
Abstract
Black mothers with HIV (BMWH) face treatment adherence (TA) challenges, shaped by gendered anti-Black racism, oppression, and structural inequalities, which hinder healthcare access, support, and well-being. Compounded by mothering responsibilities, understanding the determinants of TA is critical to addressing their unmet needs. We utilized an explanatory cross-sectional, multiphase sampling survey design. Twenty-five BMWH completed a 30-min online survey assessing their demographics, TA, and determinants. Spearman's correlation coefficient assessed associations between psychosocial and structural determinants and TA. Mann-Whitney U-tests explored group differences by TA status (< 85%; ≥ 85%). BMWH were middle-aged (M = 42, SD = 13.77), single (64%), low-income (60%), long-term survivors (M = 15, SD = 9.72), and treatment adherent (85.36%). HIV-related resilience was associated with increased TA (rs = .46, p = .05), while perceived stress was associated with reduced TA (rs = −.46, p = .05). Statistically significant differences were found in depression and perceived stress scores by adherence status. Sub-optimally adherent BMWH reported greater perceived stressors (Mdn = 174.5), and higher depression (Mdn = 167). Findings suggest that stress and mental health symptoms contribute to suboptimal TA. Multilevel interventions are needed to address maternal distress and improve HIV treatment outcomes among BMWH.
Compared to other racial and ethnic groups in the U.S., Black women with HIV experience lower adherence to antiretroviral therapy (ART) treatment and lower rates of viral suppression—key indicators of the continuum of care for people living with HIV (Centers for Disease Control and Prevention [CDC], 2024). Viral non-suppression — an immune system's inability to fight and suppress a foreign pathogen, in this case HIV — has been linked to insufficient adherence to ART (CDC, 2021). Optimal ART adherence is defined as maintaining at least 95% medication adherence as prescribed, whereas suboptimal adherence is characterized by medication adherence rates falling below 95% (CDC, 2021). Factors that promote optimal adherence to ART include the establishment of consistent medication-taking routines, regular attendance at medical appointments, continuous engagement with prescribed treatment regimens, and timely initiation of ART when clinically indicated (CDC, 2021; Panel on Antiretroviral Guidelines for Adults and Adolescents, 2017). Consequently, suboptimal ART adherence is frequently a key factor in the progression of acquired immunodeficiency syndrome (AIDS), primarily due to the elevated levels of HIV virus in the system and the subsequent depletion of healthy immune cells (i.e., CD4 T-cells). The onset of immunodeficiency, characterized by a reduced capacity of the immune system to combat infectious agents, leads to an increased vulnerability to opportunistic infections and co-occurring diseases, including tuberculosis, pneumonia, and Hepatitis C virus (HCV) (Fauci et al., 1996; Palefsky & Holly, 2003; Skarbinski et al., 2015). This increased vulnerability to opportunistic infections and co-occurring diseases underscores the critical importance of structured and comprehensive healthcare frameworks, such as the HIV Care Continuum, in managing and treating people living with HIV.
HIV Care Continuum for People Living with HIV
The HIV care continuum provides a well-defined clinical framework for the treatment and management of HIV (CDC, 2021; Gardner et al., 2011; Roscoe & Hachey, 2020). It consists of five key domains: testing and diagnosis, linkage to care, engagement in care, adherence to antiretroviral therapy (ART), and viral load suppression (Gardner et al., 2011). Structured in a sequential manner, each stage of the continuum is designed to build on the previous one to ensure the best possible health outcomes.
The first stage of the HIV care continuum is testing and diagnosis, where individuals receive a clinical diagnosis as living with HIV. The second stage, linkage to care, involves connecting patients to specialized healthcare providers who have expertise in HIV care. After linkage, the third stage focuses on engagement or retention in care, which involves ongoing monitoring and documenting HIV care outcomes. The fourth stage centers on the initiation and adherence to antiretroviral therapy, a key treatment for both managing HIV and preventing its transmission. The final stage of the HIV care continuum, viral suppression, is achieved when HIV RNA test results show fewer than 200 copies/mL (CDC, 2020). Research indicates that a viral load below 200 copies/mL sustained for at least six months is considered undetectable, which signifies that HIV is intransmissible, meaning it cannot be transmitted through sexual contact (Eisinger, Diffenbach & Fauci, 2019; Rathbun et al., 2021). While traditional guidelines suggest that optimal adherence to ART requires 95% compliance, recent studies show that viral suppression can still be achieved with lower adherence rates. For example, a study found that an adherence rate of 82% was sufficient to achieve viral suppression in 90% of viral load tests, aligning with adherence levels seen in other chronic conditions, such as hypertension (Byrd et al., 2019).
ART Treatment Adherence Considerations for Black Women
Adopting behaviors that support consistent use of ART is essential for improving health outcomes for Black women living with HIV (Lambert et al., 2018). As of 2024, the CDC estimated that the viral suppression rate for Black women was 62.1%, lower than that for White women (63.9%), Latina women (65.8%), and American Indian/Alaska Native women (62.9%), but higher than that for Native Hawaiian/Pacific Islander women (59.7%) (CDC, 2024). However, data from the Ryan White HIV/AIDS Program (RWHAP), which provides insurance and support services for people with HIV, show more promising results for Black women, with a viral suppression rate of 89.1% in 2024, compared to the national target of 95% (HRSA, 2024).
The treatment adherence challenges experienced by Black women are often shaped by gendered anti-Black racism, oppression, and structural inequalities, which hinder healthcare access, support, and overall well-being (Dale & Safren, 2020). The demands of mothering can further complicate treatment adherence (Etowa et al., 2022). Notably, Black mothers with HIV (BMWH) prioritize their role as caregivers as they navigate the complexities of maternal well-being and family well-being (Mangum et al., 2024). The enduring cycle of balancing personal unmet needs and family unmet needs leads some BMWH to prioritize their children's care over their own, enacting triage behaviors to address their children's needs first (Boehme et al., 2014; Kedia et al., 2020; Mangum et al., 2024). Additionally, many BMWH navigate social systems shaped by HIV-related stigma and discrimination, structural and systemic racism, poverty, and caregiving responsibilities being the head of household (Caiola et al., 2018; Etowa et al., 2020). These intersecting challenges significantly affect their ability to achieve optimal treatment adherence outcomes. There has been a dearth of research within the last decade focusing on BMWH and ART adherence outcomes. Therefore, the ability to comparatively assess previously identified factors is limited. This work extends the existing body of research on psychosocial factors and structural factors impacting ART treatment adherence among BMWH.
