
Abstract
Intimate partner violence (IPV) is a serious public health problem associated with increased risk of developing mental health conditions. Assessment of IPV in mental health settings is important for appropriate treatment planning and referral; however, lack of training in how to identify and respond to IPV presents a significant barrier to assessment. To address this issue, the World Health Organization (WHO) advanced a series of evidence-based recommendations for IPV-related training programs. This study examines the relationship between mental health professionals’ experiences of IPV-related training, including the degree to which their training resembles WHO training recommendations, and their accuracy in correctly identifying relationship problems. Participants were psychologists and psychiatrists (N = 321) from 24 countries who agreed to participate in an online survey in French, Japanese, or Spanish. They responded to questions regarding their IPV-related training (i.e., components and hours of training) and rated the presence or absence of clinically significant relationship problems and maltreatment (RPM) and mental disorders across four case vignettes. Participants who received IPV-related training, and whose training was more recent and more closely resembled WHO training recommendations, were more likely than those without training to accurately identify RPM when it was present. Clinicians regardless of IPV-related training were equally likely to misclassify normative couple issues as clinically significant RPM. Findings suggest that IPV-related training assists clinicians in making more accurate assessments of patients presenting with clinically significant relationship problems, including IPV. These data inform recommendations for IPV-related training programs and suggest that training should be repeated, multicomponent, and include experiential training exercises, and guidelines for distinguishing normative relationship problems from clinically significant RPM.
Introduction
Intimate partner violence (IPV) is defined as any behavior within a relationship that causes—or has reasonable potential to cause—physical, sexual, or psychological harm to a partner (Foran et al., 2015; WHO, 2012). Globally, it is estimated that 35% of ever-partnered women have experienced lifetime IPV (WHO, 2013). IPV is associated with increased risk of developing mental health problems including depression, anxiety, post-traumatic stress disorder (PTSD), substance use disorders, and suicidal ideation (Bacchus et al., 2017; Laskey et al., 2019; Miller & McCaw, 2019; WHO, 2005). A systematic review of IPV prevalence studies conducted in psychiatric settings reported that the median prevalence of lifetime IPV was 30%–33% among female patients (inpatient and outpatient) and 18%–48% among male inpatients (Oram et al., 2013). Furthermore, systematic reviews suggest that women living with serious mental illness (i.e., who have a recurrent or persistent mental disorder that significantly impacts their functioning) are more than twice as likely to have experienced violence of any kind, including IPV, compared to the general population (Khalifeh & Dean, 2010; Mauritz et al., 2013).
WHO guidelines recommend that health professionals screen for IPV when assessing or treating individuals with mental health symptoms (WHO, 2013). Identification of IPV by global mental health professionals (i.e., clinicians who are involved in the assessment and treatment of individuals living with mental health symptoms) may lead to more accurate IPV prevalence data (Ellsberg & Heise, 2005), and help enhance our understanding of IPV risk factors and mental health consequences (Foran et al., 2015). Additionally, IPV assessment in mental health settings may contribute to improved case conceptualizations and referrals to care. Advocacy-based interventions have been shown to improve survivors’ quality of life and perceived social support (Sullivan & Bybee, 1999), whereas psychological treatments (e.g., cognitive behavioral therapy) have contributed to improved coping and social adjustment (Johnson & Zlotnick, 2006; McNamara et al., 2008) and decreased ratings of PTSD symptom severity (Johnson et al., 2011).
Despite the existence of best practice recommendations related to the assessment of IPV in mental health settings, IPV remains under-detected in these settings (Howard et al., 2010). Studies from Australia (Forsdike et al., 2019) and the United Kingdom (Nyame et al., 2013) found that more than half of mental health clinicians did not ask new patients about IPV. Furthermore, a survey of U.S. mental health service users identified that 45% of women and 73% of men had never been asked about their experiences of IPV (Chang et al., 2011).
Lack of IPV-related training has been identified as an important barrier for IPV assessment in mental health settings (Forsdike et al., 2019; Rose et al., 2011; Trevillion et al., 2016). Clinicians without training report lower confidence and competence in addressing the needs of patients experiencing IPV (Rose et al., 2011). IPV-related training is often not a mandatory component of professional training programs (Fricchione et al., 2012; Kamimura et al., 2015). Studies from the United States (Campbell et al., 1999), the United Kingdom (Nyame et al., 2013), and across 24 countries in South America, Europe, and Asia (Burns et al., 2020) show that nearly half of mental health clinicians have never received this form of training.
IPV-related training has been linked to improved outcomes for clinicians, including increased IPV-related knowledge (Burns et al., 2020; Forsdike et al., 2019; Jayatilleke et al., 2015; McColgan et al., 2010; Trevillion et al., 2016), improved confidence in addressing IPV (Forsdike et al., 2019; Jayatilleke et al., 2015), reduced unhelpful attitudes towards survivors (e.g., victim blaming; Jayatilleke et al., 2015; McColgan et al., 2010), and greater likelihood of screening for IPV (Murray et al., 2016). Given the apparent benefits of IPV-related training, the WHO advanced a series of evidence-based training recommendations for health care professionals (WHO, 2013). These recommendations specify that IPV-related training should be multicomponent and offered at several time points (e.g., at the prequalification and professional level). Recommended training components include didactic training (e.g., basic knowledge about IPV laws, prevalence, and risk factors as well as local support services for survivors) and skill-building exercises (e.g., teaching clinicians how and when to inquire about IPV, and how to respond to survivors). There has been no previous research evaluating the relationship between mental health professionals’ experiences of IPV-related training, including the degree to which their training resembles WHO training recommendations, and their accuracy in correctly identifying IPV.
