
Abstract
Intimate partner violence (IPV) affects millions of individuals across all demographics and ethnicities. Research has revealed a direct link between experiencing IPV and having adverse physical, mental, and financial outcomes which can create difficulties for survivors. Survivors experiencing these adverse outcomes are likely to seek out support to address these issues, increasing the likelihood that they will encounter mental health professionals (MHPs). MHPs can play a significant role in assessing and addressing IPV since they are often critical access points for those experiencing violence and are likely to counsel victims. Accurate identification of current or past IPV victimization is crucial to avoiding the potential of misdiagnosis of survivors. In addition, by applying and emphasizing an understanding of the connection between individual and structural explorations of gender, race, class, and other socially constructed identities, mental health professionals can utilize the skills necessary to challenge inequalities, which in turn can encourage survivors to create strategies that make sense to themselves and their communities. This study explores what is known about how MHPs are prepared to work with IPV. Peer-reviewed journals that were published between 2005 and 2019 were reviewed systematically to develop a better understanding of the existing literature. We sought to answer the question, “What is known about how MHPs are prepared to work with IPV?” This review identified 20 articles regarding training experiences of MHPs and how these experiences shaped their responses to and practice with those experiencing IPV.
Intimate partner violence (IPV) is a widespread and crosscutting public health and social issue affecting more than one in three women in the United States (Fedina et al., 2017) and can be formally defined as “an ongoing pattern of coercive control maintained through physical, psychological, sexual, and/or economic abuse that varies in severity and chronicity” (Warshaw et al., 2013, p. 2). In the United States, one of the most dangerous places for a woman is her own home as reported by a recent United Nations Report (2018). According to research conducted by Everytown for Gun Safety (2019), an average of 52 women are shot and killed by an intimate partner every month. Black women, in particular, are killed by an intimate partner at two and half times the rate of white women (Stockman et al., 2015), and murder rates of Indigenous women are up to 10 times higher than the national average (Bachman et al., 2008).
Multiple studies have revealed that IPV was significantly associated with mental health outcomes including depression, posttraumatic stress disorder (PTSD), sleep disorders, anxiety, and self-harm (Dillon et al., 2013). Survivors often experience antisocial and suicidal behaviors, fear of intimacy including forms of emotional detachment, and problems trusting others (Taylor, 2019). In addition, survivors are at higher risk of engaging in health risk behaviors such as smoking, binge drinking, and sexual risk behaviors (Centers for Disease Control and Prevention, 2019). In a study conducted by Walby and Allen (2004), compelling evidence revealed that many common mental health problems that women experience are a direct consequence of IPV, and negative impacts can often last for years (Franzway et al., 2019). A large portion of gender-based violence research has focused on medicalized interventions including how physicians, nurses, and other medical professionals can screen and intervene with a focus on physical violence. Within both medical and nonmedical professions, primary intervention and prevention efforts have centered on physical safety (Mehrotra et al., 2016). Emotional and psychological abuse defined as nonphysical forms of coercion and control that include criticism, gaslighting, isolation, and threats (National Network to End Domestic Violence, 2020) can take longer to identify as the vernacular is not as far-reaching and the emphasis is often placed on physical acts of violence that are more easily identifiable. Mental health providers are often critical access points for those experiencing violence. Although survivors of IPV use mental health services more frequently than the general population, only between 10% and 30% of cases are documented by mental health services (Howard et al., 2010; Oram et al., 2013). According to Howard et al. (2010), clinicians often do not ask mental health service users questions about domestic violence (DV).
The National Alliance on Mental Illness or NAMI (2019) defines mental health professionals (MHPs) as those having the ability to evaluate a person’s mental health, diagnose, and provide therapeutic interventions. Categories of MHPs include psychologists, therapists, counselors, and clinical social workers. Additional studies reveal that many MHPs lack sufficient training needed to recognize and provide treatment for DV survivors (Gauthier & Levendosky, 1996; Murray & Graves, 2013; Wingfield & Blocker, 1998). Although studies reporting MHPs’ personal DV histories are limited, according to a previous study, 92% of social workers state that they have had contact with DV victims professionally, and more than 50% reported having experienced DV personally (Danis & Lockhart, 2003). Therefore, it is important for MHPs to know how to integrate screening, safety planning, differential assessment, and best practices regarding IPV into their interventions in order to safely and effectively respond to survivors and/or perpetrators of abuse.