Relevance to Social Work
Examining how psychosocial and structural factors impact ART adherence among BMWH is essential for advancing social work research, practice, and education. Social workers play a crucial role in helping people living with HIV connect to medical care and support services, advocating for their rights, and shaping local, state, and federal HIV-related policies (Shukla et al., 2017). Given the diverse roles that social workers fulfill and the range of their training, those with specialized expertise in HIV prevention and treatment can offer vital support to mothers’ post-diagnosis, ensuring continuity of care throughout their treatment. Moreover, social workers are skilled at working within interdisciplinary teams, bringing diverse perspectives, focusing on individuals’ strengths, and using a person-in-environment approach to create effective solutions to challenges.
In line with this framework, the National Association of Social Workers (NASW) Code of Ethics highlights the ethical duty of social workers to challenge social injustice, urging professionals to “engage in social change, particularly on behalf of vulnerable and oppressed individuals and groups” (NASW, 2017). Similarly, the National Association of Black Social Workers (NABSW) advocates for “a world where individuals of African descent are free from racial domination, economic exploitation, and cultural oppression, emphasizing the need for Black social workers to work toward this vision” (NABSW, p. 2). The NABSW's code of ethics further calls for Black social workers to actively support social change, acknowledging the interconnectedness of people of African ancestry and the importance of uplifting marginalized communities. By addressing the needs of these vulnerable groups, Black social workers contribute to the broader well-being of Black families and communities. Additionally, women and children represent a substantial portion of the populations social workers engage with, particularly within family contexts. Therefore, it is only fitting that social workers are equipped with the knowledge and skills necessary to effectively support people living with HIV (Parrish et al., 2003). To effectively support people living with HIV, it is essential for social workers to draw on theoretical frameworks that inform their understanding of treatment adherence, particularly among BMWH.
Theoretical Frameworks for Understanding Treatment Adherence among Black Mothers With HIV
The ongoing HIV epidemic in the United States has affected diverse populations over a span of 43 years (Read et al., 2022). Since the initial cases reported among gay, white men, initiatives have been developed, implemented, and prioritized to reduce the new cases of HIV (Ojikutu & Mayer, 2021). Despite various national and state specific policy interventions aimed at addressing HIV acquisition, HIV disparities continue to disproportionately impact Black women compared to their white counterparts. This ongoing inequity underscores the need for more targeted and inclusive strategies that address the challenges encumbered by Black women in the fight against HIV (Rajabiun et al., 2023). Before this can occur, greater discussion of the differential structural and psychosocial factors impacting HIV health disparities outcomes is warranted. Health disparities are commonly understood as “preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations” (CDC, 2024, p.1). Health disparities are often attributed to structural factors such as social determinants of health (e.g., poverty, racism, education, poor housing conditions), environmental factors (e.g., neighborhood divestment, pollution, community violence, built environment, transportation), individual factors, and historical factors (e.g., differential distribution of resources, power, and privileges) (Braveman, 2006; Mullings, 2005). To elucidate the interconnection of health disparities, psychosocial and structural factors and BMWH health outcomes, Black Feminist Thought, Sojourner Syndrome, and Stress and Coping Theory together offer a comprehensive understanding of why and how challenges with sub-optimal treatment adherence and non-viral suppression emerge and subsequently impact U.S. Black women differently than other ethnic and racial groups. This intersectional approach sheds light on how systemic inequalities and stressors affect the health outcomes of Black women, highlighting the constraints Black women face, how they navigate these spaces as acts of survival, and forces us to reckon with the demonstrative effects of White Supremacy.
Black Feminist Thought
Black Feminist Thought contextualizes Black womanhood in the U.S. by highlighting how subjugation and marginalization at the intersections of multiple minoritized social identities— such as race, gender, and class—perpetuate oppression and discrimination, including gendered anti-Blackness, and economic disparities, across multiple aspects of life (Hill Collins, 2000). For Black mothers who are managing the household and are the primary caregivers, structural and institutional experiences of discrimination and oppression can exacerbate and increase the load they already bear. Hill Collins describes these practices as manifesting through three key constructs: matrix of domination, controlled images, and outsider within (2000). The matrix of domination explains the ways in which oppression is organized and maintained in society. For example, the U.S. operates within caste-like systems that maintain social order by establishing dominant and subordinate groups, such as men vs. women, old vs. young, white vs. non-white, wealthy vs. poor, etc. Social order is further delineated within social rankings on the basis of gender, race, and class, such that a rich white man holds a higher social position than a Black rich man, or a poor white woman holds greater social capital than a poor Black woman. These systems of oppression are reinforced by socially constructed identities and are perpetuated through the socialization processes that uphold these hierarchical distinctions (Love, 2000).
Controlled images illustrates how opposing social constructions and stereotypes of Black womanhood compared to expectations for white womanhood, form the basis for the subjugation of Black women and justify discrimination against them. Controlled images thrive within the matrix of domination and are a byproduct of socialization processes that perpetuate the dominant group's superior position. The concept of outsider within describes Black women's experiences of marginalization and othering within predominantly white spaces, similar to tokenism, where representation in a majority space occurs without genuine inclusion and a sense of belonging. Consequently, being relegated to disequal, disadvantaged, and often disenfranchised societal positions impacts Black mothers profoundly, affecting their personhood and their roles as caregivers of dependent children.
Stress and Coping Theory
Stress and Coping theory explicates the iterative process of encountering and responding to environmental stressors. It focuses on how individuals experience stress and their strategies to manage and adapt to these challenges (Lazarus & Folkman, 1984). It delineates the process of engaging in cognitive and behavioral responses to the cognitive appraisal of stimuli perceived as threatening, challenging, or harmful. Researchers studying the stress and coping phenomena among Black populations have adapted the theory to account for social cognitive processes and responses to racial stressors induced by social constructions of race, racial hierarchy, and anti-Black racism to contextualize the lived experiences of Black people more fully (McGuffey & Sharpe, 2015). This impacts how we interact with systems and experience oppression, influencing the physiological, physical, and emotional effects of racial and gendered stress and the coping responses that follow.
Sojourner Syndrome
Sojourner Syndrome is an interpretive intersectional framework, developed by Mullings (2005), to describe and explain the consequential effects of gendered anti-Blackness and resource inequality, inclusive of structural and systemic discriminatory policies and practices perpetuated against Black women, and its subsequent effects on Black women's health. Mullings describes Sojourner Syndrome, as a gendered form of John Henryism, and considers the phenomenon a survival strategy and coping resource for Black women, with both short-term and long-term benefits (2005). The framework's strengths lie in the conceptualization of how society invokes differential expectations, protections (e.g., womanhood, motherhood, femininity), and guarantees of freedom and living through inherently inequitable processes at the group level as opposed to focusing on individual-level behaviors, which directly impacts the observed differential health outcomes among U.S. social groups across socioeconomic status. In addition to naming the harmful effects of subjugation and marginalization, Sojourner Syndrome highlights how Black women cope with multiple structural stressors and resist the substandard realities, hopelessness, helplessness, and apathy, that accompany these experiences. Considering the implications of optimal ART adherence outcomes, these theories and frameworks help to contextualize how structural and systemic oppressive factors are often the cause of poorer health outcomes among BMWH. As our study sought to identify structural and psychosocial factors associated with treatment adherence among BMWH, our guiding research question was “What are the perceived psychosocial and structural factors impacting treatment adherence among BMWH?”