Context for the Present Research
This research was conducted in the context of a larger study evaluating the clinical utility of proposed relationship problem and maltreatment (RPM) guidelines, created as a part of the development of guidelines (First et al., 2015) for Mental, Behavioral and Neurodevelopmental Disorders for the Eleventh Revision of WHO’s International Classification of Diseases and Related Health Problems (ICD-11), approved in May 2019 by the World Health Assembly. RPM guidelines are intended to assist clinicians with the identification and classification of clinically significant relationship problems, including IPV, that may lead people to seek health services. The larger study, created in English and later translated into French, Japanese, and Spanish, was developed to compare the use of proposed ICD-11 RPM guidelines to guidance provided in ICD-10. Heyman et al. (2018) reported the English-language results of the field trial (N = 738) and showed that ICD-11 RPM guidelines improved clinicians’ performance over ICD-10. French, Japanese, and Spanish results have not yet been reported.
Aims and Objectives
The present study uses data collected from specialized mental health professionals (i.e., psychiatrists and psychologists) who completed the ICD-11 RPM field trial in French, Japanese, and Spanish. The primary objective of this study was to explore how global clinicians’ experiences of IPV-related training were related to accuracy in distinguishing between different forms of IPV and normative relationship problems in a series of case-controlled vignettes. We hypothesized that clinicians with IPV training would be more likely to correctly identify relationship problems, including IPV, than those without training. We also hypothesized that clinicians with training that more closely resembled WHO training recommendations would perform better at identifying relationship problems. A secondary objective of this study was to assess differences in performance between the use of ICD-11 versus ICD-10 RPM guidelines within our sample. We hypothesized that, concordant with earlier findings (Heyman et al., 2018), ICD-11 guidelines would improve performance.
Method
Participants
Demographic Information (N = 321).
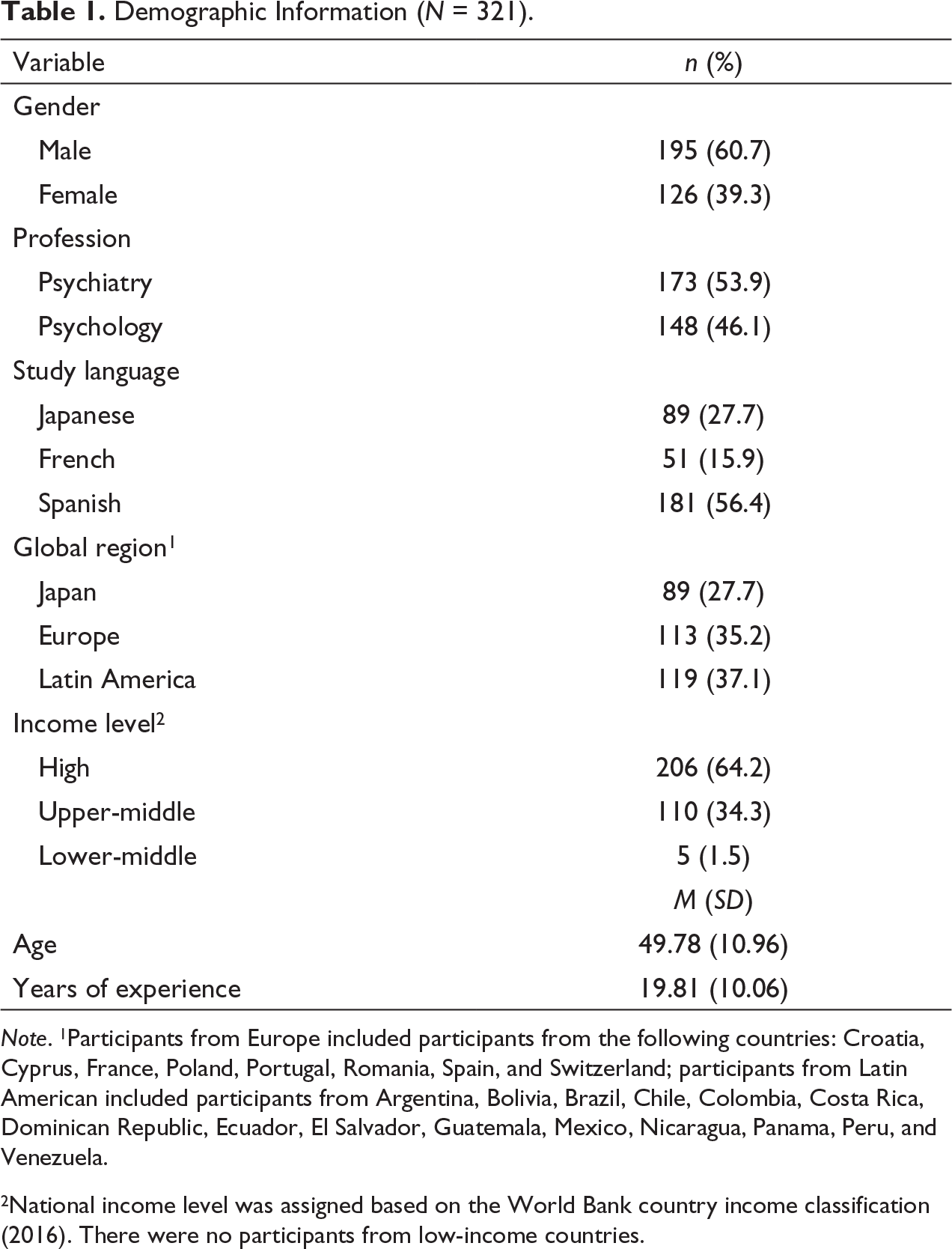
Note. 1Participants from Europe included participants from the following countries: Croatia, Cyprus, France, Poland, Portugal, Romania, Spain, and Switzerland; participants from Latin American included participants from Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Dominican Republic, Ecuador, El Salvador, Guatemala, Mexico, Nicaragua, Panama, Peru, and Venezuela.
2National income level was assigned based on the World Bank country income classification (2016). There were no participants from low-income countries.
