
Abstract
This qualitative study explores South Asian immigrant women’s experiences of domestic violence, their views on help-seeking, and access to informal or formal sources of supports. Drawing from grounded theory approaches, this article focuses on one major theme, revictimization, which provides insights into the mistreatment and experiences of seven women who encountered challenges when disclosing abuse. Through an intersectional lens, this article examines how participants were revictimized and mistreated by people within and outside their own community including service providers who they trusted. Implications to reduce levels of mistrust for community members and service providers working with this specific population in Canada are discussed.
In recent years, research on domestic violence (DV) 1 has begun to capture the unique experiences of immigrant women in Canada, including South Asian (SA) women seeking help (Ahmad et al., 2009; Ahmad et al., 2004; Alaggia et al., 2009; Guruge, 2010; Shirwadkar, 2004). Yet little is written from the perspective of SA immigrant women with lived experiences of DV. Indeed, literature on SA women’s experiences of DV “is largely invisible, especially within Canada” (Chokshi et al., 2010, p. 155). Studies in Canada likewise remain limited to larger metropolitan cities such as the Greater Toronto Area and the Greater Vancouver region, even while many new immigrants have established themselves in the prairie provinces (Statistics Canada, 2017; see also Ahmad et al., 2009; George & Rashidi, 2014a, 2014b; Okeke-Ihejirika et al., 2018; Thandi, 2011).
This research contributes to scholarship on DV by examining the multiple interrelated challenges faced by seven SA immigrant women in Edmonton, AB, when reaching out for support. In line with previous studies, I apply the theoretical lens of intersectionality to analyze the interlocking systems of oppression from the community, professional agencies, and the dominant society, which I argue work to revictimize SA women (see also Sokoloff, 2008; Sokoloff & Dupont, 2005). The term revictimization means to victimize again instead of preventing further harm. Shankar et al. (2013) use the term double victimization to classify experiences in which SA women first encounter abuse from their spouse/family and then from mainstream service providers. I expand this concept, using the term revictimization to indicate secondary victimization from professionals within SA or mainstream organizations who share the same ethnic or religious identities as the SA women seeking support.
Importantly, this study distinguishes between informal and formal supports for DV (Ahmad et al., 2009; Barrett & St. Pierre, 2011; Guruge & Humphreys, 2009; Menjivar & Salcido, 2002; Okeke-Ihejirika et al., 2018). Informal support refers to the role family (including extended members), friends, coworkers, neighbors, and SA community members play in responding to DV disclosures. Informal supports can also include faith-based and community leaders who play a role in supporting abused SA women. Often, informal supports are first to hear about abuse (Ahmad et al., 2013; Guruge & Humphreys, 2009; Raj & Silverman, 2002b). Formal support refers to service providers from mainstream service organizations (MSOs) and South Asian women’s organizations (SAWOs) that also intervene in DV cases. Formal supports include social workers, shelter systems, health care services, police, and other professionals within the criminal justice system.
In what follows, I argue that disclosure of DV to informal and formal supports can work against SA women as it silences their voices, and to some degree, encourages the abuse to continue. First, I contextualize my research within the existing DV literature. Second, I describe the intersectional theoretical framework and grounded theory (GT) methodology I used to examine SA women’s experiences of DV in their own words. Thirdly, I share my analysis of participants’ experiences of revictimization as a significant theme emerging from the research findings. I also offer implications for best practices to prevent further revictimization when SA women disclose abuse regardless of venue. Finally, I call for additional research into the complexity of the concept of revictimization since more information is needed to understand the power embedded in informal and formal supports for DV.
DV in SA Communities in Canada
SA women are not a homogeneous group. There is significant variation across SA countries in terms of languages spoken, cultural experiences, rituals, practices, and customs. SAs are one of the fastest growing immigrant groups in Canada: By 2031, they are projected to be the largest visible minority group ranging from 3.2 to 4.1 million (Statistics Canada, 2010). According to Statistics Canada, the number of SAs in Canada rose to as many as 1,924,635, with the majority being foreign-born, accounting for 5.4% of the Canadian population (Statistics Canada, 2017). In this study, I use the term SA women to refer to those who have migrated from the top three countries of origin, namely, India, Pakistan, and Sri Lanka (Chokshi et al., 2010; Merali, 2009).
While activists continue to view DV as a serious problem within the SA diaspora in Canada, the problem remains largely hidden, in part because of a lack of appropriate support services (Shankar et al., 2013; Thandi, 2011). Nevertheless, demand for initiatives serving SAs is increasing in Canada (Chokshi et al., 2010). For example, Punjabi Community Health Services (PCHS4U) has expanded its culturally appropriate DV services from Toronto to Calgary and Ottawa. In Edmonton, key stakeholders have taken important steps to create awareness of DV at SA cultural and religious events. Through initiatives such as PARIVAAR, which formed in 2010, service providers, faith-based, and community leaders have worked together to positively impact perceptions of how the SA community responds to DV. The acronym PARIVAAR (meaning “family” in many SA languages) stands for Peaceful Alliance Rejecting Injustice and Violence and Advocating Respect. Such advocacy is needed as migration stress contributes to settlement experiences of DV and can influence disclosure for SAs. Thus, a strong rationale for research on help-seeking strategies has emerged in Edmonton in order to improve supports for SA immigrant families (Ahmad et al., 2009; Chokshi et al., 2010; George & Rashidi, 2014a, 2014b). To my knowledge, this is the first study examining SA immigrant women’s lived experiences of DV supports in Edmonton.
