
Abstract
The majority of sex workers are mothers. Although participation in sex work is primarily driven by the prioritization of their children’s needs over their own, mothers are stigmatized, subject to poorer health, and lack access to quality health care and social services. Interviews with 25 mothers in Mumbai, India, were analyzed using theory-driven coding to reexamine participation in sex work in context of Gilligan’s three-stage ethic of care, a feminist theory of moral reasoning. Stage 1 (decision making focused on self) themes were (a) sex work served as a means to survival and (b) exploitative and unfulfilling relationships required a focus on self. The transition from Stage 1 to 2 theme was language of selfishness versus responsibility. Stage 2 (selflessness is goodness) themes characterizing the majority of narratives were (a) sex work is justified, (b) duty to prioritize care of others, and (c) self-sacrifice to achieve aspirations for children. The transition from Stage 2 to 3 had one theme: consideration of self. While Stage 3 represents women taking holistic care of themselves and others, the data did not reflect this. Reframing mothers’ participation in sex work using the ethic of care framework may support destigmatization, decriminalization, and security of human rights.
Background
Globally, most sex workers are mothers (Sloss & Harper, 2004; Willis et al., 2016). Mothers who are sex workers commonly experience violence, stigma, marginalization, and separation from their children, families, and broader society (Basnyat, 2014). Stigma—deeply tied to perceptions about morality and the choice to participate in sex work—limits sex workers’ ability to access to health care and social services (Basu & Dutta, 2011; Praimkumara & Goh, 2016; Wahed et al., 2017). More specifically, sex workers report multiple physical and mental health symptoms and conditions that often go unaddressed. For instance, concerns have been documented about communicable diseases (e.g., respiratory and sexually transmitted infections, tuberculosis, malaria, HIV), reproductive health (e.g., miscarriages, perinatal bleeding, and abortion), hunger and malnutrition, physical abuse and rape, substance abuse, and symptoms of depression and anxiety (Kaloga et al., 2019; Pardeshi & Bhattacharya, 2006). When sex-working mothers do access health care, they often experience discrimination and receive a lower standard of care (Duff et al., 2015; Ryan et al., 2019; Scorgie et al., 2013).
Despite such maltreatment, mothers who are sex workers continually point to this work as a means to provide better lives for their children. In doing so, sex-working mothers routinely prioritize the needs of their children above their own. For instance, sex workers—frequently subjected to violence in the workplace—may be more likely to participate in unsafe sex and related high-risk behaviors when they are mothers who have the financial responsibility to provide for their children and families (Reed et al., 2013). Additionally, sex-working mothers are more likely to prioritize making money over addressing their own health-related concerns or accessing medical care when it is needed (Basu & Dutta, 2011).
Previous research has shown that some sex-working mothers are motivated by aspirations that their children will have better lives, become educated and employed, and grow their families (Basu & Dutta, 2011; Dalla et al., 2019). In order to support these goals, mothers frequently use their wages to provide for their children’s education in addition to basic survival needs (Praimkumara & Goh, 2016). Although society often labels sex-working mothers as “bad” because of their vocation (Basu & Dutta, 2011; Dodsworth, 2012), mothers’ actions help improve the likelihood that children will become formally educated and economically independent.
Sex Work in Kamathipura
Gezinski & Karandikar (2013) explain that Kamathipura is a well-known red-light district in Mumbai, India, that first developed in the early 1800s to entertain British soldiers stationed there. After India gained its independence in 1947, the red-light area continued to operate, this time by brothel owners and sex workers themselves. While sex work and sex trafficking are illegal in India, sex work remains the primary economic focus of the area, and in addition to those from India, many sex workers are trafficked from other parts of Asia (e.g., Bangladesh, Nepal) to work in Kamathipura. While Kamathipura used to be one of the largest red-light districts in Asia, home to approximately 30,000 sex workers in 2002, efforts to redevelop the area and curb human trafficking and sex work have resulted in a dramatic reduction to approximately 2,000 sex workers in 2012 (Gezinski & Karandikar, 2013; Kaloga, et al., 2019; Borges & Fernando, 2016).
Much research on sex work in Kamathipura has focused on gender-based violence and HIV prevalence, intervention, and prevention (Karandikar & Prospero, 2010; Gezinski & Karandikar, 2013; Silverman et al., 2014). This research addresses an important gap in our understanding of the unique experiences of sex workers who are also mothers in Kamathipura. More data are essential to advocate for targeted policies and programs that provide culturally sensitive and effective health and social services to meet the needs of sex workers and their children.
Theoretical Framework
Carol Gilligan (1977), a feminist and social psychologist, was the first to formally theorize that women and men were socialized differently in terms of moral reasoning and related decision making. Whereas Lawrence Kohlberg—an American psychologist well-known for his theory of moral development based upon research on White, male participants—concluded that men are more likely to make decisions motivated by personal autonomy, individual achievement, and clear ideas about right and wrong (an ethic of justice), Gilligan (2003)—Kohlberg’s former student—observed that women more often made decisions motivated by the influences of and effects on important relationships in their lives (an ethic of care). The ethic of care refers to the idea that the self and others are interdependent. As women and girls are socialized to maintain caring relationships and responsibilities to others, these powerful beliefs and practices carry over into decision making. As a result, it may be more common for women to make decisions to preserve significant interpersonal relationships with others even at the expense of their own individual well-being.
