
Abstract
As one of the world’s most vulnerable populations, women with disabilities are frequent victims of physical, emotional, sexual, and financial abuse. Indeed, they experience abuse at higher rates than women and men who do not have disabilities and men with disabilities. They are also more likely to experience intimate partner violence (IPV) than any other adult group. Yet there is not one psychosocial intervention tailored to the needs of women with disabilities who have experienced IPV that facilitates their recovery from complex trauma. This is largely the result of limited (albeit growing) research on the risk factors for IPV, barriers to leaving abusive relationships, and trauma-related issues that women with disabilities face, especially among racialized women with disabilities, 2SLGBTQ+ women and gender nonconforming persons with disabilities, older/aging women with disabilities, and other subgroups. In order to develop the most culturally competent, effective interventions and policies to address the prevalence of IPV among women with disabilities, an approach that is informed by a combination of critical disability theory, feminist disability theory, and complex trauma theory is recommended. IPV among women with disabilities is a global injustice; therefore, this concern is highly relevant to the field of social work and its mission to advance social justice.
Women with disabilities are one of the world’s most vulnerable populations and, therefore, are also frequent victims of physical, emotional, sexual, and financial abuse (Ballan & Freyer, 2017). Indeed, women with disabilities experience these abuses more often than women and men who do not have disabilities, and more often than men with disabilities (Breiding & Armour, 2015). Brownridge (2006) reported that the physical abuse endured by women with disabilities is typically severe (e.g., kicking, punching). Other forms of abuse are more covert, such as withholding medical treatment and denying access to social support (Lund, 2011). While family members and medical personnel are among the known perpetrators of these abuses, intimate partners are frequent perpetrators of abuse against women with disabilities. Hahn et al. (2014) have demonstrated that intimate partner violence (IPV) impacts the lives of women with disabilities more than any other adult group.
Adding further support to this phenomenological finding, the 2013 National Crime Victimization Survey identified that people with disabilities have violent crimes committed against them at a rate that is 3 times higher than the rate of violent crimes committed against people without disabilities; and the crimes were observed to be perpetrated most often by intimate partners (Harrell, 2015). Similarly, the 2010 National Intimate Partner Violence and Sexual Violence Survey indicated that women with disabilities were much more likely to experience violent crimes—more specifically, physical and sexual assault, psychological aggression, stalking, and control of biological reproduction—than were women without disabilities (Breiding & Armour, 2015). In addition to the obvious physical consequences (i.e., injuries) that result from these crimes, the World Health Organization (2011) reported that women with disabilities who experience IPV are at risk of reduced overall health, both immediate and long-term, leading to mental health issues, drug abuse/addiction, and even death. Dillon et al. (2013) noted that the specific mental health issues connected to IPV include depression, anxiety, post-traumatic stress disorder (PTSD), self-harming behavior (e.g., cutting), and disordered sleep. In earlier research, Weissbecker and Clark (2007) also identified a link between the experience of trauma—including IPV—among women and maladaptive health behaviors.
Risk Factors for IPV
Women with disabilities have a dense and enduring history of devaluation, segregation, lack of community support, lack of reproductive rights, educational inequality, and numerous other manifestations of discrimination. As a result of this history, several unique risk factors have been identified among women with disabilities that increase their vulnerability to IPV. These factors include physical and social isolation, difficulty with identifying abuse, dependence on abusive partners to meet basic and other personal needs, and overall vulnerability that is secondary to having a disability, which may include the inability to leave an abusive environment (Plummer & Findley, 2012). Stigmatization also impacts the vulnerability of women with disabilities and engenders social oppression. Pérez-Garín et al. (2018) noted that stigmatization occurs “when a person or group possesses (or is believed to possess) some attribute or characteristic which conveys a social identity that is negative or devalued in a particular context” (p. 1). Thus, intimate partners may, for example, capitalize on the stigmatization of women with disabilities as asexual and physically undesirable by making derogatory statements and engaging in other forms of verbal abuse, which significantly impacts women’s self-esteem. This abuse also reduces women’s self-concept—more specifically, the belief that they deserve better than an abusive relationship (Hassouneh-Phillips & McNeff, 2005).
