
Abstract
This study aimed to develop a scale assessing the early signs of infant neglect and to test its reliability and validity. Neglect is a frequent type of child maltreatment and a serious problem worldwide, but it has received limited research attention. Previous studies of neglect assessment have mainly been targeted toward assessing the risk of apparent neglectful caregivers and neglected children. Early needs assessment scale focused on neglect evaluated by public health professionals in infants is necessary for the urgency of preventing neglect from infancy. Participants were community/public health nurses across Japan with experience working with neglectful caregivers of infants. The initial Signs of Neglect in Infants Assessment Scale (SIGN) was developed and refined based on previous studies, community/public health nurse consultation, and expert review. In 2017, 474 community/public health nurses completed a questionnaire regarding one infant neglect case. Item analysis, exploratory factor analysis, confirmatory factor analysis, and comparisons with a preexisting scale and case reporting status were used to narrow the scale and assess its psychometric properties. Item and exploratory factor analyses reduced the scale to 14 items on three factors: lack of basic supervisory care, child underdevelopment, and lack of emotional behavior. A confirmatory factor analysis indicated a good model fit (adjusted goodness-of-fit index = 0.921). Cronbach’s alpha was >.80 for total SIGN and all three factors. SIGN score was positively correlated with the preexisting scale (r = .335, p < .001) and with child protection services reporting status (M = 12.8 for reported cases vs. 9.2 for unreported cases, p < .001). The SIGN is an innovative scale with good psychometric properties for assessing signs of infant neglect. It has the potential to contribute to preventing infant neglect by providing early support to infants and their caregivers.
Introduction
Neglect is the most frequent category of child maltreatment and is a serious problem worldwide, as has been reported by child protection agencies in several developed countries (Gilbert et al., 2009; International Society for Prevention of Child Abuse and Neglect, 2018; World Health Organization, 2016), although prevalence estimates vary (Clement, Berube, & Chamberland, 2016; Stoltenborgh, Bakermans-Kranenburg, & van IJzendoorn, 2013). In the United States, an estimated 676,000 victims of child abuse and neglect were reported to Child Protective Services in 2016, and the majority of these children suffered from neglect (79.5%; Centers for Disease Control and Prevention, 2016). In Japan, 122,575 victims of child abuse and neglect were reported in 2016—a substantial increase from 56,384 in 2010, and 25,842 of these children suffered from neglect (Statistics Bureau, Ministry of Internal Affairs and Communications, 2018).
The World Health Organization separates the definition of neglect into specific incidents and a repeated pattern of failure by a parent/caregiver or other family member to ensure the development and well-being of a child (World Health Organization & International Society for Prevention of Child Abuse and Neglect, 2006). The basic concept of neglect in eastern Asia is consistent with the World Health Organization definition, and this consistency is seen in the definition put forward in the Child Abuse Prevention Law in Japan. Previous studies have suggested that the definition varies across different cultures (Stewart, Kirisci, Long, & Giancola, 2015; Stowman & Donohue, 2005). However, few studies have established clear cultural differences in the definition of neglect. Straus and Kantor (2005) included cultural aspects in defining neglect as neglectful behavior by a caregiver that constitutes a failure to act in ways that are presumed by the culture of a society to be necessary to meet the developmental needs of a child and which are the responsibility of a caregiver to provide (p. 20).
Coope and Theobald (2006) did not define neglect but identified societal and cultural norms—especially gender roles and relations—and poverty as major factors predicting neglect in developing countries. A cross-cultural study on the reliability and validity of a neglectful behavior scale (Straus, 2006) suggested that cultural differences caused by the prevalence of neglect exist even within a single country and that the internal consistency of the scale items varied across cultures, with the lowest alpha coefficients seen in non-Anglo, non-European countries in Asia, the Middle East, and Latin America. Considering cultural context is clearly important in assessing child neglect.
Preventing child neglect is a high priority for public health policy because neglect seriously affects not only the victims’ physical and mental health, well-being, and development throughout their lives but also has negative consequences for society in general (World Health Organization & International Society for Prevention of Child Abuse and Neglect, 2006). Systematic reviews suggest causal relationships between neglect and negative long-term health consequences, including depressive disorders, drug use, suicide attempts, sexually transmitted infections, and risky sexual behavior (Norman et al., 2012; Yıldız & Tanrıverdi, 2018). For infants, neglect represents severe adversity because the first year of a child’s life forms the foundation for a lifelong developmental trajectory (Rayce, Rasmussen, Klest, Patras, & Pontoppidan, 2017). To eliminate negative health consequences for children, public health interventions beginning in infancy that are aimed at early prevention of neglect are necessary. Neglect could be prevented through community engagement in identification and in early support. Effective prevention requires two vital processes: (a) defining the problem conceptually for empirical study, and (b) identifying the causes and risk factors that appear to affect susceptibility to maltreatment (World Health Organization & International Society for Prevention of Child Abuse and Neglect, 2006). To reduce the prevalence of child neglect, both of these processes are essential and professionals in public health fields must identify potential neglect through assessments of early signs of neglect among infants.
However, to date, no scale has been developed to measure the early signs of neglect, establishing a clear conceptual definition of neglect for empirical study and allowing professionals to identify potential neglect among infants. A few studies have developed scales to identify risks of both physical abuse and neglect among parents with infants. One self-report scale used in the Netherlands focuses on identifying parenting stress (Horrevorts et al., 2017; van der Put, Bouwmeester-Landweer et al., 2017). Another scale, the Scale for Home-Visiting Nurses to Identify Risks of Physical Abuse and Neglect Among Mothers With Newborn Infants (SIRPAN), is based on home-visiting nurse reports. This scale has targeted newborn infants and their mothers in Belgium who are at risk of physical abuse and neglect (Grietens, Geeraert, & Hellinckx, 2004), evaluating early risk of physical abuse and neglect among mothers with infants aged up to 3 months, and measures maternal isolation, psychological issues, and problems communicating with professionals. The SIRPAN can be used to prepare preventive supports provided by home-visiting nurses (Grietens et al., 2004). These previous scales are limited because they focus on “risk” rather than “signs” or “needs,” and they do not include items on the environment or the development and well-being of infants—factors that are indispensable for dealing with neglect—but only assess parenting behaviors.