Unique Barriers in Reporting Abuse and Accessing Supports
Existing research on immigration and DV has identified unique barriers that increase women’s vulnerability to DV or impact disclosure (Alaggia et al., 2009; Dasgupta, 2000; George & Rashidi, 2014a, 2014b; Jayasuriya-Illesinghe, 2018; Menjivar & Salcido, 2002; Shirwadkar, 2004). Barriers that are well-founded in the literature include stressors from migration/acculturation, cultural norms about marriage, lack of language skills, economic dependency on the abuser/sponsor, lack of knowledge of immigration laws and policies, discrimination, and limited access to available services. As Shankar et al. (2013) found, SA migrants have left behind their family support networks, often have no trusted family members they can turn to for support and may be terrified of consequences such as ostracism from the community…if they talk about intimate partner violence or are seen accessing help. (p. 259)
A small body of Canadian scholarly work finds similar barriers in reporting DV. Ahmad et al. (2004) found that a significant number of the 47 SA immigrant women in their study held strong patriarchal beliefs. These interfered with women’s ability to recognize abuse and seek formal supports from health care professionals. Instead, they often approached friends and family. In a later study, Ahmad et al. (2009) explored reasons for and against seeking help from professionals. Their findings reveal that SA women experienced a wide range of reasons for delays in help-seeking such as social stigma and loss of supports after migrating. These studies focused on women’s experiences with health care professionals. SA immigrant women’s experiences with other informal and formal supports remain underexplored in the existing literature.
In Canada, little information exists on immigrant communities and DV due to a fear of negatively stereotyping newcomer groups (Alaggia et al., 2009). As Jayasuriya-Illesinghe (2018) states, “if [the] information is not gathered from all groups of immigrants, their experiences [will] become less visible than that of those who are included and help support a different and often culturally essentialist discourse about their issues of concern” (p. 345). To address this gap, this qualitative study focused on the unique issues that SA women in Edmonton encounter and how to inform culturally responsive supports in that city. Sokoloff and Dupont (2005) emphasize the need for culturally sensitive research, “giving voice to marginalized women” (p. 49) especially in the arena of DV, while identifying the need for attending to immigrant specific communities.
Theoretical Framework
Black feminist scholars such as Collins (2000) and Crenshaw (1991) conceptualize intersectionality as the mutually constituting oppressions that women of color experience in their lives. 2 Crenshaw (1991) applies intersectionality to emphasize the DV experiences of women of color and accounts for how gender and race are inseparable in such situations. To interpret the findings using an intersectional lens, I considered the following factors of oppression: isolation, patriarchal values in SA communities, dependency on abuser, language barriers, lack of support networks in Canada (e.g. family, friends, and community), institutional racism, and stereotypes. I also considered how social identities such as gender, race/ethnicity, culture, religion, and precarious status interacted to shape DV experiences and access to supports (Crenshaw, 1991; Menjivar & Salcido, 2002; Raj & Silverman, 2002b; Sokoloff & Dupont, 2005). Additionally, since some communities actively silence women and thus perpetuate violence, intersectionality helps us understand how power and privilege operate across different contexts.
Method
Although the literature on the SA diaspora and DV is emerging, voices of SA immigrant women are relatively marginal even in this body of research. This study thus uses a qualitative research design to enable SA women to tell their own stories. The purpose of research was to analyze SA immigrant women’s perceptions of, challenges in, and responses to reporting DV and accessing support. SA women were invited to share their stories of abuse and subsequent interactions by answering the question: What were some of the challenges you encountered when seeking information or help for abuse, whether it be from informal (friends/family) or formal supports (organizations)?
This project used a GT approach, which allowed me to ground data analysis in the lived experiences of SA women. GT is often used to advance knowledge on understudied topics (Corbin & Strauss, 2008) and was best suited for this exploratory study. I wanted to emphasize participants’ agency and help them feel comfortable when discussing DV.
The study received ethics approval from the University of Alberta. I recruited participants through a combination of gatekeepers in mainstream and SAWOs, 3 police services, and word-of-mouth referrals. Recruitment was challenging because of the sensitive research topic, and although I self-identify as SA, I still needed to build trust with gatekeepers and participants. Because the SA community is tightly knit, I took measures to establish rapport in the community. I also took steps to reassure participants of confidentiality. For example, I introduced myself as a researcher and DV advocate, and participants were informed that I had no connection to the organizations the women had accessed. To attend to validity issues, I avoided directly connecting the study to any one particular organization. As a result, the SA women who participated trusted me and willingly spoke about the challenges they encountered with supports.
I used the following inclusion criteria for selecting my sample: being a woman over 18; having immigrated to Canada from either India, Pakistan, or Sri Lanka 4 ; identifying as part of the SA community in Edmonton; and self-identifying as a survivor of DV. Experiences of DV vary significantly across cultures, affect the whole family unit or community, are described differently based on culturally specific forms of abuse (Sokoloff & Dupont, 2005), and are not explicitly conceptualized as mainstream forms of DV. Also, because the term domestic violence does not exist in all SA languages, there are variations in how experiences are named. I therefore included participants who had experienced DV by either an intimate partner or family member, given the family structures and dynamics of this cultural group.
Interviews
Interviews were conducted one-on-one with seven SA women. To ensure each participant felt safe when conducting the interview, I asked participants for their preference on a safe place and time to schedule the interview. One participant stressed the need to interview in her home since her abuser worked near the university site. Two interviews were completed at the University of Alberta campus, one at a SAWO office, and four in participants’ homes. In order to protect myself and participants, I checked in with someone before and after meeting participants in their homes. All participants provided written informed consent and agreed to have interviews audio-recorded. Participants were informed that any identifying information would be kept confidential (e.g., names of individuals and organizations) to protect their involvement in the study. I selected pseudonyms to refer to participants with respect to regional and cultural backgrounds and their religious affiliations (see Table 1). Interviews lasted 2–3 hr. Participants were reimbursed for transportation costs.
Sociodemographic Characteristics From Interviews With South Asian Immigrant Women.
