
Abstract
Young women who have had contact with the criminal justice system (justice-involved young women) have an increased risk of being a victim of violence. However, no reviews have synthesized the evidence on interventions to prevent or respond to violence against justice-involved young women. We conducted a scoping review to identify interventions designed to prevent or respond to violence against justice-involved young women. We searched Medline, Criminal Justice Abstracts, Web of Science, and Google Scholar for peer-reviewed and gray literature published in English from January 1, 2000 until March 23, 2021. Consistent with the public health approach to violence, we included primary, secondary, and tertiary interventions. Excluding duplicates, our search returned 5,603 records, 14 of which met our inclusion criteria. We narratively synthesized the included studies, all of which were conducted in the United States. Most included studies examined a tertiary intervention (n = 10), and few examined a primary (n = 2) or secondary (n = 2) intervention. Across the Joanna Briggs Institute Critical Appraisal Tools, the percentage of items met ranged from 0% to 78%. There was some limited evidence that tertiary interventions that included cognitive behavioral therapy reduced the mental health impacts of violence victimization among justice-involved young women. There was little evidence on primary and secondary interventions. Effective and evidence-based interventions to prevent violence victimization and revictimization against justice-involved young women remains a critical gap in knowledge.
Critical Findings
There is a dearth of interventions that have been designed to prevent violence victimization or revictimization among justice-involved young women. Of the interventions that have been developed, very few have been rigorously evaluated.
Research in this area has focused on addressing the impacts of violence victimization (i.e., tertiary prevention).
There is some evidence that interventions that include cognitive behavioral therapy may reduce the mental health impacts of violence exposure (e.g., post-traumatic symptoms) among justice-involved young women.
Effective, evidence-based primary and secondary violence prevention strategies are urgently needed for justice-involved young women to reduce violence victimization and revictimization.
We identified critical geographical gaps in the literature. All of the published research on interventions to prevent violence against justice-involved young women has been conducted in the United States, which may have limited generalizability to other countries.
Implications for Practice, Policy, and Research
There is a need for all types of violence prevention (i.e., primary, secondary, and tertiary prevention) across different settings (e.g., detention and community settings) to effectively prevent and respond to violence victimization and revictimization among justice-involved young women.
Cognitive behavioral therapy may be a promising option to reduce the mental health impacts of violence victimization among justice-involved young women.
Future research should incorporate the views, experiences, and perspectives of justice-involved young women in designing programs and interventions to prevent and respond to violence. This may assist understanding what works, for whom, and under what circumstances.
Multisectoral data linkage and participatory methods are rigorous and complementary approaches that may assist in evaluating interventions that aim to prevent and respond to violence against justice-involved young women.
Research on interventions to prevent and respond to violence against justice-involved young women is urgently needed from countries other than the United States.
Introduction
In high-income countries, young people (aged <25 years; Sawyer et al., 2018) are more likely than other age groups to be involved in the criminal justice system (i.e., criminalized through contact with police, courts, community corrections, youth detention, or imprisonment—hereafter “justice-involved”) (Richards, 2011). Globally, young people have a higher rate of dying from violence in 1 year compared to adults (United Nations Office on Drugs and Crime, 2019). Many of the correlates of violence victimization—including mental illness, substance use issues, and homelessness—are highly prevalent among justice-involved young people (Borschmann et al., 2020; Hughes et al., 2020), particularly young women (Chesney-Lind et al., 2008; Mullis et al., 2004). Justice-involved young women comprise approximately 6% of all incarcerated young people aged under 18 years (United Nations, 2019), but generally experience worse health outcomes and more disadvantage than both their male counterparts (Borschmann et al., 2020) and young women in the general population (Kerig, 2018).
Although the vast majority of young women who are victim-survivors of violence do not have contact with the criminal justice system, many young women who have contact with the criminal justice system have experienced violence. In the United States, it is estimated that between 70% and 96% of justice-involved young women have been a victim of violence at some stage in their life (Kerig & Ford, 2014). Compared to young men, these young women disproportionately experience family violence, intimate partner violence, and sexual violence perpetrated by peers, family members, or trusted adults, and often experience multiple co-occurring forms of violence (Kerig, 2018). For many young women, their criminal justice system involvement stems directly or indirectly from the trauma they have experienced because of violence (Prison Reform Trust, 2017; Saxena et al., 2014a; Stathopoulos et al., 2012). For example, young women may use substances as a coping mechanism after experiencing violence, which may lead to substance-related charges being brought against them (Saxena et al., 2014b). Alternatively, young women may be misidentified, and subsequently arrested, by police as the predominant aggressor of violence in an intimate partner violence incident (Nancarrow et al., 2020; No to Violence, 2019).
The number of young and adult women who are being incarcerated in the criminal justice system is increasing globally at approximately twice the rate of males (Walmsley, 2017). This highlights the need to build knowledge about effective violence prevention initiatives that respond to the needs of justice-involved young women. Eliminating violence against women and girls is a key target for the United Nations Sustainable Development Goals (target 5.2) (United Nations Department of Economic and Social Affairs, 2015). Although justice-involved young women are particularly at risk of violence, no reviews have synthesized the evidence on interventions to prevent or respond to violence against this group. As such, there is currently little understanding of what interventions are available that may be effective in addressing these young women’s risk of violence victimization. Scoping reviews are a useful method for providing an overview of the available evidence in an area (Arksey & O’Malley, 2005). To this end, we conducted a scoping review to examine (a) what is known from the existing peer-reviewed and gray literature on interventions to prevent or respond to violence against young women who have had, or are at risk of having, contact with the criminal justice system, and (b) whether any of these interventions have been found to be effective in preventing violence victimization, revictimization, or the impacts of violence.
