mental health and wellness among this high priority population, mental health facilities and syringe service programs may consider screening for experiences of violence and using trauma-informed mental health approaches. Harm reduction interventions must be responsive to the diverse individual and structural-level needs of PWUOs, especially those experiencing homelessness and housing insecurity. Holistic strategies and services are needed to meet the social and structural needs of this population.
Introduction
The opioid crisis continues to impact communities across the United States (Dasgupta et al., 2018; Wilson, 2020). According to the Centers for Disease Control and Prevention, drug overdose is the leading cause of injury-related deaths in the United States, and overdoses that involve illicit or prescription opioids killed 128 people every day in 2019 (Mattson et al., 2021). Furthermore, opioid overdoses killed almost 47,000 people in 2018, and 32% of those deaths were caused by prescription opioids (Mattson et al., 2021). Recent studies indicate that the coronavirus pandemic and subsequent lockdown orders have further exacerbated the crisis (Silva & Kelly, 2020; Wilson, 2020). Since 2020, the first year of the COVID-19 pandemic, the death rate of drug overdose among Black persons surpassed that of whites for the first time since the 1990s (Friedman & Hansen, 2022).
Previous studies suggest that people who use opioids (PWUOs) bear a high burden of mental health disorders and at the same time, adults with mental health challenges such as depression, mood, and anxiety disorders are more likely to be prescribed opioids (Goesling et al., 2015; Halbert et al., 2016). A cross-sectional study among a nationally representative sample indicated that about 16% of Americans who have mental health disorders receive over half of all opioids prescribed in the United States (Davis et al., 2017). Current literature supports that mental health instability and physical pain can influence opioid use and dependency, and also suggests an association between depression and opioid use and how chronic pain coupled with comorbid depression are predictors for being prescribed opioids, receiving higher doses for longer periods of time, and the misuse or abuse of opioids compared to those without depression (Goesling et al., 2015; Scherrer et al., 2016). Moreover, those with severe mental illness (SMI) experience high comorbidity risk with substance abuse (Sheidow et al., 2012) and are 10 to 20 times more likely to be homeless than the general population (Kuno et al., 2000). These alarming quantitative statistics not only demonstrate the interplay between substance use, mental health, and housing status, but also suggest the need to address multilevel needs to promote the overall well-being among people with intersecting vulnerabilities.
One potential socio-behavioral factor that could contribute to the high mental health burden and complicate the interplay between substance use, mental health, and housing insecurity is violence victimization (Choe et al., 2008; Latalova et al., 2014). There is a growing body of literature documenting a strong association between violence victimization and psychological distress among various populations (Latalova et al., 2014). For example, studies have found that increased levels of community violence victimization were associated with greater depression among adolescents and young adults (Haden & Scarpa, 2008). Similar conclusions are drawn in studies that examined depressive symptoms among women who have experienced intimate partner violence (IPV) victimization. Two systematic reviews of the literature found that there is robust evidence supporting the association between IPV victimization and mental health issues such as depression, anxiety, post-traumatic stress disorder, self-harm, and sleep disorders (Dillon et al., 2013; Lagdon et al., 2014) and others found such associations among sexual and gender minority population (Finneran & Stephenson, 2013; Hong et al., 2022). Violence victimization experience is also frequent among PWUOs. A recent systematic review of 26 studies revealed that the prevalence of lifetime IPV victimization among women who use opioids was 36 to 94%, and 32 to 75% in the past year (Stone & Rothman, 2019). The findings of the review also indicated a “tight entanglement” of violence victimization, mental health problems, and substance abuse, especially among women. Furthermore, robust evidence in the literature suggests that those with socio-economic and structural vulnerabilities, such as difficulty securing jobs and housing, are more likely to experience violence victimization (Cho, 2012; Sanz-Barbero et al., 2018, 2019; Vest et al., 2002). There is a wealth of research which has found a strong relationship between housing instability and violence victimization (Breiding et al., 2017; Tong et al., 2021). Studies have further illustrated the negative impact of housing instability and violence victimization on health and mental health outcomes (Gilroy et al., 2016), and these effects can be even profound among PWUOs given the high rates of housing instability and victimization among this population (McLaughlin et al., 2021; Stone & Rothman, 2019). More recently, research started focusing on polyvictimization, namely the experience and exposure to multiple different forms of victimization, including emotional, sexual, physical, and IPV, and so on, and empirical studies show that these cumulative victimization experiences could lead to even worse mental and physical health outcomes, suggesting the need to further investigate this public health issue among at-risk populations such as PWUOs (Chan et al., 2021; Kassing et al., 2021; Palermo et al., 2019).