The likened stereotype that women with disabilities are perpetually single and cannot have children makes leaving an abusive environment even more difficult for married women with disabilities who do have children. This, in fact, is most often the case among women with disabilities experiencing IPV (Ballan et al., 2014). Ortoleva and Lewis (2012) found that perpetrators of IPV against women with disabilities may even claim that women’s disabilities make them unable to parent, thereby threatening the loss of their parental rights. Additional risk factors include limited access to resources, such as law enforcement (i.e., due to mobility limitations or other catalysts of social isolation), attitudinal and physical barriers (i.e., inaccessibility) of service agencies, and fear of retaliation from the perpetrator (Chang et al., 2003). Economic barriers are also major obstacles for addressing IPV among women with disabilities. The poverty rate among women with disabilities is disproportionate—that is, exceedingly higher—compared to the general population (Hassouneh-Phillips et al., 2005). Ballan et al. (2014) identified, furthermore, that the low socioeconomic status (SES) among women with disabilities is largely the result of high rates of unemployment and diminished social status.
Knowledge and Intervention Gaps
While there is growing research on the needs of women with disabilities in general who are experiencing IPV, which includes a wide range of disability types, there is a dearth of research on IPV within specific disability groups (Hughes et al., 2011). There is also limited research on the needs of diverse groups of women with disabilities experiencing IPV, such as racialized women, LGBTQ+ including two-spirit (2SLGBTQ+) women and gender nonconforming persons, immigrant and Indigenous women, older/aging women, women living in poverty, and other subgroups of women with disabilities (Ballan & Freyer, 2017). This is reflected in the narrow understanding of the multicultural and overlapping experiences of women with disabilities among disability organizations. In their systematic review, Mikton et al. (2014) discovered that there is not one intervention tailored to women with disabilities who have experienced IPV. Traditional IPV interventions, those based on domestic violence (DV) theory, have simply been applied to women with disabilities (Barranti & Yuen, 2008). Unfortunately, as Plummer and Findley (2012) have asserted, this model is founded on the assumption that the risk factors and results of IPV among women with disabilities are similar to those among women without disabilities—a claim not supported by existing research. Addressing this social justice issue, Ballan and Freyer (2017) made the following poignant observations: Abuse among women with disabilities has largely been addressed within either domestic violence organizations lacking experience with this population, or disability-focused organizations unfamiliar with IPV…. Accessibility moves beyond physical infrastructure and considers the needs of women with disabilities in their policies and practices, establishing relationships with disability organizations and interpreter services, and accommodating women with varying levels of medication use, service animals, and personal care attendants. These accessibility considerations extend to trauma-informed practice with survivors of IPV with disabilities. (p. 133)
Operationalizing Constructs and Variables
Luskin Biordi and Nicholson (2013) have defined social isolation as “the distancing of an individual, physically or psychologically, or both, from [their] network of desired or needed relationships with other persons… a loss of place within one’s group(s)” (p. 97). Existing research on IPV among women with disabilities suggests that social isolation is a significant contributing variable to their experiences of abuse. A corresponding hypothesis would propose that the more socially isolated women with disabilities are, the more vulnerable they are to IPV. Women with greater limitations in functioning due to disability have less access and supportive infrastructure in the community, less social capital, which increases their dependence, vulnerability, and social isolation. In other words, they are “disabled” by their inaccessible environment. Enduring social isolation, furthermore, is a risk factor for both high severity (i.e., more violent) and high-frequency IPV. Thus, interventions that increase social connectedness or sense of belonging among women with disabilities would be expected to reduce their risk of IPV and, in turn, reduce their experience of the complex trauma resulting from severe and long-term abuse.