Previous studies of neglect assessment have mainly been targeted toward tools used to assess the level of risk or the seriousness of cases of apparently neglectful caregivers and neglected children by child welfare protection professionals in the United Kingdom or the United States (Iwaniec, 1995; Minty & Pattinson, 1994; Slack, Holl, Altenbernd, McDaniel, & Stevens, 2003; Straus, 2006; Straus & Kantor, 2005; Trocmé, 1996), rather than toward the early assessment of levels of need and support for infants and caregivers. Additional actuarial and statistical instruments for assessing child maltreatment should be developed and strengthened by discriminating between risk assessment and needs assessment and by integrating risk assessment with case management (van der Put, Assink, & Boekhout van Solinge, 2017).
Risk assessment instruments for both neglect and multiple types of child abuse for use by child welfare protective services workers are particularly appropriate to predict future child maltreatment and to ascertain intervention urgency and intensity; however, these methods are not appropriate for needs assessment to determine targets for case planning (van der Put, Assink, & Boekhout van Solinge, 2017). Given the increasing prevalence of child neglect, it is important that neglect assessment measures continue to address limitations in an effort to obtain more accurate predictions of the problem (Stowman & Donohue, 2005). Neglect is often viewed as a category of abuse similar to emotional (Glaser, 2011), physical, and sexual abuse, and abuse and neglect are frequently evaluated comprehensively. Nevertheless, neglect is quite different from abuse; neglect has its own antecedents, characteristics, effects, and management (Golden, Samuels, & Southall, 2003).
The development of a new early needs assessment scale focused on neglect in infants and evaluated by health professionals is necessary to help infants and caregivers by providing them with a timely connection to the appropriate support. Such a scale also has the potential to contribute to the reduction of the prevalence of infant neglect and to the prevention of current and future related health consequences for children. Recent studies in the United States have evaluated child-reported parental neglectful behavior (Dubowitz, Villodas, et al., 2011; Kantor et al., 2004; Stewart et al., 2015). Self-report scales completed by caregivers of children aged 3 to 11 years have also been developed in the United States (Harrington, Zuravin, DePanfilis, Ting, & Dubowitz, 2002; Lounds, Borkowski, Whitman, & Centers for the Prevention of Child Neglect, 2004). However, empirical studies of neglectful parents using implicit measures are scarce, although implicit measures are important for assessing parental cognitions and behaviors (Camilo, Garrido, & Calheiros, 2016; Compier-de Block et al., 2015; Friedrich, Tyler, & Clark, 1985; Hildyard & Wolfe, 2007). Especially in Japan, mothers are traditionally expected to take responsibility for parenting and maintaining the home, and people conceal their family problems from others (Kayama, Sagami, Watanabe, Senoo, & Ohara, 2004). Therefore, in Japan, infant neglect is mainly affected by mothers’ parenting behavior, and it is difficult for caregivers who show signs of neglectful behavior to build trusting relationships with professionals or to seek support by themselves. Infants lack a voice to ask for help outside the home, but infants suffering from neglect are sometimes noticed and identified by professionals, relatives, or community members. Therefore, a public health professional–reported scale will be effective as a new early assessment of neglect in infants.
Worldwide, community/public health nurses (C/PHNs), as frontline workers and coordinators, have identified and supported caregivers and children in cases of child abuse (Schols, de Ruiter, & Öry, 2013) and dental neglect (Bradbury-Jones, Innes, Evans, Ballantyne, & Taylor, 2013). Similarly, in Japan, based on the Maternal and Child Health Law, C/PHNs employed in the maternal and child health section of local governments have the responsibility to prevent child abuse and neglect because they can assess almost all mothers with infants in the course of providing services, such as handing out maternity health record books, performing home visits, or conducting health checkups. C/PHNs continuously support the needs of infants and caregivers who are potentially at risk of being neglectful and those with other problems through case management, collaborating with other professionals as required (Ueno, Kayama, & Murashima, 2004). However, there are few standardized, evidence-based child neglect needs assessment tools available for use in public health services, especially by C/PHNs. Early needs assessment by C/PHNs has the potential to support caregivers, promote collaboration with other professionals, and contribute to the prevention of infant neglect.
The objective of the present study was to develop a new scale to assess the signs of neglect in infants to allow C/PHNs to begin providing effective, continuous support to caregivers and to test the validity and the reliability of this newly developed scale.
Method
Phase 1: Developing the Instrument
In Phase 1, the instrument development and refinement for initial testing were conducted. First, we developed a pool of items. The literature review focused on integrating different etiological models into a comprehensive theoretical framework and on identifying the signs that showed strong relationships with future neglect in previous studies (Barron & Jenny, 2011; Bartlett, Raskin, Kotake, Nearing, & Easterbrooks, 2014; Connell-Carrick & Scannapieco, 2006; De Paul, & Guibert, 2008; Dubowitz, 1999, 2007; Dubowitz, Black, Starr, & Zuravin, 1993; Dubowitz, Kim, et al., 2011; Dubowitz, Newton, et al., 2005; Dubowitz, Papas, Black, & Starr, 2002; Dubowitz, Pitts, & Black, 2004; Dubowitz, Pitts, et al., 2005; Dubowitz, Villodas, et al., 2011; Glaser, 2011; Golden et al., 2003; Harrington, Black, Starr, & Dubowitz, 1998; Harrington et al., 2002; Iwaniec, 1995; Kantor et al., 2004; Li, Zhong, Chen, Zhong, & Pan, 2015; Lounds et al., 2004; Minty & Pattinson, 1994; Polansly, Gaudin, Ammons, & Davis, 1985; Runyan et al., 2005; Slack et al., 2003; Stevenson, 2007; Stewart et al., 2015; Stoltenborgh et al., 2013; Straus, 2006; Straus & Kantor, 2005; Trocmé, 1996; World Health Organization & International Society for Prevention of Child Abuse and Neglect, 2006).