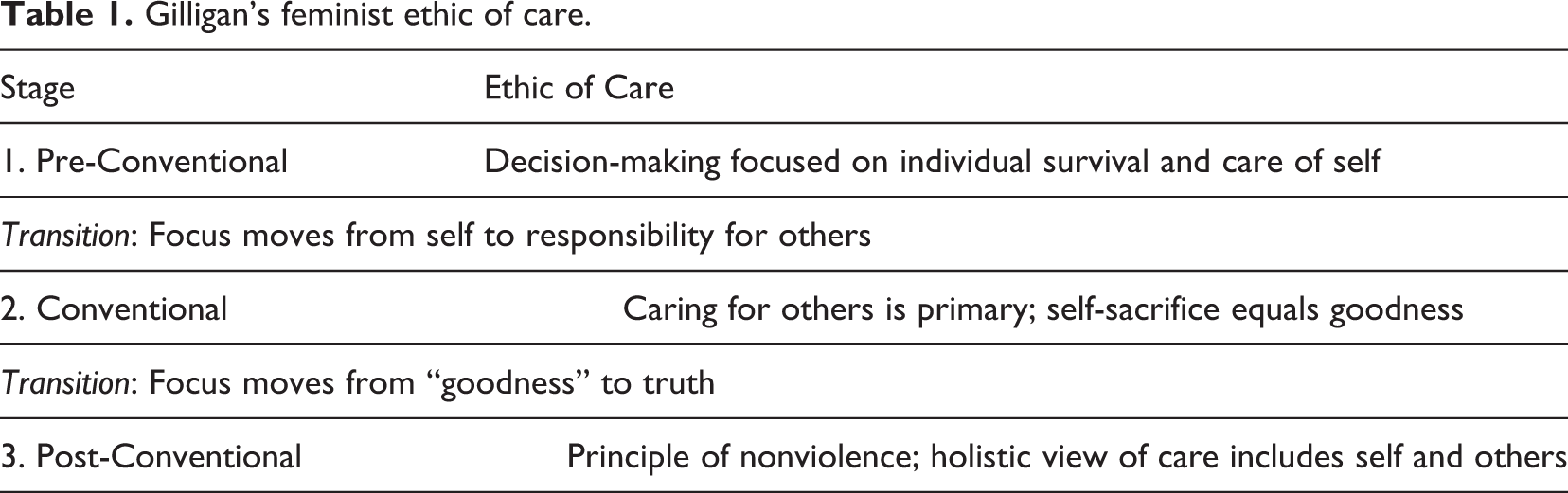
In her seminal text, “In a Different Voice,” first published in 1982, Gilligan (2003) describes women’s moral development as illustrated through three stages (see Table 1), which were developed as the result of qualitative work with female participants who were thoughtfully contemplating a hypothetical situation about whether or not they would choose to terminate their pregnancies. In Stage 1, self-interest and personal survival drive decision making. In transitioning from Stage 1 to 2, the individual begins to consider others in relation to the self. Stage 2 is characterized by a belief that sacrificing one’s needs in order to prioritize others’ needs equates to goodness and moral behavior. Women often find personal fulfillment, and thus reinforcement, in meeting others’ needs. In the transition from Stage 2 to 3, however, one begins to reconsider and question the relationship between selfishness and responsibility. Finally, Stage 3 represents a mature and holistic view of care that emphasizes a balance of care for both the self and others. The stage-based nature of the theory assumes that moral development is sequential and progressive. Further, in a male-dominated society, the ethic of care is traditionally devalued and deemed subordinate to the ethic of justice.
Gilligan’s feminist ethic of care.
While recognizing Gilligan’s contributions to expanding viewpoints regarding the process of individual development, Miller (1991) suggests that the ethic of care is Western-focused and diminished by not attending to the cultural context of moral decision making. This point is well taken and is important to state that Indian culture is collectivist in nature, which may influence the theory’s application in this context. However, it is also possible that sex workers may be an exception to the collective identity, particularly for those in the red-light area of Mumbai where sex work is considered immoral, yet legal. These workers are not legitimized, unionized, or organized to advocate for themselves (as opposed to other red-light areas of India, such as Kolkata). Due to social ostracism, they live isolated lives on the margins and may have no recourse but to become more individualistic.
While some feminist literature advocates that an ethic of care approach be used broadly to challenge structural inequalities and correct social problems (Held, 2014; Robinson, 2006), this approach has not been applied to sex work. Furthermore, because participation in sex work is largely perceived as a choice and sex workers are most often judged as immoral, we chose to understand whether an ethic of care lens would be helpful in analyzing mothers’ narratives. Finally, Gilligan’s ethic of care has not been used to examine decision making among sex workers internationally.
The Present Study
This study explores motherhood in the context of sex work in Kamathipura’s red-light district in order to reduce stigma. Reconceptualizing mothers’ decisions to participate in sex work through an ethic of care theoretical lens may change perceptions of sex work and allow for its acceptance, with the ultimate goal of improving sex workers’ overall well-being. Sex-working mothers navigate dual roles as sex workers and mothers, experiencing a layered stigma (Dodsworth, 2012; Sloss & Harper, 2004). Although much has been written about the harmful stigmatization and maltreatment of sex workers, little research has proposed the means to reconceptualize the cultural and societal perceptions of sex work, particularly in the context of motherhood (Benoit et al., 2018). Narrative research can help promote change and challenge misunderstandings about sex work that lead to its stigma and criminalization.
