
Abstract
Women living with HIV in Sub-Saharan Africa struggle for health equity while also facing the constraints of economic hardship and patriarchy. In this article, we describe the experiences of women who participated in economic empowerment groups for women living with HIV in Wakiso district, Uganda. Fifty women engaged in economic empowerment groups and ten social worker and community health worker key informants enrolled in the study. Taking a phenomenological approach, we used field notes, qualitative interviews, and focus groups with participants and key informants to describe the experiences of the women who joined the groups. We present the findings including enhanced management of HIV and increased property and business ownership due to economic empowerment group participation. We discuss the findings through an economic empowerment framework and offer implications for social work interventions and research.
Globally, new HIV infections have been decreasing since approximately 2009 (UNAIDS, 2020). HIV-related deaths have also been decreasing since 2004 thanks to improvements and access to Antiretroviral Therapy (ART) (UNAIDS, 2020). Despite these gains, countries in the Global South have struggled to contain the pandemic, and women have experienced much of the burden. Among women and girls of reproductive age, HIV/AIDS is the leading cause of death globally. According to a 2020 UNAIDS report, women and girls in sub-Saharan Africa are much more likely to be infected with HIV than men, accounting for 59% of new infections in the area. Though some improvement in the HIV/AIDS pandemic effect on women in Uganda has been made, the disease continues to punish women there disproportionately. A study conducted by the Ministry of Health (MOH) found that 7.5% of women in the country are living with HIV compared to 4.3% of men (Uganda Ministry of Health, 2017).
Researchers have noted that gender-related health disparities in HIV outcomes could be related to economic inequality. A study based on the experiences of women living with HIV from 17 countries, found that women had less access to financial resources than men, leading to barriers to their engagement in HIV care. Those barriers include practical difficulties such as getting to clinics to receive treatment, paying for childcare, and paying for medicines. Women in a study published by the International Center for Research on Women (ICRW) frequently cited being fired from their jobs due to discrimination stemming from the stigma of their HIV status, which made it difficult to afford the costs associated with accessing and staying on treatment (Golla et al., 2018).
The intersections of sexual health and gender compound the experience of poverty for women in many parts of the world. In their comparison between HIV and COVID-19 pandemics, Along and Blackstock (2023) have called for health justice to mitigate these effects on the most vulnerable. They explain that systems of oppression like racism and homophobia cause inequities in health, and that the solution is to redistribute power and resources to the most affected to improve health outcomes. Those resources can include financial security, political power, and access to care. The oppression experienced by women living with HIV requires a health justice approach if health equity is to be achieved.
In addition to HIV stigma and health disparities, women in Sub-Saharan Africa face unique economic hardships. Many women provide home-based care for low wages, reducing their earning capacity and placing unrealistic demands on their resources, thereby increasing their economic vulnerability. Due to gender role stratification frequent in these patriarchal communities, women are often responsible for family food and housing budgets, but typically have limited time to work or may receive low wages leading to them to depend on men for Kameeza-a traditional maintenance/allowance fee from a husband. Kim and others (2007) refer to the HIV pandemic as a disease of inequality often associated with economic and gender disparities that negatively impact health including HIV and Interpersonal Violence (IPV) risk. Given their economic and social vulnerabilities, the women living with HIV in Sub-Saharan Africa are significantly overstressed (Tanzarn & Bishop-Sambrook, 2003).
HIV disproportionately affects women across the global South due to their vulnerability stemming from their unequal cultural, social, and economic status. Inequitable laws, harmful traditional practices and unequal power dynamics between men and women disadvantage women (UNAIDS, 2017). The HIV pandemic is not only driven by gender inequality, but is also entrenched in economic inequality, leaving women more vulnerable to its impacts (UNAIDS, 2020). Ugandan societies are patriarchal, which limits the ability of women to be in control of decisions related to the physical and financial resources of the family. For instance, in Uganda, women need the consent of a male partner to access sexual health and reproductive services, positioning them to be less in control of their sexual health decision making (UNAIDS, 2019), and the resulting outcomes. In addition, they experience many types of interconnected social and economic barriers such as accessing funds for transportation to clinics, high-cost childcare and education fees and unpaid labor demands. In a study that examined data from the 2016 Uganda Demographic Health Survey, researchers found that socio-economic and cultural factors led to malnourishment in women of reproductive age in Uganda citing poverty and regional inequalities as determinants of poor health (Sserwanja et al., 2020).
The property rights of women are a barrier that affects their socio-economic status and consequently their health and wellness. Although women have statutory legal rights to own property due to changes in the Uganda National Land Policy outlawing discrimination, the customary laws of Uganda can supersede statutory laws, making this difficult to enforce (IGAD, 2021). The result is that despite having official rights to own land, women in Uganda have been reported to own only approximately 7% of the land. This is a stark contrast to the labor that women contribute to the food supply in the county, which is estimated to be 80%. The ownership vs labor share discrepancy is due to customary laws and marriage practices that make it unlikely for women in Uganda to inherit land from a spouse. The practice of polygamy and couples commonly engaging in domestic partnerships rather than formal marriages recognized by the government are contributing factors to land ownership inequality. According to the Uganda Association of Women Lawyers, women can only inherit 15% of land upon the death of a spouse or father, and in the case of plural marriages, all the wives share that 15%. Those in domestic partnerships (not marriage recognized by the Uganda government) cannot inherit land upon the death of a spouse (IGAD, 2021).