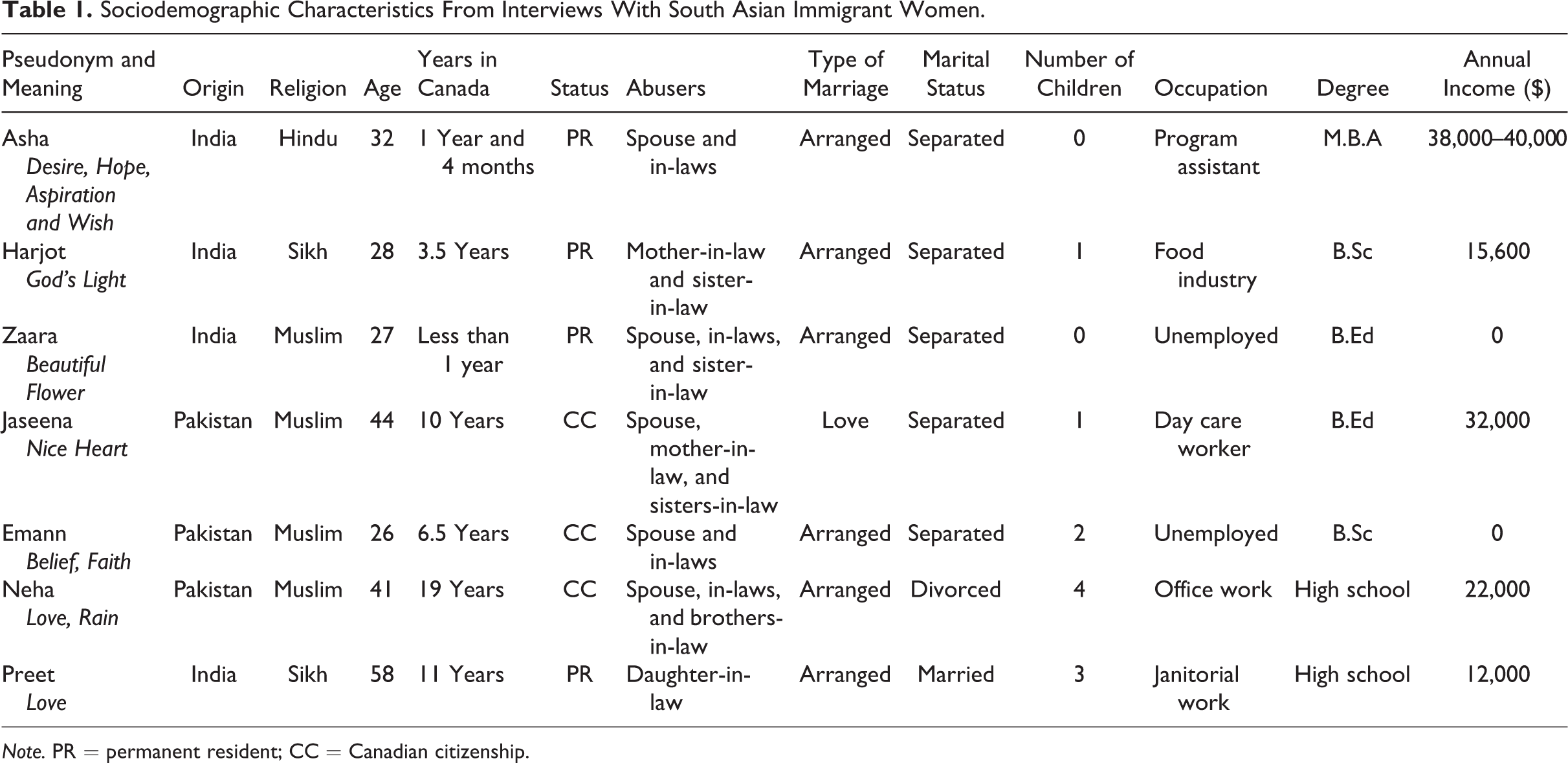
Note. PR = permanent resident; CC = Canadian citizenship.
The women were asked to specify which language, if not English, they preferred to speak during the interview. Two service providers who referred clients and who shared the same ethnic background and language as the participants acted as interpreters during three interviews. Thus, linguistic needs were met during the interview. The service provider’s awareness of the participant’s story helped the women feel comfortable when sharing their experiences with me. My ability to somewhat speak Hindi and Punjabi fluently helped participants to openly share their perspectives and build rapport with me around our shared understanding in SA native languages. However, with interviews in the participant’s native language it was useful to have an interpreter clarify questions or responses in the women’s language to avoid misinterpretations. Service providers imparted valuable feedback to me, during the design of the interviews, on issues concerning consent.
The semistructured interview guide used open-ended questions to allow participants to share their identities, lived experiences of abuse, living arrangements, relationships, and help-seeking strategies. Steps were taken to downplay the word violence, so as to avoid retraumatizing participants. For example, questions included: “How frequently would you say you were being mistreated?” and “Can you tell me what happened?” In the interviews, participants used common DV tactics to describe their experiences (e.g., emotional threats, name-calling, physical abuse including details such as slap, punch, kick, and beating). The semistructured format allowed participants to describe their relationships with spouse and extended family wherever controlling behavior, emotional or physical abuse occurred. I monitored the participants’ behavior for signs of distress and was prepared to refer them immediately to supports.
Participants
Sociodemographic information of the participants is described in Table 1. To understand their varying intersections of oppression, I identified 13 factors that impact DV experiences for immigrant women based on existing literature. Each of the women was positioned differently in negotiating their post-immigration experiences while trying to access informal and formal supports for DV. All seven women self-identified as SA: four from India and three from Pakistan. No participants from Sri Lanka were recruited. Participants’ religious backgrounds varied: one identified as Hindu, two as Sikh, and four as Muslim. Their ages ranged from 26 to 58 years, with a mean age of 36.6 years. Length of residency in Canada ranged from less than a year to 19 years. Four women held permanent resident (PR) status and three women had attained Canadian citizenship shortly after leaving the abusive relationship.
Six of the women had arranged marriages, and one had a love marriage with a distant cousin. Five were in various stages of separation from their partners: Of the remaining two, one was undergoing final divorce proceedings, and the other was still married. Five of seven participants had one or more children.
The women’s occupations varied: five were employed and two unemployed. Participants’ reasons for unemployment were sometimes linked to their experiences with DV. One woman was unemployed because of trust issues with leaving her children in the care of others due to the emotional trauma they had experienced from fleeing their abusive situation. The other woman was unemployed because she was waiting for her degree certification and Social Insurance Number card.