Data and Materials
Demographic Information
Participants provided basic demographic information (i.e., gender, age, years of professional experience, profession, and country of residence) during their registration to the GCPN, and again upon initiating the current study. Participants completed the study in one of three languages (i.e., French, Japanese, or Spanish) and were classified into one of the eight WHO regions and one of four national income levels (i.e., high, upper-middle, lower-middle, low) based on their country of residence. There was significant overlap among region, study language, and national income level variables. Notably, all participants from Japan completed the study in Japanese (n = 89), and all participants from Latin America completed the study in Spanish (n = 119). Participants from Europe completed the study in either Spanish (n = 62) or French (n = 51). Furthermore, all participants from Japan and almost all participants from Europe (99%) were from high-income countries, while most participants from Latin America (95%) were from middle-income countries. Because language and country income are dependent on region, only the region variable was included in the analyses.
IPV-Related Training
Participants’ experiences of IPV-related training were measured with five questions. The first question asked participants to respond “Yes” or “No” to the following statement: “Please indicate whether, at any point during your clinical training or professional career, you have received formal training (e.g., as a part of courses, workshops, continuing education programs) about how to detect or respond to IPV, including physical and psychological abuse.” Those who selected “No” were not shown the following questions. The second question was based on the WHO’s IPV-related training recommendations (WHO, 2013) and asked participants to specify which components from the following list were included in their training: (a) definitions, laws and risk factors related to IPV, (b) support services for survivors of IPV, (c) how and when to inquire about IPV with patients, and (d) how to respond to survivors of IPV. The final three questions asked participants to input the number of hours dedicated to IPV-related training at three different time points: during their professional training, since completing their professional training, and during the past five years.
ICD Guidelines
The proposed ICD-11 RPM Clinical Descriptions or ICD-10 RPM Guidelines (WHO, 1992) were randomly assigned to participants for use when diagnosing persons described in vignettes. RPM Clinical Descriptions and Guidelines provide clinicians with a set of essential (required) features for diagnosing the presence or absence of clinically significant relationship problems. Participants were also asked to use ICD-11 diagnostic definitions for mood disorders and anxiety and fear-related disorders.
Vignettes
Three co-authors RH, HF, and AS developed 12 vignettes for the study based on actual clinical cases with all identifying information removed. Vignettes depicted 6 male and 6 female adults of various ages who were in heterosexual relationships. Information related to cultural or religious background was omitted to mitigate participant biases when evaluating the vignettes. Vignettes reflected four study conditions: (I) features consistent with both a clinically significant RPM and a mental and behavioral disorder (MBD) (both RPM and MBD present), (II) features consistent with only a RPM (RPM present, MBD absent), (III) features consistent with only a MBD (RPM absent, MBD present), and (IV) features consistent with neither a RPM or a MBD (both RPM and MBD absent). Each vignette described a patient presenting with either the presence or absence of one of three ICD-11 RPMs (i.e., relationship distress with spouse or intimate partner; spouse or partner violence, physical; or spouse or partner abuse, psychological), and the presence or absence of one of two MBDs (i.e., single episode depressive disorder or generalized anxiety disorder). When an RPM was absent, normative relationship problems were described; when a MBD was absent, subthreshold psychiatric symptoms were described. Further details of vignette development and validation are provided in Heyman et al. 2018.
Procedure
This study was exempted from review by the World Health Organization (WHO) Research Ethics Review Committee (Protocol ID RPC569) and by the Human Subjects Committee at the University of Kansas, Lawrence Campus (HSCL #20804).
Participants were sent an email invitation to participate in the study and followed an individualized link to the survey in Qualtrics® (Provo, USA). Participants who initiated the study were randomly assigned to view either ICD-11 or ICD-10 RPM guidelines for use throughout the study, without any explicit indication as to which version they were viewing. All participants viewed ICD-11 MBD diagnostic definitions for mood disorders and anxiety and fear-related disorders. After viewing the guidelines, participants were randomly assigned to one of 6 vignette comparison conditions. Comparisons were created for each vignette to have an equal probability of being presented throughout the study, and a similar probability of being presented with any of the other vignettes. Each comparison was composed of four vignettes, and each vignette was drawn from a different study condition: (I) both RPM and MBD present, (II) RPM present, MBD absent, (III) RPM absent, MBD present, or (IV) both RPM and MBD absent. Vignettes were presented with the order of presentation counterbalanced across participants. After viewing each vignette, participants were asked to select a MBD diagnosis, or no diagnosis, followed by a RPM category, or no RPM, from drop-down lists of ICD categories (i.e., ICD-11 MBD categories and ICD-10 or ICD-11 RPM categories). Participants could consult MBD definitions and RPM guidelines while making their decisions. Participants completed this sequence four times, once for each vignette (see Heyman et al., 2018 for a full description of the methodology for the larger field trial). Finally, participants responded to the five questions about their IPV-related training experiences.
Results
Participants
The representativeness of our sample was determined by comparing participants who completed the survey (i.e., completers) to clinicians who were invited to the study but did not participate (nonparticipants), and to participants who initiated the study but did not complete it (noncompleters). Completers did not differ significantly from nonparticipants or noncompleters in terms of gender, profession, region, or proportion of participants in each survey language. However, completers had slightly more professional experience (M = 19.54, SD = 10.12) than nonparticipants (M = 18.12, SD = 11.00; t(2,447) = 2.207, p < .05) and noncompleters (M = 17.62, SD = 9.27; t(508) = 2.085, p < .05). Completers were also slightly older (M = 49.64, SD = 10.99) than nonparticipants (M = 48.10, SD = 12.15; t(2447) = 2.175, p < .05) and noncompleters (M = 47.33, SD = 10.92; t(508) = 2.094, p < .05).