One area of Uganda that has been heavily impacted by the HIV pandemic is the Wakiso district. According to a 2017 population and housing census report, Wakiso district had a total number of 2,128,142 households of which 40% were female-headed (UBOS, 2018). The ability of those affected by HIV to provide for their families’ needs was limited by their physical and social capacity to meet them (Namara-Wamanga et al., 2013). The district has one of the highest prevalence rates of HIV in Uganda (9.9%) compared to the regional prevalence of 8.5% (Uganda Ministry of Health, 2017). The higher prevalence is attributed to the peri-urban nature of the district, where the environmental and behavioral factors increase vulnerability of individuals to high-risk sexual health practices (Namara-Wamanga et al., 2013). Some environmental factors that increase sexual health risk include the lacking or inadequate infrastructure that makes accessing healthcare facilities difficult. The growing community suffers from poor road and bridge conditions, lack of clean water sources, and deferred maintenance in healthcare facilities. Shortages in healthcare staff and essential medications also act as barriers to adequate healthcare including difficulty accessing HIV medications. Medically supervised births in facilities are rare even when medically necessary. The child death and infant mortality rates are above the national average at 94/1000 vs 76/1000 respectively (Namara-Wamanga et al., 2013). To put this rate in perspective, the Centers for Disease Control and Prevention reports the U.S. infant mortality rate in 2020 was 5.4/1000 (CDC, 2023).
Factors that affect women's HIV health and overall wellness outcomes are often related to behavioral practices routed in patriarchal beliefs about property and finances. In Wakiso, women who become heads of households upon the death of their spouses, on whom they have traditionally been forced to depend, are also in danger of losing ownership of their land and assets when a male partner dies of AIDS. The Uganda Bureau of Statistics explains that a deceased spouse's family members can use patriarchal cultural beliefs and laws that allow male relatives to strip widows of their financial assets, rendering them more vulnerable to economic hardship and HIV wellness barriers (UBOS, 2018).
The dynamics of the local fishing communities in the area have contributed to high HIV risk due to the seasonal nature of the work. The risk factors include commercial sex trade and inadequate access to sexual and reproductive healthcare facilities specializing in preventing and treating HIV due to the distance between treatment sites and commercial fishing areas (Kwagonza et al., 2020). In a survey about comprehensive knowledge of HIV prevention, fishermen in rural areas that were isolated from healthcare facilities reported lower rates of knowledge. This lower knowledge contributes to higher risk behaviors that make women partners and sex workers more vulnerable to being infected and undertreated for HIV (Kwagonza et al., 2020).
Studies show that women living with HIV tend to be vulnerable to poverty and lack the economic access needed to sustain their livelihoods (Kabeer, 2012 & Najjuma, 2015). Evidence suggests that economic empowerment strategies may contribute to some improvements in the wellbeing of women (Dworkin & Blankeship, 2009; Krenz, Gilbert & Mandayam, 2014). The resources, assets, skills, and social connections forged out of economic empowerment interventions can help to improve resilience – the ability to recover from the effects of HIV (Loevinsohn & Gillespie, 2003), and improve wellbeing. While there is much literature on the connection between HIV and economics, the existing research is largely limited to examining microcredit through external interventions. External interventions include things like grants and funding paid to recipients or agencies that do not include internal participation in planning and organization with recipients/participants. Some have criticized the concept of economic empowerment as a means of supporting economic growth through capitalist endeavors that both ignore the socio-political context of women in poverty and benefit them in limited ways (Schech & Vas Dev, 2007). This external focus limits opportunities for inclusion from those who will understand how to best benefit from the programs and funding – the women themselves (Barnes et al., 2003; Beck, 2017; Goetz & Gupta, 1996; Kabeer et al., 2012; Longuet et al., 2009; Neumayer & Soysa, 2010). Little research has concentrated on the economic empowerment of women living with HIV themselves as agents of change. Hence, a deeper understanding is needed about the role that economic strategies among women living with HIV may play as part of the solution to HIV health disparities in Uganda.
Conceptual Framework
This phenomenological study of participants’ experiences in savings and loaning groups for women living with HIV draws inspiration from an economic empowerment framework. Feminists advocate for gender equality, and economic empowerment has been described as a “direct path towards gender equality, poverty eradication and inclusive growth” for women in Southern African regions (UNWomen, 2022). The World Bank has been concerned with ending poverty through economic empowerment programs for vulnerable women but has been limited to capitalist viewpoints that focus on market access only with little regard for addressing the inequalities of women or the freedom of their occupational choices (Schech & Vas Dev, 2007). Some factors affecting women's economic inequality in Uganda include gendered care and domestic labor norms resulting in women's unpaid labor. Farm labor is a topic of interest in economic development for women because farm labor has been traditionally considered part of domestic labor in the region. Domestic labor though largely unpaid has contributed to the economy for the predominant benefit of the male relatives of women, resulting in income and wealth inequality. Economic empowerment initiatives focus on changing both the cultural norms and policies relating to labor practices to improve the economic well-being of women through educational and financial interventions.