Method
Study Hypotheses
In order to answer the research question, the study aimed to identify psychosocial factors such as emotional distress, perceived social support, HIV-related resilience, and structural factors, such as access to care, associated with ART adherence among BMWH. The hypotheses of the study were:
Hypothesis 1a: There will be a significant relationship between psychosocial and/or structural factors and ART adherence such that key psychosocial (e.g., perceived stress) and structural (e.g., discrimination) factors will be associated with
Hypothesis 1b: There will be a significant relationship between psychosocial and/or structural factors and ART adherence such that key psychosocial (e.g., resilience) and structural (e.g., barriers to care) factors will be associated with
Hypothesis 1c: There will be a significant association of psychosocial and structural impacts on treatment adherence by treatment adherence status, such that BMWH with reported suboptimal treatment adherence will have increased psychosocial and structural factors adversely impacting treatment adherence than BMWH with optimal treatment adherence.
Study Design
The study employed an explanatory cross-sectional survey design to examine the relationships between psychosocial and structural factors and ART treatment adherence among BMWH. It used multiphase non-probability sampling, including purposive and snowball sampling methods, to recruit 25 eligible participants across the United States. Participants completed a web-based survey that assessed various aspects, including overall health status, perceived barriers to HIV care, social support, ART treatment adherence, parenting-related concerns, HIV-related resilience, everyday discrimination, anxiety and depression, and perceived stressors.
Participants
Eligible participants met the following inclusion criteria: 1. Black or African American, 2. cisgender woman, 3. adult (18 years old), 4. self-reported HIV diagnosis, 5. primary caregiver or legal guardian of at least one child under 18 years old, 6. engaged in HIV care, 7. prescribed antiretroviral medication at the time of the study, and 8. not married. However, married women were screened out in greater numbers; therefore, in March 2022, the inclusion criteria were revised to include married women in the study.
Procedure
Participants initially completed a pre-screening questionnaire to determine eligibility (Qualtrics, 2022). Those who met the inclusion criteria then reviewed and signed the electronic informed consent document. Detailed methods have been described previously (Mangum, 2023). Participants who completed the self-administered web-based survey received a $25.00 Mastercard gift card as compensation. They could also earn an additional $5.00 for each referral of other Black women with HIV. To ensure confidentiality, those who agreed to make referrals were provided a personalized email survey link to share within their networks. Data collection occurred from January 28, 2022, to April 25, 2022, resulting in a final sample of 25 participants.
Online recruitment was conducted through social networking sites such as Facebook and Instagram. Paid advertisements and posts were created on the study's Facebook page, Black Mothers ART Treatment Adherence Research Study and digital study flyers were shared on Facebook Group pages. An Instagram account was also established, where the study poster was posted. Additionally, recruitment materials were advertised through a university-affiliated online research participant recruitment platform Pitt+Me. AIDS-serving organizations and infectious disease clinics were also approached to recruit participants from agencies that provide services to Black women living with HIV. The University of Pittsburgh Institutional Review Board approved this study on January 27th, 2022. Participants were informed of the following verbiage on the online survey consent form “participation in the study is confidential. To safeguard your information, your name will not be attached to any data, but a study number will be used instead. The data will be kept on a password-protected computer and storage device using special software that scrambles the information so that no one can read it except members of the study team. The web-based survey will be collected using firewall-protected servers and devices. A code linking your identifiable information to your study number will be kept on a password-protected database behind the University of Pittsburgh firewall, accessible only to research study staff members.” Participants were also advised that participation in the study would not impact their medical services that they receive from the university affiliated medical center.
Measures
Data were collected on participants’ age (years), year of HIV diagnosis (“What year did you receive your HIV diagnosis?”), housing status (years of current residence), insurance coverage (yes or no) and type, educational attainment, total household income, employment status, marital status, and the number of minor children in the home. Participants responded to single-item questions regarding their substance use behaviors, mental health status, and places to receive primary care, HIV care, dental care, and mental health services. They were also asked about their HIV care behaviors within the past year (appointments scheduled vs. appointments attended, labs completed) and barriers to care. These single-item questions are a combination of categorical, nominal, and ordinal-level variables, which provided a health status profile for each participant.
ART Adherence
The outcome variable, ART adherence, was assessed using one self-report item where respondents recalled their adherence to ART over the past month. Participants were asked, “Over the past month, what percentage of the time did you take your medications as prescribed?” Participants were asked to use a visual analog scale ranging from 0 to 100. To capture the response, they adjusted the arrow on the scale to the number that best represented their ART adherence over the past month. The cut point for ART adherence status in this sample was set at 85%, based on the mean ART adherence rate of 85.36% observed in the sample. The cut point was coded as ≥ 85% = 1, indicating optimal adherence, and < 85% = 0, indicating sub-optimal adherence. An adherence level of 85% was chosen as it is considered appropriate compared to the gold standard of 95%, given the potency of ART medications and the fact that people living with HIV are achieving viral suppression at lower adherence rates (Byrd et al., 2019).
Anxiety
The Emotional Distress Anxiety (EDA) short form (Pilkonis et al., 2011) is a four-item scale used to measure anxiety. The items include: “In the past 7 days, I felt fearful,” “I found it hard to focus on anything other than my anxiety,” “My worries overwhelmed me,” and “I felt uneasy.” Participants rated each item on a 5-point Likert scale, where 1 = never and 5 = always. The EDA short form demonstrated high internal consistency in this sample, with a Cronbach's alpha of 0.92.
Depression
The Emotional Distress-Depression (EDD) short form (Pilkonis et al., 2011) was used to measure depression (“In the past 7 days, I felt worthless, I felt helpless, I felt depressed, I felt hopeless”). Participants rated each item on a 5-point Likert scale where 1 = never and 5 = always. The EDD short form demonstrated high internal consistency (a = 0.94) in this sample.
Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) (Zimet et al., 1988) is a 12-item measure to assess participants perceived social support from family, friends, and significant others. Sample items include: “I can talk about my problems with my family,” “I have friends with whom I can share my joys and sorrows,” and “There is a special person in my life who cares about my feelings.” Participants rated their agreement with each item on a 7-point Likert scale, where 1 = very strongly disagree and 7 = very strongly agree. The MSPSS demonstrated high internal consistency in this sample, with a Cronbach's alpha of 0.98.