We defined neglect as caregivers’ behavioral patterns or the care environment failing to sufficiently meet the basic needs for the child’s developmental age, resulting in unsafe living conditions and possibly the loss of the child’s life. The reasons for selecting the original items for this scale (the item inclusion criteria) were based on three factors: the degree to which the item reflected the definition of the neglect of infants, the logical clarity and understandability of the item for C/PHNs, and the practical usefulness of the item. More specifically, each item had to reflect (a) the observation of aspects of the caregiver’s behavioral patterns or of the care environment that are relevant to the definition of neglect, or (b) relevant characteristics of infants and infancy. We selected each initial item from studies conducted in Western contexts, considering the item’s applicability and appropriateness in the cultural context in Japan. We thought all the items from previous studies would be acceptable also in Japan. We expressed each item in a way that would be culturally acceptable both in Japan and in many other cultures.
Signs of neglect were defined as latent signs that cannot confirm but may predict neglect when directly observed in conversations with the caregiver(s) by a C/PHN or conveyed by professionals or neighbors who know the caregivers and the children. We decided to include indirect information about infants and caregivers heard from professionals, relatives, or neighbors to identify/assess the potential needs of infants and caregivers because a previous study has demonstrated that neglect can be prevented by the networked engagement of community members in identification and early support (World Health Organization & International Society for Prevention of Child Abuse and Neglect, 2006). At this stage, information from 28 C/PHNs was gathered through a focus group discussion and 23 face-to-face interviews focused on the C/PHNs’ perceptions of signs of neglect observed in the course of their professional experience. The narratives provided concrete information about the signs of neglect in the daily work of C/PHNs and added to the pool of items.
Next, the pool of items was reviewed by eight experts, including C/PHNs, social workers, and community/public health nursing researchers, to assess the items’ validity, readability, comprehensibility, relevance, and practical usefulness for C/PHNs.
The initial Signs of Neglect in Infants Assessment Scale (SIGN) was refined to include 50 items, consisting of four preliminary dimensions focusing on lack of emotional interaction by the caregiver (nine items), lack of parenting behavior to save the child’s life and ensure safety (17 items), lack of behavior to provide an appropriate environment (15 items), and infant physical conditions threatening life and safety (nine items). This structure was based on a neglect model that was developed through the integration of previous studies. The initial SIGN included more than one item for each of six types of neglect (Stewart et al., 2015): physical (17 items), nutritional (four items), medical (three items), supervisory (13 items), emotional (13 items), and educational (two items).
All the items were negatively formulated and scored on a 3-point rating scale, ranging from 0 (never observed or reported) to 2 (twice or more; at least two instances during daily work), either directly observed by the C/PHNs or heard from other professionals or neighbors. High scores indicated the presence of more signs of neglect. We translated the SIGN from Japanese to English, with back translation by a bilingual researcher specializing in health sciences, so that the SIGN could also be published in English. The face validity of the English version of the SIGN was reviewed by a native English speaker and public health researcher.
Phase 2: Validating the Instrument
Design
This cross-sectional study was conducted in Japan from February to April 2017.
Participants and setting
Based on data from the Ministry of Internal Affairs and Communications of Japan, we identified 1,734 municipalities across Japan. Inclusion criteria were C/PHNs who (a) were working in municipality maternal and child health departments, and (b) had experience with case management for caregivers of infants below 1 year of age with signs of neglect. Informed consent letters and the initial SIGN questionnaire were sent by postal mail to the manager of the maternal and child health department in each municipality, and eligible participants were invited to participate voluntarily. A total of 1,734 eligible C/PHNs—one from each municipality—were asked to complete the self-administered, anonymous questionnaires regarding signs of neglect and other information about one eligible case, defined as a caregiver of an infant aged below 1 year who was supported by the C/PHN’s case management where there were signs of neglect.
Measures
We collected demographic data on the participating C/PHNs, including age, gender, and duration of work experience as a C/PHN.
The C/PHNs rated the importance of each scale item on a 4-point Likert-type scale as follows: 0 = unimportant, 1 = somewhat unimportant, 2 = somewhat important, and 3 = important; there was also an I don’t know option to identify items that many professionals felt did not make sense.
To allow for the analysis of the relevance of each initial SIGN item for identifying potential characteristics of neglect of infants, participants were asked to recall one eligible case and to assess the frequency of each item appearing as an early sign of infant neglect in that specific case. Each item was assessed on a 3-point Likert-type scale (0 = not at all, 1 = once, 2 = twice or more), with higher scores indicating more signs of infant neglect.
We also asked participants to report the demographic characteristics of the specific case, including infant age in months, infant gender, family members living with the infant, timing of the start of support, and referral situation. The participants were also asked to report which of a list of demographic factors might be associated with a high risk of neglect. These factors were selected based on a literature review and on qualitative data from our abovementioned surveys of public health experts.
Measures to assess the validity of the SIGN
We used two measures to assess the validity of the SIGN. One measure was the SIRPAN (Grietens et al., 2004). We consider this scale to be reliable and valid for use in this study because (a) it contains measures reported by professionals (C/PHNs), (b) it can identify physical abuse and neglect in infancy, and (c) it includes items to assess infants’ and caregivers’ interaction during home visits. To our knowledge, the SIRPAN is the only scale with these features that is similar to the SIGN, both in Japan and worldwide. The SIRPAN includes 20 items scored on a 4-point rating scale ranging from 0 (never observed or reported) to 3 (very often observed or reported: at least once during each home visit), yielding a total range of 0 to 60. High scores point to the presence of risk factors. This scale has previously shown high internal consistency (Cronbach’s α = .92) and interrater reliability (r = .97; Grietens et al., 2004). Because the SIRPAN had not previously been used in Japan, a trained bilingual translator translated the scale for this study. The Cronbach’s alpha of this scale was .90 in the present study. The other measure used to assess the SIGN’s validity was whether the C/PHN reported the case to the Child Guidance Center (Horikawa et al., 2016). In reports to the Child Guidance Center, C/PHNs must select the main type of child abuse or neglect from four types (physical abuse, emotional abuse, neglect, or sexual abuse), as regulated by the Child Abuse Prevention Law in Japan. The C/PHNs are also asked whether both child abuse and neglect are present. We hypothesized that the SIGN scores of cases reported to the Child Guidance Center would be higher than those of unreported cases.
Data Analysis
IBM SPSS Amos 22 and SPSS, Version 22 statistical software (SPSS, Inc., Chicago, IL, USA), were used to perform all of the statistical analyses.