There are a variety of ways in which gender inequality affects women living with HIV in Uganda specifically, and they include denial of inheritance and property rights, social exclusion, stigma, shame, economic inequality, unemployment, and underemployment (Najjuma, 2015). However, economic and health risks can be mitigated to improve HIV risk and health outcomes for women in the context of economic distress and scarcity. Economic empowerment programs improve the lives of women by encouraging them to improve their financial and consequently their social status (Jennings, Ssewamala & Nabunya, 2016).
Women's economic empowerment can be defined as “the ability to succeed and advance economically and the power to make and act on economic decisions” (Golla et al., 2018, p. 4). The gender-related aspects of economic empowerment stem from patriarchal beliefs about women's place in the broader community and therefore the market. Their visibility in the community and in financial transactions are directly tied their personal and economic power affecting their ability to make decisions about money or participate in business transactions. Kabeer (1999) further defines economic empowerment as the ability to make strategic choices where that ability did not previously exist. They suggest that resources and agency, in addition to achievements, are the outcomes of the empowerment process. Kabeer (1999) further asserts that economic empowerment is the process by which those who have been denied the ability to make strategic life choices acquire such ability. It is a process that entails not only what people do with the acquired ability, but also how they make choices to influence or enhance their own lives and those of others as well as how one can tell when this ability has been acquired. Others have defined economic empowerment as the ability to make and act on decisions that involve the control over and allocation of financial resources (Golla et al., 2018; Zoynul & Fahmida, 2013). The foundation of creating a life with opportunities includes the ability to freely choose one's path in life in accordance with one's distinctive talents and abilities.
The notion of agency is essential in the empowerment process. The term ‘agent’ is employed in this study to denote someone who acts and brings about change. We agree with Sen that a person can improve her overall wellbeing through her personal capabilities and vision but only within the context of her environmental restrictions. The opposite of a person with agency is someone who is forced, oppressed, or passive (Sen, 1999). This agency, in the context of the removal of oppression and restriction, can expand the horizons of concern beyond a person's own well-being to include concerns such as solidarity with others in mutual saving through a collective mindset.
According to policy research funded by the World Bank Group, agency is the capacity to make decisions about one's own life and act on them to achieve a desirable outcome, free of violence, retribution, or fear (Fox & Romero, 2017). This promotes gender equality (Sen, 2005) in all economic domains and interactions, and encourages participation in other forms of collective action (Fox & Romero, 2017). Collective agency thus emphasizes that individuals are seen as agents in the construction of social change to improve their wellbeing and the wellbeing of others. This is a departure from an individual, narrow perspective, which had limited women's empowerment to influence over household expenditures only (Fox & Romero, 2017). While the spaces for agency vary, economic empowerment envisages women's voices and participation in processes that improve livelihoods and mitigate adverse effects of gender-based economic inequality, including poor health outcomes for women living with HIV and their communities.
Women living with HIV who are economically empowered can increase resilience and position their agency to enhance their well-being and manage adversities caused by the disease. Access to financial resources is critical for creating a strong base of social and economic resiliency and contributes to enhanced quality of life (Negash, 2006). The resources resulting from economic empowerment efforts may help to improve the resilience of women living with HIV to improve their health status by reducing their dependence on male relatives to access healthcare services. Those resources include ownership of land, equipment, livestock, and other business assets as well as access to services like childcare, transportation and education for themselves and their children. Women with the means to conduct and profit from business enterprises are freer to attend to their preventative sexual and reproductive health (preventing pregnancies, promoting safe childbirth, preventing HIV and other sexually transmitted diseases) by accessing clinic visits, but also by avoiding sex work as a means of economic stability.
Economic empowerment has been applied to social work interventions aimed at improving the well-being of women in previous studies. A study conducted in Western Australia utilized financial literacy education as a means of empowering domestic and family violence victims in a refugee camp and found that the physical health symptoms related to financial worry of the women were improved (Warren et al., 2019). In a longitudinal study of an economic empowerment intervention for adolescents in Uganda, researchers noted improvements in ART update, financial status, and school enrolment as a result of mentorship, business education and savings matching.
Economic distress and scarcity faced by women living with HIV are overarching factors that make them vulnerable to stress and trauma. Economic empowerment promotes an adaptive response among women living with HIV to survive as well as thrive after diagnosis. An economic empowerment framework addresses the unique financial issues faced by women living with HIV in Uganda by increasing their financial capacity and therefore reducing gender-based oppression steeped in patriarchal power imbalances. The notion that thriving with a disease that is associated with stigma and health disparities could be accomplished through financial rather than purely psychological means inspired us to explore the experiences of how participation in community saving and loaning groups affected women participants in Uganda. Our specific research question was “What are the experiences of women living with HIV who participated in economic empowerment groups?”
Methods
This study was carried out between 2018 and 2020 in the Wakiso district of Uganda. We employed a phenomenological approach including focus groups, individual participant interviews, key informant interviews and field observations (Creswell, 2007). Our goal was to describe the experiences of women who were engaged in economic empowerment activities aimed at mitigating the financial effects of living with HIV. The choice of Wakiso was strategically based on its geographic positioning. Specifically, it triples as an urban, peri-urban and rural location, which allowed the researchers to report findings from these three different types of settings. Wakiso district health office trains Village Health Teams and community social workers to engage people living with HIV to improve care access and provide HIV health information (Namara-Wamanga et al., 2013).