Research Question
This research is part of a larger qualitative study investigating sex workers’ reproductive and maternal health needs, infant feeding practices, and partners’ influence on health care decisions from two different cities in India. We used a narrative approach to examine pregnancy and motherhood among sex workers in Mumbai. In doing so, we aimed to answer the research question: How is a feminist ethic of care (Gilligan, 1977) reflected in the narratives of mothers who are sex workers? Taking the vantage point of the theory, we sought to analyze whether and how mothers participated in sex work to meet basic needs, preserve significant relationships, and fulfill responsibilities to others (most notably their children), even if it came at the expense of their own well-being.
Method
Participants
The sample consisted of 25 adult women who identified as female sex workers (FSWs) in the Kamathipura red-light area of Mumbai, India. Some lived in the brothels; others traveled to the area for work. The participants had been working as sex workers for an average of 15.44 years (range: 6–34 years). Approximately half of participants reported being trafficked into sex work. Participants’ mean age was 34 years, and all were mothers. More than half had their children while working as a sex worker (52%), 40% were single, and 28% were widowed. See Table 2 for demographic information about the women in the sample.
Participant Characteristics.
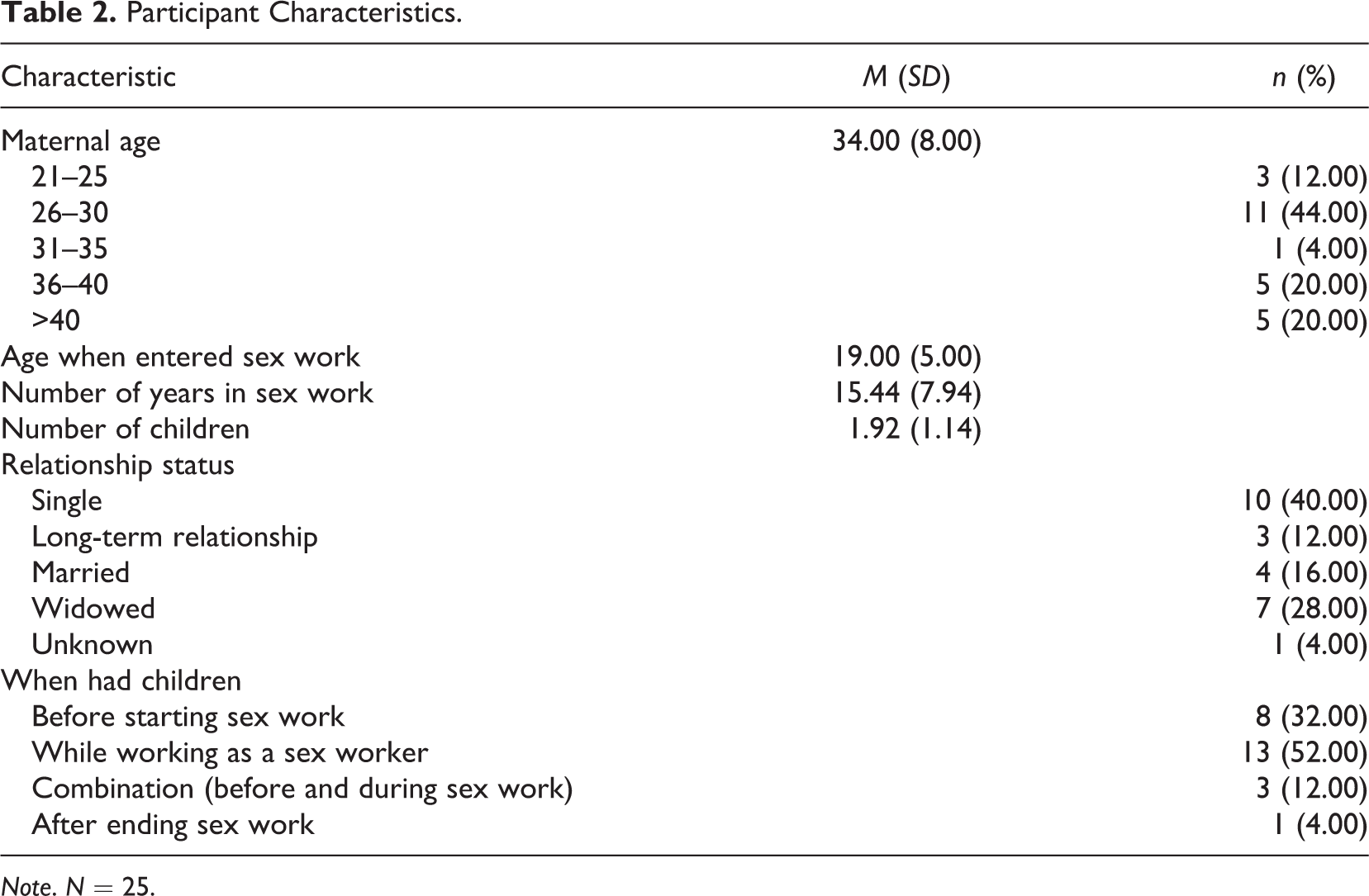
Note. N = 25.
