
Abstract
Feminist movements against domestic and intimate partner violence (DV and IPV) have long struggled with tensions around the professionalization of their work. This article uses qualitative interviews and content analysis to conceptualize the IPV movement’s field of action as an interstitial space. The movement against IPV draws together a multi-institutional audience that reflects the historical trajectory of the field. The IPV organizations in the Boston metropolitan area productively engage with and influence various institutional fields. The boundaries of this interstitial space are the multi-institutional bundles of relations drawn together by the DV movement. In the Boston metropolitan area, the institutional fields of action drawn most strongly into the liminal space of the intimate partner violence field are the wider feminist movement and the institutions of the medical/health sphere, carceral system, and education systems. The work of direct services, advocacy, and prevention defines itself in relation to neighboring institutions but remains grounded in its own interstitial space of the IPV movement through individual practices within organizations.
The contemporary domestic violence (DV) movement in the United States commonly cites the 1970s as the decade of its grassroots birth. During that decade, the first rape crisis centers and shelters for battered women were founded, and new legislation was drafted to provide support to survivors of DV (Schechter, 1982). The subsequent decades were years of pushing and pulling between a grassroots movement and the state over the appropriate response of each to the problem of DV. These negotiations resulted in improved public understanding of domestic and intimate partner violence (IPV) and improved services for survivors but also, some argue, the professionalization and depoliticization of the movement (Lehrner & Allen, 2008; Macy, Giattina, Parish, & Crosby, 2010). These narratives, however, reflect a nostalgia for a somewhat mythical grassroots past (Arnold & Ake, 2013) and do not wholly grasp the trajectory of the contemporary DV movement in the United States.
In this article, I analyze the DV service delivery organizations of the Boston metropolitan area by examining organizational mission statements and conducting semistructured interviews with employees. I demonstrate how these organizations sit in a space whose boundaries are drawn together by the feminist DV movement and examine how these organizations’ work occurs across a range of institutional sites.
The boundaries of this space are managed in bundles of relations with neighboring institutional fields including the institutional fields of the state, the law and the carceral/penal system, systems of education, and the medical and mental health systems. The DV service programs of the Boston metropolitan area are at once both feminist social movement organizations and service delivery projects. They are not concepts or entities but bundles of relations and collaborations that produce and are produced by the surrounding institutional fields. In the Boston metropolitan area, the institutional fields of action drawn most strongly into the liminal space of the IPV field are the wider feminist movement and the institutions of the medical/health sphere, legal/carceral system, and education systems. Their reflexive, diverse responses to DV mirror the reflexive evolution and complication of the feminist movement.
Literature Review
The contemporary DV movement in the United States has developed into an interstitial space, drawn into existence through its relations with neighboring institutional spheres. Medvetz (2012) defines interstitial spaces as “a semi-structured network of organizations that traverses, links, and overlaps the more established spheres” (p. 18). The U.S. IPV movement began as a grassroots social movement but has evolved into just such a semistructured network. As a consequence of these bundled institutional relations, the IPV movement is highly institutionalized, professionalized, and medicalized. Yet, it remains a liminal space for strategic action in which its discourses and practices, as well as those of its neighboring institutional fields, are negotiated. Fligstein and McAdam (2011) define a strategic action field as a “meso-level social order where actors (who can be individual or collective) interact with knowledge of one another under a set of common understandings about the purposes of the field, the relationships in the field (including who has power and why), and the field’s rules” (p. 3). By understanding the nature of the strategic action field of the IPV movement as interstitial or liminal, I intervene in binary narratives of the movement that construct it as feminist or not feminist, grassroots or institutionalized, and activist or professional. Pushing beyond these narratives to understand how these discourses and practices coexist can improve our theoretical and practical understanding of the relations between activism and social services in IPV organizations.
Unlike field theory and multi-institutional approaches, resource mobilization and political process models of social movements emphasize the state as the primary target of social action (Amenta, Caren, & Stobaugh, 2012; Giugni, 2008; Lehrner & Allen, 2008; McCarthy & Zald, 2002; McAdam, 1999). More cultural and feminist models of social action, including multi-institutional approaches, reflect an understanding of power as more diffuse and relational (Armstrong & Bernstein, 2008; Polletta, 2008). The state does serve as one of the DV movement’s immediate targets as well as one of its neighboring institutional fields. Yet, as the movement’s ultimate goal is to eradicate all forms of IPV, its ultimate target is better defined as the structural inequities and violence of a masculinist, Eurocentric, capitalist society. This, of course, is a rather hydra-headed target or targets, as reflected in the movement’s development as an interstitial field between institutional fields.