Ethical Considerations
The study was approved by the Mildmay Uganda Research and Ethics Committee at Mildmay Hospital Research Centre (Approval-Rec Ref: 0901-2021). The Centre “generates evidence to influence healthcare policy and practice in Uganda and sub-Saharan Africa (Mildmay Hospital, 2023). All the participants gave their informed consent to participate in the study. Pseudonyms were used to protect the women's anonymity and were applied to all transcriptions and photographs. To ensure privacy, photographs do not contain images of the participants. Due to COVID-19, researchers and study participants practiced social distancing, sanitizing, and wearing of masks during data collection.
About the Researchers
The lead author and Primary Investigator Dr. Saidah Mbooge Najjuma is a Senior Lecturer at the Faculty of Social Sciences at Ndejje University in Uganda. She was a visiting 2021 Fulbright scholar at University of North Carolina Wilmington where she started working with Dr. Helen T. Yates, a faculty member at the School of Social Work there.
Dr. Najuma designed, planned and secured funding for the study to achieve its objectives. She provided documents related to ethical committee approval and signed consent statements. She generated the data, conducted the literature review, collected the data and assumes responsibility of what is published. She wrote the manuscript draft and participated in analysis and editing the manuscript. She also assisted the corresponding author with reviewers’ queries when the paper was under revision. Dr Yates helped write the discussion section and made revisions to previously written sections, helped analyze the findings and searched for additional background and discussion articles. She also handled correspondence with the journal.
Economic Empowerment Groups
The groups in the study were formed by the members with guidance about financial literacy and HIV care management provided by social workers and community health workers from Village Health Teams. The groups were self-formed and self-managed, meaning they pooled their own funds and created their own rules for contributions and borrowing. Group members were given basic supplies and some guidance on where to apply for outside loans to pay for membership fees if they did not have funds to join. Participants collaborated to address the areas of economic vulnerability they wanted to address establishing the goals and procedures of their unique group. Self-governance of the groups allowed the women to engage in financial initiatives that best fit their community and personal circumstances. The choice of how to improve their economic circumstances increased their power amidst the challenges caused by living with HIV in a patriarchal society that has historically restricted their access to healthcare and financial decision making as well as their resources. Local women became group leaders and helped in recruiting group members and organizing meetings. More details about the groups’ operations are supplied in the findings section of this article.
The study participants were invited through their team leaders: 10 belonging to Alwala siyaafa savings group, 10 belonging to Ssosolye bwatafa atuuka kulyengedde, eight belonging to Tulibumu vision group, 10 belonging to Bakyala twezimbe savings group and 12 belonging to Nezikokolima gaali magi. The groups were in four of eight constituencies in Wakiso district of Uganda. In addition, individual interviews were conducted with ten key informant social workers including three HIV service linkage facilitators, three community counselors, one health trainer and three supervisors at HIV support units that were visited for the study.
Data Collection
We used three data collection methods to help understand the experiences of economic empowerment of women living with HIV in the district. The primary data was gathered in five focus group discussions with women participating in economic empowerment groups. All interviews were audio recorded and transcribed with permission from the participants. Multiple field visits in participants’ homes were carried out by the primary investigator to collect photographs and conduct individual interviews. Interviews were conducted in both English and Luganda based on the participant's choice of language to increase comfort and participation among the participants. After the focus groups, home and site visits, the recordings were transcribed and translated to English by the primary investigator for analysis and reporting.
The primary investigator was the only data collector. Inclusion criteria included identifying as a woman 18 years or older and participating in one of the economic empowerment groups as either a participant or team leader. No exclusion criteria were indicated. During the field visits, digital data in the form of photographs and detailed field notes were captured based on guidance from the participants, and this data was analysed along with the focus group transcripts.
Analysis
The first author analyzed the data using Content Analysis by identifying patterns, themes, and quotes from individual and group responses, which began concurrently during data collection (Creswell, 2007). Patterns in the data were initially noted by the primary investigator and then categorized and organized to give meaning to the collected data and create themes to describe the participants’ experiences. These themes were later discussed between the researchers until consensus was reached for clarification. The first author was able to provide clarification to help reach consensus around the themes that emerged from the data due to their involvement in the project from conception to data collection through analysis. Participants were consulted about their interpretation of the meanings and themes resulting from the quotes and photos by the primary investigator during initial data collection and again later using follow-up visits to improve the credibility of the findings.
Findings
The findings of this study describe the experiences of women living with HIV who were engaged in economic empowerment groups. We present themes, listed in Table 1, which are enriched with direct quotes from the participants and field photos. These themes illustrate the experiences of participating in economic empowerment groups. They center around social inclusion, financial literacy, HIV health resiliency, stigma reduction, and gender justice. Considering the challenges of patriarchy and living with HIV, the participants faced adversities such as stigma, fear, gender inequality, shame, and hopelessness, (Najjuma, 2015). Those adversities are difficult to overcome in the context of economic scarcity. However, the women described how they improved their economic positions to mitigate the adverse effects of living with HIV. This reflects the resilience and agency among the women whose voices are represented by these findings.
The Experiences in Saving and Loaning Groups for Women Living with HIV in Uganda.