Item and exploratory factor analyses were performed to investigate the internal consistency and convergent validity of the SIGN. The exclusion criteria for the item analysis were pass efficiency (average score ≤2.0 points), rate of response difficulty (don’t know and nonresponse ≥5%), distribution (somewhat important and important together accounting for < 95% of the sample), good–poor analysis (no significant difference between the highest and lowest scoring groups), item–total analysis (correlation coefficient <.30), and correlations between the items (correlation coefficient >.70).
The items remaining from Phase 1 after the item analysis were examined using exploratory factor analysis with promax rotation. We determined the optimal number of factors by sequentially using latent root criteria (eigenvalues >1.0) and a scree plot. Item loadings needed to exceed 0.40. The internal consistency of each factor was determined using Cronbach’s α ≥ .70.
Confirmatory factor analysis was performed on the remaining items from Phase 2 to verify the SIGN’s construct validity. The goodness-of-fit index (GFI), adjusted GFI, comparative fit index, and root mean square error of approximation were used to evaluate the data–model fit. The model was accepted if the GFI, adjusted GFI, and comparative fit index were ≥0.90 and the root mean square error of approximation was ≤0.06 (Hooper, Coughlan, & Mullen, 2008; MacCallum, Browne, & Sugawara, 1996). Furthermore, a correlational analysis was conducted to evaluate the criterion-related validity of the confirmed version of the SIGN on the level of risk as measured by the SIRPAN and Child Guidance Center reporting status. A correlation of ≥.30 was evaluated as adequate. The internal consistency of the confirmed version of the SIGN was evaluated using Cronbach’s alpha, with a value of ≥.70 considered adequate.
Results
Respondents’ Characteristics
Table 1 shows the participants’ characteristics. A total of 507 (29.2%) responses were received, and 474 (93.5%) questionnaires with valid responses were included in the analysis. The mean age of the C/PHNs was 40.2 ± 9.0 years, and 98.0% were women.
Characteristics of the Study Participants and Caregivers and an Infant Aged Below 1 Year With Signs of Neglect.
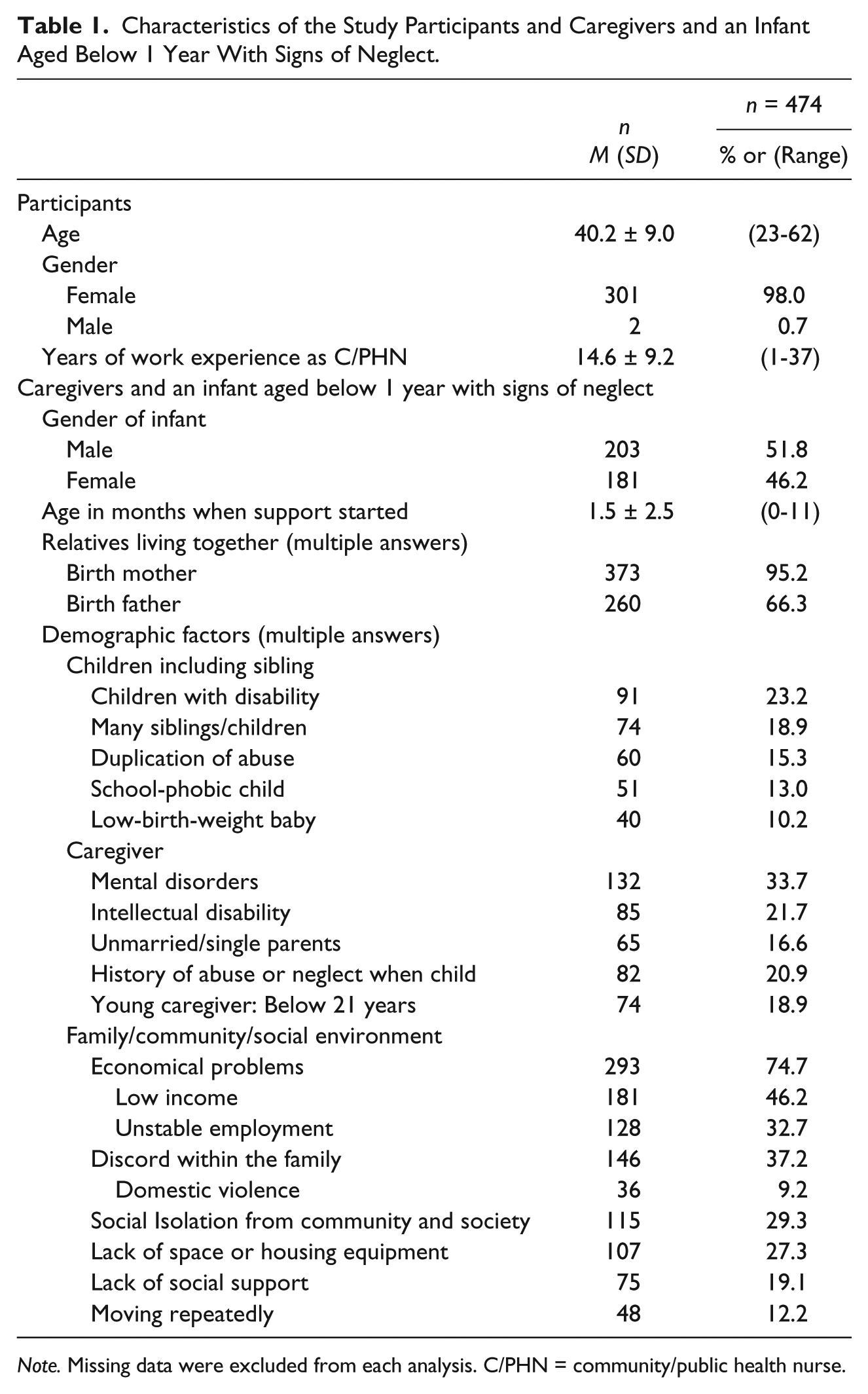
Note. Missing data were excluded from each analysis. C/PHN = community/public health nurse.
Demographic Data of Caregivers and Infants Aged Below 1 Year With Signs of Neglect
Of the cases reported by the participants, 51.8% concerned male infants, with a mean age of 1.5 ± 2.5 (range = 0-11) months when support started. The family members who most commonly lived with the infants were the mother (95.2%) and father (66.3%). The demographic factors that the C/PHNs most often considered to be associated with risk of neglect were economic problems, such as having a low income or receiving public assistance (74.7%), discord within the family (37.2%), mental health conditions of the caregiver (33.7%), and social isolation (29.3%).