ICD Version
Chi-square analyses were used to compare participants’ accuracy (i.e., percentage of those who diagnosed correctly versus those who did not diagnose correctly) while identifying RPM and MBD in each study condition, using ICD-11 versus ICD-10 RPM guidelines. The accuracy of clinicians’ diagnoses was not significantly different for the ICD-11 guidelines as compared to the ICD-10 guidelines. For this reason, the two ICD conditions were collapsed for subsequent analyses.
RPM Conditions
Each of the vignettes depicted patients presenting with MBD symptoms that either met full definitional requirements for a diagnosis (MBD present) or were subthreshold, which included some but not all the required features of a MBD (MBD absent). Differences in performance between MBD-present and MBD-absent conditions were relevant for the purposes of the larger ICD-11 field trial (Heyman et al., 2018) but were not pertinent for the current study. Therefore, for all following analyses, conditions I (both RPM and MBD present) and II (RPM present, MBD absent) were combined to form an RPM present condition, and conditions III (RPM absent, MBD present) and IV (both RPM and MBD absent) were combined to form an RPM absent condition. These new conditions represent two distinct assessment tasks for clinicians: identifying RPM in the presence of harmful relationship problems (RPM present) and identifying that there is no RPM when normal relationship problems are described (RPM absent).
Demographic Factors
Accuracy of Clinicians’ Diagnoses by Response Condition and Demographic Variable.
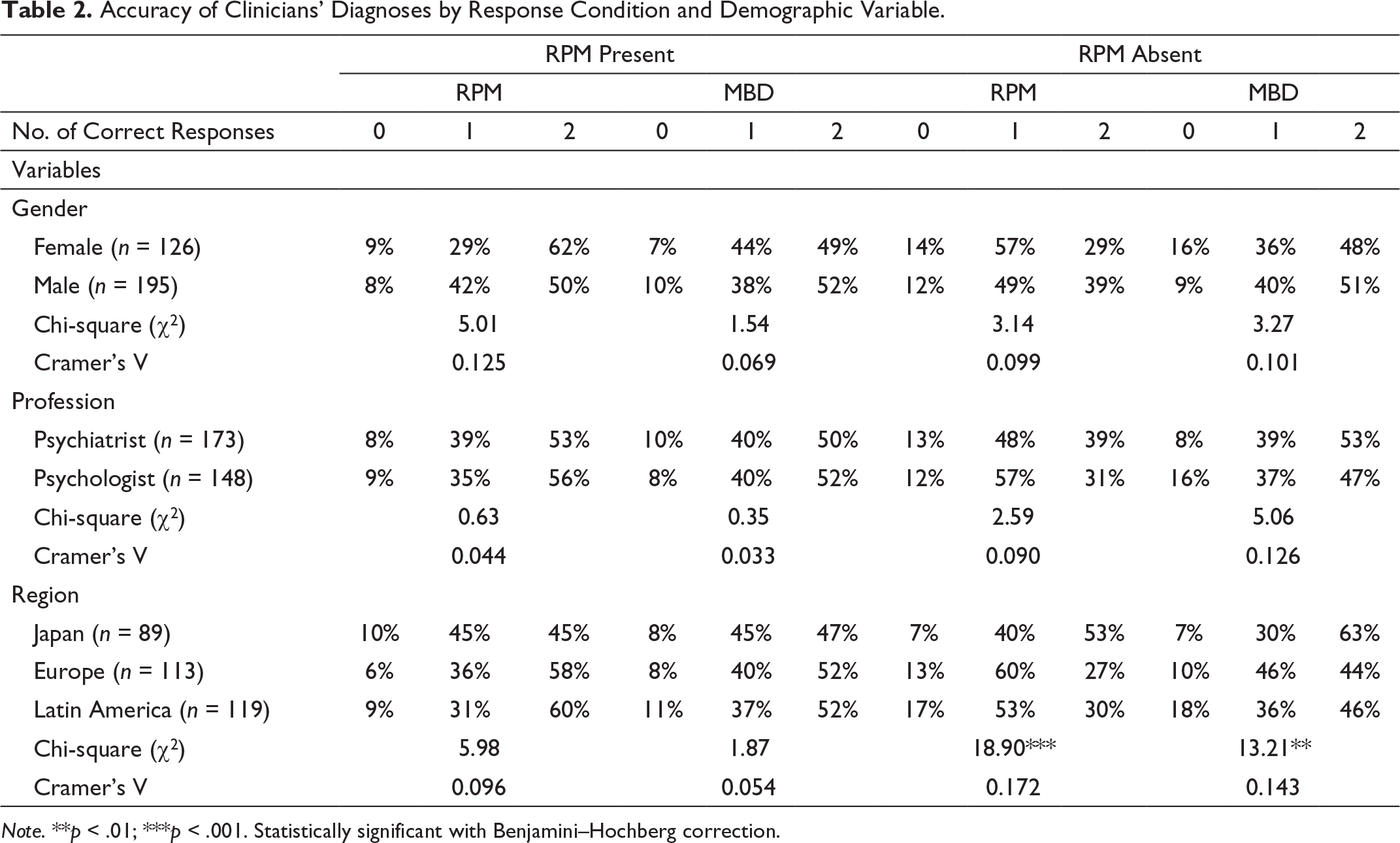
Note. **p < .01; ***p < .001. Statistically significant with Benjamini–Hochberg correction.
Multinomial logistic regressions were run to explore the relationship between age, years of professional experience, and diagnostic accuracy. In both RPM conditions (present; absent), when the task was to diagnose RPM, there was no relationship between age or years of professional experience and accuracy. However, when the task was to diagnose a MBD, accuracy was significantly related with age and years of professional experience in both RPM conditions. When RPM was present, younger clinicians were more likely than older clinicians to have 1 or 2 correct responses while diagnosing MBDs (maximum possible is 2), compared with 0 (χ2(1, N = 321) = 9.44, p < .01). Also, clinicians with less experience were more likely than those with more experience to have 2 correct responses (out of a maximum of 2), compared with 0 (χ2(1, N = 321) = 8.03, p < .05). When RPM was absent, younger clinicians were more likely than older clinicians to have 2 correct responses while diagnosing MBDs, compared with 1 (χ2(1, N = 321) = 6.76, p < .05). Also, clinicians with less experience were more likely than those with more experience to have 2 correct responses, compared with 1 (χ2(1, N = 321) = 7.46, p < .05).