Despite the high rates of psychological distress and elevated risk of experiencing violence victimization and housing insecurity among PWUOs, little is known about mental health service utilization among this population. In fact, the syndemic theory suggests that health problems such as substance use, mental illness, victimization, and HIV/AIDS often occur interact and exacerbate each other in complex ways (Singer, 2009; Stall et al., 2008). These conditions function to make each other worse and mutually reinforce each epidemic that together lowers the overall well-being and health profile of individuals. As a result, such syndemics create additional barriers to help-seeking and lead to suboptimal and poor engagement in healthcare services (Singer, 2009; Tsai & Venkataramani, 2016). In fact, a study examining the utilization of substance use disorder and mental health treatment among individuals diagnosed with opioid use disorder (OUD) found that many individuals with OUD and other co-occurring mental illnesses are not receiving necessary care and mental health treatment. However, nearly one in five diagnosed with OUD but not diagnosed with mental illness is receiving prescription medication for mental illness (Novak et al., 2019). These findings suggest a need to improve access to mental health services for individuals who abuse substances, especially including racially, ethnically, and financially marginalized populations that may experience greater difficulty accessing mental health treatment. Therefore, there is a need to understand the complex relationships between violence victimization, housing status, and mental health outcomes among PWUOs and inform the design and development of future mental health and harm reduction services. As such, this study contributes to research by addressing the following aims: (a) describe the prevalence of lifetime and recent violence victimization of different forms (emotional, physical, sexual, and IPV) and the prevalence of SMI among PWUOs in three U.S. metropolitans (Los Angeles, Las Vegas, and Atlanta); and (b) explore the association between violence victimization, housing stability, and SMI among this population. The results will add evidence to our knowledge of the challenges this population faces and provide recommendations and implications for future research, advocacy, and programmatic action.
Methods
Study Procedure and Data Collection
A full description of the parent study’s methods and sampling has been presented elsewhere (Frew et al., 2021). Briefly, recruitment and data collection were conducted from May 2019 to February 2020 across three study sites: Los Angeles, CA; Las Vegas, NV; and Atlanta, GA. The study sites were selected based on community partnerships and the population of PWUOs, especially those who were at high risk for HIV infection, viral hepatitis, and opioid-involved overdose. Trained research staff facilitated a self-administrated, tablet-based survey with well-defined study instruments in-person at syringe service programs (SSPs) sites across all three cities.
Potentially eligible participants were invited to complete a screener with the research staff, where the study team had the opportunity to collect the data confidentially and obtain consent electronically without collecting any identifiable information. Eligibility criteria included (a) 18 years of age or older, (b) participation in one of the study sites’ SSP services at least once, (c) self-reported opioid use at least once in the past 6 months, (d) ability to speak and understand English or Spanish, and (e) ability to provide consent. A total of 1,368 participants started the survey across the three cities, and 1,127 individuals completed the questionnaire and were eligible for the parent study. Study procedures were reviewed and approved by the Institutional Review Board of the University of Nevada Las Vegas.