Figure 1 is a graphical representation of the pathway to complex trauma experienced by women with disabilities as a result of severe and long-term IPV (i.e., multiple incidents of abuse that occur over time), which is strongly supported by social isolation. The graphic demonstrates how the trauma resulting from IPV becomes complex when the severity and duration of IPV increase and women with disabilities remain socially isolated from a support network. If women with disabilities were less isolated, any member of their support network could intervene and potentially facilitate the end of the abuse. For example, a coworker could notify Adult Protective Services (APS) of the abuse or assist with reporting to the police. A family member could provide alternate housing. A social worker could offer resources for safety and other emergent needs, as well as trauma-informed care, which considers the impact of violence on all facets of a person's life (Elliott et al., 2005).
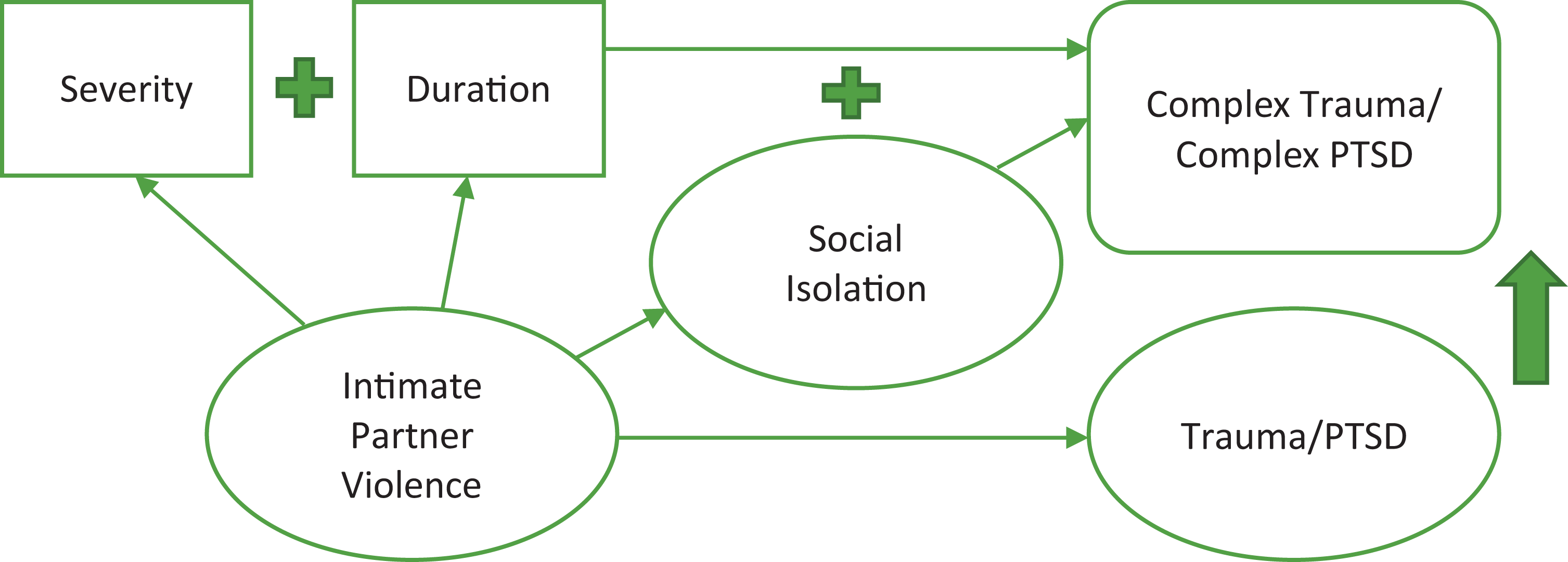
Complex trauma among women with disabilities experiencing intimate partner violence.