In this article, I intercede in narratives that force IPV organizations into a binary of feminist or nonfeminist, social movement organization or service delivery project, and grassroots or professionalized. The conceptualization of the field of action of DV organizations as an interstitial space of a social movement is in response to critiques of the movement as wholly co-opted through processes of professionalization (Richie, 2000, 2012), medicalization (Sweet, 2015), and neoliberal carceralization and criminalization (Kim, 2013). There are important truths in these critiques, but they can tend toward an overly static determinism that makes less visible those everyday moments of resistance within institutions. Recognizing DV social change and service delivery projects as an interstitial space acknowledges the impacts of the neoliberal state and other institutional fields without neglecting the work that individuals do, even while entangled with these institutions, to deflect and challenge their effects. As one employee shared, “it’s all about the connection, right? It’s all about doing the social justice work as at the same time that we’re doing the one-on-one service work.” The connection between social justice and social services is present throughout the interstitial space of Boston DV advocacy, and it shapes and is shaped by competing connections with neighboring institutional fields.
The second-wave feminist movement may have provided much of the political opportunity—the flashpoint for action—for a movement against intimate violence, but the contemporary DV movement was also initially, at least partially, survivor-directed (Richie, 2012). It is a movement that has been pushed forward and shaped from the top as much as it has been directed and managed from below. The movement’s organizations and their current practices are dually defined by their historical roots as grassroots, community-based social change organizations and their more recent iterations as social service delivery and policy advocacy programs. While the successful redefinition of DV as a social problem has brought it under the purview of state social welfare and criminal justice departments, the movement is still defined by these community-based programs.
IPV—known historically as DV, family violence, or wife battering—was not a new social problem in the 1970s. Mobilization specifically around this mode of violence, however, was new and, perhaps, newly possible. The feminist movement provided both the political and cultural resources required to recruit participants, reframe the issue for a wider audience, and speak effectively to a variety of institutional actors. The multi-institutional approach to social movements comprehends organizations as embedded in fields of multiple, overlapping, contradictory institutions and that those organizations work for material and symbolic changes (Armstrong & Bernstein, 2008). This is the work of social movements; the particular work of the second-wave feminist movement was to recognize and reframe intimate violence as gendered and as the consequence of structural inequities and arrangements.
Several recent empirical studies have questioned the degree to which DV organizations continue to be part of a social change movement (Barrett, Almanssori, Kawn, & Waddick, 2016; Hahn & Scanlon, 2016; Lehrner & Allen, 2008; Macy et al., 2010; Nichols, 2011). These studies have assessed the continued pertinence of a feminist identity for DV service providers. Other authors have suggested that mainstream service delivery and policy organizations are no longer representative of the DV movement (Arnold & Ake, 2013).
One measure of social movement success is its organized capacity to make claims to the state and achieve policy outcomes (McCarthy & Zald, 1977, 2002). According to this measure of success, the contemporary DV movement has been successful in mobilizing resources and achieving policy outcomes. The most notable success, arguably, was the achievement of the federal Violence Against Women Act (VAWA) in 1994 and its subsequent reauthorizations in 2000, 2005, and 2013. This legislation established an Office on Violence Against Women in the Department of Justice and provides funding to service-providing agencies. However, VAWA also increases multi-institutional oversight of community-based organizations and draws the movement into collusion with the state, one of its original targets (Macy et al., 2010; Maier, 2011; Mehrotra, Kimball, & Wahab, 2016; Reinelt, 1994). It has also opened up the movement—and rightfully so—to critiques of the carceralization of a feminist movement as well as the criminalization and medicalization of DV (Kim, 2013; Mehrotra et al., 2016; Richie, 2000; Sweet, 2015).
Policy outcomes and making claims against the state are only one measure of social movement success. The multi-institutional approach to social movements gathers together structural and cultural theories of social movements to foreground relations and practices of power (Armstrong & Bernstein, 2008). Power is organized around multiple sources, as both material and symbolic forces. Those sources of power are produced relationally through multiple social institutions. Social movements are not merely collective efforts to affect policy changes, as fundamentally they are collective projects of world-making. They are, at their core, vehicles for communicating their interpretations of reality to their various overlapping audiences (Benford, 1997). The framing of IPV—both to external multi-institutional audiences and to the movement’s various internal audiences—is an ongoing process.
Critical voices from the margins of feminist theory and praxis furthered the framing of intimate violence as an experience tethered to the intersection of race, gender, class, and sexuality (Crenshaw, 1991; hooks, 1984; Sokoloff, 2005). The institutionalization and professionalization of the movement is in part a consequence of the theoretical work that was necessary to define domestic and IPV as a public problem. It is the very ability of the IPV movement to speak to multiple actors—the state, the courts, the hospitals, the survivors, the media—that has made certain segments so successful. It also reflects the ubiquitous quality of the mundane phenomenon of IPV—the experiences of its effects are intersectional and various for both the individual and the community.
