
Abstract
Rates of intimate partner violence (IPV) against women in Sub-Saharan Africa are among the highest of any region in the world. Empirical studies on the effectiveness of IPV-prevention programs in Africa, though few, suggest that successful programs have emphasized community-level engagement and attitudinal change around gender roles. This study explored the relationship between adult women’s participation in an all-women’s soccer league and IPV in rural Kenya. Nikumbuke Project is a health- and literacy-based program for 702 women in Kwale County, Kenya, that also hosts a women’s soccer league. A total of 684 Nikumbuke members completed surveys for this study, 543 of whom identified as having had a partner in the preceding 12 months and were included in this analysis. Participants in the study were, on average, in their late 30s, married with 4–6 children, a primary education or less, and no source of formal employment. Logistic regression models examined the association between a woman’s participation in the soccer league and the odds that she would have experienced recent IPV, controlling for other covariates. Women who played on soccer teams had 59% lower odds of reporting physical IPV in the preceding 12 months and approximately 43% lower odds of reporting any form of IPV during the same period compared to women who did not play soccer. Support of more gender-equitable norms was associated with lower odds of all forms of recent violence. More research is needed to identify the underlying reasons for these observed effects and to determine the presence of a causal or temporal relationship between adult women’s sports and IPV-risk reduction. Nonetheless, findings from this study point to a novel IPV intervention in communities that might otherwise be resistant to more overt attempts to address gender-based violence (GBV) or where social service agencies with the capacity for IPV-prevention programming may be limited.
Intimate partner violence (IPV) against women is recognized by scholars and development professionals as a major public health and human rights concern that limits women’s role in society and is a widespread source of physical, sexual, and emotional harm (Watts & Zimmerman, 2002; Wolf et al., 2014). Data from 141 studies conducted in 81 countries revealed that in 2010, 30% of women aged 15 and over had experienced physical and/or sexual IPV in their lifetimes (DeVries et al., 2013). Rates of gender-based violence (GBV) against women in Sub-Saharan Africa are among the highest of the WHO regions, with IPV prevalence rates of 36.6% (WHO, 2013). A recently published systematic review and meta-analysis of cross-sectional studies conducted between 2008 and 2019 reported a pooled prevalence rate of GBV of 44% with rates of emotional IPV (29.4%), physical IPV (25.87%), and sexual IPV reported (18.75%; Muluneh et al., 2020).
Studies suggest GBV is a major problem in Kenya as well. Data from the most recent Kenya Demographic Health Survey report (2014) found that women experienced various forms of IPV at rates of 23.8% (emotional violence), 20% (physical violence), and 8% (sexual violence) within the 12 months preceding the survey (Kenya National Bureau of Statistics et al., 2015). A study in 2016 that examined the factors associated with sanitation use among women in Kenya reported similarly high rates of violence by an intimate partner—emotional IPV (22.2%), physical IPV (28.4%), and sexual IPV (10.3%) (Winter & Barchi, 2016).
At the heart of GBV rests attitudes about women, their place in the home and society, and their rights to self-determination, freedom from bodily, sexual, and emotional harm, and economic and political opportunity. GBV occurs all over the world but particularly thrives in households, communities, and societies in which women are accorded a lower status than men, and where women’s opportunities are constrained within gender-defined boundaries that limit women’s access to education, employment, resources, and decision-making. Accordingly, several studies, the majority of them in South Africa, have begun to explore the role that societal norms and attitudes regarding feminine and masculine roles may play in creating environments that increase, or even condone, violence against women (Dworkin et al., 2013; Jewkes et al., 2010; Jewkes et al., 2008).
In a separate domain of inquiry, a number of programs utilizing sports for adolescent girls and young women to promote health, self-confidence, greater peer-to-peer social interaction, and positive emotional development have recognized the transformative effects of sports on gendered norms about women’s roles and the social space they are expected to occupy (Brady, 2005; Brady & Khan, 2002; Chigudu, 2017; Hartmann & Kwauk, 2011; Huggins & Randell, 2007; Makau, n.d.; McGhee, 2012). Such literature reports positive effects that include increased freedom of movement and an expanded range of socially acceptable public spaces in which to socialize, greater self-efficacy, broader aspirations for future work and family, lower sexual risk behaviors, and improved health status (Huggins & Randell, 2007; Lyras & Peachey, 2011; Thompson, 1995).