Measures
Sociodemographic
The study survey captured an array of variables including detailed sociodemographic measures. Participants were asked to report their age, racial and ethnic background, gender, education, sexual orientation, relationship status, employment status, and income level (Table 1).
Sociodemographic Characteristics of People Who Use Opioids (N = 1,127).
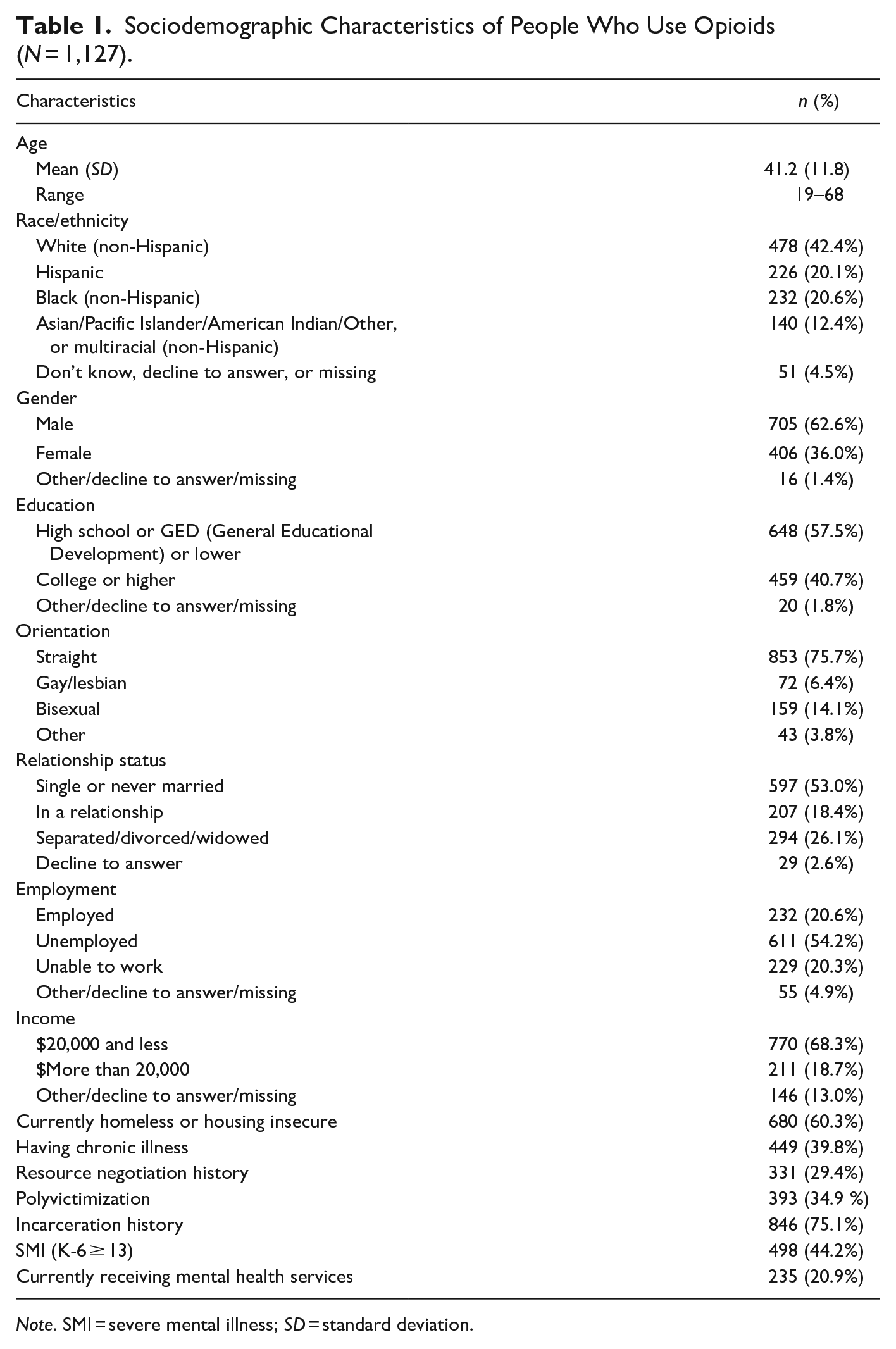
Note. SMI = severe mental illness; SD = standard deviation.
SMI and mental health service utilization
We used the validated “K-6” screening tool to discern the prevalence of mental illness among the participants in our sample (Kessler et al., 2002). The 6-item tool assesses the frequency of psychological distress within a certain period and has been widely used and validated. Participants were first asked to rate how often they felt (1) nervous, (2) hopeless, (3) restless or fidgety, (4) so depressed that nothing could cheer you up, (5) that everything was an effort, and/or (6) worthless in the past 30 days. The responses ranged from “None of the time” to “All of the time” coded from one to four, which yielded a sum between 0 and 24. A K-6 total score equal to or greater than 13 was considered SMI (Kessler et al., 2002). We, therefore, dichotomized a new SMI dummy variable indicating screened positive for SMI (1 = yes, 0 = no). Similarly, a K-6 summary score equal to or greater than 5 was considered moderate mental illness. For this study, the K-6 scale demonstrated a Cronbach’s α of .9, indicating good internal consistency.
Participants were also asked, “Are you currently receiving mental health services (examples: counseling, inpatient therapy, outpatient therapy, seeing a psychiatrist)?” Responses were grouped (1 = yes; 0 = no/not sure/decline to answer).
Violence victimization and polyvictimization
We assessed lifetime and recent (in the past 6 months) violence victimization by asking the participants to report on four types of violence victimization: emotional, physical, sexual, and IPV. For emotional violence, participants were asked, “Have you experienced any emotional violence (verbal abuse, name-calling, manipulation, etc.) from anyone else?” The question assessed physical violence, “Have you experienced any form of physical violence (slapping, hitting, kicking, pushing, etc.) from anyone else?” For sexual violence, participants were asked, “Have you experienced any form of sexual violence (unwanted touching, forced sexual activity, incest, molestation, etc.) from anyone else?” Lastly, IPV was measured by asking, “Have you been the victim of any forms of IPV (e.g. violence committed by a spouse, partner, boy/girlfriend, etc.) against you?” Response options included (1) Yes, (2) No, (3) Not sure, and (4) Decline to answer. We dichotomized a new variable to 1 if a participant responded yes, while the others were coded to 0. Polyvictimization is the sum of the four types of recent violence victimization with values ranging from 0 to 4. Each number indicates the type of violence the participants reported having experienced in the past 6 months. In the statistical model, polyvictimization was considered a dummy variable. Participants who reported experiencing two or more types of victimization were coded as 1, indicating that they had experienced polyvictimization.
Homeless or housing insecurity
Participants were asked, “Are you currently homeless or housing insecure (living on the street, in a car, at a homeless shelter)?” Response options included (1) Yes, (2) No, (3) Not sure, and (4) Decline to answer. We dichotomized this variable and coded it as 1 if a participant selected Yes.