Method
Overview
Our scoping review is reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (Tricco et al., 2018) and is consistent with the scoping review framework outlined by Arksey and O’Malley (2005). The protocol for this scoping review is registered on Open Science Framework (Willoughby et al., 2021a) on October 14, 2021, after the database searches had been completed.
Theoretical Framework
Consistent with international approaches (Krug et al., 2002), this review is informed by the public health approach to violence (Lee, 2017). This approach recognizes the impact of violence on health and views violence as a preventable condition that can be addressed by targeting socio-ecological factors that influence the risk of violence (Lee, 2017). The public health approach to violence classifies interventions into three categories: primary, secondary, and tertiary (Lee, 2017). Primary interventions aim to prevent violence before it occurs by focusing on the conditions, behaviors, and attitudes that drive violence (e.g., programs aiming to improve understanding of healthy relationships; Lee, 2017). Secondary interventions refer to responses to violence that aim to prevent reoccurrence of violence and mitigate short-term effects of violence (e.g., hospital-based assault revictimization prevention programs; Lee, 2017). Tertiary interventions include programs that seek to address the ongoing and long-term health consequences of violence (e.g., treatment for post-traumatic stress disorder [PTSD]; Lee, 2017). A comprehensive violence prevention strategy requires all three types of interventions (Lee, 2017).
Search Strategy
We searched three key health: criminology, and social science databases: Medline, Criminal Justice Abstracts, and Web of Science, using terms related to young women, violence prevention, and criminal justice involvement. The searches were limited to articles published from January 1, 2000 to March 23, 2021 to ensure that the review considered contemporary evidence. The search strategy was developed in consultation with a librarian at the Murdoch Children’s Research Institute in Melbourne, Australia (Supplemental Appendix A). We also conducted a keyword search in Google Scholar to identify additional relevant gray literature (Supplemental Appendix B). Reference lists of included studies were screened to identify additional relevant literature not identified in the database search.
Selection Criteria
Studies were eligible for inclusion if they evaluated or described a primary, secondary, or tertiary intervention (described above) that aimed to prevent or respond to violence against young women (aged <25 years, as recommended by Sawyer et al. (2018)) who have had, or are at risk of having, contact with the criminal justice system. We used the United Nations’ definition of violence against women: any act that results in, or is likely to result in, physical, sexual, or psychological harm or suffering to women (United Nations, 1993). To ensure that our review was comprehensive in capturing the available evidence in this area, our inclusion criteria were intentionally board. We included any measures of violence victimization (e.g., rates of assault, experiences of victim-survivors), factors that may influence violence victimization (e.g., sexual self-efficacy and knowledge of healthy relationships), and long-term mental health impacts of violence (e.g., symptoms of PTSD and depression).
Studies that included women aged 25 years and over were included if the mean or median age of the participants was under 25, or if the results were stratified by age. Criminal justice system contact included: contact with a criminal court or the police, being on bail or parole, serving a community-based order, being held on remand or in police custody, or current or previous incarceration in a youth detention facility or prison. Studies of young women described as “at risk” of criminal justice system contact were also included, as many young women experience violence before they have contact with the criminal justice system (Malvaso et al., 2016; Wilson et al., 2009), and to be consistent with previous research (Goodkind et al., 2006). For the purposes of the review, young women were determined to be “at risk” of criminal justice system contact if they described as such in the original study. Literature reviews, letters, commentaries, editorials, conference abstracts, and studies published in languages other than English were excluded. Reference lists of previous reviews were screened for additional eligible studies.
Study Selection
Citations from the database search were imported into EndNote X8.2 reference management software (Clarivate Analytics, 2018), then uploaded into Covidence for screening and de-duplication (Covidence, n.d.). MW, CGW, and SKw independently screened potentially eligible studies by title and abstract. Eligibility criteria were piloted to ensure that they were relevant to the identified studies. Pilot screening involved MW, CGW, and SKw independently reviewing the same 30 titles and abstracts to see if any changes or clarifications needed to be made to the eligibility criteria. No changes to the eligibility criteria were made during piloting. After title and abstract screening, the full texts of the remaining studies were screened in duplicate by two of the same three researchers (MW, SKw, or CGW). The Google Scholar searches were conducted by TC and Alex Andrawis. Any uncertainties regarding eligibility were resolved through group discussion and consensus.
Data Extraction and Quality Assessment
Data extraction was conducted independently by MW and EJ using a prespecified Microsoft Excel form. EJ and SKw checked the data extraction and amended any errors. A summary of the information extracted from the included studies is presented in Supplemental Appendix C. Although a quality assessment is not always required in a scoping review (Arksey & O’Malley, 2005), we conducted a critical appraisal of individual studies to assess the quality of evidence supporting potentially effective interventions to prevent or respond to violence. The quality of included studies was assessed independently by CGW, EJ, and MW using the Joanna Briggs Institute (JBI) Critical Appraisal Tools (Johanna Briggs Institute, n.d.). Only peer-reviewed studies and gray literature that measured an effect change in an outcome of interest were quality assessed.