Historically, MHPs have inadequately responded to IPV due to the lack of training and education, leaving graduates unprepared to effectively identify and assist victims (Fedina et al., 2017). Conversely, in practice settings, some MHP credentialing boards, such as counselors, require training yet provide minimal quality and are not necessarily extensive (Murray et al., 2016). A study was conducted to learn more about marriage and family therapists’ (MFTs) experiences associated with working with IPV clients and highlighted that therapists lacked training related to these cases, ultimately influencing the therapists’ ability to effectively practice with these clients (Karakurt et al., 2013). An additional study revealed ongoing concerns about the adequacy of family therapy training (Dersch et al., 2006).
Some MHPs may feel unprepared to address IPV confidently, thus intervening prematurely without a thorough assessment of the situation. In a study conducted by Gillian (2000), 18 counselors were interviewed regarding their caseloads involving IPV clients. Nearly all of the participants reported a loss of confidence in working with victims and perpetrators of IPV. Overall, there is a limited amount of studies examining the direct relationship between MHPs, their level of educational and professional preparation, and how this affects the work they do in therapeutic settings with clients experiencing IPV. More urgently, inaccurate and uninformed information can isolate and invalidate victims, particularly victims who are already marginalized.
This systematic review explores and seeks to discover what is known about how social workers, psychologists, MFTs, and substance abuse counselors are prepared to work with those affected by IPV. We conducted a review of peer-reviewed journals to answer the question, “How are MHPs in the United States prepared to work with survivors of IPV in practice settings?”
Method
Search Strategies
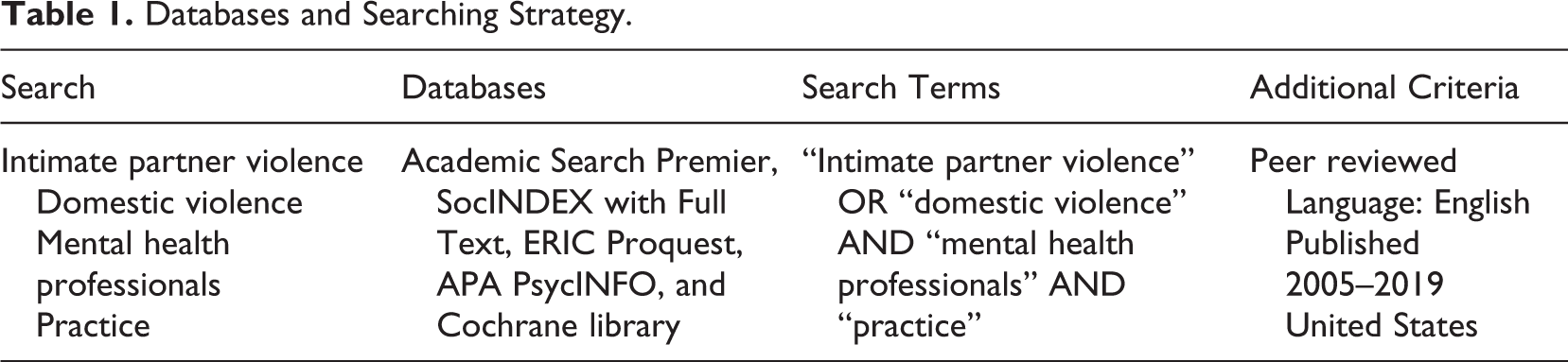
Adapting the Cochrane guidelines for systematic reviews, guidelines (Higgins et al., 2020), this study specifically reviewed peer-reviewed articles written in English and published between 2005 and 2019 focusing on the preparation of MHPs to work with IPV survivors in the United States. The sole geographical location of this review is situated in the United States based on how MHPs are defined, placing more of an emphasis on individualized talk therapy and therapeutic approaches to care. We chose to review recent studies between 2005 and 2019 based on the 2005 reauthorization of Violence Against Women Act. This pivotal U.S. federal legislation originally enacted in 1994 was created to combat violence against women and to provide protection and services to those experiencing violence. The 2005 reauthorization focused on expanding protections for immigrants experiencing domestic and sexual violence (Conyers, 2007) leading to an increase in diversified awareness and services. The comprehensive search was performed in the following databases: Academic Search Premier, SocINDEX with Full Text, ERIC Proquest, APA PsycINFO, and Cochrane library. We employed manual and electronic search techniques in order to locate all related studies. The Boolean search strategy (Brunton et al., 2017) was used to combine keywords, such as “intimate partner violence” or “domestic violence,” and “mental health professionals” and “practice.” The search terms were determined by an initial scoping search to identify keywords that are used in the literature pertaining to IPV, mental health, and practice before proceeding with the main search. The search details are presented in Table 1.