Sports programs have emerged as an effective international development tool that can improve public health, enhance socialization at all ages, encourage the inclusion of those who are disadvantaged, and generally contribute to the economic development of communities (Human Development Report, 2003; Lyras & Peachey, 2011; UNFPA, 1994). Some scholars view it as a vehicle to promote social change, empowering otherwise marginalized and at-risk youth, and young people to create new economic, social, and political landscapes (Darnell, 2010; Hartmann, 2003). Sports has also come to be seen as a tool to promote gender equity, giving women voice and empowering them to assume a greater role in the social worlds of home, community, and the political economy (Hancock, Lyras & Ha, 2013; Lyras & Hums, 2009; Meir, 2005).
Although there has been a substantial increase in the availability and number of sports programs for girls and women in Sub-Saharan Africa, some sports, notably soccer, remain traditionally male, particularly among adults (Pelak, 2010). In poor rural areas in the region, social space rarely exists for organized women’s sports; the sphere of women’s activities revolves around largely domestic activities, and little time, resources, or community support is available to women to enter the social and physical domains of organized “play.”
Despite commonalities in the gender-transforming outcomes targeted by prevention interventions for GBV and those of sports-for-development programs to promote gender equality, limited scholarly research exists on the effects that women’s participation in a sport such as soccer may have on social norms regarding GBV at the level of women’s intimate relationships, their households, and their communities (Arango et al., 2014). What limited research does exist has been conducted in Western settings only.
The salutary effects of women’s participation in sports are well-documented in the scholarly literature and calls for equity in access to sports programs have been enshrined by several bodies within the United Nations (UNESCO, 1978; UNFPA, 1994). This study focuses on an intervention already shown in other settings to improve a number of health outcomes, both physical and mental, in girls and young women (Brady & Khan, 2002) but that is as yet untested in adult women. It was undertaken in 2018–2019 as part of a large, mixed-methods study examining how a small, but established, adult women’s soccer league is perceived and experienced by the men and women in the villages and communities in which the league teams are situated. The specific aims of this study were to: (1) explore whether women’s participation in an all-women’s soccer league is associated with a decrease in emotional, physical, and/or sexual IPV when controlling for other common risk factors for IPV and (2) to explore whether socioeconomic, demographic, violence-related, and gender-norm risk factors are associated with emotional, physical, and/or sexual IPV in a population of women in rural Kwale county in Kenya.
Methods
Setting
This study took place in Lunga Lunga constituency, a rural sub-county of Kwale County in the Coast Region of Kenya. Kwale County is characterized by high rates of food insecurity, poverty, and unemployment. Roughly 70% of the households are considered food poor and 14% report not having enough food to meet their needs, leading to a high incidence of childhood stunting, general undernourishment, and acute malnutrition (Republic of Kenya, Ministry of Agriculture, Livestock, and Fisheries, 2016). Kwale County is home to the Nikumbuke Project, the local collaborating non-governmental organization (NGO) for this study, and the in-country coordinators of the women’s soccer league. Since 2012, the Nikumbuke Project has supported women in Lunga Lunga constituency, a sub-county within Kwale County, through basic literacy and health information programs, subsidies for secondary school fees for girls, and a women’s vocational training program in tailoring. In 2014, a soccer league was established at the request of the women members of Nikumbuke. At the time of this study, there were teams representing a diversity of religions (Catholic, Muslim, traditional, and other) and distinct tribal groups in eight settled villages—Godo, Mgombezi, Lunga Lunga, Kidomaya, Juakali, Perani, Mpakani, and Jirani—and two nomadic “villages” that are home to Maasai and Umoja tribal communities. Teams practice by themselves once each week except during harvest time and the rainy season; village-versus-village games take place monthly. A tournament, in which all teams participate, is held each June. At the time of this study, the umbrella Nikumbuke Project had 702 members, 229 of whom were also members of the Nikumbuke Soccer League.