Item Analysis
Table 2 presents the results of the item analysis. First, three items (Items 32, 34, and 35) were excluded by the criteria of pass efficiency and item difficulty. Second, the assessment of the importance of the items resulted in 23 items (Items 6, 7, 9, 10, 12-15, 17, 19-21, 31, 33, 36-38, 40, 41, 45, 47, 48, and 50) being excluded. Third, the assessment of item–total correlations resulted in two items (Items 2 and 8) being excluded. Finally, the assessment of the correlations between the items (correlation coefficient >.70) resulted in one item (Item 44) being excluded, leaving 21 items for the factor analysis.
Item Analysis of the Initial Signs of Neglect in Infants Assessment Scale.
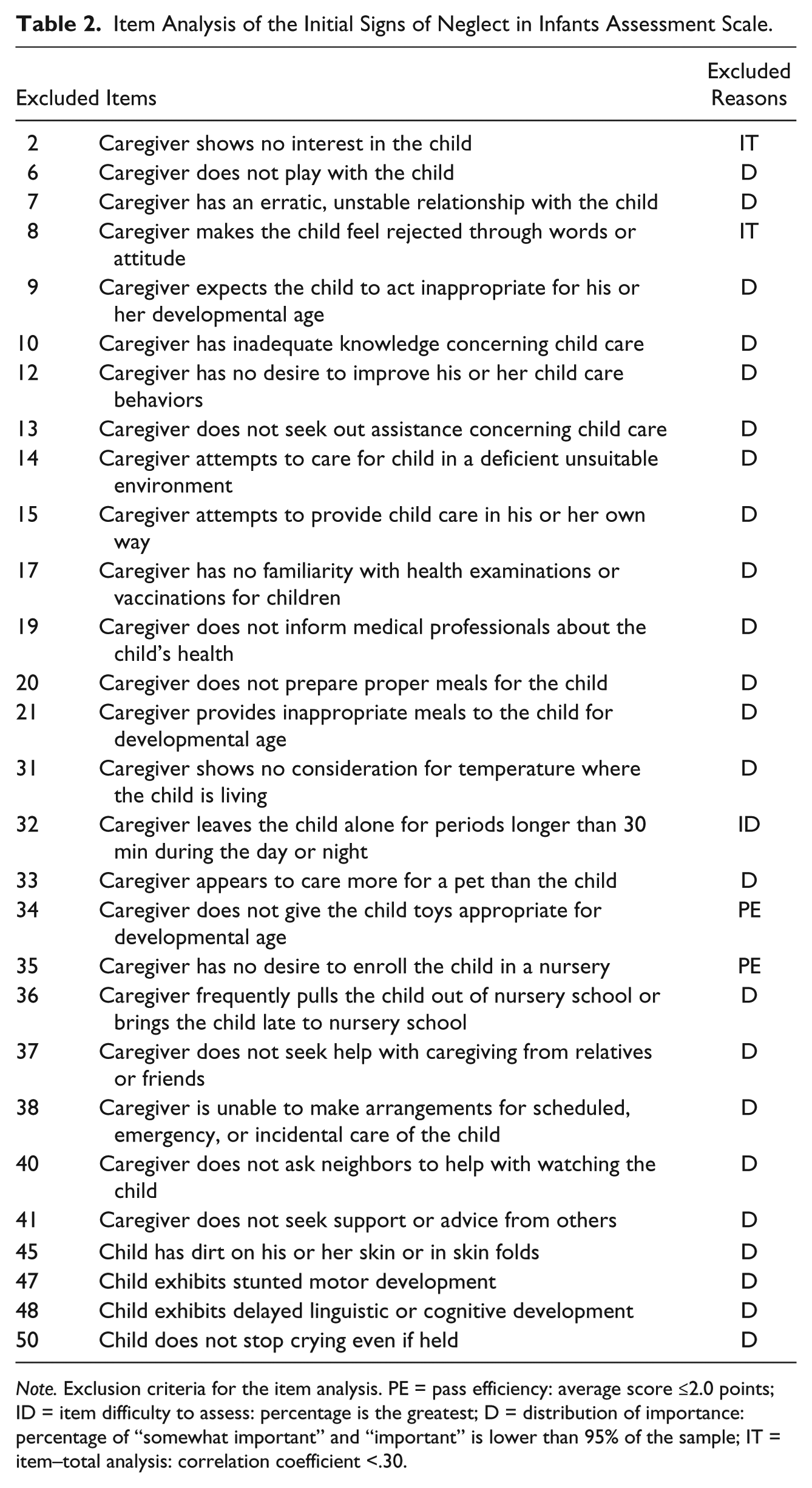
Note. Exclusion criteria for the item analysis. PE = pass efficiency: average score ≤2.0 points; ID = item difficulty to assess: percentage is the greatest; D = distribution of importance: percentage of “somewhat important” and “important” is lower than 95% of the sample; IT = item–total analysis: correlation coefficient <.30.
Factor Structure
Exploratory factor analysis with promax rotation was performed on the 21 items. This resulted in seven further items (Items 11, 16, 18, 30, 39, 46, and 49) being excluded, leaving 14 items from the initial version of the SIGN (Items 1, 3-5, 22-29, 42, and 43; Table 3). The latent root criterion suggested a three-factor model because the scree plot showed a detectable difference in slope after the first three eigenvalues. Factor I included six items (Q1-Q6; Items 24-29) interpretable as lack of basic supervisory care—that is, lack of caregiver behaviors that met the infant’s basic needs, in our interpretation. Factor II included four items (Q7-Q10; Items 22, 23, 42, and 43) interpretable as child underdevelopment—that is, the infant’s poor physical development and unhealthy conditions because of nutritional requirements not being met by any caregiver. Factor III included four items (Q11-Q14; Items 1, 3-5) interpretable as lack of emotional behavior—that is, a lack of emotional behaviors and emotional attentiveness to promote infant development (Table 3). These three factors were entered as three latent factors in a confirmatory factor analysis model. All the fit indices indicated a good data–model fit (GFI = 0.947, adjusted GFI = 0.921, comparative fit index = 0.959, root mean square error of approximation = 0.057; Figure 1) (Supplemental material: English version and Japanese version of the SIGN).