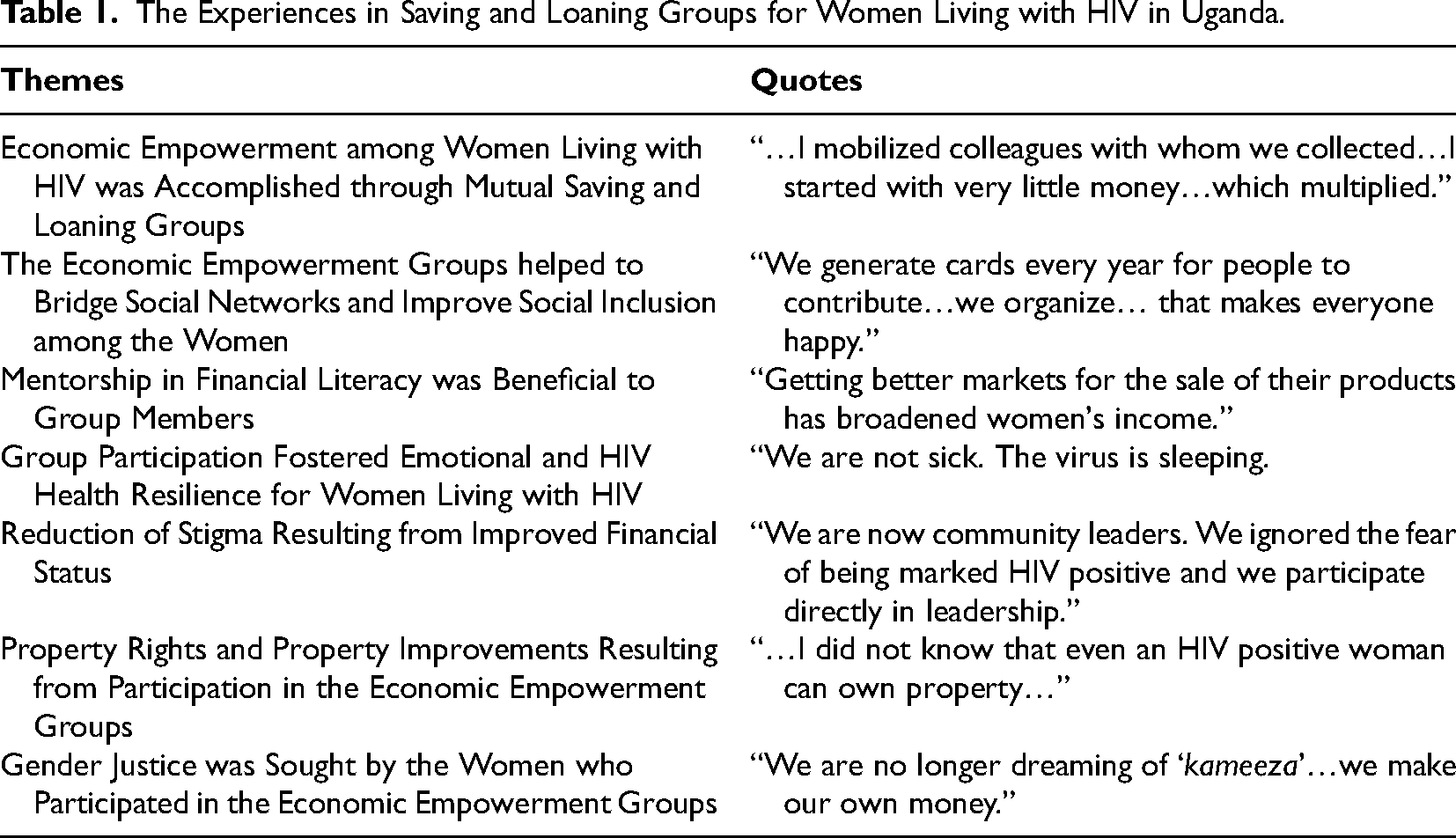
Economic Empowerment among Women Living with HIV Was Accomplished Through Mutual Saving and Loaning Groups
The women who participated in the study described navigating the economic constraints of living with HIV by mobilizing financial resources through mutual saving and loaning groups with other women. They described organizing themselves into groups to increase mutual savings with the opportunity to borrow from the group as needed. They paid a membership fee to join the group, which formed the initial source of capital. The members established their own rules for borrowing and received assistance in financial planning and HIV management from social workers and community health workers. The members continued to contribute to the group funds until an agreed upon date when they were shared between members. They invested in businesses, education, and property to improve their wellbeing. Women got small loans from their groups in the form of capital illustrated by a photo of a bag of money, which they could use to personally invest in their small businesses and agricultural resources to gain financial independence.

Social fund and savings bags used by participants.
General savings and loaning rules were established by each group collectively and are described by some of the women who participated in the groups, including savings requirements, and vetting of loan applicants. Some women also described specific funds. “In addition, they save for social fund commonly known to them as ‘Munno mukabi’…It is only accessed upon a member presenting a challenge to a group, such as, when a member loses a child, mother, father, or spouse.” Some of the special funds were used for education of children, including this description: “Also for Education fund – Members who pay fees for their children can save money and borrow for education purposes.”
The women in the study appreciated the absence of a requirement of collateral to access the loans, which enabled them to have quick access to funds saved by other group members. One participant commented: “We borrow the money from the group, depending on the need of each individual. We do not pay a lot of interest when we return the money.”