Similarly, many of the previously identified risk factors for IPV among women with disabilities, including dependence on abusive partners to meet basic and other personal needs, limited access to resources, and mobility limitations, could be abated if women with disabilities were more connected to social support networks. Indeed, a common tactic among perpetrators of abuse is to isolate those they abuse from their social networks for the very purpose of maintaining the abuse. As women with disabilities are even more vulnerable to this isolation, future policy and psychosocial interventions must consider and account for this risk factor. Agencies that serve survivors of IPV must also increase their access and preparedness to meet the needs of women with various types of disabilities who have escaped abuse. Other professionals (e.g., medical providers, case managers, vocational counselors) who serve women with disabilities are encouraged to increase their knowledge of IPV (e.g., signs of abuse) and their knowledge of the myriad barriers women with disabilities encounter when attempting to leave abusive partners, many of which are the very risk factors that exposed them to IPV (e.g., limited mobility, high unemployment rate/low SES, mental health issues).
Proposing a Combined Theoretical Approach
While it may seem appropriate to apply trauma theory to this social justice issue, as the theory has been previously applied to IPV interventions for women with disabilities, Quiros and Berger (2015) reported that traditional trauma theory does not address the individual characteristics related to race, ethnicity, disability, and other diverse cultures. (For a complete history of trauma theory, see Ringel & Brandell, 2012.) Moreover, traditional trauma theory does not account for the impact of devastating traumas that occur over time, such as physical abuse that gradually increases in severity. Complex trauma theory, however, does account for multiple and escalating traumas, and is therefore more appropriate to apply to future research on IPV among women with disabilities. Courtois (2008) defines complex trauma as “a type of trauma that occurs repeatedly and cumulatively, usually over a period of time and within specific relationships and context” (p. 86). In addition, DV, which is synonymous with IPV, has been identified as one of the primary forms of complex trauma (Courtois, 2008). This definition of complex trauma and its strong connection to DV further supports the utility of complex trauma theory for promoting social justice for women with disabilities experiencing IPV.
Although complex trauma theory can help inform future research, agency policies, and psychosocial interventions tailored to address the needs of women with disabilities experiencing IPV—that is, because it explains the effects of severe and long-term trauma—the theory does not address the group’s experiential factors related to sex (i.e., as women) and disability. Therefore, to promote change and advance justice most effectively in the lives of women with disabilities experiencing IPV, interventions must also be informed by critical disability theory and feminist disability theory. Ballan and Freyer (2017) purport that these theories are crucial to the systematic development of culturally competent practices for IPV interventions for women with disabilities. Making connections to the social model of disability, Shakespeare (2014) explained that critical disability theory defines the construct of “disability” not as a tangible medical condition, but rather as an interactive process between personal factors and contextual factors. Thus, the oppression experienced by women with disabilities, which here is narrowed to IPV, is not only a personal issue but a societal issue, with both personal and political implications.
In further application of critical disability theory to women with disabilities experiencing IPV, Ballan and Freyer (2017) identified some of the personal factors within the group: the severity of the women’s disabilities, their personal thoughts and feelings about their disabilities, and their unique personalities (i.e., psychologies). Contextual factors include “attitudes and reactions of others to [a woman’s disability], the extent to which [a woman’s] environment is accommodating of disability, and wider cultural, social, and economic issues relevant to disability” (Ballan & Freyer, 2017, p. 135). Accordingly, critical disability theory can serve as an ecological framework that incorporates the tenets of person-in-environment (PIE). The Encyclopedia of Social Work (2013) defines PIE as a principle that underlines the utility of examining the environmental contexts in which a person lives in order to understand that person and their behavior. Similarly, critical disability theory emphasizes the unique cultural experience of women with disabilities within the larger social context; and, thus, the theory can inform the development of environmental interventions.