Other covariates
To assess whether one experienced chronic illness, participants were asked, “Do you have any chronic medical problems (e.g., Diabetes, Obesity, High Blood Pressure, High Cholesterol) which continue to interfere with your life?” For resource negotiation, participants were asked, “Have you ever traded sex for goods, a place to stay, money, or drugs/alcohol?” Incarceration history was measured by the question, “Have you ever been incarcerated in a prison or jail?” The responses to these questions included (1) Yes, (2) No, (3) Not sure, and (4) Decline to answer. In addition, participants were also asked, “Are you currently receiving mental health services (e.g., counseling, inpatient therapy, outpatient theory, seeing a psychiatrist?” All variables were dichotomized and coded to 1 if a participant responded yes.
Statistical analysis
Descriptive statistics were reported using frequency measures to present the participants’ demographic characteristics. Percentages showed the prevalence of lifetime and recent violence victimization, housing insecurity, and mental illness. Bivariate associations between violence victimization, multiple victimizations, and housing insecurity were assessed using chi-square test for categorical variables and t-test for continuous outcomes. Using logistic regression, we assessed bivariate associations between each violence variable, housing situation, demographic characteristics, covariates, and SMI. Results were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CI). Next, we conducted a multivariate regression model to examine the association between polyvictimization and housing situation with SMI, adjusting variables that were significantly associated with SMI in bivariate analyses (p < .05) and study locations. We only include polyvictimization as the main predictor in the multivariate model due to multicollinearity concerns of each individual victimization. Lastly, the association between recent violence victimization and seeking mental health services was assessed using McNemar’s test among those who had a moderate or SMI.
Multiple imputation was used to incorporate all available data into the multivariable regression models while addressing missing data (Azur et al., 2011; Rubin, 2004). In multiple imputation, models of relationships between variables in the model are iteratively fit along with randomized draws from the best-fit models to fill missing data, producing several imputed datasets. Analyses are run separately on each imputed dataset and the results pooled to generate estimates and CIs that account for both estimation error in the analytic models and error from the estimation of missing data. For this analysis, the fully conditional specification algorithm was used with all model variables to generate 20 imputed datasets with 30 iterations between datasets to allow for proper convergence. Derived variables (K-6 and violence victimization) were imputed with the Just Another Variable technique and were computed prior to imputation and imputed along with the other model variables and their components. This method has been shown to reduce bias compared to other approaches (Seaman et al., 2012; White et al., 2011). For reproducibility, a random seed was generated using RANDOM.ORG’s true random number generator and used for the generation of imputed datasets (Haahr, 2022). Using multiple imputation allowed us to leverage the full information available in completed items (94% item-wise completion rate) even though most participants had at least one missing item in the multivariable model (46% case-wise completion rate). Data were analyzed using R software.
Results
Sample Characteristics
Of all participants (n = 1127), the average age was 41.2 years (range: 19–68, standard deviation: 11.8), and 62.6% were male (Table 1). Nearly half (42.4%) of the participants identified as White (non-Hispanic), followed by Hispanic (20.6%) and Black (non-Hispanic, 20.1%). Over 40% (40.7%) had some college education, more than half (54.2%) were unemployed, and about one-fifth (20.3%) reported being unable to work. Over two-thirds (68.3%) of participants had an annual income of less than US $20,000, and 39.8% had chronic medical problems. Nearly 30% (29.4%) had a resource negotiation history (e.g., trade sex for money/goods), and about three-quarters (75.1%) had a history of being incarcerated. Lastly, over 60 (60.3%) of the participants reported being housing insecure or currently homeless, and participants recruited from Los Angeles were more likely to have reported being housing insecure or currently homeless than those from Las Vegas and Atlanta (p < .01).
Prevalence of Violence Victimization and SMI
As presented in Table 2, 69.7% of the participants reported experiencing some kind of violence in their lifetime, and more than half (51.9%) reported experiencing recent violence (in the past 6 months). The most common form of lifetime violence was emotional (59.5%), followed by physical and IPV (56.1 and 34.9%, respectively). Similarly, over 40% (43.8%) of the participants reported having experienced recent emotional violence, while 35.4% reported recent physical violence victimization. Notably, 34.9% of all participants reported experiencing polyvictimization in the past 6 months.
Prevalence of Recent Violence Victimization by Housing Status Among People Who Use Opioids (N = 1,127).