Exploratory Factor Analysis for the SIGN.
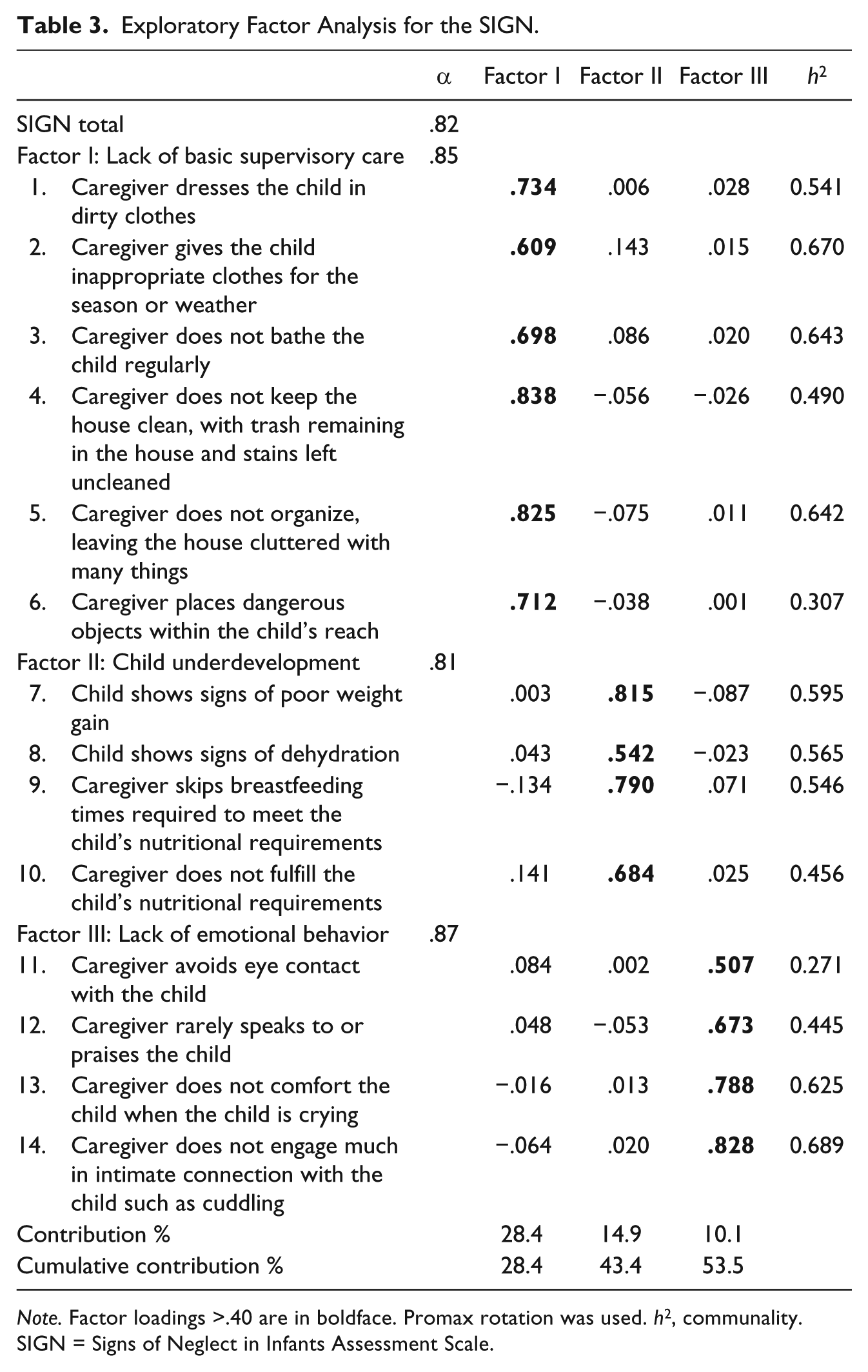
Note. Factor loadings >.40 are in boldface. Promax rotation was used. h2, communality. SIGN = Signs of Neglect in Infants Assessment Scale.
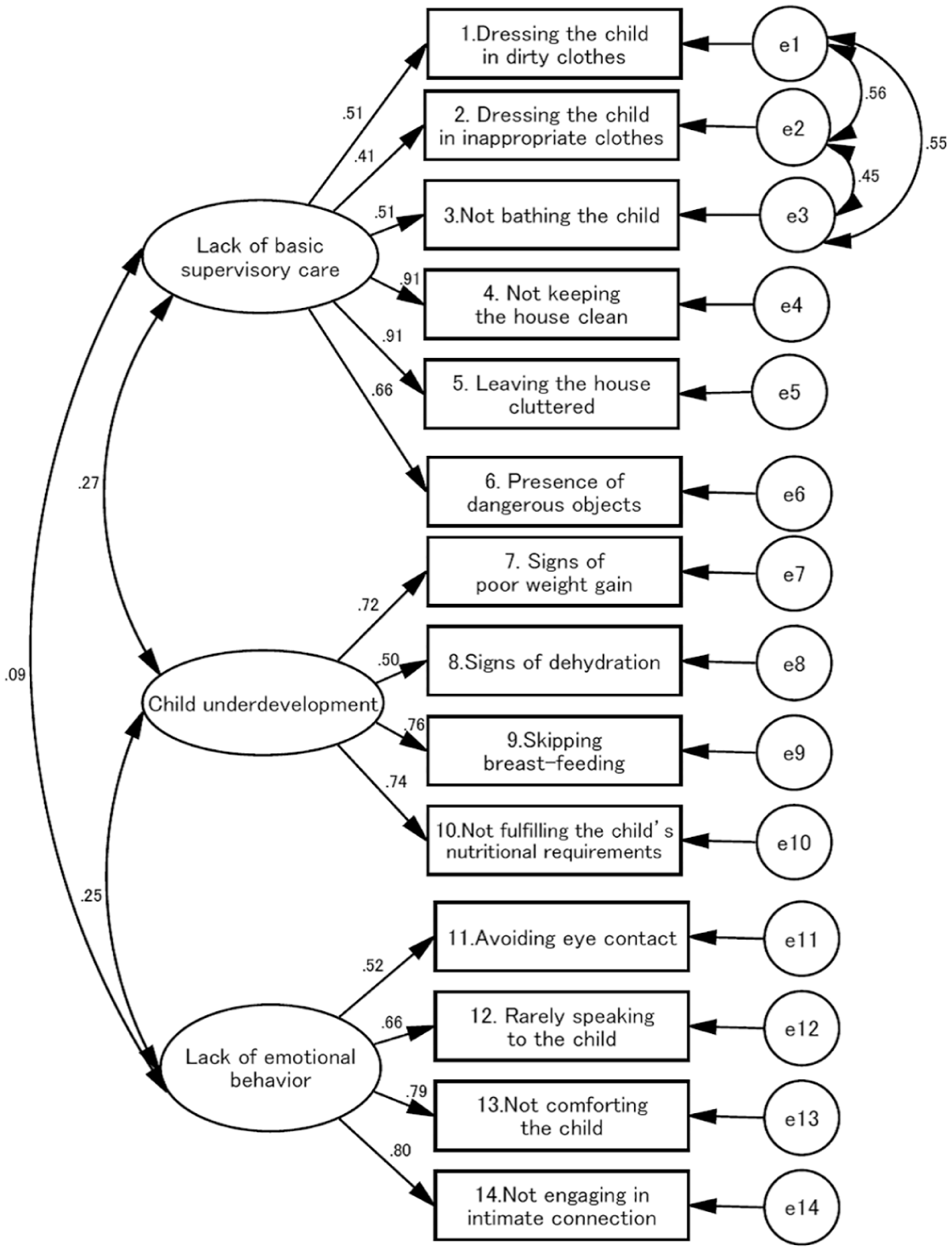
Confirmatory factor analysis for the Signs of Neglect in Infants Assessment Scale.