Feminist disability theory (Asch & Fine, 1988; Garland-Thompson, 2002) also emphasizes the intersecting identities of sex (i.e., being women) and disability (i.e., physical, intellectual, etc.). More specifically, the theory acknowledges that IPV experienced by women with disabilities is the result of the stigmatization experienced by people with disabilities compounded by the inequality experienced by women. In further support of feminist disability theory, Barranti and Yuen (2008) have asserted that the theory can resolve the insufficiencies of current IPV interventions for women with disabilities by “emphasizing issues of gender, disablism, poverty, and the inherent social oppression that intersect in the experience of IPV and abuse of women with disabilities” (p. 128). To that effect, feminist disability theory incorporates the concept of intersectionality, which was first developed by Crenshaw (1989) to describe the intersecting sociopolitical experiences of Black women.
Importance of the Combined Theoretical Approach
With a focus on the constructs of social isolation and complex trauma, a theoretical framework that utilizes critical disability theory, feminist disability theory, and complex trauma theory will best address the specific needs of women with disabilities experiencing IPV. Indeed, this combined theoretical approach will inform the most culturally competent and effective interventions, including those related to prevention. This synthesis of theories to inform policy and psychosocial interventions considers the experiences of women from a feminist perspective; people with disabilities from a critical theory perspective; women with disabilities from an intersectionality perspective; IPV from a complex trauma perspective; and all of these cultures, identities, and experiences from a PIE perspective.
Assessing Scientific Merit
A fusion of critical disability theory, feminist disability theory, and complex trauma theory—with applications of PIE and intersectionality—has strong scientific merit. Individually, each of the theories has substantive support in the literature; so combined, these theories will arguably inform even sounder research designs. They are also among the most progressive and generalizable theories relevant to disability research. Furthermore, these theories are most appropriate for explanatory research on IPV among women with disabilities. To review, critical disability theory places the construct of disability outside the person; identifying the disablement not as an inherent trait of the disabled person’s physical, cognitive, or psychiatric condition, but rather as a characteristic of the “disabling” or inaccessible environment (Shakespeare, 2014). Accordingly, the theory does not support the idea of a problem or malady being intrinsic to women with disabilities simply because they have a disability, as the medical model would, but rather asserts that the challenges they experience are the result of society’s discriminatory responses to their physical and/or cognitive differences. In other words, similar to the social model of disability, critical disability theory attributes the hardships experienced by women with disabilities to societal barriers, which include social, political, economic, physical, and psychological limitations.
Feminist disability theory calls to the forefront the intersecting identities of sex (i.e., womanhood) and disability (Asch & Fine, 1988; Garland-Thompson, 2002). Chiefly emphasized are the sociopolitical experiences of women, including their history of inequality. The applications of feminist theory to the experiences of women with disabilities, whose identities are highly politicized, are historical; however, the application of feminist disability theory to the incidences of IPV among women with disabilities is novel, particularly in combination with critical disability theory and complex trauma theory. This new theoretical approach, therefore, has the potential to inform new methods of data analysis, additional qualitative inquiry, and much-needed policy reform.
By focusing a broader theoretical lens on the issue of IPV among women with disabilities, not only can specific psychosocial interventions be developed to support the complex trauma recovery of this population, but large-scale political advocacy can also be achieved through a more comprehensive understanding of the factors that contribute to this social injustice. Indeed, the foundational awareness that oppression among women with disabilities, which in its most heinous form includes IPV, is the result of society’s attitudes toward disability has the potential to change the prevalence of complex trauma among the population. This impact, furthermore, can occur through community-, state-, national-, and global-level initiatives to reduce the social isolation that is also prevalent among women with disabilities and a major risk factor for IPV.
Examining Other Theories
Bronfenbrenner’s bioecological systems model is another useful theoretical paradigm for research related to women with disabilities experiencing IPV, as the framework compliments critical disability theory and feminist disability theory. Nelson and Lund (2017) have already applied the model to women with disabilities who have experienced IPV and have also connected the framework to social isolation. Before delving into their findings, the researchers explained that Bronfenbrenner’s bioecological systems model was developed to explain how people mature and change in response to various socioecological systems (Nelson & Lund, 2017). Some of these systems include family, which depicts a microsystem; government, which functions as an exosystem; and cultural norms/values, which produce a macrosystem. Nelson and Lund (2017) then described several proximal processes—or enduring forms of interaction—that promote the disconnect between women with disabilities and their social systems, which in turn perpetuates their experience of IPV. This defends the idea that social support could decrease the isolation experienced by women with disabilities and, as a result, help them out of IPV.