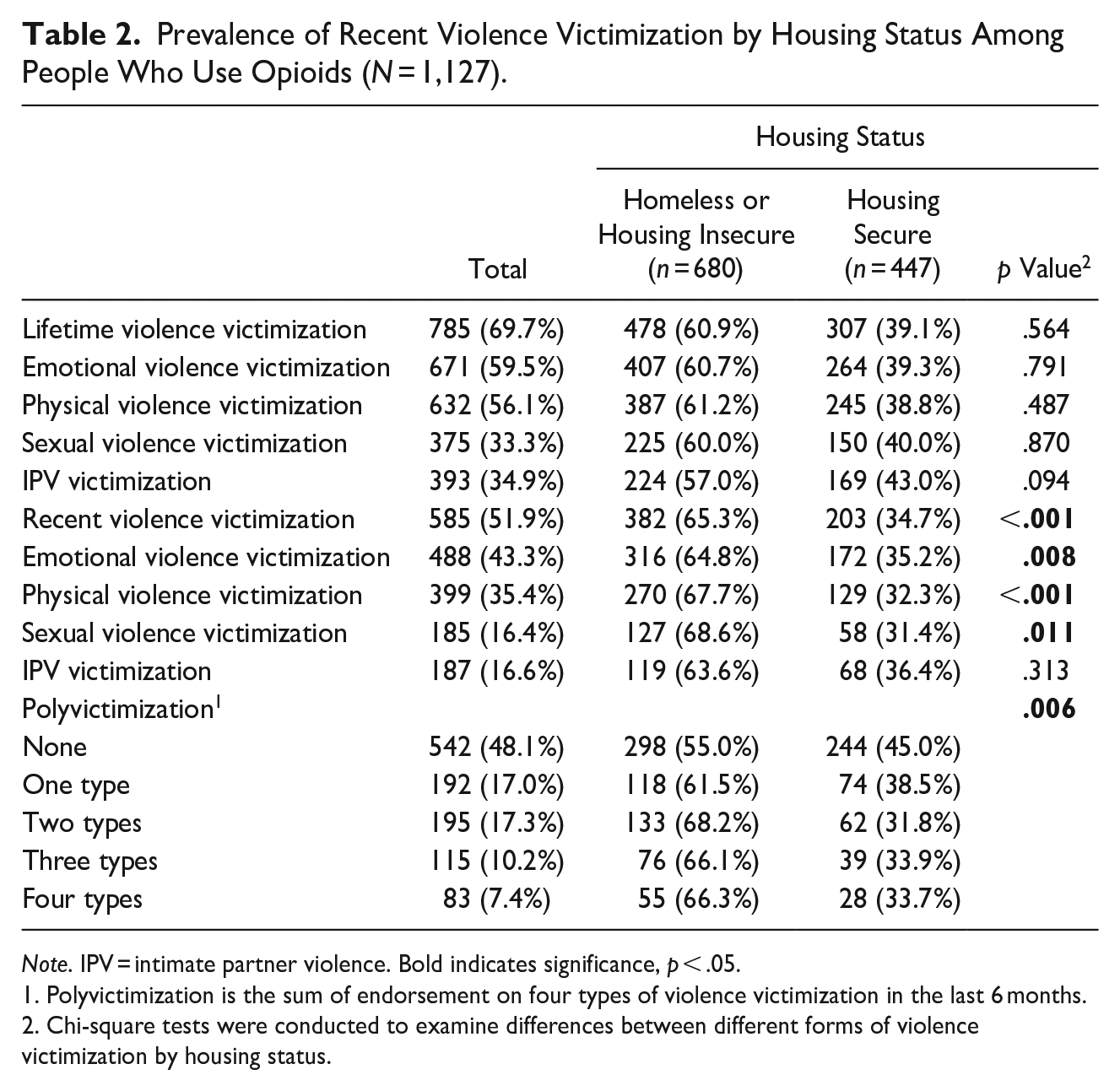
Note. IPV = intimate partner violence. Bold indicates significance, p < .05.
Polyvictimization is the sum of endorsement on four types of violence victimization in the last 6 months.
Chi-square tests were conducted to examine differences between different forms of violence victimization by housing status.
Participants who reported homelessness or housing insecurity were more likely to report having experienced recent violence victimization (p < .001), including emotional, physical, and sexual violence victimization (p < .01 for all). Lastly, those who were homeless or housing insecure were more likely to report having experienced polyvictimization than those who were housing secure (p < .01). Based on the K-6, 44.2% of all participants screened positive for SMI (Table 2).
The Association Between Violence Victimization, Housing Situation, and SMI
Bivariate and multivariate associations between violence victimization, housing situation, and SMI are presented in Tables 2 and 3. In bivariate analysis, all forms of lifetime and recent violence victimization were positively associated with SMI (p < .01 for all). Meanwhile, those who reported homelessness or housing insecurity were significantly more likely to screen positive for SMI (OR = 1.85, 95% CI [1.46, 2.38]). In terms of housing status, PWUOs who experienced housing insecurity or being homeless were significantly more likely to report experiencing recent violence victimization, especially recent emotional, physical, and sexual victimization (p < .01). In addition, housing insecurity was significantly associated with experiencing polyvictimization (p < .01). In the multivariate model, experiencing polyvictimization was statistically significantly associated with SMI (AOR = 1.53, 95% CI [1.36, 1.72]), as was homelessness or housing insecurity (AOR = 1.57, 95% CI [1.15, 2.14]), after adjusting for all the study covariates. Other factors associated with SMI included being unemployed or unable to work (AOR = 2.10, 95% CI [1.47, 3.02]; AOR = 2.45, 95% CI [1.60, 3.76], respectively), and having a chronic illness (AOR = 1.69, 95% CI [1.26, 2.25]).
Bivariate and Multivariate Associations Between Violence Victimization, Homelessness, and SMI Among People Who Use Opioids (N = 1,127).