Internal Consistency and Validity
The mean score on the final SIGN was 11.0 (SD = 6.6). Cronbach’s alpha coefficients for the total SIGN, lack of basic supervisory care (Factor I), child underdevelopment (Factor II), and lack of emotional behavior (Factor III) were .82, .85, .81, and .87, respectively (Table 3). Correlations between all of the versions of the SIGN and the SIRPAN and between the SIGN and Child Guidance Center reporting status indicated conceptual consistency. The SIGN was positively correlated with the SIRPAN (Pearson’s r = .335, p < .001). The mean SIGN score of cases that were reported to the Child Guidance Center (M = 12.8, SD = 7.0) was higher than the mean SIGN score of cases that were not reported to the Child Guidance Center (M = 9.2, SD = 5.5, p < .001).
Discussion
The SIGN is a new professional-report tool for assessing the early signs of neglect in infants. The scale was developed to enable C/PHNs, who are at the frontline of public health, to provide support to caregivers and, in turn, reduce the prevalence of the neglect of infants and prevent current and future health consequences for children.
The results show that the SIGN has adequate internal consistency and validity and a useful structure. The confirmatory factor analysis model verified the construct validity and factor “correctness” of a set of 14 observed items on three factors: lack of basic supervisory care, child underdevelopment, and lack of emotional behavior. The scale’s internal consistency was high. Cronbach’s alpha was ≥.80 for all versions of the SIGN and for the three factors. Criterion-related validity was ≥ 0.30 for the comparison between the scores of the SIGN and the SIRPAN. Based on this collective evidence, the SIGN demonstrated adequate psychometric properties to measure signs of neglect to enable C/PHNs to prevent infant neglect. The results also demonstrated that the SIGN was able to discriminate between cases reported and not reported to the Child Guidance Center: The scores of all of the SIGN factors were higher for cases reported to the Child Guidance Center than for cases that were not reported. The moderate correlation between the SIGN and the SIRPAN could be interpreted as only one factor (lack of emotional behavior) in the SIGN being related because the SIRPAN focuses on mother–child attachment and interaction and evaluates both abuse and neglect (Grietens et al., 2004).
Items in Factor I (lack of basic supervisory care) are partially consistent with the “physical needs” domain of the Neglect Scale, a self-report scale completed by caregivers with children aged 3 to 11 years (Harrington et al., 1998), and with the “supervisory neglect” domain of the Child Neglect Questionnaire, where teenagers report the neglectful behavior of their parents (Stewart et al., 2015). This supports the idea that Factor I (lack of basic supervisory care) in the SIGN, assessed by C/PHNs, is consistent with the neglectful behaviors of caregivers. Welch and Bonner (2013) have stressed the importance of ensuring safety and preventing infant death. This domain is essential for infants because a lack of basic supervisory care negatively affects infant health and may cause death.
Items in Factor II (child underdevelopment) seem to be a unique domain of the SIGN for two reasons. First, nurses’ professional skills can be used to effectively assess aspects such as hydration, weight loss/gain, and breastfeeding. To our knowledge, previous studies using existing child abuse and neglect assessment scales for primary prevention in public health have not focused on these conditions of children’s deprivation and safety. Second, these signs have been shown to be important in preventing attachment problems, cognitive and emotional difficulties (Hildyard & Wolfe, 2002; Welch & Bonner, 2013), and deprivation in living and safety conditions among infants (Lounds et al., 2004).
Items in Factor III (lack of emotional behavior) are partially consistent with the “supervisory neglect” domain of the Child Neglect Questionnaire (Stewart et al., 2015) and with the “emotional needs” domain of the Neglect Scale (Harrington et al., 2002). The explanatory theory–based model of child neglect suggests that neglectful behavior of parents may be an outcome of an absence of empathy or empathy avoidance (Lounds, Borkowski, & Whitman, 2006). Neglectful mothers have been found to be significantly less likely to realize infants’ feelings of interest, more likely to perceive sadness and shame, and more inaccurate at judging infants’ emotions (Hildyard & Wolfe, 2007), as well as to have a more limited emotional vocabulary (De Paul & Guibert, 2008). Mothers showing fewer attachment and interaction behaviors with their infants have been assessed as being at higher risk of engaging in child abuse and neglect by SIRPAN scores (Grietens et al., 2004). Factor III in the SIGN could be used by C/PHNs to assess signs of emotionally neglectful behaviors of caregivers with infants.