The educational attainment of participants was varied. All participants had completed some level of education in their home country. Five had attended higher level postsecondary education. Two had completed high school. Three participants emphasized how they were struggling to have their foreign credentials recognized in Canada, and two of them pursued some postsecondary education in Canada. Unsurprisingly, some women were highly educated yet still experienced DV (see Warrier, 2000). Five women reported an annual income under $40,000 and two stated no employment income although they were on social assistance (see Table 1).
The interviews were audio-recorded and transcribed verbatim in English. The two interviews with non-English speaking participants were translated from Urdu and Punjabi, respectively, into English. One participant, who spoke broken English asked for an interpreter to be present to rephrase questions for clarity in English and Hindi. Original words and/or sentences were kept in the native language on transcripts in cases where translation could not adequately retain their meaning. For example, all of the women reverted to Hindi, Urdu, or Punjabi when describing abusive experiences that are not easily translated into English since no word or phrase exists to capture the original meaning. These passages are recorded in the native language with an English interpretation in parenthesis.
Data Analysis
Data analysis was conducted using a GT approach. I identified recurring themes that emerged from the data in relation to my research question, following the three stages of GT coding as suggested by Corbin and Strauss (2008): open, axial, and selective coding. I immersed myself in the data as transcripts were read and reread to identify codes that were inserted in the text margins where a concept, theme, or event appeared. Each interview transcript was manually notated for significant codes that were then organized into subcategories. Subcategories were then analyzed using constant comparative techniques to identify commonalities and variations across the interviews and with existing literature. I coded the data for the types of support the women sought and for the revictimization experiences they named with help-seeking.
Although only seven women took part in the interviews, the emerging themes were consistently represented across all the interviews. Memos and field notes were kept as an audit trail of the analytical process and rationale for the codes, subcategories, and themes. My use of GT thus gave voice to these marginalized women (Creswell, 2013), allowing them to construct meaning out of their lived experiences and generating theory grounded in the data, as is GT’s focus (Corbin & Strauss, 2008).
As discussed above, I used intersectionality as a framework to inform my analysis. An intersectional lens examines intersecting forms of oppression such as socioeconomic status, age, immigration status, culture, race/ethnicity, gender, and other identity markers to produce different experiences for SA women seeking help (Crenshaw, 1991; George & Rashidi, 2014a, 2014b; Sokoloff & Dupont, 2005). In my analysis of SA women’s lived experiences, this intersectional approach gave me insight into the broader structural and institutional forces that shaped their experience of marginalization when they reported their DV experiences.
Findings
For all participants, DV did not occur in the typical gender binary framework, that is, between one male perpetrator and one female victim in an intimate partner relationship. Within this cultural context, the perpetrator was any dominating member in the family. Abuse can hail from other relationships: from in-laws or other extended family members, each of which impact DV and help-seeking behaviors (Chokshi et al., 2010; Raj et al., 2006; Shankar et al., 2013). Research on multiple perpetrators has been reported by SA women in North America and other women of color, yet helping practice fails to reflect that reality.
It was apparent from the narratives shared that all participants suffered severe and varied forms of DV from one or more family members, as they described instances of physical, psychological, sexual, spiritual, economic, and financial abuse. The interviews were therapeutic and healing, and many women had tears in their eyes when sharing their journeys. These women came to understand their experiences as abusive and unacceptable. When recalling their pre- and postmigration experiences to Canada, the women conceptualized how violence had played out in the home country and after arriving. Through the interviews, the women “de-normalized” their experiences and understood themselves as deserving of help.
The major theme of revictimization derived from the data emphasizes how such interlocking systems of power continue to impact women even after they move past initial barriers to disclose DV to informal and formal supports. After the SA women in this study described the different ways revictimization manifested for them when seeking help, I then applied intersectional analysis to conceptualize how their intersecting identities and oppressions limited their ability to seek help.
Challenges With Different Forms of Help-Seeking
Six participants had no immediate family in Canada. When I asked if their family was supportive they all responded positively saying “My family, my family! They support me” (Jaseena). This echoes Ahmad et al.’s (2013) findings that having support from family back home was helpful for SA women. Perceptions of help from family are not included in this article because once parents and extended family in the home country learned about the abuse, they were emotionally supportive and concerned. Harjot sums this up quite succinctly: “My parents they always got a clue. I never told them, but they always had a clue.…[My parents] are supportive, but I had to make them understand why all of this is happening.” Similar to the findings from Raj and Silverman’s (2007) study, the participants shared how they initially hid the abuse, sometimes for years, from their family because they did not want their parents to worry about them in Canada.
Three women felt trapped in an endless cycle that made them vulnerable to being mistreated again. After reaching out for help, they experienced further marginalization from within their ethnic community and from professionals. Neha explained her interaction with a Punjabi social worker. She did not give me any help.…Support means I need help.…I need help [to] stand on my [own feet]. Nobody gave me good advice.…When I [have to] repeat my story, I [do not] feel good,…[Nobody wants to] give you proper help.” (Neha) I respect this lady…treat her like my Grandma.…When I need help…she misguid[ed] me. She told me I have no rights in Canada [and] that [my husband] has rights to…the kids. It’s scary when you are in fear these people make your life worse, [but] in this field [they] should be more helpful. (Emann)
Disclosure of DV to Family Friends, Coworkers, and Neighbors
All participants discussed reluctance to approach family friends, 6 coworkers, and neighbors about their situation, choosing to remain silent until they could no longer tolerate the abuse. Once women disclosed, insensitive responses did not help their situation, and many informal supports were reluctant to get involved in family matters. For instance, cases of arranged marriages can become quite challenging due to levels of interference from a “controlling” mother or sister-in-law, as in Harjot’s case. Harjot approached the vichola 7 as the first point of disclosure, expecting assistance with her marital problems while living in a joint family system 8 with her husband, in-laws, and sister-in-law. However, the vichola did not take the behavior Harjot described seriously, showed no interest, and did not want to be involved. Harjot was upset with this man and his family’s behavior since she had approached them to intervene: “I was like, ‘you guys are not concerned at all! You just introduced me to him, and your job was done.’ Ok [my in-laws] can kill me, put me in the basement and you will never know!” Her disclosure further marginalized her as she felt isolated. The issue was exacerbated since she had no immediate family in Canada to support her.