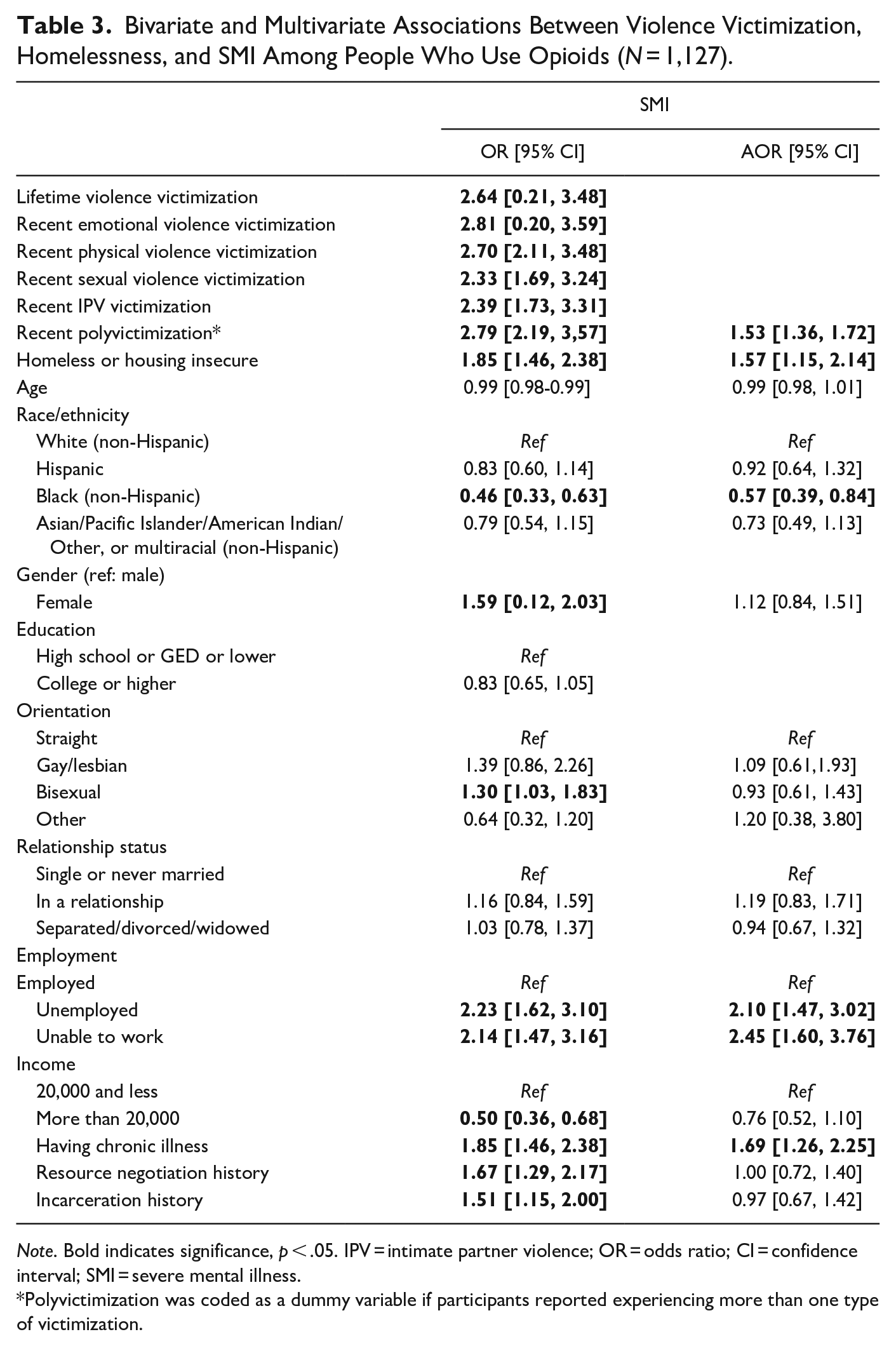
Note. Bold indicates significance, p < .05. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval; SMI = severe mental illness.
Polyvictimization was coded as a dummy variable if participants reported experiencing more than one type of victimization.
Mental Health Service Utilization Among People Who Use Opioids Screened for Mental Illness
Among those with moderate and SMI (n = 927), less than one-fourth (22%) were currently receiving mental health services (Table 4). Those who reported having experienced any forms of violence in the past 6 months were more likely to utilize mental health services than those who had not experienced any recent violence victimization (25 vs. 17.9%, p < .05).
Bivariate Associations Between Violence Victimization and Mental Health Service Utilization Among People Who Use Opioids Who Had Moderate and Severe Mental Illness (N = 927).