Sample and Recruitment
All members of the Nikumbuke Project who were over the age of 18 years at the time of the study and able to provide informed consent were eligible to participate. The study team was assisted in recruitment and data collection by a field staff of 19 local women who received training in research ethics, survey methods, and survey administration techniques. Trainees received a stipend for successfully completing the program and for each survey instrument they administered. Prior to the start of the study, the study team attended a regular monthly meeting of Nikumbuke in each of the 10 villages, accompanied by a trainee from that community, to introduce the study and answer questions about participation. Women were asked to provide their names and cell phone numbers if they were interested in participating. Follow-up was carried out by a member of the research team who visited women in their homes or at the project center, provided more detailed information about the study, and formally invited them to participate in the study. Consent was requested in oral form to reduce the likelihood that survey responses could be linked to any one individual. All women who participated in the study received an appreciation of 200 KES (approximately US $2). A total of 684 women participated in the surveys. Since the focus of this present analysis was on IPV, only those women who identified as having had a partner at any time in the previous 12 months were included in the analytic sample.
Ethical Considerations
This study received approval from the Institutional Review Board at Rutgers University and the National Commission for Science, Technology, and Innovation (NACOSTI) in Kenya.
Survey Instrument and Measures
The outcome variables of interest in this study are women’s experiences of physical, emotional, and sexual violence by an intimate partner within the past 12 months. IPV has been defined by Heise et al. as “any act of verbal or physical force, coercion, or life-threatening deprivation, directed at an individual woman or girl that causes physical or psychological harm, humiliation, or arbitrary deprivation of liberty and that perpetuates female subordination” (2002, p. 1165). The DHS domestic-violence module used in this study is a widely used instrument that examines three types of violence: emotional, sexual, and physical (Measure DHS/ICF International, 2014). IPV scores in this study were based on women’s reports of their partner’s behavior within the past 12 months. Internal consistency reliability for each of the three violence sub-scales was computed using the Kuder-Richardson Formula 20 (KR-20) (Kuder & Richardson, 1937). The emotional violence sub-scale (KR-20 = .79) consisted of 3 items focused on whether the respondent’s husband/partner had, in the past 12 months, (1) said or done something to humiliate her in front of others, (2) threatened to hurt or harm her or someone close to her; or (3) insulted her to make her feel bad about herself. The physical violence scale (KR-20 = .93) had 8 items that ranged from moderate violence (e.g., in the last 12 months did your husband/partner ever push you, shake you, or throw things at you) to severe violence (e.g., in the last 12 months did your husband/partner ever threaten or attack you with a knife, gun, or any other weapon). Finally, the sexual violence scale (KR-20 = .94) consisted of two questions about whether a respondent’s husband/partner had (1) physically forced her to have sexual intercourse with him even when she did not want to and/or (2) forced her to perform any sexual acts she did not want to in the past 12 months. Responses to each of the IPV items were dichotomized. A score of “1” on a sub-scale of violence reflected at least one affirmative response to questions within that sub-scale. A score of “0” reflected the absence of any affirmative response to questions within that sub-scale.
A dichotomous yes/no variable was included to reflect whether or not the Nikumbuke Project member was a participant in the Project’s soccer league. Each village team consists of 23 players—15 core players and 8 alternates. Substitutions when women were ill or injured and when women were pregnant were made within each team; women who were nursing small children continued to play. Team members, whether they were actively playing or not during a season, were coded as “1” if they had been a member of a team for at least one season. A total of 223 of the 229 women who were members of the soccer league agreed to participate in this study.
This study used a survey instrument containing a number of sociodemographic variables, for example, age, education, marital status, number of children, respondent and partner employment, and household income. Income was measured using a four-level categorical variable that indicated a respondent’s estimated monthly household income. Three monetary ranges were given as choices: less than 5,000 KES per month (approximately US $48), 5,000–10,000 KES per month, more than 10,000 KES, and a fourth category indicating that the respondent didn’t know. An additional binary control variable “aware of household finances” was created to account for women who did not know their household income. Only women who reported having an intimate partner at some time during the previous 12-month period leading up to the survey were included; women did not have to be married to be included. A binary “relationship status” variable was created to indicate whether the respondent was either: (1) married and living together with their partner or had a regular partner and were living together (common law marriage) or (2) had a regular partner or was married, but was not living with that individual. Very few women in the sample (8.8%) had any secondary or higher education; thus, responses to the level of education question on the survey were collapsed into a categorical variable with four levels: (1) no formal education; (2) some primary school education, but did not complete primary school; (3) completed primary school, but did not continue to secondary school; and (4) completed primary school and attended at least some secondary school or higher education.