The Economic Empowerment Groups Helped to Bridge Social Networks and Improve Social Inclusion among the Women
Because women participated in the savings and loaning groups, they could bridge their networks and expand their experience through social workers who connected them to other groups in the district. Social workers organized visits between groups in which they invited women living with HIV to socialize together. These interactions equipped the women with new ideas to improve their savings and loaning projects: Through cross visits, it is easier to master how others do work by seeing, touching, and talking with another woman about their projects and get insights on how they gather the energy to do incredible work in a state of being HIV positive.
Valuable resources embedded in the social networks of the women were important for improving the economic positions of the women in the study. The participants expanded business ideas by establishing mutual group projects, such as purchasing goods for catering community functions from which they shared the profits. Some women formed drama groups and were paid to perform at community events. These shared profits benefitted the individual women, their families, and their communities. One woman informed researchers that “Our motto is fight poverty times four.” Another woman indicated, “We generate cards every year for people to contribute…we organize… that makes everyone happy.” Collective projects also worked as channels to increase the scope of individual women's economic empowerment. Referring to how the group members can increase the visibility of their projects through social and program connections to increase revenue, a social worker key informant added “We use some of the initiatives of women living with HIV as demonstration projects…which attracts user fees for them.”
Mentorship in Financial Literacy Was Beneficial to Group Members
Social workers from non-profit and government agencies sometimes took on roles to educate the women in the savings and loaning groups around financial literacy. They trained the women in financial skills that allowed them to make informed decisions about managing finances, saving, budgeting, and investing the resources they mobilized. The women who participated in the groups reported that such training was crucial.

Safety box used by saving and loaning groups.
Some participants established workspaces near their homes to start small businesses, which was convenient for them. (Figure 3: We introduce to the women business selection, planning, and management skills, and let them understand the process of business startup, management, and monitoring. We analyze the environment where women would want to establish their businesses. Some of the factors to consider are availability of market, transport accessibility, nature of customers and government policies relating to taxation of business, among others. They can identify which ventures they can consider in starting up a business.

Village market in front of a participant's homestead.

Crafts made by participants to sell to foreign markets.
We have better markets for the products and more income from baskets, because those who train us in craft and knitting work linked us to foreign ‘white markets’ where we have been able to earn better from our sales compared to local markets.
The link to external markets in the U.S. and Europe was another opportunity accessed by the participants, as emphasized by a key informant who stated, “Getting better markets for the sale of their products has broadened women's income.”
Group Participation Fostered Emotional and HIV Health Resilience for Women Living with HIV
In addition to financial skills, the women who participated in the groups reported increased resiliency that enhanced their ability to manage issues such as marginalization and mental health related to their HIV health status. Group participation increased positive mindsets among the women, allowing them to focus on their futures with a sense of hope. One woman shared her experience stating: At first, I thought that I was going to die soon. By getting involved in saving, my mind towards life changed completely. I am able to sustain my livelihood. I have lived to see one Christmas after another, and I have been able to sit with my grandchildren. I feel emotionally stable.
Participating in the mutual savings groups helped the women act as agents of transformation for themselves and their families. Some participants reported that their health and financial condition had greatly improved. “I can help my children in which ever they need…stigma is now history on my side. I have the knowledge and plans about utilization of my money, when I get it. I feed well; I have improved our house to make it look a better homestead.” Another woman stated how managing her health was important to her; “We take good care of our lives and our projects…We have to treat any illnesses that come our way for us to be happy. It's the same way I care for my cow. It gives me wealth. I handle it with love.”
Reduction of Stigma Resulting from Improved Financial Status
The increased economic power of the women who participated in the saving and loaning groups resulted in their improved self-worth and inclusion in the community. One woman mentioned “We are now community leaders. We ignored the fear of being marked HIV positive and we participate directly in leadership.” Through improved financial capabilities, the women also commented on their ability to support the livelihoods of others in their communities. “I am a Peer Mother. I volunteer at the Antiretroviral Therapy (ART) clinic and carry out field visits to support and identify other women living with HIV.” Using a common Ghanaian proverb, a woman in one group commented; “Awaba omulwadde tewabulawo mulamu - where there is a sick person, there will be a healthy person.” They maintained that; “It is us who are healthy who help others. That is why we do what rewards us in the different ways.”
Economic improvements among the women in the study had a positive effect on other aspects of wellbeing including amplifying their voices as confident leaders in the community. One woman remarked that; ‘People know me and usually invite me as chief guest on special occasions…Even you (referring to researcher), you called me when you wanted to meet the women.” Referring to the Ugandan folklore heroine, she continues “I am Nambi, and I am the council chairperson of my village.” The social workers in the study discussed how they learned to best provide not only economic but also emotional support to the vulnerable women in the groups. A supervisor at an HIV support unit key informant noted: There are many lessons we have learned from approaching the women living with and affected by HIV in Wakiso, with socio-economic support, among other populations. Women living with HIV in particular, derive significant benefits from socio-economic support activities, including increased income, personal empowerment, improved quality of life, and increased social acceptance.
Property Rights and Property Improvements Resulting from Participation in the Economic Empowerment Groups
Another important outcome of the economic empowerment interventions experienced by the women living with HIV in this study entailed increasing rights to and ownership of property. Several women in the study reported using the monies accumulated from group savings to buy land, rehabilitate, and improve their homes, or construct new homes. One participant shared proudly “I built a house with three rooms.” Another woman stated “For me, I bought building materials one at each time I got the money, and I started construction. My house is nearly complete.” Some women used funds for small business ventures resulting in improved access to land and property. One participant explained she “renovated two houses for rentals. I am continuing to save the money, so I am now able to buy land on which to construct a house.” Other women said, “I made mud bricks on my land that I sold and made thousands of money,” and “I bought a plot of land and planted miraa, which I sold, and roofed a family house.” One participant indicated that she purchased her land with a title deed, and she boasted: I was hopeless. I did not know that even an HIV positive woman can own property…I did not know that a landlord can negotiate with me…over his land, and I stand upright to buy a plot of land. Aha!