Databases and Searching Strategy.
Selection Process
For inclusion, peer-reviewed articles were required to (a) be written in English; (b) be among nonmedical MHPs (those who by profession cannot prescribe medications and are most likely to provide counsel and therapy to clients on a regular basis) including social workers, psychologists, MFTs, and substance abuse counselors where they are employed in U.S. agencies; and (c) focus on studies published between 2005 and 2019. Studies were excluded if they did not meet the inclusion criteria. Preferred reporting items for systematic review (PRISMA; Liberati, 2009) flow diagram was utilized for the study selection process as shown in Figure 1.
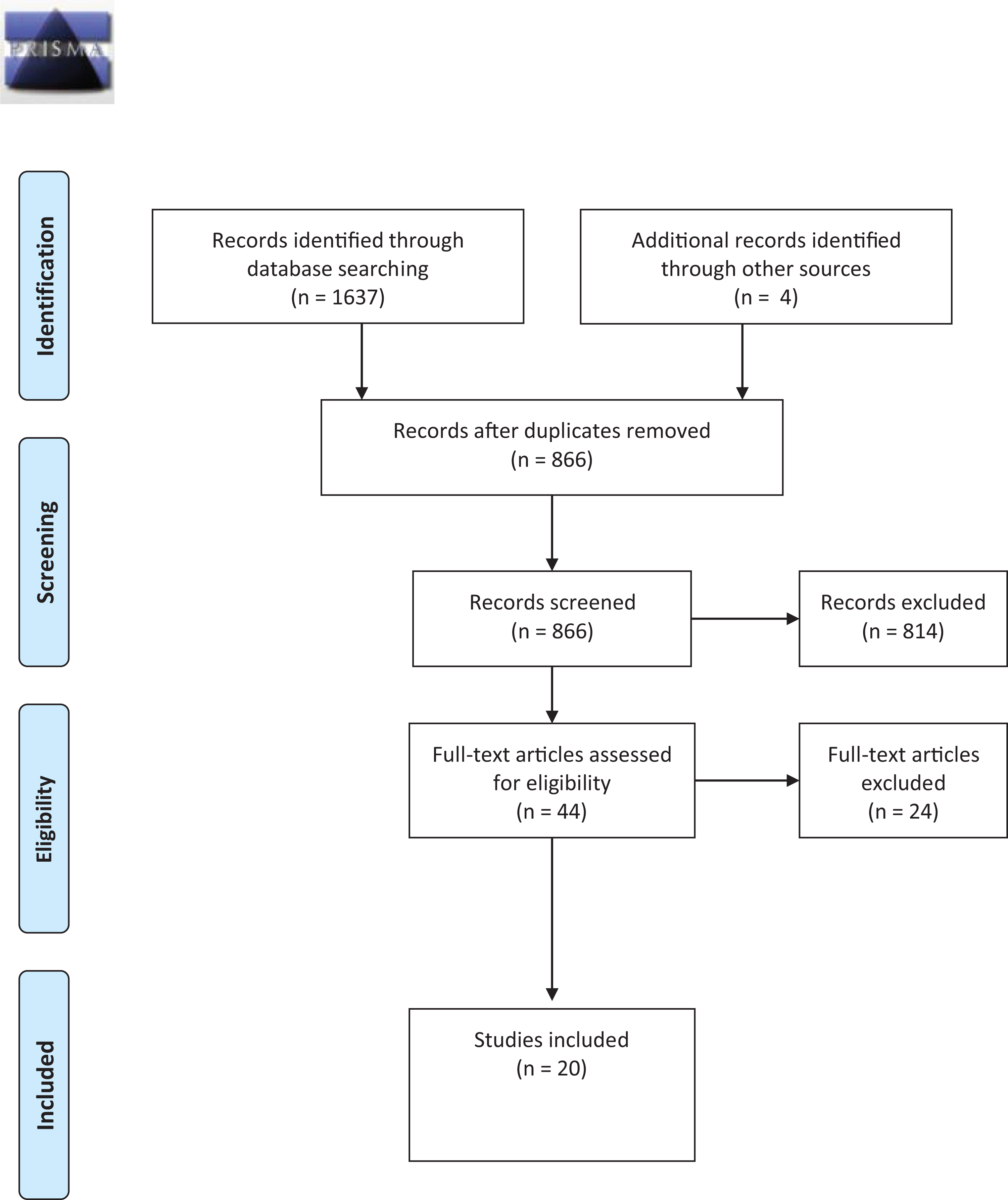
Preferred reporting items for systematic review 2009 flow diagram.
Review Process
The present review identified 20 articles that met the inclusion criteria. We began the study by articulating the research question to guide our review: “How are MHPs in the United States prepared to work with survivors of IPV in practice settings?” To address the research question of the review study, two investigators first screened titles and abstracts followed by subsequent searching for full texts. All disagreements were discussed and resolved in research meetings. The initial search yielded 1,637 potential articles which were reduced to 866 once duplicates were removed. These 866 articles were reviewed by title and following the title review, 52 abstracts were screened, leaving a total of 44 articles for full-text review. After eliminating 24 articles, 20 were included in our study. We included the results and discussion sections within the table. The content data were analyzed from the included articles and two researchers identified and coded characteristics of the participants, setting, provider type(s), and research design. Articles were stored in the EndNote database to increase the efficiency of the review process and all disagreements were discussed and solved through research meetings.