Similar responses were observed among participants who shared how betrayed they felt by friends with whom they once regularly socialized. Two women felt targeted by criticisms from the friends to whom they turned for help. Jaseena talked about feeling rejected: You realize they are your friends; they are not harmful, but people’s personalities are different. Who you go to for support matters, and who is going to give you the right support, to make you feel better. These things you find out by yourself. (Jaseena)
During the help-seeking process, another participant reached out to coworkers and family friends who became aware of her situation. Preet described an incident where she was physically attacked at home by her daughter-in-law. Not knowing where else to go, she went to her workplace. An SA coworker approached Preet and took it upon herself to inform the supervisor. When the supervisor asked the coworker—a SA woman—to take Preet off-site for help, she refused out of fear of getting involved in a family matter. This experience with a SA coworker indelibly affected Preet’s ability to trust anyone. Too ashamed to approach another coworker, she called a close family friend in the SA community who accompanied her to the police station and hospital emergency room. At first, the family friend, whom she had known for some time, was sympathetic concerning Preet’s physical injury from her youngest daughter-in-law. She helped her access care in the hospital and report the injury to the police. On reconnecting later with her husband and son, Preet learned that the family friend had approached the triage nurses to refuse the husband and son’s visitation rights. She felt sad and deceived. It took years before Preet was reunited with her husband after the medical professionals had misunderstood him to be the abuser, when in fact, the main abuser was another female family member. This same family friend visited Preet when she relocated to a senior shelter, encouraged her to pray, and brought her a Sikh religious icon to help her ease her mind. Preet was appreciative of the gesture until the family friend returned a few weeks later to ask for the icon back. Preet felt helpless as it became very difficult for her to cope without the icon.
Four women tried to rely on the support of their neighbors who found out what was happening behind closed doors. Two expressed how they were under surveillance from neighbors, who informed their abusers, ignored the violence, or were reluctant to help, making the situation worse. One participant disclosed how she was monitored by her neighbors, who refused to help. She commented on how she went two doors down for help: Oh ya, don’t ask about the neighbours (shakes head): there is a Chinese lady next door and ah next to next door is a Canadian. So Canadian is [my husband’s] friend who was stalking over me.…I went to her and asked, “Could you please in order to save my life? I need your help, could you help me out?” She said, “No, I don’t want to get involved.” She said no straightaway. So that was painful again. (Asha)
The neighbor’s comments and knocking on the door interrupted but never stopped the violence. It reinforced a divide between minority cultures as accepting abuse, unlike the rest of mainstream society. The neighbor seemed to hold negative assumptions about how men from certain racial and ethnic backgrounds or countries treat women. Similar to Chokshi et al. (2010), the “culture-blaming discourse, community stigmatization, and ongoing stereotyping of the South Asian community constitute[s] a gravely inadequate response to meeting the needs of abused South Asian women” (p. 149). In this instance, Zaara’s husband opened the door to apologize for the noise but was not held accountable for the abuse as the neighbor walked away. Zaara felt little help occurred; rather, the violence escalated. The abuse was not taken seriously and became normalized by the neighbor as a cultural practice SA woman are conditioned to accept. As George and Rashidi (2014a) found, SA men are impacted by structural and institutional violence that influences violence against women. Mainstream societal notions of DV as a problem in the SA community, as noticed in the response of Zaara’s neighbor, highlight racism rather than offering protection.
Zaara reported another occasion when she felt threatened by her husband and was worried about her safety in Canada. She built up the courage to approach a Pakistani woman in the same apartment building who could speak Urdu. Inviting the woman to her apartment, Zaara explained how her husband planned to send her back to India and that she needed to call home. The woman refused the phone call, minimized the behavior, and advised Zaara to focus on winning her husband over with love. She promised Zaara that “Right now I won’t let you call India, but tomorrow I will let you call.” She then explained that these are just empty threats as Zaara could not be so easily sent home without a PR card. Zaara had no knowledge of her rights and immigration status tied to her husband but felt reassured, Zaara trusted this woman’s advice, and tried to set aside her fears. However, her worst nightmare came true as she was sent home the next day. “That same night at 9 p.m. my husband came home with a ticket. He had made arrangements.” Zaara’s experience points at the structural barrier spousal sponsorship can play for immigrant women seeking help. Being unfamiliar with immigration policies and sponsorship rights in Canada can pose a threat for immigrant women trying to execute a safety plan (Alaggia et al., 2009; Menjivar & Salcido, 2002).
Cultural barriers to help-seeking reinforce maintaining family relationships and normalize abuse. Crenshaw (1991) highlights that threats by sponsors and other “cultural barriers often further discourage immigrant women from reporting or escaping battering situations” (p. 1248). SA women may feel reluctant to report their experiences, due to fear of bringing shame upon the family or the community-at-large and fear of being ostracized (Alaggia & Maiter, 2015; Guruge, 2010). Thus, SA women face enormous pressures to preserve a marriage because the larger community tolerates abuse, demands silence, and shames or culturally forbids divorce (Guruge, 2010; Venkataramani-Kothari, 2007). Also, a loss of a dowry may result. Thus, leaving becomes even more difficult, and many of these barriers must be overcome when considering reporting or seeking supports. Compounding this vulnerability are feelings of betrayal due to lack of support from social workers, making it more difficult for women to escape or avoid further violence and situations of subordination (see George & Rashidi, 2014b).
Seeking Help From the Broader SA Community
All seven women feared being blamed or ostracized from their cultural community. Emann described feeling shunned by women at the Mosque for her marital problems. These women advised her to keep quiet about her family business. “Some ladies, they said ‘haram’ [unlawful or forbidden] whatever your husband says, why are you sharing with…other women or involving others?” (Emann). This encounter caused her to internalize the blame and be silent about the abuse as she was too scared to return to the Mosque. Similarly, Jaseena avoided the Mosque, saying, “I don’t think [the] Mosque is a good idea. Same attitudes. I don’t have that experience, I didn’t go, but I feel like it is the same.” She compared the attitudes of those at the Mosque to that of her abuser (husband). Harjot explained how “shortly after everything happened [she] didn’t go to Gurdwara [Sikh Temple] for two months.”