Barriers to HIV Care
The Barriers to Care Scale (Heckman et al., 1998) is a 12-item measure used to assess varying barriers to medical and mental health care and service access among people living with HIV. The twelve items are grouped into four sub-scales: geography/distance barriers, medical and psychological service barriers, community stigma barriers, and personal resource barriers (Heckman et al., 1998). Participants rated each item on a 4-point Likert scale (1 = no problem at all, 2 = very slight problems, 3 = somewhat a problem, 4 = major problem). The Barriers to Care Scale 12-item measure returned a high internal consistency (a = 0.91) in this sample.
Racial Discrimination
Daily discrimination experiences were measured using The Everyday Discrimination Scale (Williams et al., 1997). The nine-item scale is designed to measure the subjective experiences of overt, daily discrimination towards a minoritized population; specifically, it captures data on chronic and routine unfair treatment in everyday life. Participants were provided with nine different descriptions of acts of discrimination (“In your day-to-day life, how often do the following things happen to you? You are treated with less courtesy than other people are? You are treated with less respect than other people are? You are threatened or harassed?”) and were asked to rate them. Responses were rated on a 6-point Likert scale ranging from 0 = never to 5 = almost every day. The Everyday Discrimination Scale revealed high internal consistency (a = 0.85) in this sample.
Parental Distress
Parenting distress was measured using seven single items capturing worry as it relates to being a mother living with HIV (“During the past six months, how often have you worried about your children's health?”, “During the past six months, how often have you been worried that your child/children will grow up without you?”). Items were gathered from a parenting self-efficacy scale administered to participants of the Women Interagency HIV Study (WIHS) longitudinal study (D'Souza et al., 2021). WIHS participants are primarily low-income African American women. Participants were asked to rate their response on a 5-point Likert scale (1 = not at all to 5 = a lot/extremely). The seven items returned a moderate internal consistency (a = 0.69) in this sample.
HIV-Related Resilience
The People Living with HIV Resilience Scale (Gottert et al., 2019) is a ten-item measure designed to assess resilience among people living with HIV. Participants evaluated how specific aspects of their lives were affected by their HIV status, with prompts such as “my self-confidence,” “my self-respect,” “my ability to cope with stress,” and “my ability to find love.” Responses were rated as +1 for aspects positively affected by HIV, −1 for negatively affected, and 0 for unaffected aspects. The initial validation of the scale, conducted with a sample of African women living with HIV in Cameroon, Uganda, and Senegal, demonstrated good reliability (Cronbach's alpha of 0.81). In this sample, the People Living with HIV Resilience Scale showed moderate internal consistency, with a Cronbach's alpha of 0.75.
Perceived Stress
The Perceived Stress Scale (Cohen et al., 1983) measured perceived stress among BMWH. The 14-item scale assessed the perception of stressors by events occurring in the last month (“In the last month, how often have you been upset because of something that happened unexpectedly?”, “In the last month, how often have you felt that you were effectively coping with important changes that were occurring in your life?”). Responses were rated on a 5-point Likert scale, where 0 = never and 4 = very often. The Perceived Stress Scale revealed moderate internal consistency (a = 0.78) in this sample.
Data Analysis
Univariate analyses were conducted to examine the distribution of various sociodemographic variables, including age, year of HIV diagnosis, housing stability, health insurance status, type of health insurance, highest level of education, income level, total household income, employment status, marital status, and the number of children living in the home. These analyses included measures of central tendency and dispersion. Next, bivariate analyses were performed to explore the relationship between ART adherence and potential confounding variables using Pearson's correlation coefficient. A chi-square test of independence was then conducted to assess differences in ART adherence based on categorical demographic characteristics, such as age (younger than 45 years vs. older than 45 years) and recent alcohol use (yes vs. no). Independent samples t-tests were also used to examine mean differences in perceived stress, everyday discrimination, depression, anxiety, parenting distress, resilience, and social support between sub-optimally adherent and optimally adherent Black mothers with HIV. All univariate and bivariate analyses were conducted using STATA v. 17 (StataCorp, 2023).
A power analysis was conducted to ensure adequate power for each statistical test. For Research Question #1, which involved Pearson's correlation coefficient and independent samples t-test, the following estimates were made:
To detect a medium-sized effect (correlation of 0.50) with an alpha of 0.05 and a power of 0.80, a total sample size of 24 participants was required (Kohn & Senyak, 2022). For the independent samples t-test, to detect a medium-sized effect (0.50) with an alpha of 0.05 and a power of 0.80, a total sample size of 26 participants was needed (Faul et al., 2007). The final sample size of the study was 25 participants. To test for skewness and normality of the data, a set of Shapiro Wilk tests were conducted. It was determined that the data were not normally distributed. As such, the non-parametric test of the Spearman's Correlation Coefficient was conducted in substitution of the Pearson Correlation. In addition, to account for the sample being under powered for independent samples T-test analyses, the Mann-Whitney two-sample rank sum Test— the non-parametric equivalent to determine mean differences by adherence status for our non-normally distributed variables, which can also be used for studies with small sample sizes (Conover & Iman, 1981) - was used.