Data Collection Procedures
Informed by a narrative approach (Riessman & Quinney, 2005; Sandelowski, 1991), the second author completed in-depth, semistructured interviews with participants. She has worked as a social worker with FSWs in India and has conducted prior research with the population. After receiving institutional review board study approval from The Ohio State University, the second author conducted daily field visits in Kamathipura for 2 weeks in December 2018 to establish rapport with FSWs, discuss the purpose of the research, and complete individual interviews. After this initial point of contact, snowball sampling was used to recruit participants until saturation was reached. Saturation was determined by the second author who continued a few more interviews after beginning to see patterns in responses and no new emerging information.
Only FSWs who contacted the second author and who voluntarily consented to take part in the study were interviewed. The majority of participants were unable to read and write. Therefore, the consent form was explained verbally to each respondent prior to the interview. Participants gave verbal consent and chose a pseudonym—by which they are referred throughout this research—and interviews were then immediately conducted in participants’ location of choice, most often in the brothels where the women worked and/or lived. Each respondent received Rs. 500 (approximately $8) for participation. The incentive amount was based upon the second author’s previous experience and as a result of discussions with professionals and researchers who have conducted similar research in Mumbai. Interviews were conducted in Hindi and were audio-recorded with participants’ permission.
Interviews lasted from 1 to 3 hours and focused on mothers’ stories relevant to sex work in the context of maternal and sexual health, infant feeding, and mothering. While participants were not explicitly asked about their moral decision making, moral decision-making practices emerged as a key theme in participants’ responses to questions about how and when the women entered sex work, their experiences of becoming a mother for the first time, and their ultimate desires for their children. The second author translated and transcribed the interviews into English and maintained a detailed audit trail during the data collection and transcription and translation process, including a journal to check for reflexivity and to maintain rigor in this qualitative study.
Data Analysis
The first author uploaded all transcribed interviews into NVivo 12 Plus for Windows (QSR International, 2018) for data tracking and analysis. Demographic attribute data and sample characteristics were recorded first to increase familiarity with the overall sample (Saldaña, 2015). All the authors repeatedly read through the transcribed interviews to fully grasp the meaning of participants’ experiences and to begin to recognize key concepts and topics that recurred across narratives. Additionally, memos on coding decisions and reflections on reviewing the transcripts were written by the first and the second author and discussed with all the authors of the study.
The ethic of care framework was applied by the researchers during the data analysis phase. Theory-driven coding was applied to analyze the data. Theory-driven coding is an iterative process whereby a codebook is generated based upon theoretical concepts, and codes are reviewed and revised throughout examination of the theory in context of the data (DeCuir-Gunby et al., 2011). The first author created a spreadsheet with key concepts and general descriptions representing each stage of Gilligan’s ethic of care. She then independently coded the transcripts line-by-line and established initial codes and a codebook. Throughout coding, there was continuous referencing between the transcripts and the theory spreadsheet to more readily recognize representations of the theory in the data. After initial coding was completed, data were organized into primary themes and reviewed for the frequency in which participants made relevant comments to the codes under inquiry. The research team met periodically to provide peer debriefing and critical reflection on findings. Final themes were chosen after group discussion. Themes were organized using the stages of the theory as overarching categories.
Findings
Overall, study participants identified numerous challenges related to pregnancy and mothering in the context of sex work. Some participants reported pregnancy and childbirth-related complications such as weakness and bleeding. Many participants reported unplanned pregnancies and histories of miscarriage and abortion. Furthermore, many experienced pregnancies while under conditions of extreme poverty (e.g., lack of food, shelter, and basic necessities) and violence. About half of the participants reported experiencing physical and sexual violence by partners, family members, clients, and brothel owners. Finally, the majority of participants had a very limited understanding of prenatal care needs or recommendations or of reproductive health and family planning options.