Another participant Neha described how trapped she felt. Her husband and his family allowed her to walk her children only to and from school, so she approached a SA woman from her community on her route: I said, I want to talk to my parents. Could you give me permission [to make] one phone call? She said okay. She give me permission, but after…she tell me about money. I had no money to give her. I hate my community. I hate my community; I don’t like my community and my community people…Yeah, I need help, and I want to take help from anybody, but I don’t take help [from] my Muslim people. They are not helpful people. They just make fun [of you], and that’s it. They are interested in [making] fun and then they hurt your feeling, that’s it. They don’t give any kind of help. (Neha) You know my country there are stupid people. If I talk to somebody, I have problem [with] my husband, my community [won’t] help…They make problems to increase.…Nobody gives you help, and I don’t trust anybody! I don’t trust anybody! (Neha)
Another participant shared her discomfort in approaching the community, also because of gossip: “I didn’t tell anybody; I didn’t want the community to know” (Jaseena). She feared that disclosing DV to people in the community would impact her husband’s career as a physician. Her fear led her to remain silent, which inadvertently protected the abuser. Since Jaseena and Neha encountered people who held similar attitudes to their abusive husbands and who spread gossip, they avoided community interactions. Most of the participants echoed these concerns and felt somewhat removed from their communities and religious institutions.
Similar to existing literature, participants found that SAs prefer not to be involved in social issues like DV and were in denial that abuse happens (see Abraham, 2000; Dasgupta, 2000, 2007; Thandi, 2011). When some women, such as Asha and Preet, approached the SA community for help, they were made to feel they had erred. Asha shared how she self identifies as SA and thought she should be able to find support from her community in Canada. Initially, she was under the impression that other SAs would understand her problem. Instead, Asha reflected on the lack of intervention and being taken advantage of by other SAs. In response to this tendency to encounter SAs who were not helpful, she stated: Never talk about your personal details to others because the moment people know that you are alone in this country, you have nobody here…they will…exploit you. Especially Indians…, they know how to take undue advantage of you. (Asha)
Support from MSOs and SAWOs
Participants reflected on how encounters with MSOs and SAWOs were problematic. While MSOs aim to be inclusive of all abused women regardless of specific community or culture, the women I interviewed expressed a strong need for culturally and linguistically appropriate services. Their suggestions for interpreters and resources in various languages echo existing literature (Chokshi et al., 2010; Guruge & Humphreys, 2009; Menjivar & Salcido, 2002; Thandi, 2011). Three participants recommended hiring more SA staff familiar with various cultural backgrounds. For example, Jaseena noted that “…sometimes we cannot express ourselves. In our language we express everything and then that helps. So I think from everywhere and every country and every language at least one or two people [should] work in one organization, [because] it helps.” Similarly, Emann expressed “I am seeing less people in our community who are [South] Asian in this social worker field so they should hire more. Hire more Pakistani ladies and stuff like that even at the mainstream organizations.” However, others argued that instead of similar culture or language skills of the client, staff should have some basic training or knowledge of SA culture. One big difference between a mainstream and SAWO was having to educate staff on cultural practices such as dowry exchange. Asha explained: Indian organizations know the background. They know…what dowry means, what men think like, and…what the expectations of NRI’s [non-resident Indians] are. They know how the mind frame…of Indians, wherein the English people I had to explain everything to them. I have to let them know…what my culture is. That’s how things work there. So it’s like tedious to make them understand what’s going on. (Asha)
Although Asha did not have a preference for a particular type of organization, she described a bad experience with a male SA worker from an SAWO. Through his formal role as a social worker, he abused her informally. The male SA worker did not inform her about shelter services and instead took her into his home. Asha paraphrased what he had said to her: “I am going out of my way to help you because you are like my daughter, so just come and stay with us. We would be happy to keep you just like our own daughter and whatever money you have, we are ok with…” Now, these guys were in [a rural community outside of Edmonton], which is like, I never knew where [this community] is. I didn’t know anything that time, there were no buses there, no commuting, I was stuck! (Asha) I mean again, I got hit…because it was like sugar-coated words initially, but when you get inside the house, Indians are used to maids and maid servants. Ah, it was bad. [They] took money from me, monthly rent. No rent receipt, nothing, no rental agreement. (Asha) What do you expect of me? But still, I was like I didn’t have that strength to argue with somebody at that point in time and this lady [social worker’s wife]—already I had gone through so much—…used to do the same what my husband used to do. (Asha)
Two other participants shared similar problems when approaching SAWOs and speaking with SA workers. For example, Emann felt betrayed after she approached a close family friend who was an SAWO social worker. Instead of getting help, she was further put down, instructed to be thankful that the family provided her with food, and harshly told she was a “very thankless person” and “not a good daughter-in-law.” She felt blamed for what was happening and advised not to report the abuse as her mother-in-law was highly respected in the community. Emann found this type of intervention unprofessional since the SA worker pressured her to remain quiet despite being a community advocate for women’s rights. Emann later found out that the SA social worker communicated to her mother-in-law how Emann was trying to access support, putting her at greater risk of violence from family members. She explained that confidentiality was breached and she felt betrayed: “I talked to her like a lady, and personally I opened up to her and what she did was talk to my mother-in-law!”
Intersecting factors such as family and community relations, lack of social support, community beliefs, financial dependency, and immigration issues made her more vulnerable to DV and prevented her from accessing help. The same social worker advised her husband’s family to withdraw the sponsorship application for her parents immediately. Emann had run a family business for her father-in-law and husband and was financially dependent as they were not even paying her minimum wages, just a monthly allowance to pay for certain things. This financial abuse along with her interaction with the SA social worker kept her from leaving the relationship. The social worker’s unethical disclosure to the family led Emann to fear further consequences from her in-laws and husband. Once she broke free, she struggled to find employment to support her two children and the withdrawn sponsorship application.