Findings
Among the 20 articles, demographic information was provided about the participants including their age, profession, years of experience, gender, race/ethnicity, education level, and geographic location. It is important to note that within these articles, the term domestic violence (DV) was often used interchangeably with IPV, and as a result, the themes reflect the terminology used by included authors. Table 2 presents details of the 20 studies reviewed. The methodology for these 20 studies included five qualitative studies, eight quantitative studies, one mixed-methods study, two case vignettes, two systematic reviews, and two literature reviews. Of the studies included, MHPs included MFTs, social workers, counselors, psychologists, IPV service providers, substance abuse counselors, welfare managers, social work students, and family and marriage therapy students. Five themes were identified including lack of preparation and inadequate training in DV (Dersch et al., 2006; Fedina et al., 2017; Karakurt et al., 2013; Kress et al., 2008; Murray et al., 2015; Raphael-Dudley et al., 2008; Schneider, 2018; Todahl et al., 2008), benefits of DV training (Forgey et al., 2013; Kulkarni et al., 2015; McCloskey & Grigsby, 2005; Murray et al., 2016; Payne et al., 2007; Saunders et al., 2006), need for collaboration between service providers (Capezza et al., 2014; Macy & Goodbourn, 2012; Macy et al., 2009), stigmatizing attitudes and behaviors toward survivors (Crowe & Murray, 2015), and the advocate–survivor connection (Bogat et al., 2013; Wood, 2017). These studies can be found in Table 2.
Mental Health Professionals and Domestic Violence (DV) Training.