Results
Sample Sociodemographic Characteristics
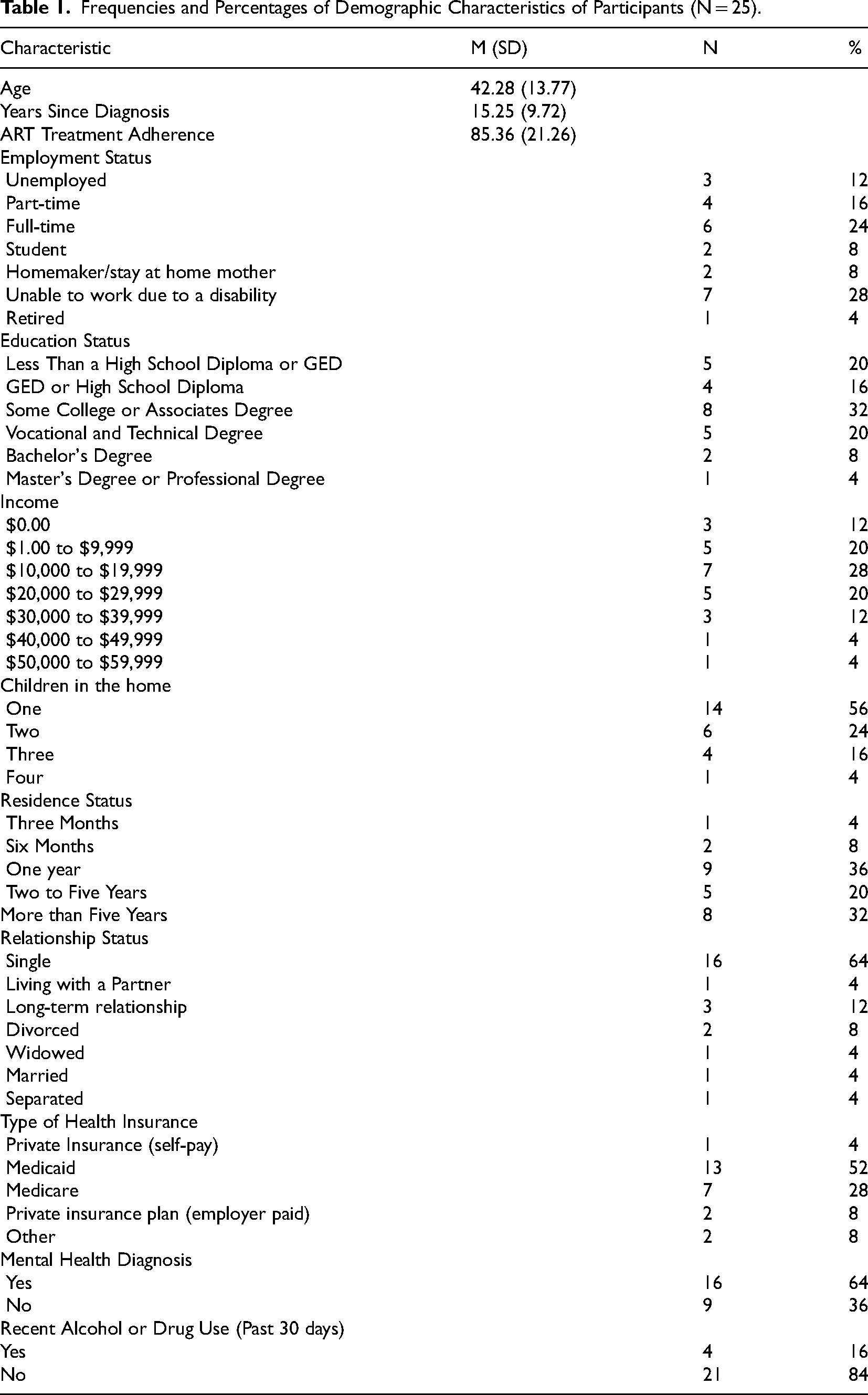
Table 1 summarizes the sociodemographic characteristics of the sample (N = 25). On average, BMWH were middle-aged (M = 42.28, SD = 13.77), single (64%), and nearly one-third (28%) reported being unable to work due to a disability. On average, participants’ years with HIV was 15.6 years (SD = 9.72), and the average ART adherence was 85.36%. Most of the participants (64%) reported having a mental health diagnosis. Sixty percent of participants reported an annual income of less than $20,000.00 or living below the federal poverty line, and 32% reported having some college education or an associate degree. Most participants (88%) reported being stably housed.
Frequencies and Percentages of Demographic Characteristics of Participants (N = 25).
Psychosocial and Structural Correlates of Antiretroviral Adherence
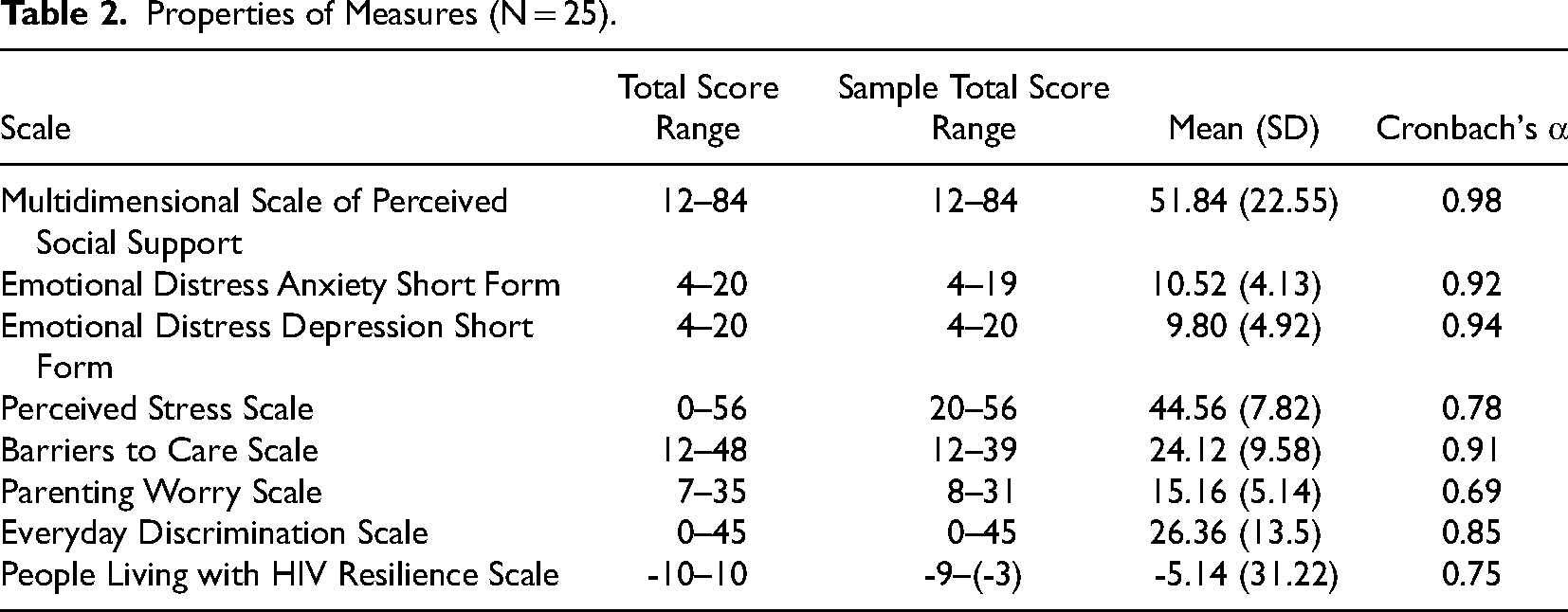
Table 2 summarizes the properties of the measures and the sample's statistics. Table 3 outlines all statistically significant Spearman's correlation coefficients. HIV-related resilience was moderately correlated with ART adherence rs = .49, p = .05. Conversely, perceived stress was negatively correlated with ART adherence, rs = -.46, p = .05. There was no statistically significant relationship found between everyday discrimination, barriers to care, parenting worry, social support, depression, and anxiety, and ART adherence. In addition, a chi-square test of independence showed that there was no significant association between age (younger than 45 years vs. older than 45 years) and ART adherence, and recent alcohol or drug use in the past 30 days (yes vs. no) and ART adherence.