In another example, Neha shared how helpless she felt after approaching an SAWO because the female SA worker refused to assist. The SA worker foresaw a conflict of interest, saying, “I know your husband” but made no effort to take Neha’s disclosure seriously or to refer her case to another colleague. Neha described the help-seeking process as one where she was let down by a woman well known in the community. She said she was deterred from accessing another SAWO. Elaborating on the experience, she exclaimed, “What kind of help did she give me? Never help! I am disappointed, I grab my bag, and then I cry and go away.”
As the women navigated formal supports, three deliberately avoided interactions with people from their own ethnic and/or religious community out of fear of revictimization. Professional intervention requires following a code of ethics that focuses on safety, confidentiality, and being culturally sensitive when approached for help (Ahmad et al., 2009; Guruge & Humphreys, 2009). The workers whom my participants interacted with lacked basic awareness of DV, professional boundaries, nonvictim blaming language, and the importance of remaining nonjudgmental. Instead of supporting vulnerable victims, SAWOs thus replicate the dominant/subordinate power relations at play in the larger community. While the cultural knowledge of SAWOs has its benefits, this study shows that these organizations are not immune from revictimizing victims of DV.
Notably, three participants did not believe that SA women need to be served by people from religious, ethnic, or cultural backgrounds similar to their own. For example, Jaseena found it helpful to go to an MSO over an SAWO since “people from other communities [work] there.…if we go to Canadian organizations, it is much better I think.” She recommended asking to speak to someone who can speak the same language if English is a barrier. Hearing these negative experiences from others thus may lead other SA women to avoid interacting with members of their ethnic community and SAWOs, instead seeking mainstream services.
In contrast, MSOs did not seem to engage in actions similar to what was occurring at SAWOs, although this is difficult to know conclusively since in two interviews, a SA worker from a MSO was present as an interpreter. However, one women, Harjot, did express concerns with MSO policies. In describing her interaction with a mainstream distress center that turned her away following a physical attack from her mother-in-law, she stated: I went there, and…I didn’t know [my mother-in-law and sister-in-law] were following me…The Director said [my] baby couldn’t be here with us, that only two people can be inside the room and then she said “ok you can come on [the next] Monday. Then I will see you and we can help you out”…I was thinking this is the only chance and I told the Director that I don’t know if I can come again…She didn’t tell me anything. (Harjot)
Participants also described challenges in seeking help from the police when they found themselves in severe crises. Six of the participants shared how they were reluctant to seek help from the police. Asha recalled her negative experience with the police: [my husband] literally beat the crap out of me and always used to scare me that he is going to dial 9-1-1 and that he is going to call the police. So I used to be so damn scared.…Honestly, speaking when I had the cop come over too…I was crying.…I was totally losing myself. This [police officer] he wasn’t really bad, but he just said this to me, “Why don’t you go back home in case if you miss your family and if things are not working out for you? You should get back home.” (Asha) I was too scared to give any statement or anything, but I have a bruise here (points to her where the bruise was), and my arm was like swelling.…I was lying like no, no nothing happened and then…the police [officer] start[ed] yelling at me. He said don’t hide, even you charge him or not. Then I say I don’t want to charge my husband.…Yea, and this guy [police officer] I must say he was very rude. He was very strict and he said “because of your kind of women, men get worse and worse. So even though you are not charging him, I am going to charge him.” I was so scared; I was like “no! don’t take him to this!” (Emann)
Additionally, non-SAs are unfamiliar with what it means for an abused immigrant woman to assist police in criminally charging a family member or returning to her home country. These findings are consistent with previous studies that speak to immigrant women’s reluctance to call the police and the lack of protection from the legal system (e.g., laying criminal charges; Abraham, 2000; Alaggia et al., 2009; Menjivar & Salcido, 2002). This suggests that, similar to other professionals, police require diversity training that is anti-racist and anti-oppressive toward racialized communities. When responding to DV calls, law enforcement must confront their racial biases, discriminatory practices, and lack of understanding of the societal pressures that complicate leaving for SA women. As Asha recommended, “…cops should also be given some…briefing about our culture, our society, how people think.”
Discussion
Drawing upon the narratives of SA women in Edmonton, AB, this study applies an intersectional analysis in understanding how both informal and formal supports can cause harm and create barriers for immigrant women experiencing DV. Hearing the voices of these seven SA women reveals why many women are reluctant to seek help. Consistent with U.S. research, the findings from this Canadian study and other scholars (Agnew, 1998; Shankar et al., 2013) suggest that there is little family and community support available to SA women leaving abusive situations, which increases their vulnerability when seeking support from service providers. Because SA community members encourage silence about abuse to prevent shame upon the community and families involved, some women continue to struggle with their own agency to leave abusive relationships (Guruge, 2010). When seeking help, these SA women quickly learned to distrust those to whom they had reached out for help. These findings partially parallel previous studies that indicate similar challenges which make women reluctant to report abuse or leave abusive situations (Abraham, 2000; Dasgupta, 2000; George & Rashidi, 2014b; Menjivar & Salcido, 2002; Merali, 2009; Raj & Silverman, 2002a, 2002b; Shirdwakar, 2004). As Dasgupta (2000) has argued, SAs may fail to acknowledge any problems exist in the family due to the silence around DV within the larger community. Some SAs believe that if they report problems, they risk losing their community’s support. As a result, they endure the abuse as loyalty to their family and community (Shirwadkar, 2004).
This study, however, is unique as a significant theme emerged, that of the power of professionals and SA community members to silence women and thus perpetuate the abuse. Why are SA social workers, irrespective of gender, using power and privilege to revictimize women from their communities? Discussion about this occurrence needs to be further explored. It is important to understand the complications of SAWOs revictimizing the women and actually causing harm, when their stated intention is to protect women and prevent further harm. An intersectional lens further helps demonstrate how SA women experience oppression from various supports when seeking help. Gender intersects across migration, religion, and cultural practices to revictimize SA women. As Sokoloff and Dupont (2005) explain, the standpoints of women of color are voiced as an “intersectional approach providing ways to [legitimize] the experiences of women who have been marginalized and hidden from dominant cultural discourses about battered women” (p. 49). Ongoing research is needed, including a complex analysis of the intersectionality framework as it applies to SA women.