Data Synthesis
We provide a descriptive overview of the characteristics of the included studies. We narratively synthesized the included studies by intervention type (i.e., primary, secondary, and tertiary) and whether the studies evaluated the intervention.
Ethics
The scoping review is exempt from ethics approval as it is based on findings of published studies. This review followed best practice recommendations for conducting and reporting scoping reviews (outlined above).
Results
Our search retrieved 6,937 records (Figure 1). After duplicates were removed, 5,603 records were screened by title and abstract. Of these, 81 were screened by full text. Fourteen studies (12 peer-reviewed articles and 2 gray literature reports) met the eligibility criteria and were included in the review.
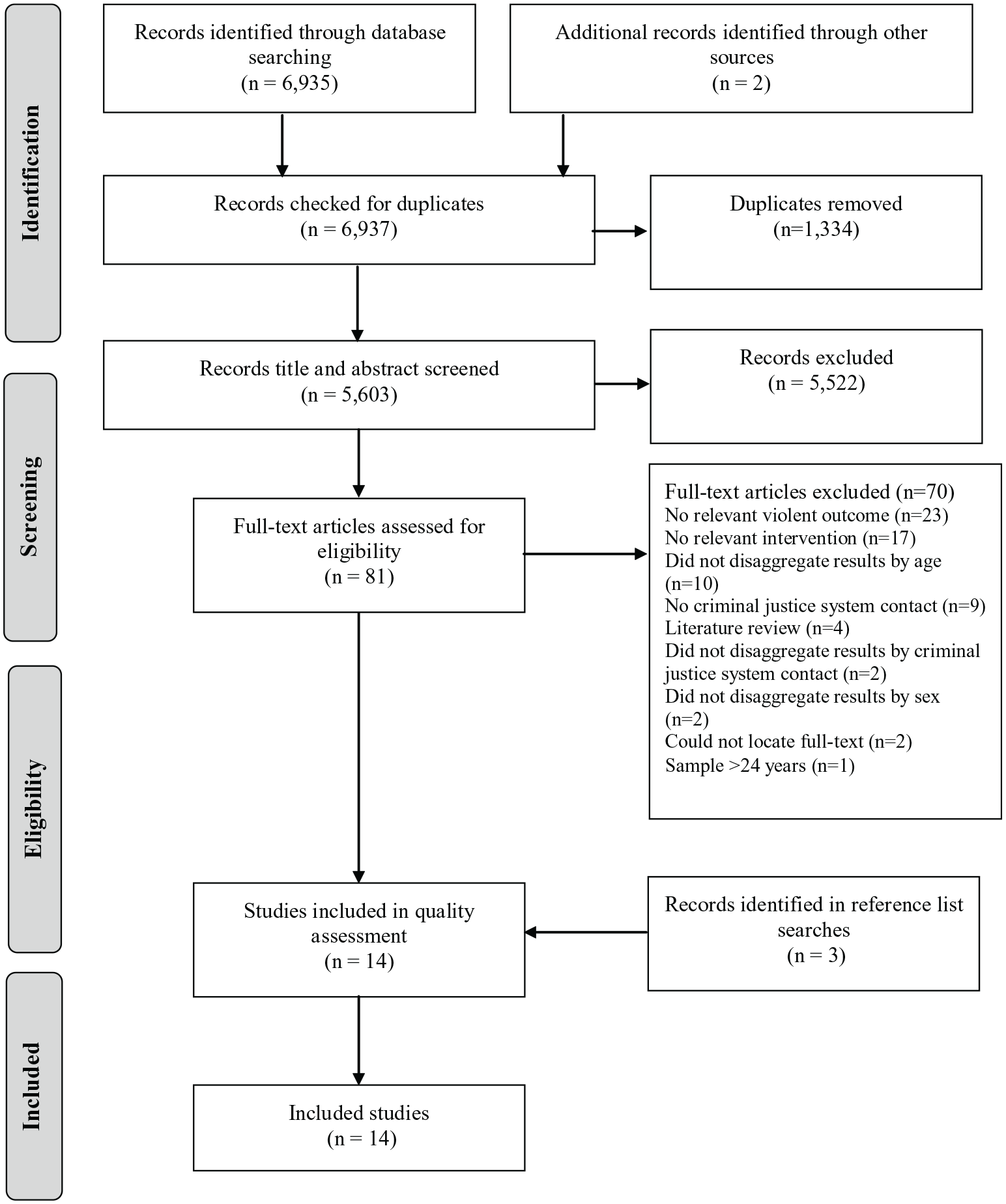
PRISMA flowchart.