The fundamental principles of the bioecological systems model illustrate the bidirectional influences of the various socioecological systems with which people interact every day. For example, a woman with a disability interacts with her family (whomever that may include), her workplace (if she is employed), potentially her spiritual congregation, her local community, and the larger political network (i.e., government), and likely with unique methods that accommodate her abilities. These systems, in turn, affect the woman’s daily experience. What this model does not highlight, however, is that women with disabilities are one of the most vulnerable populations. Moreover, the theory does not consider that not all women with disabilities have strong connections with their family, are employed, attend a place of worship, and so on. Critical disability theory and feminist disability theory together spotlight the issue of increased vulnerability by focusing not just on the stigmatization experienced by people with disabilities in general, but also on the stigmatization experienced specifically by women with disabilities.
Multiple other models have been used to conceptualize disability in previous research. Among these other models is the medical model (as noted), which identifies disability as a disease needing to be cured; the social model (also noted), which identifies disability as a social construct; the identity model, which is similar to the social model but claims that disability is a positive identity; the human rights model, which identifies disability as a social justice issue and, therefore, informs policy related to disability; and the economic model, which focuses on the challenges with labor and employment that often accompany disability (Retief & Letšosa, 2018). Fortunately, society has progressed far enough past the medical model that people with disabilities are much less often institutionalized immediately after a disability is observed. Nevertheless, while each of the subsequent models addresses important components of the experiences of people with disabilities, none of them is comprehensive. To that effect, critical disability theory combined with feminist disability theory is herein proposed to be the most effective model for comprehensively conceptualizing disability. Moreover, with the addition of complex trauma theory, critical disability theory and feminist disability theory are the most culturally competent frameworks for the theoretical explanation and academic investigation of IPV among women with disabilities.
Additional Applications
What makes the combined theoretical approach even more unique is the opportunity to apply these theories through participatory action research (PAR) and narrative theory (and by extension, narrative therapy), which can be used to create rich and profound qualitative data. Chevalier and Buckles (2019) described PAR as “collective reasoning and evidence-based learning focused on social action” (p. 4). The authors further explained that PAR involves the people on whom research is focused, rather than simply conducting research on or for people without their engagement. Other proponents of PAR have catch-phrased the method as “nothing about us without us.” Accordingly, PAR is notably applicable for future research and policy development addressing women with disabilities experiencing IPV, because arguably no one knows better about their challenges and complex trauma needs than the women themselves. Partnered with social work researchers, community organizers, and political advocates, PAR could further support the recovery of women with disabilities who have experienced IPV through the process of their own sociopolitical empowerment.
Puckett (2016) has defined narrative theory as “an effort to understand particular narratives in relation to assumptions and expectations that govern either some kind of narrative or narratives in general” (p. 1). Most societies have an ingrained narrative of disability. By a certain age, children develop a seemingly innate understanding of what “normal” bodies look like and how “normal” people behave, standards that perpetuate into adulthood. Any corporal vessel that diverges even slightly from those societal standards, any person who appears even slightly different from the norm, is perceived as less than and typically treated accordingly. What if women with disabilities—more specifically, women with disabilities who have survived IPV—had a platform to share their own narratives, their own stories of survival, to figuratively rewrite the socially imposed script of what it means to be a woman with a disability recovering from complex trauma? A theoretical framework that has applications for PAR and narrative theory would further advance that justice.