Properties of Measures (N = 25).
Spearman's Correlation Matrix of Psychosocial and Structural Factors and ART Adherence
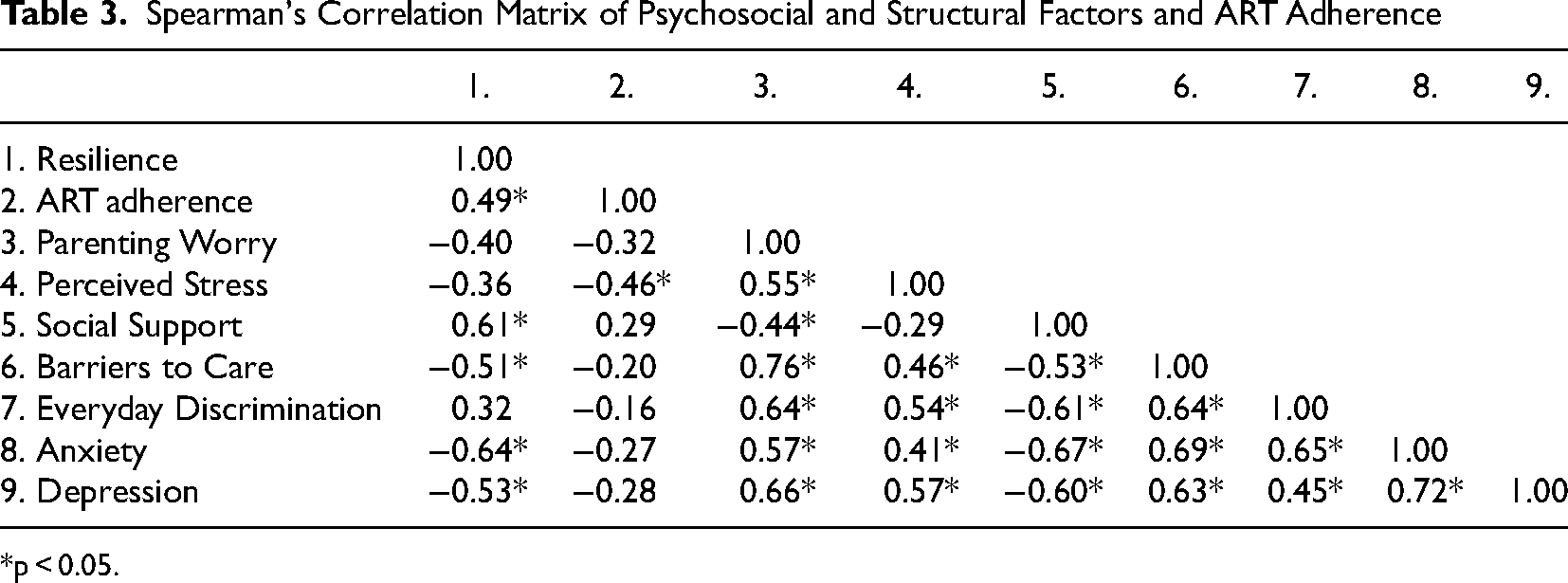
*p < 0.05.
Group Mean Differences in Antiretroviral Treatment Adherence
Table 4 summarizes the results of the Mann-Whitney two sample rank-sum U-tests for each psychosocial and structural measure by ART adherence status (group A: sub-optimally adherent N = 10, group B: optimally adherent N = 15). There was a significant difference in perceived stress scores between sub-optimally adherent and optimally adherent BMWH.; U = 325.00, z = 2.49, p = 0.01. Perceived Stress scores were higher among group A (Mdn = 174.5) while perceived stress scores were lower among group B (Mdn = 150.5). Similarly, there was a significant difference in depression scores between sub-optimally adherent and optimally adherent BMWH; U = 325.00, z = 2.06, p = 0.03. Emotional Distress Depression scores revealed higher depression scores among group A (Mdn = 167) compared to lower depression scores which were found among group B (Mdn = 158). No statistically significant group mean differences by ART adherence status were observed in HIV-related resilience, social support, barriers to care, anxiety scores, parenting worry, and everyday discrimination scores.
Two-Tailed Mann-Whitney U Test for Psychosocial and Structural Factors by Treatment Adherence Status.
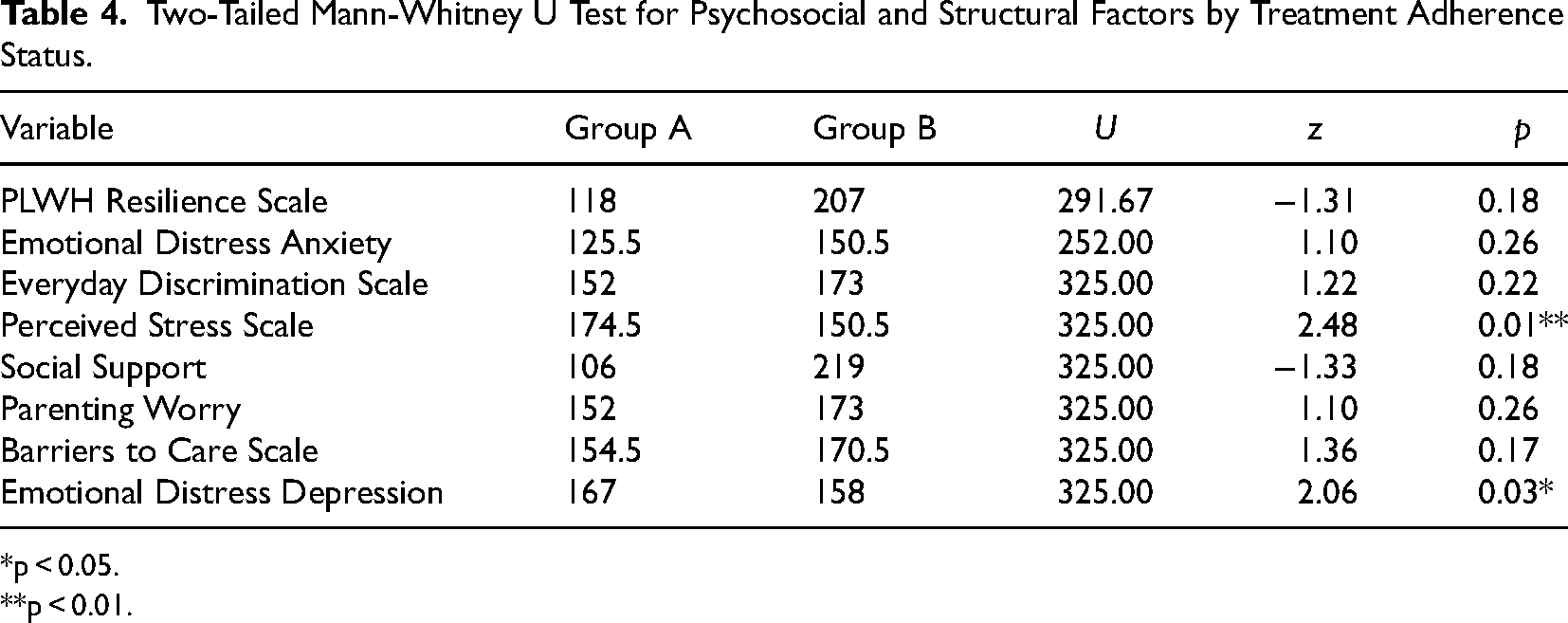
*p < 0.05.