Study Characteristics
All 14 included studies were conducted in the United States (see Table 1). Most studies described or evaluated a tertiary intervention (n = 10), and few studies examined primary (n = 2), or secondary (n = 2) interventions (see Table 2). Half of the studies examined young women who were incarcerated, including in youth detention (n = 6) (Arnold et al., 2002; Emerson & Shelton, 2001; Middleton et al., 2019; Palidofsky & Stolbach, 2012; Roe-Sepowitz et al., 2009; Shekar et al., 2020) and in an adult county jail (n = 1) (Pomeroy et al., 2001). Two studies examined community-based samples, including young women who were released from detention (n = 1) (Harris & Malone, 2014) or on probation (n = 1) (Davidson et al., 2011). An additional three studies examined combined samples of young women in detention and in the community (e.g., on probation and contact with a diversion program or a court) (Burke et al., 2003; Gaarder & Hesselton, 2012; Kelly et al., 2007). Two studies included combined samples of young women who were considered “at risk” of criminal justice system contact and young women who had contact with the criminal justice system (e.g., arrested, on probation, and contact with a juvenile justice program). “At risk” of criminal justice system contact was defined in these studies as self-reported delinquency using the Self-Report Delinquency Behavior Scale (Ford et al., 2012), and as having risk factors for criminal justice system contact (e.g., having friends who have a criminal record) (Millenky et al., 2019). Among studies that reported mean age (n = 9 studies), the mean age of the participants at baseline ranged from 15 to 16 years (see Table 1). The youngest participant at baseline in the included studies was aged 11 years, and the oldest was aged 20 years. Ten studies reported on the race and/or ethnicity of the sample. There was little consistency in the way that race/ethnicity was reported across the studies. The most frequently reported racial and ethnic groups were White/Caucasian (n = 10 studies; range 4%–46%), Black/African American (n = 8 studies; range 5%–73%), and Latina/Hispanic (n = 7 studies; range 16%–75%; see Table 1).
Characteristics of Included Studies.
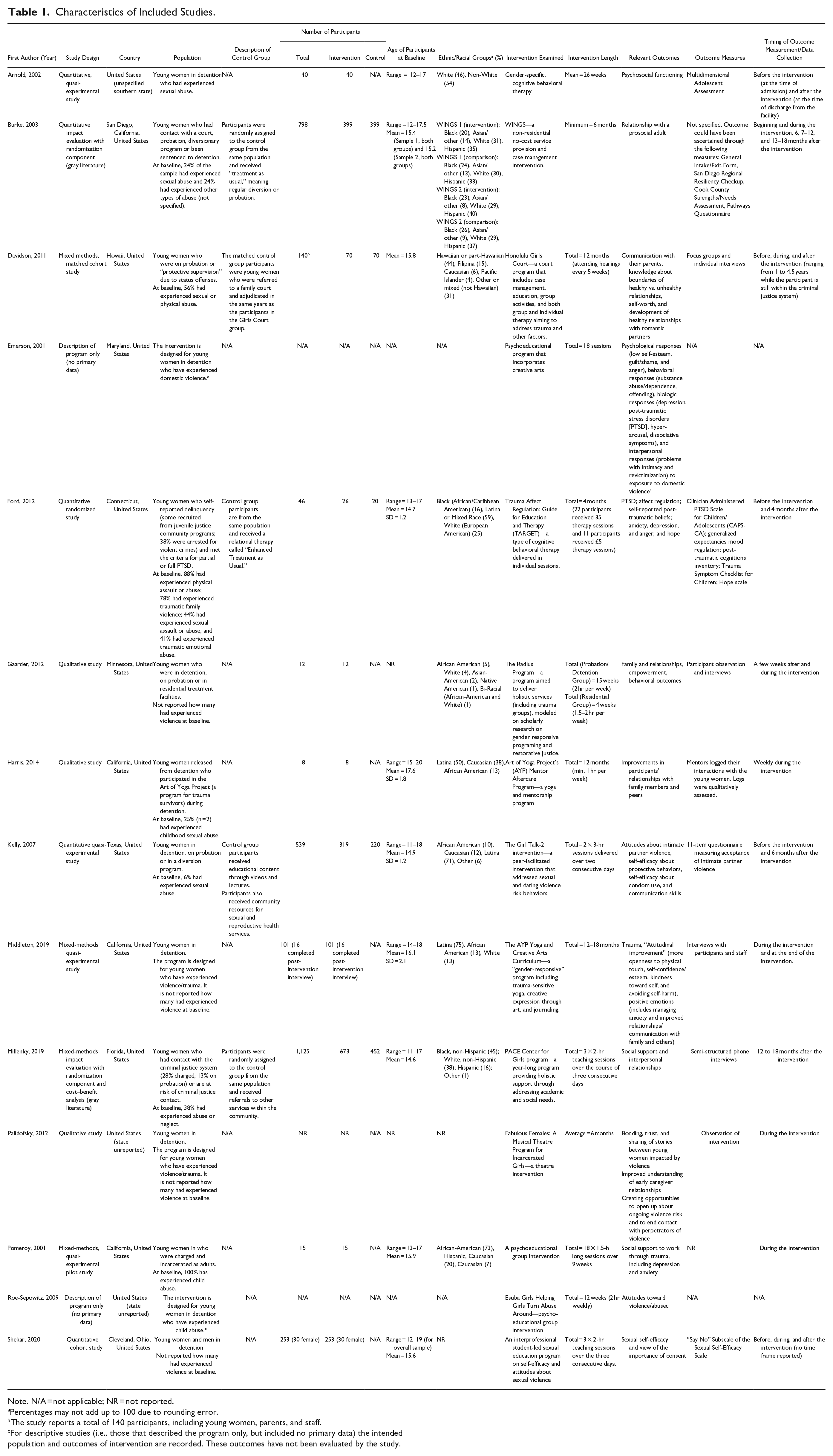
Note. N/A = not applicable; NR = not reported.