The Gender-Equitable Men’s (GEM) Scale is a widely used instrument designed to measure attitudes and beliefs surrounding women’s roles relating to domestic and sexual life and intimate relations (Pulerwitz & Barker, 2008). A version of this scale (Cronbach’s α = .83) that had been previously modified and translated into Kiswahili by other investigators for use in Tanzania was used in this study (Kazaura et al., 2015). In addition, a question was included about whether the participant had ever witnessed her father beat her mother, as well as an “acceptability of wife-beating” scale used in the Demographic Health Surveys (Measure DHS/ICF International, 2014). Responses in this 6-item scale were converted to a dichotomous variable in which “1” indicated that a woman agreed that a man would be justified in beating his wife in at least one of the six instances described and “0” indicated that a woman did not feel that any of the six instances justified wife-beating (Cronbach’s α = .86).
Analysis Plan
For the purposes of this analysis, variables of interest included the IPV outcome measures, individual- and household-level demographic measures, violence-related and gender norm variables, and participation in soccer. Only women who reported having a male partner at some time during the previous 12-month period leading up to the survey were included in the analysis (n = 543). Frequencies were run for all variables and chi-square tests of independence were used to identify significant associations between various attributes of women in the sample and participation in the soccer league. An item non-response analysis of the survey responses indicated minimal missing data (less than or equal to 7%) on the independent and dependent variables of interest. Single imputation was used to approximate responses for missing data (Schonlau, 2012). In addition, approximately 10% of the women in the sample did not know their household income. Single imputation was used to estimate these values, and a binary variable (aware of household finances) was included in the model to account for the women who reported not knowing their household finances.