**p < 0.01.
Discussion
This study examined the relationship between psychosocial and structural determinants—including emotional distress, perceived social support, HIV-related resilience, and barriers to care—and ART treatment adherence among a national sample of Black mothers with HIV. It was hypothesized that psychosocial and structural factors such as emotional distress, perceived discrimination, and barriers to care would be associated with reduced ART adherence, while factors such as perceived social support and HIV-related resilience would be associated with increased ART adherence. In addition, it was hypothesized that Black mothers with suboptimal ART adherence would experience elevated emotional distress (e.g., anxiety, depression, perceived stress), discrimination, and barriers to care compared to Black mothers who experience optimal ART adherence. In both cases, the findings supported the hypotheses that there is a relationship between psychosocial factors and ART treatment adherence in this sample.
HIV-related resilience was found to be associated with ART adherence. Although research on resilience and ART adherence among BMWH is limited, these findings align with existing evidence suggesting that, over time, Black women with HIV tend to develop greater acceptance of their diagnosis, improve their ability to cope with HIV-related stigma and achieve higher levels of self-acceptance (Dale & Safren, 2018; Sangaramoorthy et al., 2017). In our sample, Black mothers had been living with HIV for an average of 15 years. It is plausible that, as long-term survivors, these mothers have developed positive and adaptive coping mechanisms to manage HIV-related stressors effectively. The People Living with HIV Resilience Scale aligns well with the Stress and Coping Theory, which emphasizes self-efficacy and perceived situational control as key constructs. According to this theory, having a sense of control over stressful situations enhances one's self-efficacy in managing perceived stressors. Sojourner Syndrome would suggest that with perceived situational control and self-efficacy, Black mothers are able to engage in “transformative work” to not only address change but “transform the constraints that confront them” to which they had control over (Mullings, 2005, p. 80). It can also be argued that resilience is an act of survival (McLane-Davison, 2016; Mullings, 2005). The Sojourner Syndrome would also suggest that the demonstrated resilience is an act of resistance to the gendered Anti-Black experiences one faces on a daily basis. Thus, as a result of being subjected to multiple oppressions and structural vulnerability, Black mothers have acquired mechanism to manage, outside of the roles and scripts society assigns to them. In addition, existing research has highlighted that motherhood often serves as a strong motivator for engaging in HIV care, thereby supporting effective self-management and optimal adherence to ART (Boehme et al., 2014; Duthely et al., 2021). Sojourner Syndrome would suggest that this strong conviction for mothering is guided by an inherent value held by Black women which is the importance of family ties, stemming from family separation during chattel slavery. A lack of HIV-related resilience could look like avoidant behavior, disengagement from family, lack of involvement with children (Smith et al., 2001). As social workers providing care and treatment to BMWH, we must tailor our health assessments and mental health screenings to include a focus on self-efficacy and perceived control. Additionally, linking BMWH to maternal and family health services is essential for providing long-term support for both acute and chronic mental health trauma.
Consequently, perceived stress was negatively associated with ART treatment adherence. These findings are consistent with existing research, which shows that maternal stressors can contribute to decreased ART adherence among BMWH (Duthely et al., 2021; Murphy et al., 2010). Stress and Coping Theory would suggest that BMWH are identifying stressors in their environment that are harmful, challenging, or threatening. What is left to be deciphered and assessed are their coping resources to equip their coping responses to stressors. Given that the sample predominantly consisted of single women, these findings may indicate that single mothers experience higher levels of stress. Additionally, being the primary caregiver for multiple children could further contribute to maternal distress. Existing research suggests that BMWH who care for two or more children tend to have lower ART adherence than those who parent only one child or are childless (Merenstein et al., 2008). Assuming sole responsibility for child-rearing imposes additional burdens on BMWH, compelling them to manage their children's needs, handle household tasks, and fulfill various non-parental roles and responsibilities (Etowa et al., 2022). These challenges may stem from a lack of social support or a limited social network to help (Edwards et al., 2012; Kedia et al., 2020). Additionally, HIV non-disclosure to family and friends could contribute to these difficulties, as it may limit the availability of emotional and practical support (Mangum et al., 2024). As a result, neglecting HIV care can negatively impact their physical health, which in turn affects their ability to fully perform their caretaking duties and responsibilities. To further illustrate, an unintended consequence encountered by BMWH is that, due to their difficulties with self-management, their minor children often assume caregiving roles and responsibilities within the household to support their parents (Edwards et al., 2012). Moreover, Black mothers with HIV may experience a lack of perceived control in areas where they feel the most worried. This is significant because Black mothers often see themselves as protectors of their families; if they believe they are unable to safeguard their children, it could lead to increased distress. Together, these findings further articulate the impact of maternal stressors on BMWH. The daily stressors of parenting and navigating the world are compounded by racial inequality, gender discrimination, and resource inequality, which are drivers of HIV health disparities. HIV care interdisciplinary teams must adopt culturally relevant and BMWH-centered clinical approaches into routine care that are responsive to the needs of the family system, which is inextricably linked to HIV care outcomes for BMWH. By acknowledging the existence of chronic subjugation and marginalization and structural vulnerabilities in addition to mothering responsibilities, healthcare providers can offer more effective, compassionate care tailored to their specific circumstances.