Key Themes
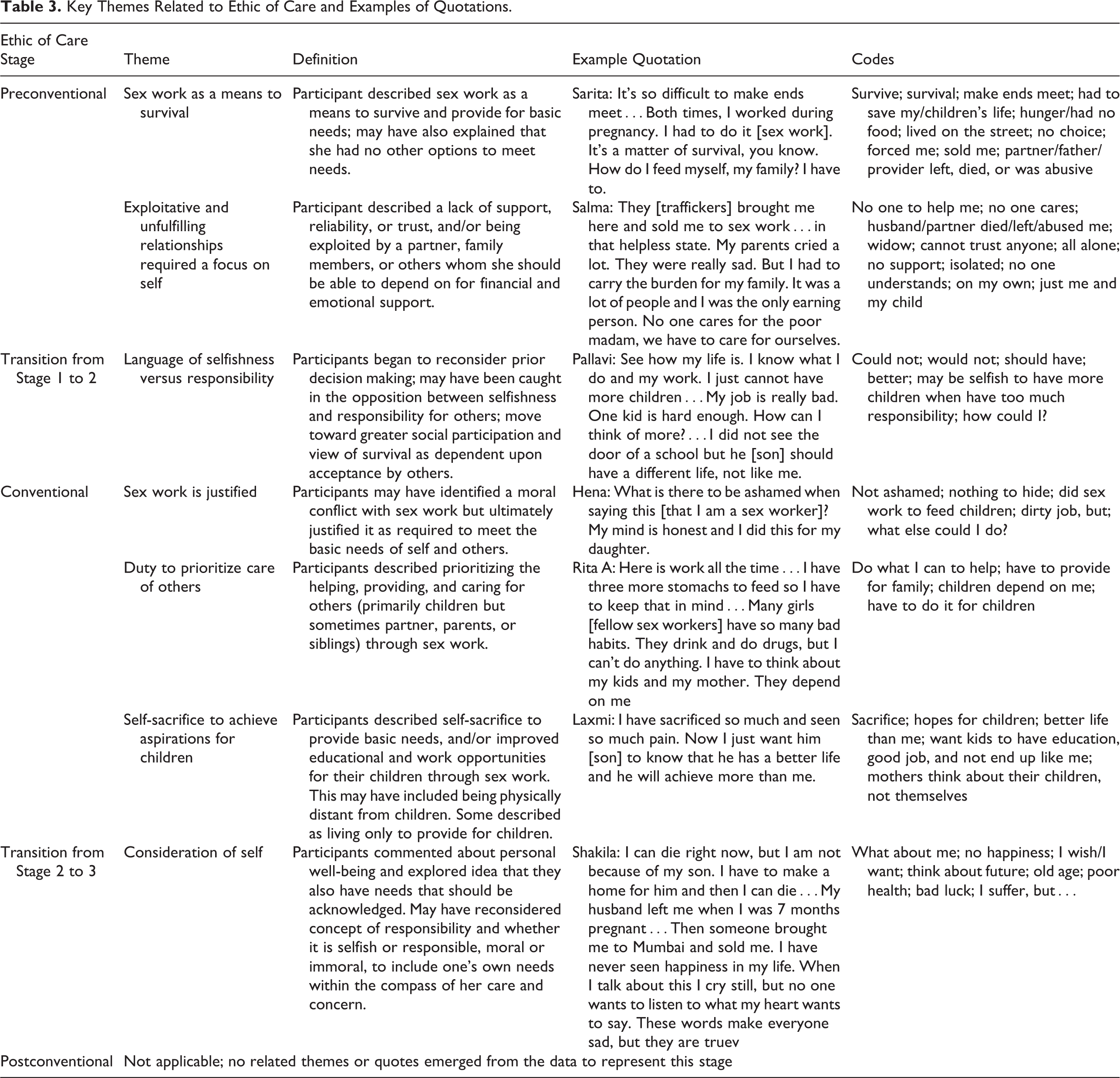
Participants’ narratives reflected several stages of the feminist ethic of care. We used the stages of the ethic of care framework to organize the critical themes that emerged from our analysis. See Table 3 for the key themes and their definitions, alongside each corresponding stage of the theory, and example quotes and codes that characterized the theme.
Key Themes Related to Ethic of Care and Examples of Quotations.
Stage 1: Preconventional
In their narratives, the majority of participants made remarks emblematic of the first stage of the ethic of care, which includes a need to focus on the self and make efforts toward survival. Comments were indicative of the sense of powerlessness and disconnection from others that women often describe in this stage (Gilligan, 2003). Two themes emerged under the Stage 1 category: (a) sex work as a means to survival and (b) exploitative and unfulfilling relationships that required a focus on self.
Sex work as means to survival
Participants described needing to participate in sex work to physically survive and meet basic needs for self and family, most often one’s children. Most participants first entered sex work and continued in sex work because of extreme poverty and the inability to meet basic needs for shelter, food, and clothing. Many were forced and sold into sex work by family members and friends. Describing how extreme poverty led her to engage in sex work, Salima stated: I was left on the street. I had to beg for money or work in some odd jobs with my daughter. So, people would talk and say bad words to me and take advantage of me. One man tried to rape me when I was sleeping on the street at night. My life was horrible. So, I came here [brothel]. I decided I will now work where at least there is money. My mother’s brother brought me here and sold me to a brothel when I was 10…and here I am still…I cried a lot and protested, but I had a lot of money to pay back so I started doing this work. It was not my choice.
Frequently, participants shared that illness or death of family members or husbands led to a family’s inability to make ends meet and pushed them toward sex work. Sex work was credited with participants’ ability to survive and secure basic needs. As Rita explained: I had two children and my husband had a heart attack and died…Then what do you do? My life is over, but I had to save my children’s lives, so I came here. I am here because my husband was a drunkard, and I had two children to look after. I could not have done it without a job. This is dirty job for some women, but for me, it saved my children. My life.
Exploitative and unfulfilling relationships required a focus on self
This theme characterizes participants’ descriptions of adult relationships as generally unreliable and sometimes abusive. Participants explained that they were often maltreated by parents, siblings, partners, and friends—those with whom they expected to have the most trust. Participants described being trafficked and abused by loved ones. For some participants, this experience began while they were children. Sarita explained being trafficked as a young child, by her aunt: I am here from my childhood, right from when I was 10 years old. My aunt brought me here by deceiving my parents…She brought me here and did the devadasi ritual [women considered given in marriage to God]…Because of this my parents did not allow me to go back to their home again. I lived with my aunt from 10–12 years…She took all my earnings and I would do dhanda [sex work]…We worked but never got any good treatment. How many years could I have continued with her? So, I ran away…
After describing disappointing relationships with her husband (who had been her client) and other sex workers, Nisha said “I cannot trust anyone anymore.” Unfulfilling relationships were sometimes the result of violence, illness, or death of a parent(s) or partner. Additionally, many participants described significant grief related to the loss of loved ones. Anji described her hopelessness after her partner died: My admi [partner] died when I was pregnant…There was so much poverty, no proper clothes to wear, no shoes, no food, sometimes no roof over our head. Both my parents were not there. What is the future for an orphaned girl? I wish I had a big brother. I would have had some support in my family. I got beaten up a lot in my life…They always lied to me. The madam, the pimp, even the other girls…I have to give money to my parents and child. Here I still feel isolated. Even if I am sick here, no one will ask me.