IPV-Related Training
Chi-square analyses were performed to evaluate the relationship between IPV-related training (i.e., received training: yes or no) and accuracy (i.e., percentage who had 0, 1, or 2 correct diagnoses) when assessing for RPM and MBDs in both RPM conditions (present; absent).
Accuracy of Clinicians’ Diagnoses by Response Condition, RPM Condition, Region, and IPV-Related Training.
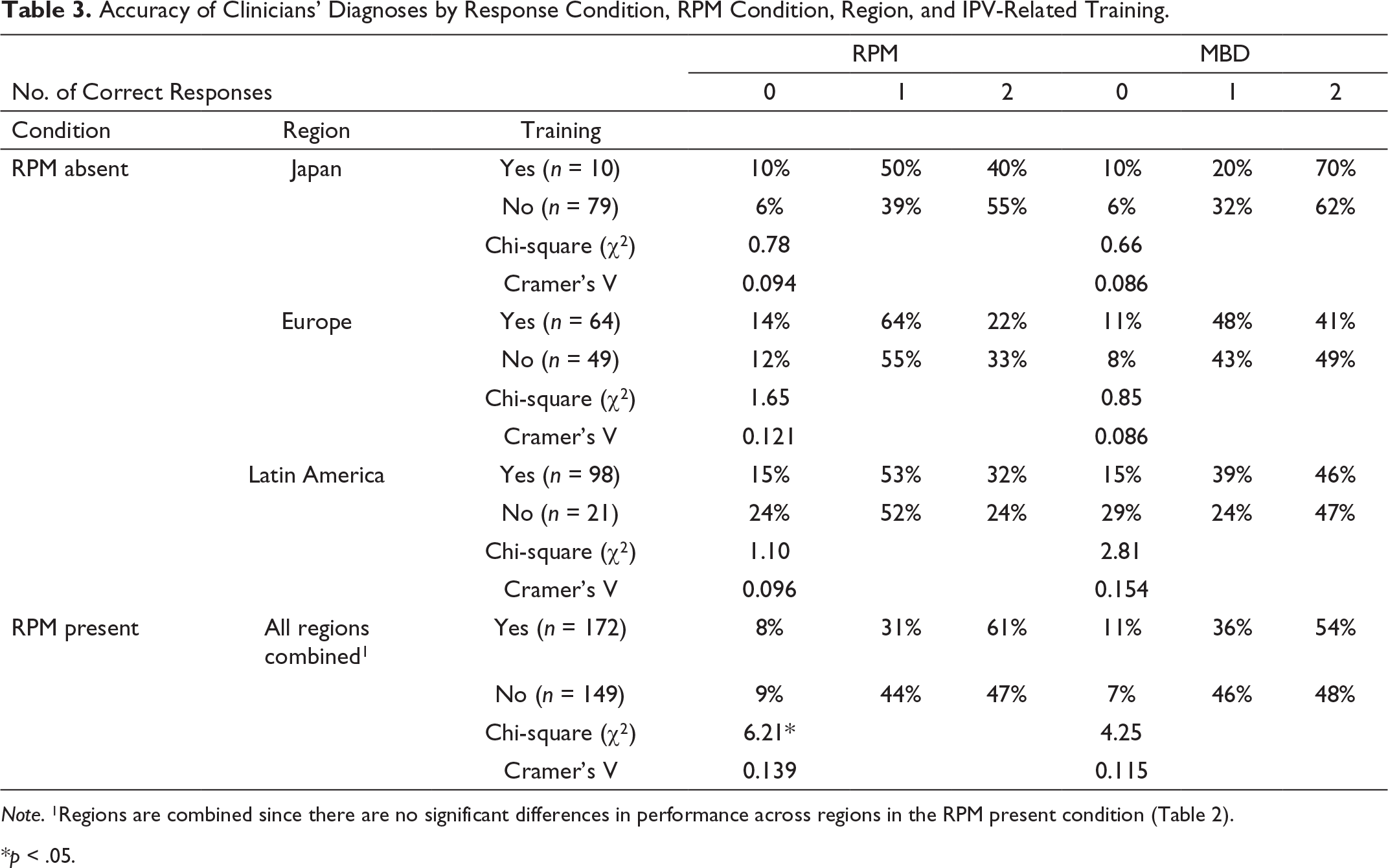
Note. 1Regions are combined since there are no significant differences in performance across regions in the RPM present condition (Table 2).
*p < .05.
Table 3 also shows clinicians’ performance when assessing for RPM and MBDs when RPM is present. Results showed that clinicians with IPV-related training (n = 172) were significantly more likely than those without training (n = 149) to have more correct responses when identifying RPM. As anticipated, there was no relationship between IPV-related training and the likelihood of correctly identifying a MBD.
Training factors (i.e., timing of training, number of hours, and depth of content) were examined to determine their impact on the likelihood of accurately identifying RPM.
Timing of training:
Hours of training: Two multinomial logistic regressions were carried out to investigate whether the number of hours of IPV-related training (during professional training and since completing professional training, respectively) were related to clinicians’ accuracy in identifying RPM (i.e., the likelihood of having 0, 1, or 2 correct responses). Boxplots adjusted for skewed distributions (Walker et al., 2018) were used to detect and remove outliers for each “number of hours of IPV-related training” variable (i.e., during professional training [n = 5], and since completing professional training [n = 8]). Multinomial regression results showed that the number of hours of training did not significantly predict the likelihood of having a greater number of correct responses, either during professional training (χ2(2, n = 148) = 1.40, p >.05) or after professional training (χ2(2, n = 152) = 0.57, p >.05).