Relevance to Social Work Practice
Utilizing a combination of critical disability theory, feminist disability theory, and complex trauma theory—with the integration of PIE and intersectionality—to address IPV among with disabilities is strongly related to social work practice on the micro, mezzo, and macro levels. In addition to direct practice (e.g., psychosocial interventions, resource brokering), the knowledge resulting from additional research informed by these theories could have implications for health policy, including violence prevention; community organizing; and, of course, the disability rights movement. Expanding on these connections to social work practice, Quiros and Berger (2015) have argued that, in order for service agencies to be authentically trauma-informed, agencies must be aligned with the mission of social justice on which the social work profession is founded. Service agencies must also consider structural and environmental factors when assessing the trauma of those they serve, which includes trauma experienced in interpersonal and sociopolitical contexts (Quiros & Berger, 2015). Indeed, not only is trauma-informed practice an integral treatment model that promotes social justice, it is a practice that has evidence-based support as an effective intervention for women who have experienced IPV (Taft et al., 2016).
Crenshaw (1989) developed the concept of intersectionality to describe the sociopolitical experiences of being both a woman and Black. This concept has equivalent and profound applications for women with disabilities. Indeed, further layers of intersectionality occur for racialized women with disabilities, Indigenous and immigrant women with disabilities, 2SLGBTQ+ women and gender nonconforming persons with disabilities, older/aging women with disabilities, and other subgroups. Ortoleva and Lewis (2012) have commented on the intersection of SES and age (i.e., gerontology) among women with disabilities. Complementing the work of Ballan and Freyer (2017), Nosek et al. (2001) found that poverty and unemployment significantly reduce the opportunities for women with disabilities to escape IPV. Accordingly, while knowledge gaps still exist, this research has helped to elucidate the intersectional experiences of women with disabilities, which are highly relevant to current and future social work practice.
Research related to the experiences of women with disabilities is moving toward an orientation that is more inclusive of the PIE framework and the concept of intersectionality. Researchers, furthermore, are increasingly involving women with disabilities in the research on their experiences, thereby engaging the tenets of PAR. When combined, these theories, models, and frameworks, along with the unique and invaluable perspectives of women with disabilities themselves, have the potential to combat the major social injustice reflected by the lack of specialized support for women with disabilities who have experienced IPV, which is precipitated by insufficient knowledge of their multivariate experiences. These knowledge and intervention gaps are a social justice issue because they are the compounded results of ableism, sexism, racism, ageism, heteronormativism, classism, and other forms of discrimination, as both conscious and unconscious processes. Addressing the lack of support for women with disabilities, therefore, will mitigate the social, political, and economic injustice that is inherent in their life experience.
In sum, research on the experiences of IPV among women with disabilities has multiple implications for social work practice. While the implications for direct practice are more obvious (i.e., developing effective psychosocial interventions with individual or groups of women with disabilities who are recovering from the complex trauma of IPV), change can also be affected at the macro level of social work through political advocacy. Summoning the feminist argument that “the personal is political”, the utopian goal is to utilize the results of existing and future research on the contributing/risk factors and complex trauma outcomes of IPV among women with disabilities to inform new local, state, and federal policies that increase systematic protections for this special population. Women with disabilities are among the most vulnerable people all over the world; therefore, their exposure to IPV is a global injustice. Moreover, the most effective efforts to change this social justice issue must be founded on cogent theoretical models—namely, the proposed synthesis of critical disability theory, feminist disability theory, and complex trauma theory.
Accordingly, the overall recommendation for social workers is to learn and implement the theoretical paradigms and intervention frameworks that are effective for advancing the social justice of women with disabilities who have experienced and may still be experiencing IPV. Furthermore, social workers are encouraged to engage in policy practice and research in order to support the local, state, national, and global justice of women with disabilities. Involving women with disabilities, at all their levels of ability, in these advocacy efforts is crucial. The perpetual vulnerability of women with disabilities to IPV, and the prevalent complex trauma they endure as a result of IPV, will not lessen until much greater understanding of the population’s history, ongoing stigmatization, intersectional experiences, risk factors for recovery, protective factors for prevention, unique support needs, and physical barriers is achieved through theory-driven research and research-based policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.