All of these interpretations and criticisms lead us back to the question of why it remains important to understand DV organizations as both feminist social movement organizations and service delivery projects. They are neither and both. The actions and presence of these organizations are better understood in relation to one another, the broader feminist movement, and other institutional actors. Neither the contemporary DV movement nor its advocacy and service delivery organizations were inevitable. Their emergence and evolution were never guaranteed to occur as they did; nor is it guaranteed that their structure, purpose, and identity will remain constant in the future. The success of these organizations is determined by their ability to strategically engage with diverse audiences and to re-frame their goals to infiltrate multiple arenas. The contemporary DV movement and its organizations may be best understood as an example of how the feminist movement has drawn together different institutional fields into an interstitial space (Eyal, 2013; Medvetz, 2012).
The IPV field is just such an interstitial space, bounded by the fields of the feminist movement and the medical, education, psychological/social work, legal/penal, and policy/legislative spheres. The range of practices and discourses in each of these spheres are pulled into a dialogue by the space between them that is created by the IPV arena. In the specific case of the Boston metropolitan area, this arena is most strongly informed at this time by the fields of medicine, the education system, the legal/penal system, and the feminist movement. In my later discussion, I will outline how these institutional relationships impact the practices of individuals working at IPV organizations in ways that both constrain them with the intertwined forces of neoliberalization, professionalization, and criminalization (Mehrotra et al., 2016) but also enable opportunities to challenge these forces and affect change within other institutions.
The feminist IPV movement pulls these neighboring fields together into the interstitial space of its strategic action field. These organizations both challenge and comply with the structural direction of the state. In other words, both the social movement and its ancillary organizations are recognizable as “bundles of relations”—as flows of collaborations and conflicts between themselves and with their audiences (Eyal, 2013). These relations and activities do not themselves form a field; rather, they exist in an interstitial space between fields, a space of opportunities and reflexive change. This liminal, generative space is understood through the modalities of its activities and its practices of boundary work. The space of DV service provision and advocacy is filled with a diversity of activity as actors cross through it into other fields. The work—and with whom it is performed—is defined through collaboration with and in relation to these surrounding arenas. The particular arrangement of this space is outlined in Figure 1 as a honeycomb-like structure that both constructs and is constructed by its separate cells (diagram partially inspired by Medvetz, 2012).
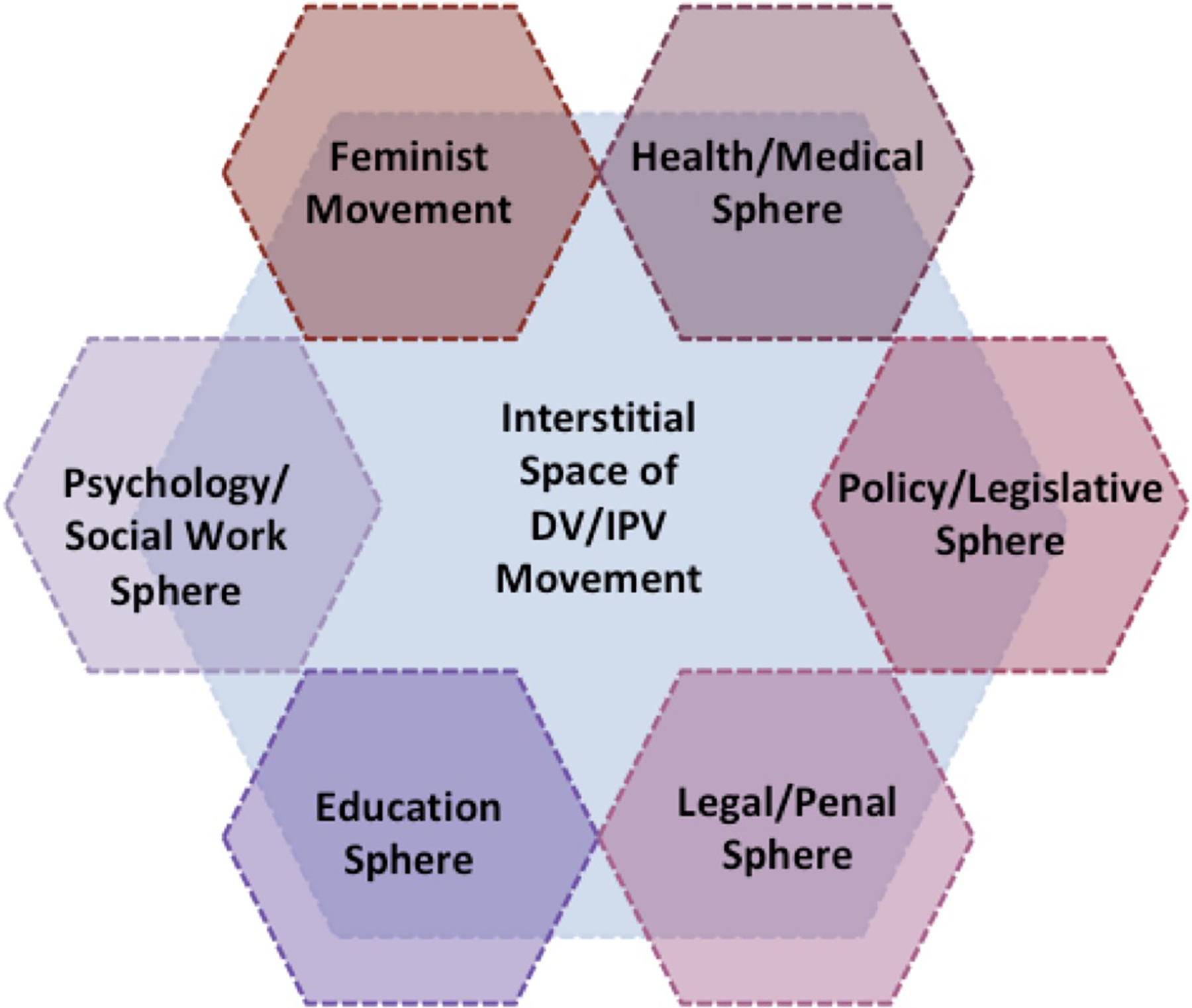
The interstitial space of intimate partner violence service and advocacy.