In the present study, BMWH who reported higher levels of perceived stress and depression demonstrated suboptimal treatment adherence to ART. In contrast, those with lower levels of perceived stress and depression exhibited optimal ART adherence. These findings support existing evidence indicating that BMWH who experience various forms of stress face negative impacts on their maternal well-being, parenting responsibilities, and work commitments (Mellins et al., 2003; Penniman, 2009). The findings also support evidence that depression adversely impacts ART adherence and, subsequently, viral non-suppression (Crockett et al., 2020). While psychosocial factors may individually adversely affect ART adherence, the compounded presence of multiple stressors, as described by Mellins et al. (2003), can significantly threaten the well-being of BMWH. Future interventions aimed at improving adherence should address outcomes across multiple systems to effectively support BMWH in managing these intersecting challenges and prioritize maternal mental health supportive services. In addition to the findings on depression and perceived stress by adherence status, 64% of the study sample self-reported having a mental health diagnosis. This tells us that BMWH are discussing and seeking mental health care from providers. Existing research has demonstrated that the confluence of a mental health diagnosis, negative stressful life events, and caregiver burden are associated with suboptimal adherence among BMWH (Mellins et al., 2003). In addition, extant research suggests mental health diagnoses among Black women living with HIV can be attributed to past trauma, such as childhood physical/sexual abuse, and adult physical/sexual assault (Travaglini et al., 2018). Although this study did not find evidence for it, existing research has demonstrated that structural determinants—such as housing, discrimination, transportation, and economic disparities—affect ART adherence among BMWH (Caiola et al., 2018). Therefore, structural determinants should be considered when developing strategies to improve treatment adherence and address maternal distress.
This study enhances our understanding of the psychosocial factors affecting Black mothers living with HIV in the twenty-first century. Research on BMWH has mainly been concentrated in the late 1990s and early 2000s, with limited studies conducted in the past five years. However, recent work by Black women HIV prevention and treatment researchers has increasingly focused on viral suppression within this population. Additionally, social work literature on Black mothers remains sparse and is often limited to negative portrayals of Black women's experiences with motherhood (Corley et al., 2022).
Another unique contribution of this study is its addition to the HIV resilience literature, specifically focusing on Black mothers. While researchers have previously utilized resilience scales (Connor & Davidson, 2003), this study is distinct in that it employs a scale explicitly developed for populations living with HIV and specifically normed for individuals of African ancestry. Lastly, our study uniquely captures parenting distress among BMWH by using quantitative data to measure parenting worry and parenting-related stressors. This is significant because Black mothers frequently place their children's health above their own because Black women center family ties, motherhood, and nurturance. Standardized mental health screenings that do not specifically address parenting-related stressors may overlook these critical issues, potentially neglecting a prioritized domain of social functioning for mothers and failing to provide the comprehensive support they need. The experience of mothering is a critical yet often overlooked factor in the treatment adherence process. For BMWH, caregiving duties may also include navigating the emotional and practical challenges of raising children while coping with HIV-related health issues. These overlapping responsibilities can lead to feelings of guilt, isolation, and burnout, which negatively impact their ability to engage in self-care, including adherence to ART. As such, healthcare providers may be hyper focused or fixated on the slow success with treatment adherence, but not attentive to the strengths of their caregiving and the selfless acts of mothering. Although this study did not find statistically significant associations between structural factors and ART adherence, the distribution of sociodemographic characteristics offers valuable insights into how structural factors—such as employment status, income level, education level, and housing stability, and the inequitable distribution of resources—can influence ART adherence. This could easily be interpreted as resource and economic inequality, within the larger scope of systemic oppression and structural discrimination. In order to combat suboptimal treatment adherence and truly eradicate new cases of HIV among this population, intervention development must center Black women and their families as experts of their own lives, acknowledging their resilience and privileged perspectives, while decentering traditional ways of knowing and hierarchical social order and power statuses.
Limitations
While the findings enhance our understanding of psychosocial determinants of ART adherence among BMWH, there are limitations to this study. The adherence level cut point for this population was set at 85%, based on the mean score for the sample. However, recent research suggests that individuals with treatment adherence rates as low as 70% can still achieve viral suppression, depending on their specific medication regimen (Byrd et al., 2019). Furthermore, the ART adherence measure used in this study is based on self-report, which may result in inflated adherence rates. Despite this, significant associations were observed, suggesting that using a lower adherence cut-off would likely still yield meaningful results. The advantage of a self-report measure is that it allows participants to assess their own progress and actively engage in their HIV self-management. Additionally, it eliminates the need for access to medical records or blood samples to determine CD4 counts and viral loads, focusing instead on the behavior of medication management. This approach aligns with a more patient-centered perspective. The study utilized a convenience sample with a small sample size, which impacts the generalizability of the findings to the broader population of BMWH and limits the replicability of the results. Additionally, the sample was predominantly comprised of older, insured, and stably housed BMWH, which further constrains the generalizability of the findings. Future research should focus on recruiting a more diverse group of BMWH, including those who are younger, uninsured or underinsured, and experiencing housing insecurity. Such studies could provide valuable insights into the comprehensive programming and interventions needed to address the diverse needs of BMWH.
Implications
Undoubtedly, many of the challenges imposed on BMWH cannot be resolved solely at the individual level. Therefore, multi-level interventions are necessary to address these needs comprehensively. Specifically, in relation to safety, freedom from discrimination, and marginalization, there is a need to enhance awareness of HIV Pre-Exposure Prophylaxis (PrEP) and promote HIV prevention and treatment from a status-neutral perspective. A status-neutral approach includes engaging all individuals, regardless of their HIV status, in prevention efforts and ensuring that those living with HIV are actively involved in treatment and care (Myers et al., 2018). Another example of such an intervention could be an evidence-based home visiting program tailored to address the specific needs of BMWH.
In addition to the development of biobehavioral prevention interventions to improve suboptimal ART adherence among BMWH, collective efforts must adopt policy changes that govern the ways in which institutions respond to the needs of this group, which includes advocating for social welfare policies that are HIV specific. For instance, supporting policies like the Ryan White HIV/AIDS Program Core Medical Services Waiver Policy could help reduce economic disparities by easing the financial challenges faced by Black mothers. This policy would allow Ryan White HIV/AIDS Program (RWHAP) recipients to allocate 75% of service funds toward support services related to medical outcomes, up from the current 25% limit (HRSA, 2020). Many of these support services tackle psychosocial and structural barriers to ART adherence, particularly for those living with HIV who live in resource restricted homes or communities.
Conclusion
Sub-optimal treatment adherence among BMWH can be attributed to experiencing multiple simultaneous stressors, which are exacerbated by gendered anti-Black racism, structural oppression and discrimination, and other explicit socially created and upheld inequalities. HIV-related resilience can be a protective factor for optimal ART treatment adherence. Providing BMWH with social, supportive services, inclusive of mental health support in conjunction with HIV care, can help shift the landscape. The integration of family support services must be prioritized to retain BMWH in HIV care. Thus, intervention development should emphasize a multi-level, multisystem, parent- and family-centered approach to ART treatment adherence. Understanding ART adherence among BMWH is critical for advancing biobehavioral research among this population, specifically to reduce gendered-racial HIV disparities this decade.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Society of Family Planning, (grant number Emerging Scholar in Family Planning).