Transition from Stage 1 to 2
Some participants alluded to a conflict between making decisions solely for oneself and making decisions based upon the needs of others. This was indicative of the transition between the first two stages of the ethic of care. We identified the language of selfishness versus responsibility as a key theme representing this shift.
Language of selfishness versus responsibility
This theme symbolizes the movement participants described from considering one’s own survival needs to placing increasing emphasis on the needs of others. Conflict existed between making a decision for personal benefit or based on one’s individual desire (e.g., to get married, to have more children, to leave sex work) and what was perceived as best for their children. Devi described having to prioritize her children’s needs over her own: After I started work, I got several regular clients. They gave good money and it was alright. One of them wanted to get married also, but I said no. I had my own kids to worry about. How could I even think of other men? I had one miscarriage after coming here…when I went to the clinic, the doctor said I was pregnant and then lost it…But what happened is for good. My friends all said it’s for good. I cannot support my own self and my family. How can I keep another child? See how my life is?…I know what I do and my work. I just cannot have more children…My job is really bad. One kid is hard enough. How can I think of more?
Stage 2: Conventional
The majority of participants’ comments were coded under Stage 2, where others’ needs and concerns are prioritized over one’s own. Participants routinely described relinquishing their personal wants and needs when they came into conflict with others’ needs. Furthermore, according to the respondents, prioritizing others was expected—and even associated with proper behavior. Likewise, good intentions potentially eclipsed any dishonorable associations with sex work. We identified three key themes under this category: (a) sex work is justified, (b) duty to prioritize care of others, and (c) self-sacrifice to achieve aspirations for children.
Sex work is justified
Despite recognizing that sex work may be viewed by others as unethical, some participants stated that sex work was defensible and honest work because it provided for the needs of self and others that could not be secured otherwise. In fact, some staunchly affirmed their decision to be a sex worker because of their pure intentions. Sarita explained that sex work allowed her to feed her family: This work has given me money. Why should I deny this? Yes, this [sex work] is dirty and the area is bad, but this work feeds us. So, I am back on the street selling sex. I am telling you the truth. What is there to hide? I have to feed my child and me, send money home. I have to do this.
Additionally, participants received some satisfaction in the recognition that their work was able to provide for their children. Salima described the pride she feels when she is able to send money for her daughter: Even when life is so, so hard, there is peace in this. In knowing that money is going to her [daughter]. I go and meet her, see her and my sister, and I become happy. They are able to live because of the small money I give them. That is the only thing that keeps me going.
Duty to prioritize care of others
Participants unanimously described an obligation to care for others—most often their children, but this sometimes also included care for partners, parents, and siblings. Financial earnings through sex work allowed participants to provide for their loved ones, their first priority. Sanika explained the precarious position she was in after her husband died, that sex work helped alleviate: …after he [husband] died, everything was over…When the baby was born I took him to my mother…I left and came here [Kamathipura]. It was difficult for me, but the money was here so I came here. I had to carry the burden for my family. It was a lot of people [parents, 12 siblings, and 4 children] and I was the only earning person…they [my children] always come first. I met my admi [partner] who was my client. He even took me to his house and told me to leave sex work. But I had to feed my family my brothers and sisters, so I told him I will just continue work and keep him and his family happy and my own brothers and sisters also happy. (Rekha)
Duty to prioritize care of children also extended beyond biological children as well. Two participants cared for children they adopted. One respondent chose to raise a child she found abandoned on the street. Another was caring for her deceased sister’s two children in addition to her own.
Self-sacrifice to achieve aspirations for children
In addition to meeting children’s basic survival needs, participants described sacrifice through sex work as a means to secure a better future for their children. Participants explained that earnings via sex work allowed for children’s improved educational opportunities. Some used earnings to pay for private schooling. Participants aspired for their children to receive formal education, job training, and work opportunities—things they had never received themselves. In our interview with Nisha, for example, she described feeling pride in recognizing that her self-sacrifice was leading to better life circumstances for her children: I have been in this area for the past 20 years. I have two children. My daughter is 19 and my son is 18. Both of them are back in Calcutta and going to college. I think this is my biggest achievement. I sacrificed a lot in life only to make sure they go to college. They should have good life partners and get married. That is my desire. I hope their life is better. I only think about my daughter, not about me. What I have in life is not good. I want only her marriage to be good, a good job for her. So that is all I want…No women will think about herself. She will always think of her children and nothing else…I miss her [daughter] day and night, but all I do is for her. What is there in life other than this? My kids don’t come here…Even though it was really difficult for me [sending children to live with family away from her], they [family] saved the boys. The boys growing here have bad influence. As their mother, I wanted them to have a good life. What happened with me I cannot let happen with them.
Some respondents suggested that their mere existence was predicated on providing for their children. Nisha said, “My two children are my life. I live because of them. If they were not there, I would not have any reason to live.” When explaining that her only child was now grown, married with children, and working as a nurse, Amma said: “Now I have no hopes and aspirations.”
Others referred to their sacrifice to provide for children through sex work as a kind of death of the self—both literally and figuratively. Deepa experienced many physical and mental health struggles that may have resulted from sex work: My own health is really bad. I have so much weakness. I feel sleepy all the time and don’t feel like doing anything. I have HIV and I know I may not have a long life, but that’s why I just want my son to be okay. If he is okay, I am free to die. I can die right now but I am not because of my son. I have to make a home for him and then I can die.