Four, separate, binary-logistic regressions were run to identify whether recent experiences of emotional, physical, or sexual IPV were significantly associated with participation in the soccer league, while controlling for demographic information and potential violence-related, and gender-norm confounders. Variables were tested for multicollinearity using variance inflation factors (VIFs); values were all less than or equal to 1.4 and tolerance was .7 for all variables in the model—well below the threshold indicating multicollinearity (Hair et al., 2009). Data analyses were conducted using Stata/MP v15 statistical software (StataCorp, 2017).
Results
Descriptive Statistics
Descriptive statistics for this analytic sample are summarized in Table 1. The percentage of women reporting experiences of IPV in the past 12 months was 17% (emotional violence), 10% (physical violence), 7% (sexual violence), and 22% (any form of violence). The majority of respondents were between the ages of 25 and 49 and married with 4 to 6 children. More than 70% of respondents had not completed primary school and only 24% of women had formal employment. Over one-half of respondents reported monthly household incomes less than 5,000 KES (approximately US $48). Attributes with significant association with playing league soccer in the bivariate analysis included past-year experience with physical or emotional IPV, age, education, and number of children.
Sample Characteristics and Bivariate Association with Participation in Nikumbuke Soccer League.
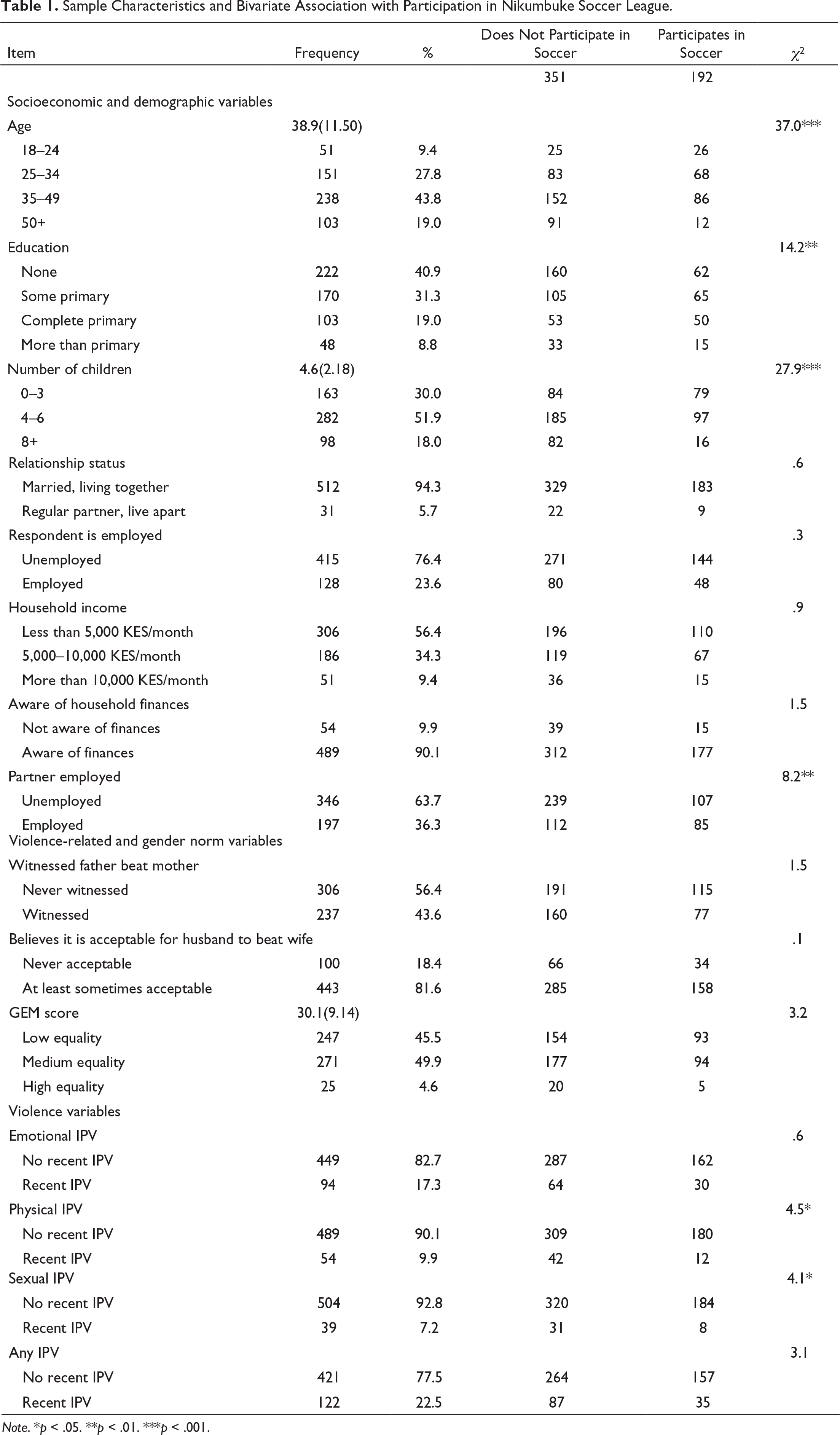
Note. *p < .05. **p < .01. ***p < .001.
Associations Between Women’s Participation in the Soccer League and IPV
Findings from the multivariate analyses are shown in Table 2. They suggest that women who participated in the soccer league had 59% lower odds of having experienced physical IPV in the past 12 months than women who did not (OR .41, CI 95% .199, .843, p = .015). In addition, women who play league soccer had approximately 43% lower odds of reporting any form of IPV (emotional, physical, and/or sexual) within the past 12 months than women who did not (OR .57, CI 95% .346, .990, p = .024). There was no significant association between soccer league participation and recent emotional or sexual IPV when controlling for other attributes.