Depth of training. The WHO recommends 4 components to be included in IPV-related training protocols (i.e., basic information on IPV, information about local support services for survivors, how and when to inquire about IPV, and how to offer support to survivors; WHO & PAHO, 2013). Depth of training was defined as the number of training components that participants reported receiving as part of their IPV-related training. Less than half of participants (49.4%, n = 85) indicated that all 4 components were part of their training, and 31 participants (18.0%) noted that their training contained only one component, most often basic information on IPV (n = 15). Twenty-nine participants (16.9%) reported receiving two components of training, most often basic information on IPV paired with information about local support services (n = 14). Twenty-nine clinicians (16.9%) reported three components of training, most often basic information on IPV paired with how and when to inquire about IPV and how to offer support to survivors (n = 11). Four participants (2.3%) indicated that they received training that contained none of these components. A full report of participants’ IPV-related training experiences is provided in (Burns et al., 2020).
Accuracy of Clinicians’ Diagnoses of RPM by Number of Training Components.
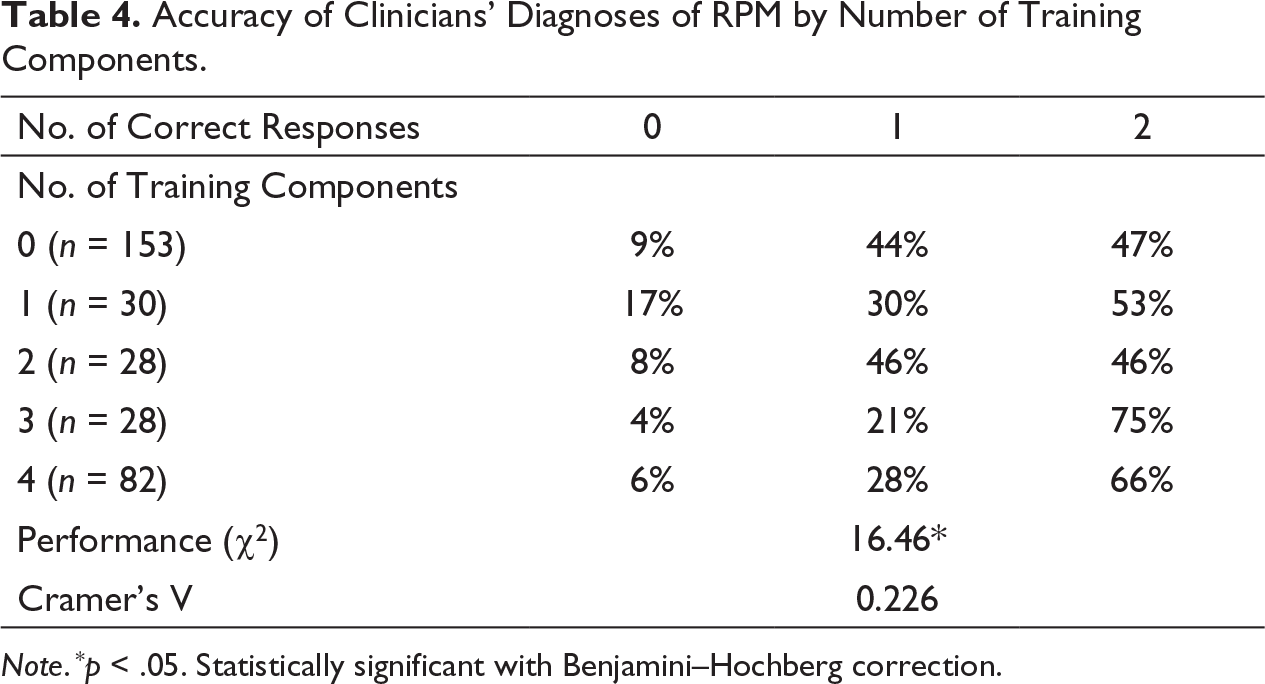
Note . * p < .05. Statistically significant with Benjamini–Hochberg correction.
Discussion
This study explored the relationship between global psychologists’ and psychiatrists’ IPV-related training experiences and diagnostic accuracy in the context of relationship problems and partner violence. Specifically, we hypothesized that IPV-trained clinicians with training more closely resembling WHO recommendations (WHO, 2013) would be more likely than those without training to accurately distinguish among different forms of clinically significant RPM and normative relationship problems. This study also assessed differences in performance between the use of ICD-11 versus ICD-10 RPM guidelines within our sample.
The findings show that, across all study conditions, the use of ICD-11 guidelines did not improve participants’ performance over ICD-10 for specific case vignettes. Heyman et al. 2018 reported on the English-language data and found that ICD-11 outperformed ICD-10. These authors considered participants to have correctly responded if they selected any RPM category, regardless of whether it was the one described in the vignette. This was done to increase comparability between ICD manuals. In contrast, in the current study, to measure response accuracy participants were only rated as having a correct response if they selected the specific RPM described in the vignette. Results from both studies suggest that ICD-11 guidelines assist clinicians in identifying when an RPM is present but are less helpful in making accurate distinctions between different forms of relationship problems. Further review and revision of proposed ICD-11 RPM guidelines may be needed to address this issue, prior to the planned release of the ICD-11 clinical descriptions and diagnostic guidelines in 2022. Importantly, this finding highlights the need for additional training to assist clinicians in making accurate assessments of patients presenting with relationship problems, including IPV.