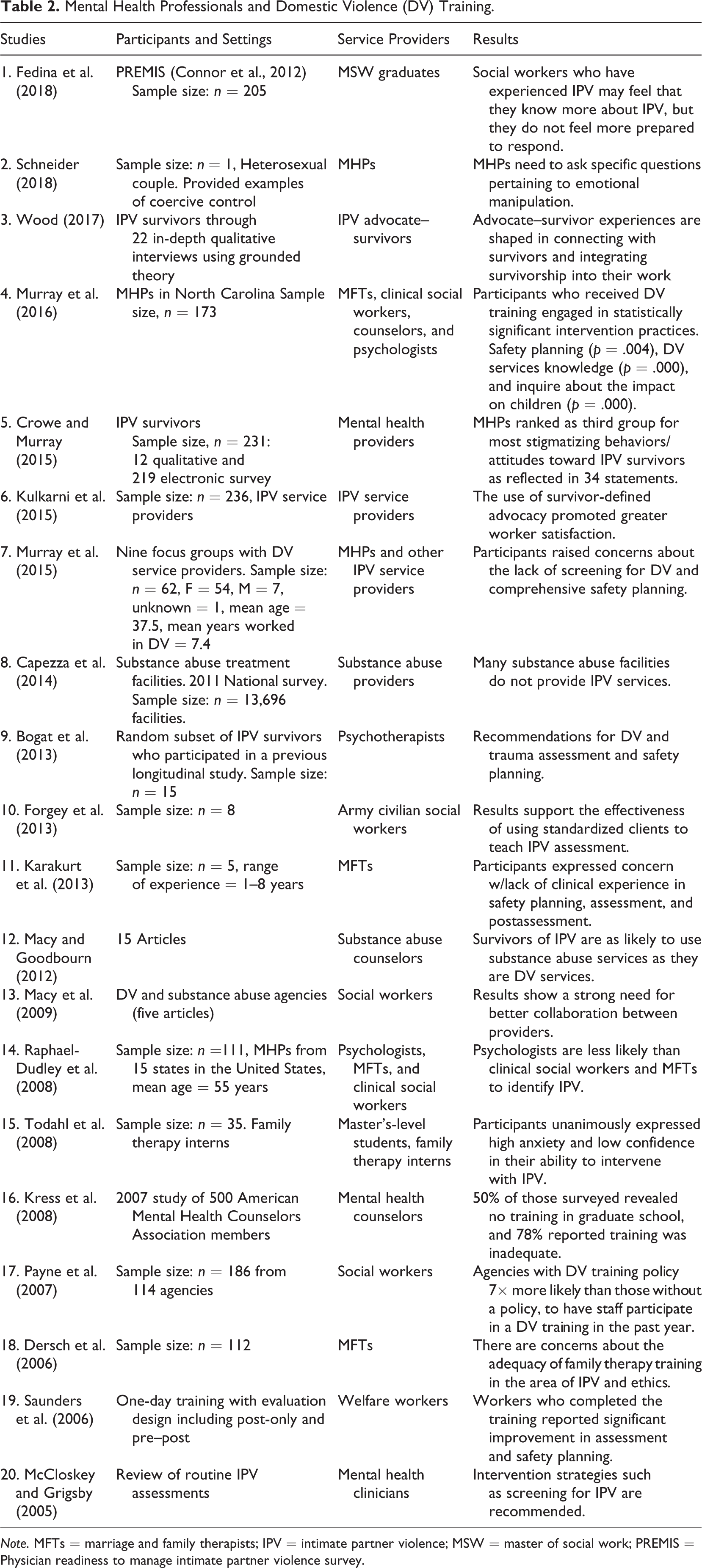
Note. MFTs = marriage and family therapists; IPV = intimate partner violence; MSW = master of social work; PREMIS = Physician readiness to manage intimate partner violence survey.
Theme 1: Lack of Preparation and Inadequate Training in DV
This review found that many MHPs felt underprepared with inadequate training specifically related to DV. Several studies revealed that MFTs and other mental health counselors expressed concern about the lack of confidence in safety planning and intervention due to a lack of course materials and clinical experience (Dersch et al., 2006; Karakurt et al., 2013; Kress et al., 2008; Murray et al., 2015). In addition, psychologists were less likely to identify IPV compared to other MHPs (Raphael-Dudley et al., 2008). Additional articles revealed that MHP students including master’s-level family therapy interns (Todahl et al., 2008) and master’s-level social work students (Fedina et al., 2017) were inadequately prepared to work with clients experiencing IPV with limited formal education and coursework specifically addressing IPV. More specifically, Schneider (2018) found that MHPs lacked more in-depth training related to other forms of IPV such as coercive control and emotional manipulation.