Percentages may not add up to 100 due to rounding error.
The study reports a total of 140 participants, including young women, parents, and staff.
For descriptive studies (i.e., those that described the program only, but included no primary data) the intended population and outcomes of intervention are recorded. These outcomes have not been evaluated by the study.
Overview of Interventions Included in the Review.
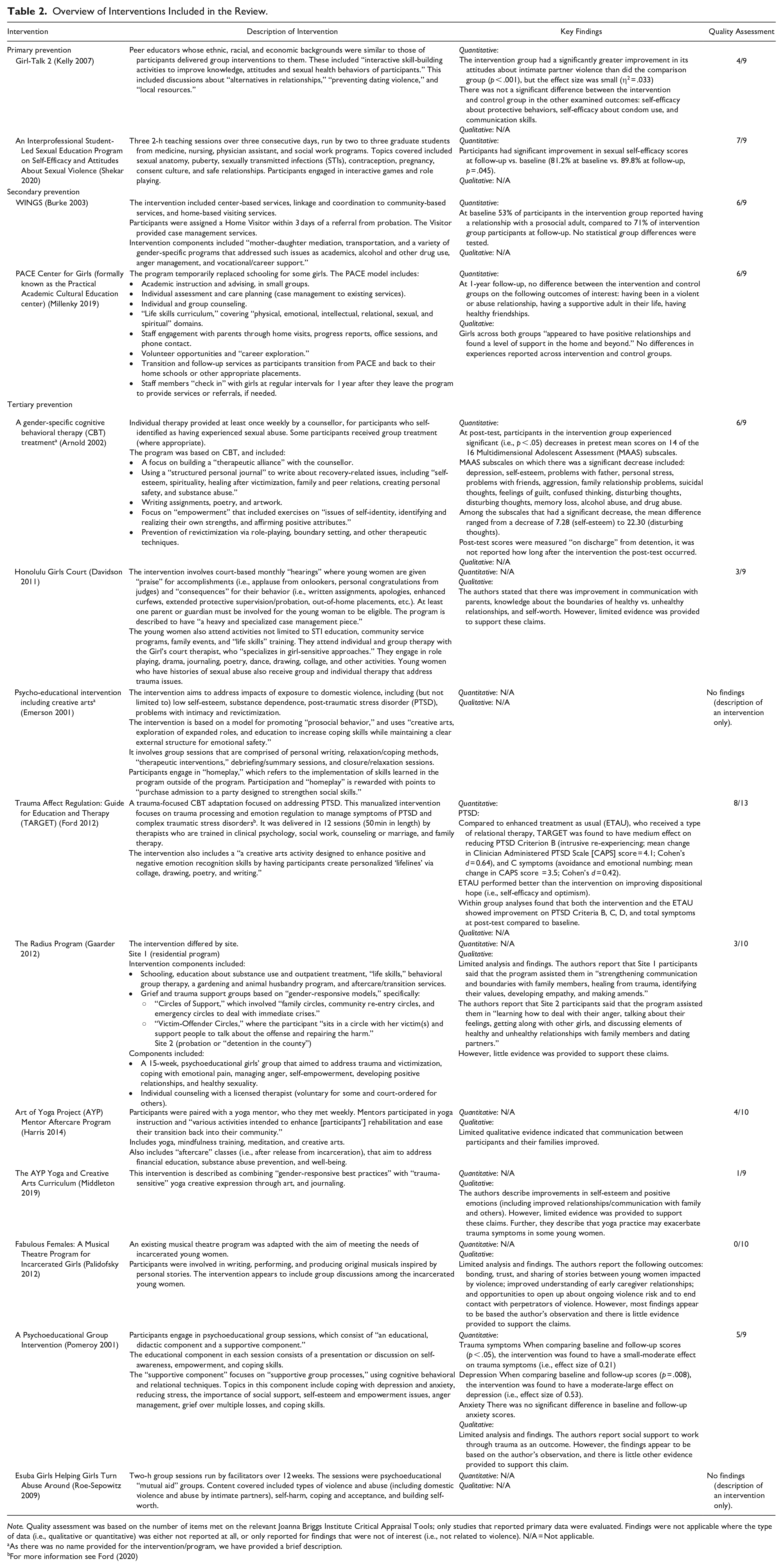
Note. Quality assessment was based on the number of items met on the relevant Joanna Briggs Institute Critical Appraisal Tools; only studies that reported primary data were evaluated. Findings were not applicable where the type of data (i.e., qualitative or quantitative) was either not reported at all, or only reported for findings that were not of interest (i.e., not related to violence). N/A = Not applicable.
As there was no name provided for the intervention/program, we have provided a brief description.