To determine whether clinician factors impacted performance, we assessed the relationship between seven demographic variables and participants’ diagnosis of RPM and MBDs in two study conditions (RPM present; RPM absent). Findings showed that when the task was to correctly identify an RPM (i.e., RPM present condition), none of the demographic variables impacted performance. However, when the task was to correctly identify the absence of RPM (i.e., RPM absent condition), significant differences in performance were found across regions. Clinicians from Europe and Latin America were more likely to misclassify normative relationship problems as clinically significant RPM, compared to participants from Japan. Cultural differences in clinical decision-making may have influenced these results. Western clinicians have been found to employ a more analytical approach to diagnosis, retaining only details that assist in making categorical judgments, whereas East Asian clinicians appear to take a more holistic approach by gathering and remembering various types of details (Nisbett et al., 2001). Vignettes were created to depict normative relationship problems with features that fell just below the threshold for an RPM. It is possible that clinicians from Europe and Latin America (i.e., Western) were more likely than Japanese clinicians to adopt an analytical approach and sought to fit subthreshold vignette features to clinical guidelines, leading to over-identification of RPM.
A second possible explanation for regional differences in performance is that certain cultural factors may impact clinicians’ familiarity with diagnosing relationship problems in clinical practice. Research suggests that Japanese individuals hold more patriarchal gender norms than individuals living in Western countries (Hofstede et al., 2010; Yamawaki et al., 2009), which can contribute to the perception of IPV as a private family matter rather than a public health issue (Nagae & Dancy, 2010; Nguyen et al., 2013; Yamawaki et al., 2009). IPV survivors in Japan report feeling ashamed of disclosing violence (Nagae & Dancy, 2010; Weingourt et al., 2001), and a national survey revealed that only 6% of women who experienced IPV had disclosed this to a health professional (Cabinet Office, 2012, as cited in Umeda et al., 2017). This is a lower rate of disclosure than reported in Western countries (e.g., Canada, where 32% of IPV survivors disclosed violence to a health care worker; Mont et al., 2005). Furthermore, a randomized control trial of IPV screening practices in Japanese antenatal care found that women were more likely to disclose IPV using a self-report questionnaire, compared with a face-to-face interview with a health provider (Kataoka et al., 2010). It is possible that these cultural factors could contribute to Japanese clinicians having less experience assessing and identifying relationship problems in their regular practice, compared with clinicians from other regions. Thus, when presented with ambiguous patient presentations, participants from Japan may have been more likely to rely on ICD guidelines to make correct diagnoses. In contrast, participants from Europe and Latin America, who may have more clinical experience with IPV, could have been more likely to apply clinical intuition instead of guidelines to diagnose vignettes, leading to over-identification of RPM
Findings also showed that in both study conditions (i.e., RPM present; RPM absent), age and years of professional experience were related to performance when assessing for a MBD. Younger clinicians and those with less experience were more likely to correctly diagnose a Mental or Behavioral Disorder (presence or absence), compared with older clinicians and those with more experience. Clinicians with more experience are more likely to rely on faster intuitive judgment than slow, deliberate, analytical judgment when presented with familiar patient presentations (Schwartz & Elstein, 2009). Intuitive judgment relies on heuristics, and although it is more time-efficient, it can lead to diagnostic errors (Croskerry & Nimmo, 2011). It is possible that when presented with patients describing familiar mood and anxiety symptoms, older clinicians with more experience were more likely to rely on intuitive judgment than younger clinicians with less experience, leading to misclassification of subthreshold mood and anxiety symptoms as clinical disorders.
The main findings of this study described the relationship between IPV-related training and mental health clinicians’ performance when assessing for RPM across two study conditions: when RPM was present (i.e., when the task was to identify RPM and distinguish between its different forms), and when RPM was absent (i.e., when the task was to distinguish between normative relationship problems and RPM). In the RPM-absent condition, results showed that across all regions, IPV-related training was unrelated to performance. Specifically, clinicians with and without training appeared to have similar difficulty with correctly identifying that RPM was absent. Amongst clinicians without training, 45%–76% incorrectly classified normative relationship problems as RPM on at least one occasion. Similarly, 60%–78% of clinicians who had received IPV-related training made at least one classification error across the two presented vignettes. It is possible that over-identification of RPM was related to the study design, whereby clinicians were asked to assess for RPM and therefore may have been more likely to assign subclinical features to clinically significant RPM. Nonetheless, these results suggest that IPV-related training programs may benefit from including specific guidelines on how to distinguish normative relationship problems from clinically significant RPM.
In the RPM present condition, participants who had prior IPV-related training were more likely than those without training to accurately identify RPM. This finding suggests that IPV-related training assists mental health clinicians in making more accurate clinical decisions while assessing patients presenting with RPM. It builds on previous research citing benefits of IPV-related training including improved knowledge and confidence with regards to addressing IPV (Burns et al., 2020; Forsdike et al., 2019; Jayatilleke et al., 2015) and improved IPV-related screening practices (Murray et al., 2016). As hypothesized, in both the RPM-present and RPM-absent conditions, IPV-related training was not associated with clinicians’ performance while identifying a MBD. This suggests that participants’ superior performance while assessing for RPM is related to IPV-related training specifically, rather than their amount of overall professional training. Clinicians with more overall training would presumably have also performed better at identifying a MBD.
To help inform IPV-related training protocols, the current study also sought to explore the relationship between performance and different components of IPV-related training, based on the WHO’s evidence-based training guidelines (WHO, 2013). Our findings showed that clinicians who received training in the past five years or after completing their professional training programs were more likely to accurately identify RPM than clinicians without training. Clinicians who had received IPV-related training during their professional training programs, however, were not more likely than those without training to correctly identify RPM. Furthermore, the number of hours of IPV-related training was not related to performance. Overall, these results imply that the recency of IPV-related training is more important than the amount of training to improve RPM identification. In line with WHO training recommendations (WHO, 2013), this suggests that clinicians would benefit from periodic IPV-related training throughout their careers.