Despite the increased property access resulting from the economic prosperity of many of the participants in the study, some continued to face gender-based oppression due to patriarchal social structures in the community. For example, one woman reported that she gave her husband all the money she had collected over time, who then traveled to the village to buy livestock, but did not return with the intended purchase. Another woman explained how she had to make efforts to protect her investments from her children due to laws and cultural norms that would allow her male heirs to take ownership of her assets: I have established small-scale businesses in the form of animal rearing: goats, cows, sheep, and local chicken among others. I have erected a structure for rental and have bought land for growing food items. I make sure I keep records and share them with my children. There is the property that is owned as a family, and I also have personal property and my children know it.
Gender Justice Was Sought by the Women Who Participated in the Economic Empowerment Groups
In addition to financial literacy initiatives, the women in the study also received support to promote their self-worth, self-appreciation, and to utilize their capabilities and intellect to improve their economic position. These initiatives were useful in the women's efforts to counter the patriarchal situations that threatened their well-being and economic security. For instance, some women chose not to remarry after the death of a male partner due to HIV disease progression to AIDS. They chose to focus on themselves to increase their funds and improve or maintain their HIV health. They indicated that taking on another male partner might threaten their economic security. One woman mentioned “The men are only there to ‘lift’ women's money…he pockets it and goes to drink. I got tired.” The participants in the study set positive examples in their communities by pursuing economic security and independence.
Several women referred to how mutual savings groups allowed them to improve the educational disparities experienced by their children, which was important for increasing access for girls. One woman noted “I get my children's fees from the group's education fund, and this is why my children never lack school fees.” She continued “We raise money from our projects for household needs… buy children's books.” Another woman shared; “After getting bedridden for a long period and I was able to recover, I had lost everything. I will forever thank one [woman] who invited me to save…where I draw money to invest in my children's education.” This was an important factor for women's progress toward gender equality, since Uganda's political climate promotes privately funded education and childcare, which results in economic and gender disparities.
Some women reported utilizing a male partner's financial support when they required it, but not feeling dependent upon it. “I am not around to beg a husband all the time, but he comes in to support where I need help.” Others remarked how they felt satisfied by not having to rely on the traditional Kameeza or maintenance/allowance fee from a husband, which was oppressive to them before their economic empowerment gains. “We are no longer dreaming of ‘kameeza’…we make our own money.” “We are self-managing… we are contributing to family development.” Economic empowerment was an important factor in addressing gender stratification both at the household and community levels. A key informant added: …being economically empowered, women have a more complementary role in both the household and the community, especially on children's scholastic materials, and women never wait for their husbands. Even when the husband does not buy soap and salt, women can buy it, because they have friends from whom they make the resources. The days when Vaseline and other minor household necessities used to generate home quarrels are gone.
Discussion
This study aimed to provide a rich and descriptive understanding of the experiences of women in the Wakiso district of Uganda who are living with HIV and participating in economic empowerment programs with social workers and other health care workers. To describe their experiences, a qualitative study was conducted utilizing interviews and field observations. Participants’ positive experiences including improved financial independence, social inclusion and HIV health improvements resulting from the economic empowerment processes were described in the findings. The findings were illustrated with direct quotes and images that illustrated the economic empowerment and savings and loaning group participation of the women living with HIV in the study.
These findings are similar to previous studies outlining the efforts of social workers and other community organizations focused on the economic empowerment of women (Beck, 2017; Dworkin & Blankeship, 2009; Jennings et al., 2016). The experience of social, financial and household equality was notably similar to previous studies of economic empowerment groups for women in the Global South, as discussed in a qualitative article about a microfinance intervention in India (Krenz, Gilbert & Mandayam, 2014; Warren et al., 2019). In an article exploring projects aimed at empowering women to improve wellbeing, Beck (2017) suggested we adjust our understanding of women's agency to include the agency women exercise when they engage in empowerment projects themselves.
This article provides new insights into the nature of women-led groups that expand on the agency of members by capitalizing on their unique interests, social connections, and desire to support one another in their communities. This expands on the practice of providing microfinance loans without educational or collaborative components. This matters because gender-based economic oppression thrives on restricting financial power and control of women to maintain the patriarchal status quo. It is necessary to reposition that power in the hands and pockets of women to improve gender equality and subsequent HIV health outcomes for women in vulnerable communities.
The study examined the effect of an economic empowerment intervention conducted by social workers collaboratively with women living with HIV who were struggling economically. The empowerment groups provided training, counseling, financial literacy education, financial assistance and exposure to resources and opportunities that allowed them to earn a decent income, while maintaining control over their choice of work. The freedom of choice and control over work choices has been highlighted as an important aspect of economic empowerment interventions since the World Bank called for them as a means of combatting poverty in the Global South. Some neoliberal models of economic empowerment entice vulnerable women into capitalist traps involving predatory bank loans or low-wage jobs that ultimately benefit multinational corporations (Power, 2020). This was a more collaborative approach where social workers provided support to the women in their own businesses, and also partnered with other social work organizations and extension workers to provide support services to achieve economic stability. This allowed the women to earn a fair income and remove the barriers they faced from the stigma of living with HIV.