Results from Multivariate Logistic Regressions.
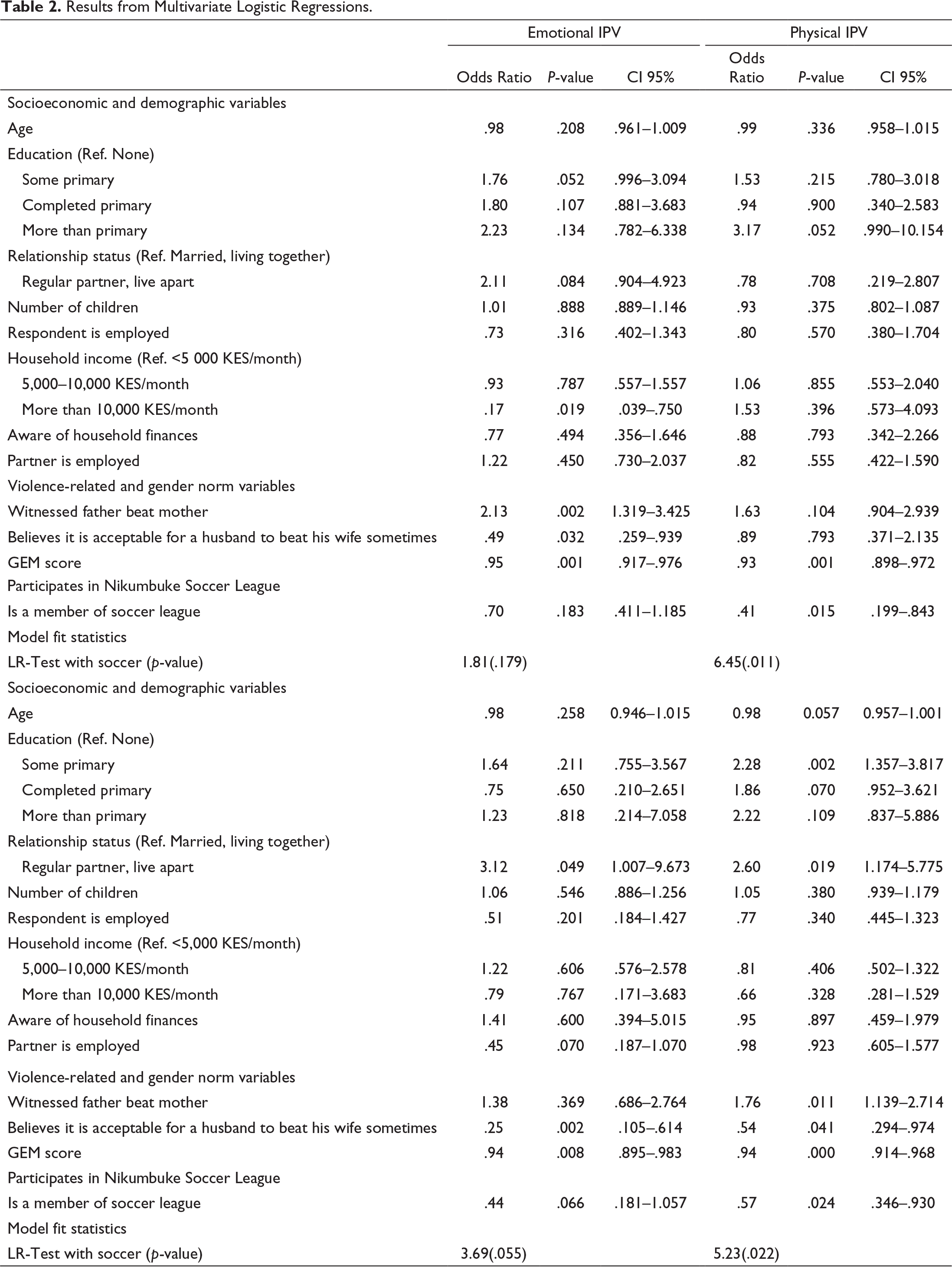
Monthly household income, having witnessed father beat mother, acceptance of wife-beating, and scores on the GEM scale were also significantly associated with emotional IPV. Women who reported monthly household incomes of 10,000 KES (approximately US $97) or more had lower odds (OR .17, CI95% .039, .750, p = .019) of experiencing recent emotional violence than women who reported incomes of under 5,000 KES (approximately $48 USD). Women who reported they witnessed their father beat their mother had over twice the odds of having experienced recent emotional IPV (OR 2.13, CI95% 1.319, 3.425, p = .002). Women who responded that wife-beating was justifiable in at least one instance had lower odds of reporting recent emotional IPV (OR .49, CI95% .259, .939, p = .032) and recent sexual IPV (OR .25, CI95% .105, .614, p = .002). Higher scores on the GEM scale (reflecting support for more equitable gender norms) were associated with lower odds of recent emotional (OR .95, CI95% .917, .976, p = .001), physical (OR .93, CI95% .898, .972, p = .001), and sexual (OR .94, CI95% .895, .983, p = .008) IPV.
Education and marital status were also significantly associated with women reporting experiences of any form of IPV in the preceding 12 months. Women with some primary education had 2.3 times the odds of having experienced some form of IPV (OR 2.38, CI 95% 1.357, 3.817, p = .002) than women with no education, and women who had a regular partner with whom they did not cohabitate had 2.6 times the odds of reporting some form of recent IPV (OR 2.60, CI 95% 1.174, 5.775, p = .019) than married women living with their husbands. Having witnessed one’s father beat one’s mother was associated with higher odds of a woman reporting any form of IPV in the preceding 12 months (OR 1.76, CI 95% 1.14, 2.71, p = .011). Acceptability of wife-beating was associated with lower odds of reporting any form of IPV in the past 12 months (OR .54, CI95% .294, .974, p = .041) as were higher scores on the GEM scale (OR .94, CI 95% .914, .968, p = .000).