This study also looked at the relationship between the number of WHO-recommended IPV-related training components and performance. WHO guidelines propose that IPV-related training should include didactic components (i.e., basic information about IPV, and local support services for survivors), and skills training components (i.e., how and when to inquire about IPV, and how to offer support to survivors; WHO, 2013). Our findings show that clinicians whose training included three or four of the recommended components were significantly more likely to correctly identify RPM than participants without training. However, participants whose training contained only one component (most commonly basic information about IPV) or two components (most commonly basic information about IPV combined with information about local support services) performed similarly to those without training. It appears that clinicians whose IPV-related training more closely resembled WHO training recommendations were more likely to perform well at identifying RPM. Because clinicians who received three or more training components necessarily participated in at least one skills training exercise (i.e., learning how and when to inquire about IPV and/or how to respond to IPV), these results suggest that training that only provides basic information about IPV, without the addition of more experiential skills training, is not enough to improve clinical decision-making in the context of RPM. IPV-related training programs should be delivered in-depth and include experiential learning tasks. This finding in line with previous research showing that clinicians who participated in experiential IPV-related training activities, compared with didactic training, were more likely to report improved IPV-related attitudes and knowledge (Buranosky et al., 2012).
Limitations
Participants in this study were clinicians who volunteered to be members of the WHO’s GCPN and responded to an invitation to participate in an online field trial for the revision of the ICD-11 relationship problem and maltreatment guidelines. Only 10% of GCPN members who were sent an invitation constituted the final sample. These clinicians may have chosen to participate because they had expertise in the assessment and treatment of patients presenting with RPM. Furthermore, participants were psychologists and psychiatrists only, from high-income (64.2%) and middle-income countries (35.8%) across three global regions: Japan, Europe (French- and Spanish-speaking Europeans only), and Latin America. Thus, results may not be generalizable to a broader sample of global mental health professionals.
A vignette-based method was used in this study to experimentally control case presentation. Research supports the use of vignettes as a valid and reliable method for assessing clinical practice (Evans et al., 2015); however, vignettes are necessarily brief and may lack the richness of information that clinicians would collect in their regular practice. Furthermore, clinicians’ assessment of RPM in real-world clinical practice may be impacted by factors (e.g., discomfort asking about IPV; Sprague et al., 2012) that are absent in a vignette-based study. Thus, this study can only provide an analogue of participants’ real-world assessment of RPM. Vignettes depicted patients presenting with relatively mild RPM, which included instances of IPV (i.e., physical and psychological partner violence) that met minimum definitional requirements for an RPM, as well as relationship distress with a spouse or intimate partner. Relationship distress is not a form of IPV; it was included because it is an important risk factor for IPV (Stith et al., 2008) and is associated with negative mental health outcomes (e.g., depression, anxiety, and alcohol use disorder; Foran et al., 2015; Whisman, 2007). Less prevalent forms of IPV (e.g., sexual partner violence) were not included due to concerns about survey length. Thus, this study reports on the relationship between IPV-related training and clinicians’ assessment of milder forms of RPM and may not be representative of clinical decision-making in the context of more severe IPV (e.g., intimate terrorism).
Clinicians’ experiences of IPV-related training were measured using self-report data and may have been subject to bias. For example, participants could have inflated their training experiences to appear more socially desirable, or may have had difficulty accurately recalling the timing, duration, and content of their IPV-related training. Training experiences were also observed rather than experimentally manipulated, signifying that the content of training could vary widely across participants. Although we assessed for specific components of IPV-related training based on WHO training recommendations, it is possible that participants’ unique training experiences included elements not captured in our survey that could have influenced performance. Moreover, participants were asked to select as many WHO-recommended training components as were included in their IPV-related training program from a drop-down list. Although this provided information on the characteristics of clinicians’ training (e.g., content and number of components), participants’ responses to this question were not independent and therefore it was not possible to compare between training components to determine which were more strongly related to performance.
Conclusion
This study evaluated the relationship between the use of ICD guidelines, IPV-related training, and global psychologists’ and psychiatrists’ accuracy when assessing for relationship problems, including IPV. Findings suggest that the use of descriptive ICD guidelines is not sufficient to guide clinicians in making accurate clinical decisions in the context of RPM. As such, study results will be used to assist the WHO in making improvements to proposed RPM guidelines for inclusion in the ICD-11. Results also imply that IPV-related training leads to improved diagnostic decision-making in the context of RPM. Clinicians who received IPV-related training were more likely than their counterparts to accurately distinguish between different forms of RPM and normative relationship problems. Training appeared to yield the best results when it was delivered recently and contained at least three WHO-recommended training activities, including more experiential skills training exercises. Overall, these findings provide empirical support for the WHO’s IPV-related training guidelines (WHO, 2013). Interestingly, clinicians with and without training appeared to misclassify normative relationship problems as RPM, suggesting that IPV-related training programs should also provide guidance on how to distinguish between normative and clinically significant relationship problems.
This study provides a glance at the relationship between global mental health professionals’ experiences of IPV-related training and their diagnostic accuracy when assessing for relationship problems. Results can help to inform the development of IPV-related training programs to improve clinicians’ decision-making in the context of RPM. Future research may expand on these findings by experimentally manipulating clinicians’ experiences of IPV-related training in real-world settings, for improved ecological validity and better specification of components for inclusion in training programs.
Footnotes
Acknowledgments
The opinions contained in the article are those of its authors and, except as specifically stated, are not intended to represent the official policies or positions of the WHO. The authors are grateful to the following individuals for their assistance with statistical consultation, translation and testing of the study materials: statistical consultation: Jared Keeley; French translation: Stéphane Sabourin; Japanese translation: Yukiro Morino; Spanish translation: Alejandra González Salas, Omar Hernández, Carolina Muñoz, and Juan F. Rodríguez-Testal.
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.