Theme 2: Benefits of DV Training
From this review, we found that formal DV training revealed a plethora of benefits. Multiple authors found that MHPs who received DV training were more prepared to work with survivors and showed improvement in their ability to administer assessments and safety plans (McCloskey & Grigsby, 2005; Murray et al., 2016; Saunders et al., 2006). Additionally, agencies with DV training and policies embedded into their organization were more likely to have MHPs participate in those trainings suggesting that organizational support increased participation (Payne et al., 2007). Another study found that the survivor-defined advocacy model increased MHP worker satisfaction and decreased the pressure to be an expert on DV while working with clients (Kulkarni et al., 2015). One specific study revealed that army civilian social workers benefited from utilizing simulated clients in order to better assess IPV (Forgey et al., 2013).
Theme 3: Need for Collaboration Between Service Providers
The Office on Women’s Health: Washington, DC. (2019) reported that 90% of women with substance abuse problems have experienced violence. Capezza et al. (2014) revealed that most substance abuse service providers do not include IPV services. Macy and Goodbourn (2012) also found this to be accurate and urged for further collaboration between DV agencies, service providers, and substance abuse providers. Additionally, Macy et al. (2009) found that when DV and substance abuse agencies collaborate, better services are provided showing that more successful collaborations are needed between these service sectors.
Theme 4: Stigmatizing Attitudes and Behaviors Toward Survivors
IPV victims and survivors often report blaming, dismissing, and shaming from MHPs. Crowe and Murray (2015) conducted a study that revealed stigmatizing language and behavior from MHPs toward victims including statements such as, my marital counselor said, make a list of all the sins you committed against him and ask him for forgiveness and he told me I was triggering my exes controlling behavior and sexual assaults and encouraged me to focus on my own contributions. (p. 172) she [on campus counselor] told me that my partner was controlling. When I came to hear [sic] with what I know now are clearly PTSD symptoms, she told me that couldn’t be what is was. (p. 172)
Theme 5: The Advocate–Survivor Connection
Over half of social workers disclosed that they have experienced IPV themselves (Danis & Lockhart, 2003) allowing for a special bond between these advocates and survivors. Wood (2017) found that IPV advocate–survivor provide a unique approach to IPV work from their lived experiences in addition to their professional training and can inform practice approaches designed to meet the survivor’s needs. Bogat et al. (2013) advocate for psychotherapists to integrate a trauma-informed model that honors the survivor’s narrative, help the client reach insight, and identify social supports that can aid in safety and healing.
Discussion
The primary themes of this review related to DV training, collaborative service providers, stigmatized attitudes and behaviors, and advocate–survivorship are closely tied to the need for increased understanding of intersecting identities and multifaceted perspectives. Such experiences of survivors are not limited to isolated identities or siloed histories of trauma. It is evident that MHPs would benefit from receiving more specialized training in how to understand and incorporate an intersectional feminist framework. Through this approach, mental health practices could be tailored when clients seek or are referred for services. Intersectionality can unite MHPs and individuals experiencing violence in a truly meaningful way as this framework is an ever-important reminder for MHPs to center the most marginalized communities in the work (Mehrotra et al., 2016) and to develop and strengthen therapeutic responses for all survivors.