Implications for Practice
Given the growing diversity among the immigrant population in Canada, we must reconceptualize DV (Menjivar & Salcido, 2002). There is a need to apply an intersectional/anti-oppressive approach (George & Rashidi, 2014a, 2014b) and to develop responses that are sensitive to the possibility of women experiencing multiple forms of abuse by multiple perpetrators. Therefore, the help-seeking failures identified from the SA women in this study are important to facilitate reporting of abuse in Alberta, so this subgroup can be served by culturally safe and appropriate services. The voices of service users are rarely included in policy. Thus, these narratives can help us understand DV from multiple perpetrators but also challenges with help-seeking.
Like DV, revictimization occurs behind closed doors. The risk must be minimized for women who are already marginalized yet hold the courage to reach out to supports. These findings demonstrate the need for ongoing community education and policies (see Barrett & St. Pierre, 2011; George & Rashidi, 2014b; Okeke-Ihejirika et al., 2018) to address the role that family friends, coworkers, neighbors, and acquaintances played in the women’s stories. Often, informal supporters were the first people to whom the women disclosed the abuse, and they sometimes engaged in harmful practices that revictimized participants. Thus, addressing this concern requires enabling women and men who are not being abused to empower each other to be better neighbors, resist violence, and support women who are experiencing DV.
Additionally, professionals who are also community members need to be cognizant of how to support SA women as lack of care hinders help-seeking. The women I interviewed quickly removed themselves from their community to avoid further stigmatization, so these discourses must be challenged and reconnection encouraged. Also, more training is required for social work practitioners providing service to SA community members to adopt culturally relevant responses informed by intersectional awareness. Efforts should be made to ensure that SA women are empowered throughout the help-seeking process. Thus, social workers should take specific steps to protect SA women from further abuse by understanding the ways that harm can be caused within communities and culturally specific organizations. While at the same time, these spaces can and do have value to prevent revictimization: It is powerful for social workers to understand how they play a role in the creation of supportive services.
Social services, although available in Edmonton, cannot have a significant impact unless SA community members and the dominant society actively work against revictimization. Thus, a recommendation is for increased culturally safe practices to empower SA women to disclose. Moreover, there is a need to work on rebuilding trust as it has much to do with vulnerability. This involves believing SA women’s experiences, listening to what they require from their positionality across statuses such as race, gender identity, and immigration status, and reminding them they deserve support (Warrier, 2000). Confidentiality violations directly affected the participants in this study. 9 Ethical practices need to be established as participants’ experiences suggest a lack of trust in professionals from their community. Supports within and outside the SA community need direction to be approachable and consistent. When these supports develop welcoming and nonjudgmental practices, they can be important for women experiencing DV. Otherwise, SA women reach a turning point, preferring to talk to female family physicians who they find to be trustworthy or nonjudgmental (Ahmad et al., 2009). Finally, cultural and religious leaders have a responsibility to assist with changing strong cultural stigmas that serve as barriers to disclosures of DV (Ahmad et al., 2009; George & Rashidi, 2014b; Okeke-Ihejirika et al., 2018; Shankar et al., 2013; Thandhi, 2011). Faith-based institutions need to work collaboratively with formal supports to stop the violence. Sustainability of initiatives such as PARIVAAR can allow for intersectoral collaboration and partnerships to continue building capacity for community knowledge and safety for SA women.
Limitations and Future Research
This study’s small sample size offers depth in understanding personal experiences but reduces the ability to generalize to larger populations and is smaller than recommended for GT studies (Creswell, 2013; Padgett, 2017). The process of data collection in GT continues until theoretical saturation is reached (Corbin & Strauss, 2008); however, as is congruent with other studies, it was difficult to recruit women to participate because of real issues of fear and confidentiality. This difficulty may explain why many scholars have acquired information from community activists and service providers who assist SAs (Ahmad et al., 2004; Agnew, 1998; Chokshi et al., 2010; George & Rashidi, 2014a, 2014b; Okeke-Ihejirika et al., 2018; Shirwadkar, 2004; Thandi, 2011). Therefore, though small, this initial study of SA women’s direct perceptions may help facilitate a much needed larger look into immigrant experiences with revictimization.
The absence of Sri Lankan participants and participants from smaller SA communities is a further limitation. Also, because all seven participants had left their abusive relationships and were still receiving supports for DV, their views may differ from SA women who may not report or access services.
Furthermore, since interpreters represented the organizations accessed by the participants, this may have impacted the responses to some interview questions, specifically those concerning challenges with services. Because interpreters were not accredited or certified, they checked for clarification with either the participant or researcher several times during an interview. I also did not return to check with the participants whether my interpretations represented their experiences.
Future research should scale up to pilot whether intersectoral collaborations have shifted cultural practices by offering sensitive supports and services. Community-based initiatives such as PARIVAAR have allowed SA faith-based institutions to partner with MSOs and SAWOs and other professionals (social workers and police), so a review of PARIVAAR’s work could determine whether there has been improvement for SA women. Of particular importance is the need to explore revictimization further in the context of DV, as it can have important implications for social work practice. Such research is a critical step toward understanding SA cultures in the interplay of informal and formal responses to DV disclosures and help-seeking.
Footnotes
Acknowledgments
I would like to acknowledge the support of seven participants who courageously opened up to me, a stranger and researcher, to retell their lived experiences of DV. I would also like to thank Dr. Jana Grekul for her valuable insights and critiques on earlier drafts of this manuscript. I also wish to thank Drs. Rupaleem Bhuyan, Terra Manca, and Nancy Clark for their valuable comments and guidance. Finally, I would like to thank Lynne Martin and Sherrie Winstanley for their encouragement with writing and editing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.