For more information see Ford (2020)
Twelve studies evaluated an intervention and two studies (Emerson & Shelton, 2001; Roe-Sepowitz et al., 2009) provided descriptions of an intervention with no primary outcome data reported. Of the 12 studies that evaluated interventions, most used quasi-experimental designs (n = 8; see Table 1). There was only one randomized controlled trial (RCT), which examined an individual therapy intervention (Ford et al., 2012). Five studies that evaluated an intervention reported quantitative data only, three reported qualitative data only, and four used mixed methods (see Table 2). In terms of quality, no studies met all of the items on the JBI Critical Appraisal Tools (Johanna Briggs Institute, n.d.). Across the Critical Appraisal Tools, the percentage of items met ranged from 0% to 78% (see Table 2). Limitations in quality that were common in quantitative studies included lack of control groups or control groups that did not allow for meaningful comparisons, short follow-up periods, lack of reported follow-up fractions, and inappropriate or unclear statistical analysis. Limitations that were common across qualitative studies included poorly described qualitative methodology and synthesis. Across both quantitative and qualitative studies, limitations in quality included insufficient or no explanation of participant characteristics and settings, and lack of explicit ethics approvals.
Primary Interventions
We found two studies that evaluated primary interventions (Kelly et al., 2007; Shekar et al., 2020) (see Table 2). The interventions examined by these studies included: (a) a sexual health and violence education group intervention delivered by peer educators from similar ethnic, racial, and economic backgrounds to participants (Kelly et al., 2007) and (b) a graduate student-led sexual education program (Shekar et al., 2020). There was some, albeit limited, evidence to support the effectiveness of these interventions across the studies. One study, which examined a peer educator program (Girl-Talk 2), reported that at 6-month follow-up, participants in the intervention group had a significantly greater improvement in attitudes about intimate partner violence than the comparison group (p < .001) (Kelly et al., 2007). In this study, attitudes about intimate partner violence were measured using an 11-item questionnaire on attitudes indicating acceptance of intimate partner violence among 539 justice-involved young women (mean age = 15 years). However, the effect size of this difference was small (η2 = .033). There was no significant difference at 6-month follow-up between the intervention and control group in the other examined outcomes: self-efficacy about protective behaviors, self-efficacy about condom use, and communication skills. The second study, which examined a graduate-student-led sexual education program, reported that participants had a significant improvement in sexual self-efficacy scores at follow-up (i.e., 81.2% at baseline vs. 89.8% at follow-up, p = .045) (Shekar et al., 2020). In this study, sexual self-efficacy was measured using the “Say No” Subscale of the Sexual Self-Efficacy Scale among 30 young women in detention (mean age = 16 years). However, this study did not use a control group, and the scores for sexual self-efficacy were already high at baseline.
Secondary Interventions
We found two studies that evaluated a secondary intervention (Burke et al., 2003; Millenky et al., 2019). A proportion (24%–38%) of the young women included in these studies had previously been victims of violence or abuse at baseline (see Table 1). Neither study found substantial evidence to support the effectiveness of these interventions. One study found no evidence that a year-long program (the PACE center) that provided academic support, case management, parental engagement, and post-service transitional support had any effect on violence-related outcomes (i.e., having been in a violent or abusive relationship, having a supportive adult in their life, having healthy friendships) (Millenky et al., 2019). In this study, violence-related outcomes were measured in 1,125 young women (mean age = 15 years) 12 to 18 months after the intervention concluded. The second study examined a program that involved direct service provision to young women, linkage with community services, and home-based visiting services (the WINGS program) among 798 justice-involved young women (mean age = 15 years). This study had inconclusive findings that the program increased the number of justice-involved young women who had a relationship with a prosocial adult (Burke et al., 2003).
Tertiary Interventions
Most of the included studies examined tertiary interventions (n = 10; see Table 2). Of these studies, eight evaluated an intervention and the remaining two described an intervention with no primary data reported (Emerson & Shelton, 2001; Roe-Sepowitz et al., 2009). Most studies that evaluated a tertiary intervention (n = 5/8) reported on samples of young women who were in or had experienced detention (Arnold et al., 2002; Harris & Malone, 2014; Middleton et al., 2019; Palidofsky & Stolbach, 2012; Pomeroy et al., 2001). Where reported, between 25% and 100% of the young women in the samples had previously been a victim of violence or abuse at baseline (see Table 1).
The most common intervention format used across the eight studies that reported primary data were group sessions (n = 5) (Gaarder & Hesselton, 2012; Harris & Malone, 2014; Middleton et al., 2019; Palidofsky & Stolbach, 2012; Pomeroy et al., 2001). These included psychoeducational group sessions, “trauma-informed” yoga and mentorship programs, and musical theatre interventions. Findings for the effectiveness of these interventions were weak (see Table 2). One study (Middleton et al., 2019) reported that a “trauma-informed” yoga program exacerbated trauma symptoms for some of the participants 16 young women (mean age = 16 years) in detention who completed the post-intervention interviews as they felt vulnerable in some yoga poses during the program.
The other interventions examined involved individual psychotherapy or counseling (n = 3) (Arnold et al., 2002; Davidson et al., 2011; Ford et al., 2012). Two of these studies used adaptations of cognitive behavioral therapy (CBT) (Arnold et al., 2002; Ford et al., 2012). The first CBT intervention was evaluated using a pre- and post-test design and reported that participants showed decreases in personal and social problems, as measured by the Multidimensional Adolescent Assessment scale (Arnold et al., 2002).