Birthed out of the black feminist movement nearly 30 years ago, Kimberlé Crenshaw (1991)) introduced the concept of intersectionality to feminist theory. Conceptualized as a methodology grounded in black feminist epistemology, the theory of intersectionality posits that socially constructed categories of oppression and privilege interact to create unique life experiences (Collins, 2000; Crenshaw, 1991; King, 1988; McCall, 2005). Intersectionality is central to a practitioner’s inquiries about how and why people act in certain ways and not others and can “highlight how those in power develop perspectives and practices that can stigmatize and pathologize the behaviors of marginalized groups” (Aronowitz et al., 2015, p. 405). Intersectionality can effectively meet the needs of survivors by acknowledging the “uniqueness of women’s experiences of violence and a pattern of culturally and historically specific epidemics of violence against women” (Nixon & Humphreys, 2010, p. 154). In addition, intersectionality to education and practice can make for a more inclusive and gender-sensitive process that helps rather than hinders individuals experiencing this national crisis and destigmatizes abuse. Specifically, intersectionality approaches can encourage MHPs to share power by facilitating meaningful survivor participation, individualizing interventions, and expanding expertise and advocacy for systems change (Kulkarni, 2018). Through the application of this framework, therapists can move beyond the survivor-centered model to more survivor-informed work that honors lived experiences and self-determination (Mehrotra et al., 2016).
Recommendations for MHPs
IPV is not a singular event but instead a complex and multidimensional pattern and is intricately woven into larger social and political injustices. It is essential for MHPs to bring attention to the effects of violence against women including harder to identify tactics of abuse such as manipulation, gaslighting, isolation, and symbolic violence. MHPs are called to be responsible consumers of this knowledge and can critically examine how state and federal legislation either assist or oppress victims as through funding, available resources and access to care, and institutional support (Dutton et al., 2015). Appreciating individual experiences particularly through an intersectional lens, MHPs can implement effective assessment tools that take into account trauma histories, identify risk, and discuss safety planning measures that move beyond just physical abuse or leaving one’s partner. These engagement strategies will be more impactful than simply relying on traditional talk therapy approaches as this population has unique needs. A more nuanced understanding of IPV including safety planning and tangible strategies that clients can use to match with the reality of their lives and address their unique safety risks is required (Murray et al., 2015). It is also necessary for designing treatment approaches that speak to individuals with varying and intersecting identities as their experiences and barriers will look quite different.
Requiring continuing education, professional training, increasing academic courses offered on the topic, and including IPV-specific scenarios on licensing exams could be solutions to increasing MHP’s awareness about IPV and influence their practice. Additionally, debunking common myths and misconceptions including the notion that leaving an abusive relationship is the only answer for survivors is key in meeting their multifaceted needs. MHPs can assist survivors by inquiring about past stigmatization received from other professionals to ensure negative experiences are not repeated as well as confront any negative attitudes they might hear from other professionals (Crowe & Murray, 2015). Shifts in the MHP’s own perspectives through self-reflective practices could also have the potential to reduce stigmatizing attitudes and beliefs and to recognize the value of their own lived experiences as survivors and of those who have no formal training in IPV. Positionality and reflexivity call for MHPs to question and challenge their assumptions and beliefs as practitioners and as advocate–survivors (Wood, 2017) and the social constructs that aid in the perpetuation of IPV. It is noteworthy that if MHPs have not engaged in their own personal work, they should not expect survivors to do the same.
A major component of reflexivity and positionality calls into play for MHPs to engage in their own personal work around their lived experiences and traumas, not just as therapists but as people. Unaddressed traumas can interfere with assisting survivors and can unintentionally recreate power imbalances between therapist and client. In addition, reflexivity practice requires that practitioners remain open to change and to critically examine practice, research, and policy. It is as equally as important to be aware of ethical considerations per one’s profession, to be transparent regarding limits of confidentiality, and to emphasize a survivor-informed model. As social workers, researchers, and advocates, we must also challenge our own privilege and identity on a daily basis in order to effectively and intentionally engage in this work.
Relevance to Social Work
It is clear that social workers have a unique and influential role to play as professional social workers comprise the largest group of mental health service providers in the nation (National Association of Social Workers [NASW], 2020). Named as one of the profession’s grand challenges, social work’s responses to addressing gender-based violence remain inadequate, and we have room to expand our creativity and collaborative efforts particularly as it relates to tailoring counseling services that promote safety for all family members (Edleson et al., 2015). Social workers have the ability to reimagine the mental health profession’s response to those impacted by IPV and to hold ourselves and each other accountable for creating solutions that are founded within the core principles of feminism, which require that we be open to other ways of knowing (Hyde, 2013) and revision what it means to truly meet people where they are.