Transition from Stage 2 to 3
The fewest number of codes were attributed to the shift between Stage 2 and 3 of the ethic of care theory, where individuals begin to acknowledge the limits of self-sacrifice and consider the possibility of simultaneously balancing personal needs with others’ needs. In the context of participants’ narratives, the one theme that emerged representing this stage was consideration of self.
Consideration of self
During this phase, the authors observed that participants began to question their futures and express concerns for their own health and longing for happiness. Participants expressed sadness, grief, and disappointment about their lot in life. Rather than purely focused on survival needs or others’ needs, participants—for the first time—reflected on their own. While identifying their personal suffering, most nevertheless referred back again to the need to continue sex work to provide their children with a better life than they had. For instance, Deepa shared how stress was affecting her: My life is bad because my luck is really bad. Now, I hope at least my children are okay. They don’t have the bad luck like me…I have too much tension in life. I have so much stress. I have just all these thoughts in my head all the time. If I think of how my health is so bad it gives me so much stress. I have to think about my future. About my old age…I have lot of knee pain, but that is because of my weight…I just want to go back home…Only right now I can’t. I still have work, now after my work is done, I will go.
A few participants commented on using substances—food, alcohol, and/or drugs—to self-medicate the emotional pain resulting from their work. In this way, participants identified that they had unmet needs but had to do subdue them in the best interest of others’. Salima stated: But, what about me? I was left on the road. Now I have to see clients, drunks from the road who have little money, sometimes no money. I have to entertain and have sex with them…but, what can I do? I really need it…Every time I have money I think of what can I eat and drink, what is good. But then I miss my daughter. What will she be eating? What can I tell you? This pain never goes away.
Stage 3: Postconventional
No codes, themes, or quotes emerged from the data that represented the postconventional stage of Gilligan’s ethic of care whereby individuals—in the practice of nonviolence—no longer sacrifice their own needs at the expense of others and attempt to balance the needs of both. While participants recreated their own version of balance in earning for the children and native families while making attempts to keep themselves healthy and safe in sex work, physical and or structural violence made it impossible for mothers to honor and equate their own needs on par with their children’s.
These larger structural influences—sexism, patriarchy, violence against women, cultural beliefs about sex work, and lack of economic security—that affect decision making may be a reason why participants’ narratives did not reflect the third stage of the ethic of care theory. Rather than signifying participants’ limited moral development, we argue that the participants were unable to move to Stage 3, which Gilligan (1977) considered to be the fully feminist way of thinking—a complete condemnation of violence and decision making based on what is best for both self and others—because social, cultural, and economic circumstances do not allow this. Many participants acknowledged the pain and sacrifice of sex work but felt they had no true choice about whether or not to participate. Doing so was a matter of survival and a resolution to do everything in their power to make things better for their children—in spite of their own banishment within a patriarchal society that devalues women. The authors suggest viewing this decision as a noble act of self-agency within an oppressive environment. Further, experiences and decision making unfold within the larger, dominant cultural context. Thus, a lack of findings relevant to Stage 3 may also be related to Indian culture’s conceptualization of individuals as interdependent beings who place increased value on a duty-based interpersonal moral responsibility over individualism and personal autonomy (Miller, 1994).
Discussion
This study analyzed sex-working mothers’ narratives in the context of Gilligan’s three-stage ethic of care, a theory of moral development. Findings determined that the first two stages and two-stage transitions of the ethic of care were illustrated through participants’ narratives. However, the final stage of the theory did not apply. What was most evident in mothers’ narratives was that the decision to participate in sex work was driven by their dedication to providing basic and educational needs of their children. Participants’ desire for their children to have a better life than they had led them to prioritize sex work over self-care.
As with previous literature on sex work, participants reported various health care barriers, food insecurity, violence, perinatal health complications, lack of safe childcare options, and breastfeeding challenges because of an immediate need to return to work (Gezinski & Karandikar, 2013, 2019; Sloss & Harper, 2004; Swain et al., 2011; Willis et al., 2016). Moreover, participants’ stories reflected a lack of support and rejection by family members and stigma associated with sex work, despite honorable intentions. Given societal conditions and lack of other employment opportunities, participants also described a fatalistic attitude about their own lives and future (Chakrapani et al., 2009). Participants’ acceptance of their bleak social and economic circumstances served as a significant barrier to honoring nonviolence toward the self and balancing one’s needs with those of others.
Thus, a conflict exists in describing participants’ agency in making the decision to participate in sex work. Guha (2018) acknowledges the dichotomous viewpoint in existing literature that tends to frame sex workers as either self-empowered agents or victims of their social environment. In line with previous findings, participants described a sense of resiliency, personal power, and fortitude in their decision to enter and continue in sex work as a legitimate means to provide financially for their families (Dodsworth, 2012; Praimkumara & Goh, 2016). Sex workers identify as mothers first and contend that it is their responsibility to care for their children ahead of their own needs (Basu & Dutta, 2011). In this way, their decision making was thoughtful and purposeful; rather than being victims, some participants described being active agents in their lives—making plans and working toward achieving life goals they had for their children (Praimkumara & Goh, 2016).