The second CBT intervention was a trauma-focused intervention (called Trauma Affect Regulation: Guide for Education and Therapy [TARGET]) (Ford et al., 2012), which was evaluated using an RCT. This intervention was delivered to 46 young women (mean age = 15 years) who had a history of PTSD by trained therapists in a maximum of 12 sessions over 4 months. Each session was 50 min in length and included a creative arts component. Young women in the control group (n = 26) received enhanced treatment as usual (ETAU). At 4 months follow-up, the intervention was found to have a medium effect on reducing some PTSD symptoms, including intrusive re-experiencing, avoidance, and emotional numbing (see Table 2). However, ETAU performed better than the intervention on improving dispositional hope (i.e., self-efficacy and optimism).
Discussion
We conducted a scoping review to examine interventions to prevent violence victimization or revictimization, or respond to the impacts of violence against justice-involved young women. Fourteen studies, all of which were conducted in the United States, were included in our review. The majority (n = 10) of these studies evaluated or described a tertiary intervention, with few studies examining a primary or secondary intervention (n = 4). We identified critical methodological and geographical limitations of the literature, which limits our ability to draw robust conclusions.
We found that tertiary interventions that include psychological modalities (e.g., CBT and a trauma-focused CBT adaptation) are a promising option to reduce the mental health impacts of violence exposure (e.g., post-traumatic symptoms) among justice-involved young women (Arnold et al., 2002; Ford et al., 2012). A previous systematic review and meta-analysis that examined the outcomes of psychological therapies among incarcerated women and men with mental health problems found limited evidence for the effectiveness of psychological therapies (including trauma-focused therapies) in reducing trauma symptomatology (Yoon et al., 2017). Although this systematic review did not exclusively focus on trauma symptomatology among young women, taken together with our review, these findings highlight the urgent need for more research on effective responses to trauma in incarceration settings, especially for young women. Additionally, more research is needed on the design and delivery of tertiary interventions to address the impacts of violence exposure among justice-involved young women in the community, including those who have and have not experienced detention. Irrespective of the setting, future research should be consistent with the available best-practice and evidence-based guidelines on managing trauma (National Institute for Health Care Excellence, 2018). This evidence should always incorporate and align with service users’ lived experience as a key element of best practice (Glasby & Beresford, 2006).
The majority of research in this area has focused on interventions to address the mental health impacts of violence victimization among justice-involved young women. This is consistent with the findings of a previous review on violence prevention among adult and young women in the general population, which found that evaluations were skewed toward “response rather than prevention” (Ellsberg et al., 2015). Given that many young women in youth detention have histories violence and abuse victimization (Kerig & Ford, 2014), it is unsurprising that most of the tertiary interventions included in our review examined young women in detention. Supporting justice-involved young women who have experienced violence is critically important to for their health and well-being, and evidence-based interventions to address trauma should be available for young women in detention. However, detention is not an optimal environment to address trauma, and it may even be a retraumatizing experience for some young women who have experienced violence due to the lack of autonomy and practices such as body searches in detention (Anderson et al., 2020).
There is a clear lack of evidence-based approaches to preventing, as opposed to responding to, violence victimization or revictimization among justice-involved young women. This information is crucial for reducing the risk of violence before such victimization occurs. Previous reviews of interventions for reducing gender-based violence among young people in the general population have also found that interventions for those who are at an elevated risk of experiencing violence (such as justice-involved young women) have been largely overlooked (Crooks et al., 2019). Primary and secondary interventions that target justice-involved young women may be more difficult to design, implement, and evaluate than tertiary interventions. For example, rigorously evaluating primary or secondary interventions, such as through an RCT, may present feasibility and ethical challenges in terms of (a) randomizing participants to the intervention or control arm, (b) requiring large sample sizes to detect meaningful differences, and (c) accurately measuring participants’ experiences of violence (as opposed to measuring trauma symptoms) (Crooks et al., 2019). Multisectoral data linkage (i.e., linking administrative records from multiple sectors, such as criminal justice, health, housing, and welfare) (Harron et al., 2020) is a rigorous method for following large samples of people over time and can be used in conjunction with randomized and quasi-experimental studies (Kinner et al., 2013). Additionally, participatory methods (e.g., involving people with lived experience in the design and development of interventions or data linkage studies) may also be an appropriate avenue for developing interventions for groups of people who experience an increased risk of violence (Crooks et al., 2019).
Interventions that address one or more risk factors for violence victimization or revictimization among justice-involved young women may reduce violence exposure. An Australian study found that violent deaths among justice-involved young women most frequently occurred in the context of intimate partner violence (Willoughby et al., 2021b). However, risk factors for intimate partner violence among justice-involved young women are not well established. Historically, young women have been largely overlooked within family violence discourses (Johnston et al., 2022), with relatively little youth-specific inquiry into their experiences of intimate partner violence (Daff et al., 2021). Risk factors for intimate partner violence victimization among young women in the general population include mental health issues, substance use, social and relational pressures regarding perceived gender roles (Chung, 2007; Vezina & Hebert, 2007), and youth homelessness (Watson, 2017). The risk of young women experiencing intimate partner violence can also be influenced by the perceived seriousness and duration of the relationship (Giordano et al., 2010), the positioning of the relationship among peers, and the acceptance and endorsement of relational aggression, gender inequality, and violence in the young person’s social group (Foshee et al., 2013). Mental health and substance use issues have been found to increase the risk of injuries from violence among adult women and men released from prison (Willoughby et al., 2022). Future studies examining interventions that aim to improve health and reduce disadvantage among justice-involved young women should consider whether these interventions also impact the risk of violence victimization and revictimization in this group. Given that many of these factors are also associated with criminal justice contact (Kerig, 2018), addressing these risk factors may reduce both violence victimization and further criminal justice contact.