The profession of social work should pay particular attention to those directly affected by IPV and the direct mental health services they often provide. Social workers are also uniquely situated in micro-, mezzo-, and macrolevels of care and can address IPV within the United States directly, in communities, and through policy and research avenues. Embedded in the Social Work Code of Ethics are the principles of autonomy, self-determination, and dignity and worth of a person (NASW, 2017). If any profession is posited to examine structural, political, and representational barriers, it is social work. Social workers who identify and practice as MHPs can apply comprehensive and holistic approaches to identifying and addressing IPV. Our challenge to the profession is to lean into our ethics and values which call for respecting and including diverse perspectives, to acknowledge our own privileges, and to honor stories that might be different from our own, all of which are the cornerstones of intersectionality.
Strengths and Limitations
There are several strengths in the present study. First, we engaged in an extensive search and screening process to verify eligible studies included in this review. Second, the present study includes mental health providers from various helping professions that offer services to IPV survivors, reflecting diversity as synthesized from the literature. The study also provides a context to understand the existing strengths of mental health practice and current gaps that can be used to improve service delivery. However, despite conducting a comprehensive search, it is possible that additional eligible studies may have been missed. Studies that were not published in the United States in English and gray literature were not included in this study. This study primarily focused on MHPs defined as therapeutic service providers specific to the United States. Future studies should consider including those outside the United States and how they define MHPs as other countries may have similar findings.
Additionally, the inclusion criteria limited participants by nonmedical mental health professions (those who by profession cannot prescribe medications and are most likely to provide counsel and therapy to clients on a regular basis) and so medicalized professions such as psychiatry were not included. As mentioned earlier, a large number of researchers have focused their efforts on medicalized interventions, with gaps still remaining on how nonmedical, therapeutic providers can implement their own responses. The selected providers such as social workers, psychologists, MFTs, and substance abuse counselors cannot represent all mental health providers interacting with IPV victims, which potentially influenced the implications of this review’s findings. The majority of articles contained smaller sample sizes and/or represented concentrated geographical locations. When demographic information was presented, the majority of participants identified as Caucasian and female.
From an intersectional lens, studies are lacking in representing other identities and speaking to other demographics of MHPs providing services to clients experiencing IPV. These underrepresented voices are important and need to be included in future research to understand the issue more holistically and for creating broader solutions for both survivors and those who perpetrate violence. To increase future generalizability, future researchers should include studies with larger sample sizes of the mental health professions including professions classified as medical and cast a wider net for recruiting professionals in varying locations within and outside of the United States. Although the authors minimized potential biases using the PRISMA protocol, since only peer-reviewed publications were selected and other types of studies were excluded, the authors acknowledge a potential publication bias. Despite these limitations, our review provides an important contribution to MHPs and for clients experiencing IPV who seek out mental health services.
Conclusion
In this review, we critically examined and synthesized 20 studies addressing the level of educational and professional preparation of MHPs and how this affects the work they do in practice settings with clients experiencing IPV. The study provides contributions to recognize how MHPs are prepared and in what ways they are underprepared to address IPV. According to the current literature, IPV training for those providing mental health services remains inconsistent, and as a result, practitioners feel unequipped to effectively assist clients who are experiencing violence. In addition, there is a lack of exposure to IPV and the intersectional feminist framework lens within current coursework, agency training policies, and continuing education opportunities for clinicians to learn practical application skills.
Therefore, we conclude that most MHPs are not adequately prepared or supported in their work with clients experiencing IPV, which may result in lower worker and client satisfaction, increased risk of danger and harm to clients, and higher rates of burnout and secondary trauma. By applying and emphasizing a more nuanced understanding of the connection between individual and structural explorations of gender, race, class, and other socially constructed identities, MHPs can utilize the skills necessary to challenge inequalities which in turn can encourage survivors to create strategies that makes sense to themselves and their communities. MHPs can be an important component of the healing process for many victims, and the mental health field needs to take additional action steps to ensure that clients feel safe, heard, and understood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.