In addition, Factor I (lack of basic supervisory care) and Factor III (lack of emotional behavior) in the SIGN may be able to assess the support needs of caregivers with mental health problems including postpartum depression and other mental conditions that are a potential cause of neglect. The present study showed that over 30% of the studied cases were characterized by mental health problems among the caregivers. Although the Edinburgh Postnatal Depression Scale (Cox, Holden, & Sagovsky, 1987) has been translated into Japanese (Okano et al., 1996) and has frequently been used to assess the severity of depression in Japan, the SIGN could add more information about the concrete support needs of households and individuals engaged in child rearing and thus contribute to the provision of appropriate support.
There are similarities and differences between the SIGN and other relevant tools. The measures differ in terms of the specificity of the core concept, the prevention level, and the age of the child. The core focus of the SIGN is on early signs of infant neglect, in contrast to other measures, which are mainly targeted at risk assessment for potential or apparent neglectful caregivers and neglected children referred to child protective services by child welfare professionals to assess the level of seriousness. Rayce et al. (2017) pointed out that the first year of a child’s life forms the foundation for a lifelong developmental trajectory. Other measures of child neglect are limited in their assessment of child neglect in infancy. The SIGN, however, explicitly measures signs of neglect in infants and their caregivers; this scale aims to help these groups by connecting them to the appropriate support at an early stage through public maternal and child health channels. The scale will make it possible to prevent neglect among infants by assessing signs of neglect.
Potential users of this new scale are C/PHNs working at maternal and child health sections in municipalities, home-visiting C/PHNs, and other nursing professionals. The SIGN could be used in maternal and child health programs, especially to assess the early signs of neglect. This scale could be used to evaluate the situation during home visits, to indicate the potential need for continuous support, and to monitor and reassess signs of neglect and review case management plans. Further research is needed to develop assessments for signs of neglect that focus on different developmental ages, for example, focusing on caregivers with children aged 1 to 5 years.
In addition to capturing latent signs that cannot be confirmed, the measurements of neglect in the SIGN may also predict neglect when these signs are directly observed in conversations with the caregivers. These predictors may affect outcomes among both caregivers and infants and influence community-level strategies and policies in the public health field aimed at preventing child neglect. The SIGN has potential utility to evaluate the strengths and weaknesses of caregivers, promote support, and prevent infant neglect. Effective programs and systems may use the SIGN for preventing neglect among infants in communities in the public health field and for promoting well-being among infants in the future.
The present study had several limitations. First, the cultural applicability of the SIGN scale should be carefully considered. Although this scale was developed in Japan, much of the literature used to create the tool was from Western contexts, and definitions may vary significantly by region despite being based on a comprehensive international review of previous studies. As Slack et al. (2003) have suggested, legal definitions and interpretations of child neglect may change over time and differ across regions, and may depend on the environment and community or social contexts. Second, the response rate in the present study was low, although we sampled one third of Japan’s municipalities where C/PHNs worked. It may be useful to examine data from other community and/or country contexts. Third, the tools used to assess validity (the SIRPAN and reporting to the Child Guidance Center) did not show only neglect but included both child abuse and neglect. This limits the external validity of our scale although 90% of the cases in this study were characterized by neglect only. Finally, this study had a cross-sectional design, which did not allow for the establishment of a causal relationship between SIGN score and the neglect (neglectful behaviors and infant outcomes) or well-being of children as a final outcome. A prospective design is needed to determine the scale’s predictive validity.
Conclusion
The SIGN was developed to enable C/PHNs to assess signs of infant neglect based on characteristics of infants and their caregivers in terms of a lack of basic supervisory care, child underdevelopment, and a lack of emotional behavior. It is a novel instrument with good psychometric properties. The results regarding validity and reliability show this scale to be an appropriate instrument for assessing signs of neglect to enable C/PHNs working in public health fields to prevent neglect among infants. Caregivers showing signs of neglect often do not perceive their needs or problems and do not seek support by themselves, and infants are unable to ask for help. The SIGN can contribute to understanding the early signs of neglect and to helping infants and caregivers with multiple needs for continuous case management that could lead to neglect. Future studies in cross-cultural different populations are needed to validate the SIGN scale’s properties using in English version or translating in other languages; then, this scale might be utilized to aid in prevention efforts internationally. Further prospective research is essential to determine the scale’s predictive validity and to explore the factors for infant neglect. The SIGN has the potential to contribute to preventing infant neglect and to promote well-being in both infants and their caregivers by providing early support.
Supplemental Material
9.AppendixA_SIGN_Scale_English_and_Japanese – Supplemental material for Developing and Validating a New Scale to Assess Signs of Neglect of Infants and Caregivers
Supplemental material, 9.AppendixA_SIGN_Scale_English_and_Japanese for Developing and Validating a New Scale to Assess Signs of Neglect of Infants and Caregivers by Azusa Arimoto and Etsuko Tadaka in Journal of Interpersonal Violence
Footnotes
Acknowledgements
The authors thank the community/public health nurses of all of the municipalities who participated in the study, as well as the experts who participated in the focus group at the beginning of the project. They thank Michelle Pascoe, PhD, from Edanz Group (![]() ) for editing a draft of this article and Jennifer Barrett, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this article and helping to draft the abstract.
) for editing a draft of this article and Jennifer Barrett, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this article and helping to draft the abstract.
Authors’ Note
A.A. was the principal investigator. A.A. and E.T. contributed to conception and design, analyzed the data, and wrote the manuscript. A.A. performed the survey for acquisition of data, A.A. and E.T. interpreted all the data, and A.A. was a major contributor in writing the manuscript. Both authors read and approved the final manuscript. The current study was approved by the Institutional Ethical Review Board of the School of Medicine, Yokohama City University, in Japan (No. A1608022) and has been conducted in accordance with the Ethical Guidelines for Epidemiological Research of the Japanese Government. All study participants provided written informed consent by completing and submitting the questionnaire, which was returned anonymously to ensure participant anonymity. The informed consent form explained the voluntary nature of participation, management of data, and publication of results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number JP26861988 (Principal investigator [PI]: Dr. Azusa Arimoto).
Supplemental Material
Supplemental material, English version and Japanese version of the Signs of Neglect in Infants Assessment Scale (SIGN), for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.