In a state of economic scarcity, the women in this study faced a myriad of disadvantages while living with HIV including stigma, hopelessness, limited access to credit, and patriarchal limitations on property and asset ownership. Despite these challenges, they embraced economic empowerment with impressive levels of engagement as a means to overcome the economic, social, and health effects of living with HIV. The participants engaged in saving and loaning in their communities to improve their personal, familial and community financial and social status. They bridged social networks with the support of social workers and other community health workers, who also mentored them in financial literacy, fostered social connections and addressed their health needs (Najjuma, 2016). The groups served to create economic initiatives, foster new projects, and supported their goals of investing in businesses to support themselves and their families. The connection to external valuable markets also boosted women's income. The women in this study leveraged their agency (Sen, 1999), and by improving their economic wellbeing, they increased their individual freedom to make decisions related to the HIV health outcomes.
Researchers have argued that the empowerment process is enhanced by supportive services, including financial education, training, and social support services (Kabeer, Mahmud & Castro, 2012). In our study, savings and loaning groups helped build connections and increased women's capacity to fight HIV at the individual, family, and community levels. The women who participated reported their collective efforts to empower themselves economically as a means of managing adversities due to living with HIV. The efforts made by the women and their social work collaborators can be considered a form of health justice as it reduced the problem of poverty caused by intersecting systems of oppression (sexism, HIV stigma) by redistributing resources including wealth and social status (Along & Blackstock, 2023).
Despite experiencing stigma in their communities, study participants highlighted the importance of seeing themselves as learning to manage a chronic illness rather than identifying as sick. They were highly motivated to participate in economic empowerment because they desired financial independence and the ability to care for their own health and the well-being of family and community members. The increased economic power among the women gave them the confidence to also improve their social status and inclusion. This expanded to election into leadership positions, invitations as motivational speakers, and as chief guests at social events as a result of their improved standing in the community. According to Sen (2005) when wellbeing is enhanced, women can be dynamic promoters of social transformation in their communities.
Findings from this study revealed that despite the economic hardships they experienced, women living with HIV benefited from acquiring financial independence and in turn supported other women's economic empowerment. They used economic empowerment as means of increasing equality, such as acquiring, allocating, and selling assets and improving property and education access (Negash, 2006). Their collective efforts led to success that traditionally had been recognized as male-only domains in their culture.
The women in the study played powerful roles in both the household and the community by exercising their agency to counter the patriarchal hierarchies and gender inequality that women living with HIV in Uganda often face. Poverty and denial of women's inheritance and property rights are major obstacles to victory over the virus of HIV, and the path around these obstacles seems to have been made easier by economic empowerment programs.
Enhanced economic empowerment is a prime factor in reducing gender inequality and central to realizing the rights of women, particularly regarding property ownership (Duflo, 2012; Kabeer, 2012). The positive effects of property ownership for women were evident in the findings of the current study, as in previous studies in developing countries. Enhancing women's economic resources not only contributes to their economic power, but also may reduce male violence against them (UNAIDS, 2021). In their scoping review of 14 countries, Leddy, Weiss & Yam (2019) found that Gender Based Violence impeded women's uptake of HIV prevention and therapeutics, making them more vulnerable to the disease than men. This highlights the importance of supportive and empowering services for women who are vulnerable to HIV by social workers and other community health workers. To know whether economic empowerment services offered by social workers are effective at protecting women from these intersections of vulnerability, we recommend that a quantitative intervention study be conducted as a follow-up to these findings. It will be important for future studies to flesh out whether it is most beneficial to encourage women to seek economic equality through private business ventures within a capitalist framework or if unintended consequences of competition and scarcity will ultimately reduce the gains in gender-based economic equality over time.
Conclusion
The women who participated in this study utilized the tools of economic empowerment to help them overcome adversities due to HIV by utilizing their inherent and collective strengths. While economic empowerment may not guarantee enhanced livelihoods, especially in the face of patriarchy, it was still a vital component of the fight against HIV in the study communities.
This research contributes to the literature by providing a detailed account of women's voices and experiences of economic empowerment, with the potential to inform social workers developing innovative curriculums for economic empowerment, and promoting collaborations with communities that can be generated out of practical women's experiences.
This study centers the power of decision making about the nature of the economic empowerment intervention and desired outcomes with the women themselves. HIV research in Social Work tends to highlight interventions that ignore the economic needs of women that are the result of deeply engrained social inequities. When women are economically oppressed and dependent on the men who infected them with HIV, a solution that reduces poverty in a manner that recenters power is essential. These findings demonstrate that women can gain financial security despite financial distress and oppressive social climates and can contribute to strengthening their communities and sustainable development. Social workers in communities where HIV has caused extreme hardships for women may want to consider augmenting the typical HIV health and social interventions with economic empowerment programs aimed at improving the status of women. More study is needed to determine if the positive feedback from women in Uganda translates to other areas of the world that are similarly affected by the HIV pandemic.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fulbright Visiting Scholar Program, Ndejje University Staff Development Grant, (grant number NA).