However, participants would not have first engaged in sex work if not for oppressive familial, cultural, and economic conditions that directly or indirectly forced them to consider this line of dangerous and stigmatized work. Similar to previous research of sex-working mothers in India, participants were often trafficked into sex work or chose sex work due to death and/or desertion by their native family members and/or partners, leaving them as single parents and sole economic providers for their (and sometimes others’) children (Basu & Dutta, 2011). While some participants powerfully stated their choice of sex work to provide financially for their children and family members, many continued to simultaneously hide their work from them, reflecting the far-reaching cultural and societal shame surrounding this work (Dalla et al., 2019).
Thus, while the ethic of care theory—particularly Stage 3—may have limitations in the context of motherhood among sex workers, Gilligan’s work is usefully situated within an understanding of the deep influence of patriarchy and demonstrates that an ethic of care (represented by love, relationship, and democracy) exists as a powerful counter to it. Creating political change in gendered spaces can be supported by a feminist ethic of care poised to examine issues of power and privilege through paying particular attention to those made most vulnerable. Moreover, it provides a tool in which to analyze the male-dominated causes of poverty that serve as a prerequisite to sex work.
This requires ongoing qualitative inquiry with sex workers whereby researchers and practitioners listen with inquisitiveness rather than judgment to the voices of those marginalized (Gilligan, 2014). This should include more research around stigma associated with sex work generally (Benoit et al., 2018) and sex work stigma in the context of motherhood. This study works toward this by reframing participation in sex work using an ethic of care framework, providing a new approach for developing empathy toward sex workers as a step toward reducing related stigma and criminalization and improving health.
The findings also have important implications for policy and practice aimed at improving the health and well-being of sex-working mothers. Findings may be used to develop and advocate for programs that serve to facilitate empathy among the broader community toward sex workers to reduce stigma and reframe sex work as a legitimate means of employment to provide financially for one’s family. If the public perceived mothers’ participation in sex work using an ethic of care lens, they may better understand mothers’ decision to participate as a simple means to improve the lives of children; over time, society may come to regard sex work as a vocation—chosen of necessity—as opposed to judging sex workers as immoral characters. This outcome requires a long-term commitment to ongoing research and social education about sex work, including improved understanding about the best modes of disseminating this information to the public. Ultimately, reducing stigma and decriminalizing sex work is needed to allow for access to quality health care and social services to better provide for the needs of sex workers and their children.
There is a need for effective social policy that is supportive of personal agency while simultaneously recognizing and dismantling systems and structures that create victimization and oppression (Chetkovich, 2004). Such efforts may include prioritizing harm reduction, such as through education, safety, improved access to health care, and activities to help normalize sex work as work and decriminalization (Karandikar, 2008; Benoit et al., 2018; Howard, 2018). These activities should be developed in collaboration with and for sex workers and other stakeholders including family and community members, nongovernmental organizations, and antihuman trafficking agencies. To create investment in these strategies, Ryan and colleagues (2019) suggest labeling sex work–related stigma as a social determinant of health negatively influencing access to quality health care that is free of bias and discrimination.
Limitations
The notion to investigate the application of the ethic of care to the mothers’ narratives occurred after data collection, upon reviewing the insights shared by participants. Because we applied the theoretical framework at the data analysis stage, this led to some limitations in our data collection process. For example, it is possible that the questions asked were not the best ones to assess the application of the theory to mothers’ reasoning about participation in sex work. Furthermore, for some mothers in the study, participation in sex work was not perceived as an ethical dilemma. It was simply a means of survival. For these participants, it is logical to argue that the theory and its implications for moral development may not apply. Gilligan’s (2003) work in interviewing U.S. women focused more on the psychological and spiritual survival of the self; in contrast, for these study participants, physical survival was at stake. Indeed, sex workers’ needs to focus on physical survival may preclude the privilege of moral developmental processes (Gezinski & Karandikar, 2013; Gilligan, 1977).
Conclusion
This study used theory-based coding to apply Gilligan’s ethic of care to the narratives of sex-working mothers in Kamathipura, a red-light district in Mumbai, India. Findings showed that moral decision making primarily occurred within the first two stages and transitions of the theory. None of the mother’s narratives fit the third, postconventional stage of the theory focused on finding a balance between one’s needs and those of others. In sum, most mothers stated that they participated in sex work—sacrificing their own health and needs—in order to provide a better future for their children. These findings do not represent participant inadequacies but are reflective of the patriarchal structures that maintain poverty and the lack of economic opportunity that fuels sex work.
Willis and colleagues (2016) issued a call to action to reduce stigma and secure human rights for sex workers. Reframing mothers’ participation in sex work using Gilligan’s feminist ethic of care—as demonstrated through this qualitative research—lends support toward this goal. Listening to mothers’ personal circumstances that lead them to participate in sex work can function a bridge to empathizing with them. Increased understanding and compassion for sex-working mothers is needed in order to destigmatize the work. Suggestions for future research include using an ethic of care to inform all aspects of study design to understand the experiences of sex workers in other contexts. Additionally, an ethic of care can be used in partnership with sex workers to develop and pilot interventions aimed to reducing sex worker stigma. Furthermore, recharacterizing sex work as an economic practice in which mothers participate to meet the needs of their children may provide support for the decriminalization of sex. Ultimately, improving perceptions of sex-working mothers and their decisions to participate in sex work can be a step toward societal inclusion and improved treatment, including access to supports, services, and equitable healthcare.
Footnotes
Acknowledgment
The authors would like to thank the mothers who generously shared their time and experience for the purposes of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.