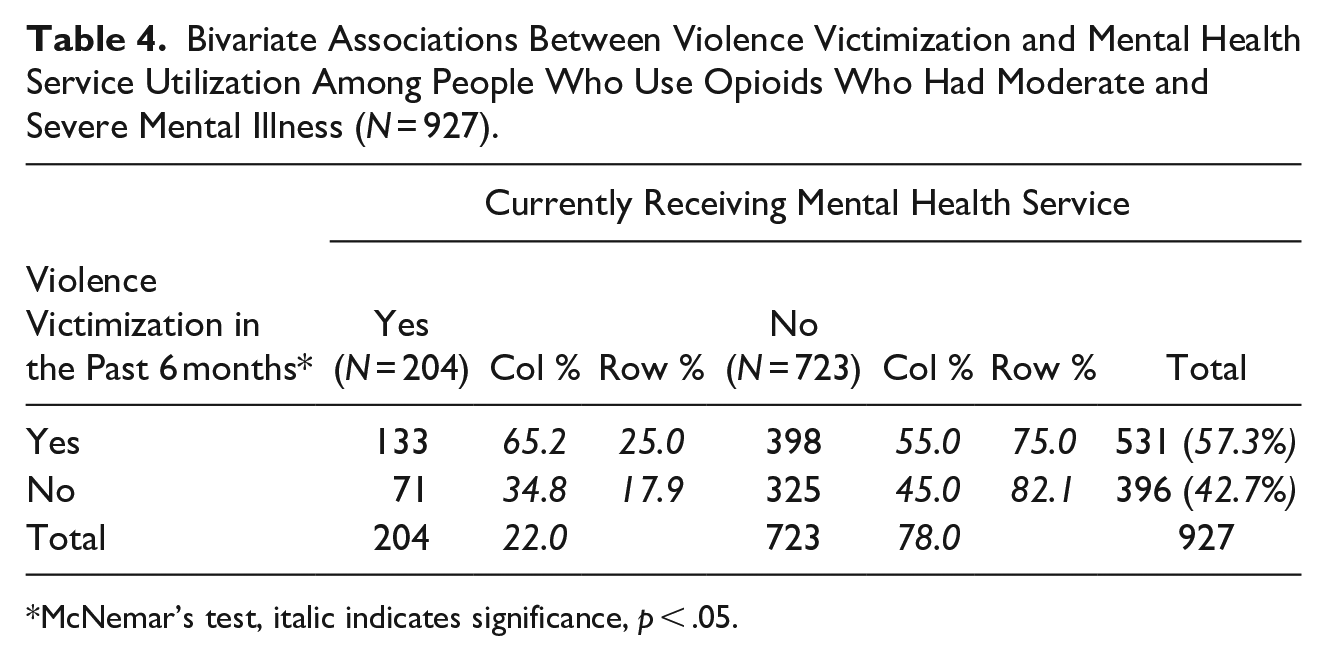
McNemar’s test, italic indicates significance, p < .05.
Discussion
Among PWUOs in these three U.S. cities, we observed a high prevalence of lifetime (69.7%) and recent (51.9%) violence victimization and SMI (44.2%). We also found that experiencing violence victimization is significantly associated with SMI among our study sample. These results were consistent with previous evidence on the high rates of victimization and mental health distress among people who use drugs (Colledge et al., 2020; Sells et al., 2003; Walters et al., 2021). These high rates of violence victimization and mental health burden suggest the need to provide comprehensive violence and mental health screening services to PWUOs, a population that already has adverse health outcomes and faces multilevel barriers to healthcare services.
In our study, nearly 70% of the participants reported having experienced violence victimization in their lifetime and more than half experienced some form of violence victimization in the past 6 months. These rates are consistent with a previous systematic review on opioid use and IPV, which suggests higher rates of IPV victimization among people who use drugs (Stone & Rothman, 2019). Our findings provide a wider variation of experiences of victimization and suggest that emotional violence was the most common form of lifetime and recent violence victimization, which is similar to a study among MSM living with HIV (Davis et al., 2020). In addition, our results indicate differences in endorsement of different types of recent victimization and multiple forms of victimization by housing status. We found that participants who were homeless or housing insecure were more likely to experience recent violence victimization. This is in line with the existing literature where studies have reported the association between social and economic vulnerabilities and violence victimization (Hong et al., 2022; Walters et al., 2021). For example, one study conducted in California also found that men who inject drugs reported being homeless were more likely to experience violent victimization (Walters et al., 2021). Efforts to prevent violence should continue integrating the social-ecological model and addressing multilevel factors to achieve and sustain prevention efforts over time (Centers for Disease Control and Prevention, 2015). Interventions to promote safety and mental health well-being must address the basic housing needs and provide new models of rehousing among PWUOs that are currently experiencing homelessness.