Discussion
This study explores the association between adult women’s participation in sports and their experiences of IPV in rural communities in southeast Kenya. Findings from the study suggest that women in the Nikumbuke Project who participate in the soccer league have lower odds of reporting physical or any past-year experiences of IPV than those who do not, controlling for other attributes—suggesting that women’s participation in soccer could be a potential IPV-prevention strategy in this and similar settings in the Global South. While girls’ and women’s participation in sports has been shown in a variety of settings to improve health outcomes and transform certain social norms (Brady, 2005; Brady & Khan, 2002; Hartmann & Kwauk, 2011; Huggins & Randell, 2007), the empirical work on the link between GBV and women’s sports participation has focused to date on adolescents (Hershow et al., 2015; Sinclair et al., 2013) or women in U.S. populations (Milner & Baker, 2017). Research on a possible link between adult women’s participation in organized sports and IPV-risk reduction has been notably absent in Sub-Saharan Africa where opportunities at the community-level for adult women to play sports are limited. While soccer programs exist for adolescent girls as part of local education programs and sports-for-development initiatives led by NGOs, we know of no other soccer program for women in Kenya who are over the age of 18 or in which the vast majority of participants are married women with children.
Because the data used in this analysis were drawn from cross-sectional data, it is not possible to determine the causal or temporal relationships between IPV and any of the covariates included in this study. Data for this study were collected after the Nikumbuke soccer league was well established in 10 villages in Kwale county. Without baseline data from before the initiation of the soccer league, the data and results from this study cannot capture or account for changes in IPV since the start of the soccer league. While study findings suggest that women in the Nikumbuke Project who participate in the soccer league have lower odds of reporting physical or any past-year experiences of IPV than those who do not, controlling for other attributes, further research will be needed to determine whether women in Nikumbuke experience reductions in IPV as a direct result of their playing on a soccer team or if some other attribute not included in this analysis and unrelated to participation in organized sports accounts for these women experiencing less violence than their non-soccer peers.
Previous research has identified a number of risk factors for IPV that were included as covariates in this analysis. Numerous studies of women and IPV around the world have documented the protective effects of women’s education (Ackerson et al., 2008; García-Moreno et al., 2005). These and similar studies often compare 12 years women’s education to a reference category of “no education.” By contrast, a study of IPV in Kenya in 2003 that used “post-secondary education” as the reference category reported that women whose educational attainment fell into any of the other categories (no education, primary education, or secondary education) had increased odds of domestic violence (Lawoko et al., 2007). None of the women in this study had completed secondary education and only 9% had any education beyond primary school. Results from this study suggest that women who have completed only some years of primary school may be more susceptible to IPV than women with no education at all, but cannot support or refute previous findings about the protective effects of higher education on IPV risk. If, as some researchers have suggested, the expanded access to resources, delays in marriage, family formation, and anti-violence messaging that may come with more education are causal pathways between education and IPV (Weitzman, 2018), it may be that women in this setting, the majority of whom have 0–6 years of schooling only, have not had the opportunity for these causal mechanisms to take full effect.
In this study, unmarried women with a regular partner with whom they did not live had over 2 ½ times greater odds of experiencing any form of violence than women who were married and lived with their spouses. The 2014 Kenya DHS report distinguishes women’s relationships status as “never married,” “married or living together” or “divorced/separated/widowed” and therefore does not capture any attributes that may be particular to those unmarried women with regular partners with whom they do not cohabitate. Findings from this study suggest that it may be important to distinguish this sub-population of women from those who were never married, are divorced, or are widowed in order to have a more complete understanding of risk factors for IPV in this and similar populations.
Having witnessed one’s father beat one’s mother was associated with emotional violence in the past 12 months—a finding that is consistent with evidence from previous studies that suggest exposure to domestic violence as a child is associated with risk of experiencing and/or perpetration of violence in adulthood (Abramsky et al., 2011; Capaldi et al., 2012; Esquivel-Santoveña et al., 2013; Stöckl et al., 2014). Support of more equitable gender norms was associated with lower odds of reporting all forms of IPV in the past 12 months—a finding that is consistent with previous research (Ellsberg et al., 2015).