Our review focused on interventions that targeted justice-involved young women. It is possible that population-level approaches to prevent violence (i.e., universal interventions) that do not specifically focus on justice-involved young women may have some benefit in preventing violence against this group. However, to our knowledge, the impact of universal interventions on justice-involved young women has not been empirically assessed. Although effective at reducing overall rates of violence (Krug et al., 2002), universal strategies may not be sufficient to address inequities in violence victimization, meaning that certain groups may still experience an increased risk of violence (Cerdá et al., 2014; Frolich & Potvin, 2008). The stigma of criminalization experienced by justice-involved young people may hinder their engagement with or access to universal programs, for instance. Given the elevated rates of violence victimization among justice-involved young women, it is likely that universal interventions will need to be paired with interventions that have been specifically designed to meet the needs of justice-involved young women for violence victimization to be meaningfully reduced in this group (Frolich & Potvin, 2008). For interventions to be appropriate and acceptable by participants, they should also consider the unique needs of different groups of justice-involved young women, such as First Nations young women.
The methodological limitations of most included studies (e.g., the absence of control groups, small sample sizes, and short follow-up periods), along with few rigorous evaluations, and the diversity of the interventions themselves, meant that drawing definitive conclusions about the effectiveness of interventions was difficult. The dearth of evaluative studies clearly highlights a need for high-quality research examining all types of violence prevention (i.e., primary, secondary, and tertiary) across different settings (e.g., detention and community settings) to both prevent and respond to violence victimization, and revictimization, among justice-involved young women. We acknowledge that high-quality research needs to incorporate the views, experiences, and perspectives of justice-involved young women themselves to present a well-rounded picture of violence prevention initiatives and their effectiveness (Glasby & Beresford, 2006). Middleton et al.’s (2019) finding about approaches that have been designed to be trauma-informed potentially exacerbating trauma symptoms for some participants highlights the importance of ensuring that lived experience insights are embedded in research, and the importance of rigorously evaluating interventions, particularly those that have the potential to cause unintended harm.
All of the studies included in our review were conducted in the United States, which may limit the generalizability of our findings to other countries. The rate of violence, particularly firearm violence, in the United States is higher than in other high-income countries (Grinshteyn & Hemenway, 2016). Among young women and men released from youth detention in the United States, violence, predominantly firearm violence, is the most common cause of death (Teplin et al., 2014). However, in other countries, such as Australia (Coffey et al., 2004) and Finland (Sailas et al., 2006), the most common cause is often suicide or drug-related, with deaths from violence being considerably less prevalent.
Our review was limited to English-language studies, which may have introduced some bias. However, there is evidence that excluding studies in other languages may not meaningfully change the findings of reviews (Morrison et al., 2012; Nussbaumer-Streit et al., 2020). Despite the overrepresentation of ethnic and racial minorities in the criminal justice system, no studies considered the how the effectiveness of interventions differed by race and/or ethnicity. As additional searches for gray literature were only conducted in Google Scholar, some gray literature may have been missed. To our knowledge, this is the first review to examine violence prevention and response efforts targeted at young women who have had, or are at risk of having, contact with the criminal justice system. We specified our methods a priori (Willoughby et al., 2021a) and used a comprehensive search and broad inclusion criteria (including gray literature along with peer-reviewed literature), allowing us to search widely from the existing literature.
Conclusions
Effective interventions to keep young women safe from violence are contingent on the production and dissemination of high-quality evidence. Although we identified some tertiary interventions to address the impact of violence victimization, the paucity of effective and rigorously evaluated primary and secondary interventions to prevent violence (re)victimization against young women who have had, or are at risk of having, contact with the criminal justice system remains a critical gap in the literature. A comprehensive approach to reducing violence victimization requires intervention at all levels of violence prevention (i.e., primary, secondary, and tertiary) (Lee, 2017). In the absence of effective and evidence-based violence prevention initiatives that are specifically designed to meet the needs of justice-involved young women, the high rates of violence victimization among these young women will persist.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231171183 – Supplemental material for Interventions to Prevent and Respond to Violence Against Justice-Involved Young Women: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231171183 for Interventions to Prevent and Respond to Violence Against Justice-Involved Young Women: A Scoping Review by Melissa Willoughby, Emilia Janca, Sohee Kwon, Bianca Johnston, Tamlynn Collins, Stuart A. Kinner, Diana Johns, David Gallant, Clare Glover-Wright and Rohan Borschmann in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to thank Alex Andrawis for assisting with the gray literature searching. MW, RB, and SK are researchers in the NHMRC-funded Centre of Research Excellence in Driving Global Investment in Adolescent Health (GNT1171981). RB is funded by a National Health and Medical Research Council (NHMRC) Emerging Leadership-2 Investigator Grant (GNT2008073).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bianca Johnston and Tamlynn Collins are employed by the Youth Support and Advocacy Service (YSAS), who is also a funder.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the Melbourne Social Equity Institute at the University of Melbourne and received funding support from the Youth Support and Advocacy Service (YSAS) Industry Partnership Program.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.