Nearly half of PWUOs in our sample screened positive for SMI in our study. This is consistent with the literature where studies suggest a high burden of psychological distress among people who use drugs across different settings (Jones & McCance-Katz, 2019; Mackesy-Amiti et al., 2014; Saing et al., 2020). To our knowledge, our study is among the first to examine the association between violence victimization and SMI among PWUOs. These findings add additional evidence to the literature and echo previous studies indicating the impact of violence victimization and mental health outcomes among various populations, including sexual and gender minority and people living with HIV (Brown et al., 2016; Buller et al., 2014; Finneran & Stephenson, 2013; Hong et al., 2023). We also found that having SMI was associated with multilevel factors, including individual factors such as being female, identifying as bisexual, lower income and being unemployed, and structural barriers, such as having resource negotiation history and being incarcerated. These results are consistent with previous work in the field and suggest that interventions to promote mental health well-being must address the social and structural inequalities (Pinto-Meza et al., 2013; Reiss, 2013). More importantly, these results confirmed the co-occurring substance use, mental health distress, and violence victimization among individuals with multilevel vulnerabilities and syndemic conditions and suggest the need for multiple levels of intervention. Future research may utilize longitudinal design and qualitative approach to understand the long-term impact of these condition on one’s overall well-being and how each condition may mutually reinforce and further exacerbate the existing health disparities among PWUOs.
Our study also identified a significant gap in providing accessible and adequate mental health services among this priority population. The findings reflect that less than a quarter of PWUOs in this study (22.0%) identified as having moderate or SMI were concurrently receiving mental health services. Other research has previously shown that people who use drugs with probable SMI were less likely to utilize mental health and other healthcare services (Adams et al., 2020). Potential barriers to healthcare engagement include anticipated stigma, medical mistrust, and limited accessibility (Kendall et al., 2020; Lister et al., 2020; Phillips et al., 2020). Previous studies also found that having stable housing is a strong predictor of engaging in healthcare services among people who use drugs (Kendall et al., 2020). Taken together, future research should identify the unique challenges and barriers to accessing mental health services among PWUOs and design interventions that increase accessibility accordingly. Additional investigations are also needed to explore the underlying mechanisms linking victimization, housing instability, and mental health distress among people are at high risk of these syndemics such as PWUOs. Our results suggest that those who have experienced recent violence victimization were more likely to receive mental health services. This finding indicates experiences of recent violence victimization may be a driving factor in seeking mental health services among PWUOs, but also suggests the need and opportunities for mental health professionals and community partners (e.g., SSPs) to assess and screen for experiences of violence victimization among their clients. Mental health service providers should utilize a holistic and multi-tiered approach to violence and substance use screening in mental health facilities, as well as provide options for drug treatment resources in these settings.
This study has some limitations. First, study participants were recruited in three cities in the United States, therefore limiting the generalizability of our findings to the broader community of PWUOs. Second, the cross-sectional design of the study limited our ability to draw causal inferences from the analyses. SMI could be the result of and/or contribute to violence victimization among PWUOs. Future studies could utilize longitudinal data to test the effect of violence victimization on mental health outcomes and vice versa. Lastly, all the data were self-reported and therefore may be subject to social desirability and recall bias; however, this may have been less likely due to the anonymity of data collection and the ability to complete surveys in a private location.
Conclusion
This study examined violence victimization and mental health illnesses among a vulnerable population, PWUOs, across three major U.S. cities and community partnerships. Study participants were racial and ethnically diverse. Individuals included in this study also reported diverse sexual orientations. PWUOs in our study experienced a high prevalence of violence victimization and SMI. Lifetime and recent violence victimization were associated with a higher likelihood of having SMI. To improve mental health and wellness among this high priority population, mental health facilities, and SSPs may consider screening for experiences of violence and using trauma-informed mental health approaches. Harm reduction interventions must be responsive to the diverse individual and structural-level needs of PWUOs, especially those experiencing homelessness and housing insecurity. Holistic strategies and services are needed to meet the social and structural needs of this population.
Footnotes
Acknowledgements
PMF was affiliated with the University of Nevada, Las Vegas when work was conducted and is currently affiliated with Merck & Co, Inc, Kenilworth, NJ, USA. We are deeply appreciative of our community partners, including but not limited to TracB, Atlanta Harm Reduction Coalition, The Elizabeth Foundation, Bienestar Human Services, and Asian American Drug Assistance Program, and the clients of these agencies who volunteered their time to complete our survey. This endeavor was a collaborative effort that consisted of a number of staff, including subject matter experts who assisted with instrument development and data collection procedures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: IWH is supported by the California HIV/AIDS Research Program (RP15-LA-007). PMF received internal funding from the University of Nevada, Las Vegas to facilitate partner engagement.
Author Biographies
Paula M. Frew, PhD, MPH, was a tenured Professor at the University of Nevada with academic and administrative appointments in the School of Public Health, Medicine, and through the Office of Research and Economic Development. Prior to that experience, she was an Associate Professor at Emory University in the School of Medicine and at the Rollins School of Public Health, wherein she conducted numerous infectious disease and vaccine-related studies at the intersection of clinical trials development and implementation, immunization and vaccine research, and community and clinical interventional strategies to improve uptake, adherence, and acceptability of biomedical prevention products (i.e., immunizations, PrEP) and immunotherapeutics. With a research agenda focused on addressing social determinants of health within vulnerable communities, she is particularly interested in identifying factors that contribute to health disparities and developing, testing, and evaluating interventions to surmount persistent threats to population health and well-being.