Findings from this study that suggest a negative correlation between acceptance of wife-beating and experiences of recent emotional and sexual IPV run counter to previous research in Kenya using DHS data (Memiah et al., 2018). This may simply be a reflection of the differences between the rural, largely agrarian population from which this study sample was drawn and the more diverse populations found in urban and other rural communities that comprise the DHS sample. Alternatively, findings from this study may suggest that women who accept wife-beating may adopt avoidance strategies to reduce IPV within their homes, that is, avoiding behaviors that they have learned are associated with being beaten. Data from the 2014 Kenya Demographic Health Survey also report higher national rates of past-year physical violence than those reported in this study as well as variability across regions of the country. Identifying the underlying reasons for the lower rates of physical violence observed in this study falls beyond its scope and would require access to more detailed data regarding structural, behavioral, and community-level factors in various other regions of Kenya that might have contributed to this finding.
More broadly, findings from this study may point to a limitation with the measurement of violence in some contexts. Most of the widely used, internationally recognized measures of violence were developed in Western nations with detailed definitions of violence that encompass a broad range of behaviors. Deeply engrained norms about the role of a woman in relationships—norms that may vary in different contexts—may make it difficult for women to recognize certain normalized behaviors as violent. This may be especially true in the case of measuring emotional and sexual violence. While concepts such as “humiliation,” “threats,” “insults,” and “force” may have clear meanings in some contexts, they may not be understood in the same way in others, particularly as criteria for recognizing whether or not an action constitutes “violence.” For example, if sexual intercourse is considered a duty or obligation in marriage, as it has traditionally been perceived in some Kenyan contexts (Spronk, 2005), the notion of “forcing” sexual intercourse or performance of other sexual acts may not be interpreted or responded to in the same way.
While further research is needed to understand the precise nature of the role that adult women’s participation in organized sports may play in shaping women’s experience of physical IPV, there are a number of potential pathways that, while beyond the scope of this present analysis, merit future exploration. Of particular interest may be the effects of sports on women’s self-esteem and social support, associations that are well documented in adolescent populations (Ekeland et al., 2005; Liu et al., 2015), and which have also been shown to have protective effects against victimization (Milner & Baker, 2017; Taylor et al., 2012). Another area for further inquiry lies in exploring the impact of women’s participation in community-level team sports and relationship quality at home, a factor that has also been shown to be associated with reduced risk of IPV (Bourey et al., 2015). Although adult-women’s entrance into what is regarded in most African settings as an exclusively adult-male domain could be a potential source of conflict, it may also introduce opportunities for shared experiences that minimize conflict and improve relationship dynamics.
Conclusion
Despite extensive literature supporting the beneficial effects of sports and physical activity on women’s physical and emotional health, few studies to date, and none that we are aware of in the Global South, have argued that the participation of adult women in organized sports may be an effective intervention to reduce their vulnerability to IPV. Findings from this study suggest that women’s participation in the Nikumbuke Soccer League program was significantly associated with lower rates of physical IPV. Considerably more research is needed to understand whether these findings are merely a reflection of some unique combination of contextual factors in this small sub-county in rural Kenya or whether, instead, adult women’s participation in organized team sports actually alters the dynamics of intimate relationships and reduces the occurrence of violence. Programs that change norms about adult women’s participation in organized sports may have a “spillover” effect on other more intractable norms about women’s role in society and the acceptability of the use of violence towards them. Given that sports are already part of the social fabric of communities around the world, such programs might prove particularly effective at reducing GBV in communities that might otherwise be resistant to more overt attempts to address GBV or where social service agencies with the capacity for IPV-prevention programming may be limited.
Footnotes
Acknowledgments
Special thanks are due to the Nikumbuke Soccer League-US, for its unstinting support of this study, Ken Wakia for seeing the potential of women’s sports to contribute to community well-being, and the many individuals at Rutgers University who contributed in various ways to making this research possible. Of particular note are Frances Loeser, Keri Ferreira, Patrick Hobbs, Dennis DeMarino, Asenath Dande, and the staff of Rutgers Global. Importantly, this study would not have been possible without the enthusiastic participation of the staff of the Nikumbuke Project in Lunga Lunga and the remarkable women of Nikumbuke.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of a large mixed-methods study supported by grants from Patrick Byrne, Adidas North America, and the United States Department of State, Kenya. In-kind support was received from Rutgers University-Division of Intercollegiate Athletics, the Nikumbuke Soccer League-US, the Sports Bra Project, and the Nikumbuke Project-Kenya.