This space of action for the IPV movement is an interstitial space formed by the interactions and relations between multiple institutional and organizational fields. Using interviews and organizational mission statements, I demonstrate the shape of that local interstitial space in the Boston metropolitan area. This field of action is particular to this location, as a consequence of the history of practice of the movement locally and its overlapping relations with regional, national, and transnational fields of action. The meaning of IPV and the action around its prevention and treatment has taken on various shades of significance throughout the development of the movement. It is at once the state’s problem of gender-neutral crime (Whittier, 2016), an increasingly medicalized social problem (Sweet, 2015), an experience that is exacerbated by intersectional layers of historicized oppression (Richie, 2000), a human rights violation (Bettinger-López, 2008; Merry, 2006; UNWomen, 2016), and perhaps, torture (Cooper, Anaf, & Bowden, 2006). The meaning of the work—and with whom these organizations are working with—is shaped by both conceptual and material exchanges.
Method
This investigation examines the DV service delivery organizations in the Boston metropolitan area. This set of organizations includes the first DV organization to be founded in Massachusetts (RESPOND, Inc.), the first DV shelter to be founded in New England (Transition House), and one of the most recently established programs in the state (Boston Medical Center’s Domestic Violence Program). These organizations were identified through the Massachusetts state coalition on DV, Jane Doe, Inc. As members of the state coalition, these organizations occupy the mainstream, dominant space of DV advocacy. The sample is limited to these organizations at the core of the field in order to understand how dominant logics meet and define the center of the field of practice for the IPV movement in Boston. These organizations vary in their size, structure, affiliation to other institutions, and modality of service provision. Together they constitute the interstitial space of DV service provision and advocacy in Massachusetts.
In the course of this project, I completed nine semistructured interviews with employees of organizations in the Boston metropolitan area. My number of interviews is small, in part because of the challenges of recruiting participants with busy schedules. For this reason, my analysis also relies heavily on the use of the organizations’ financial reports and other institutional documents. Unlike other investigations of DV organizations, I did not interview only the program directors. Instead, I interviewed employees who directly engage with survivors and victims. I recruited participants by contacting organizations by phone and e-mail. Where possible, I contacted staff members whose titles indicated that their work involved community engagement, direct service with survivors, or both. The interviews were conducted in person whenever possible, but two of the interviews were conducted by phone due to the interviewee’s schedule.
The interviews were semistructured and lasted between fifty to 75 min. All were recorded and transcribed by the author. Interviewees were asked about their entry into the field of advocacy and direct services for survivors of IPV, their history with their current organization, and their engagement with feminist movements and discourse. They were also asked about the challenges and successes they saw in their work as an individual, within their organization, and within the wider field of practice in the Boston area. Interviewees also responded to questions about the relationships they saw between their organization, other IPV organization, and other organizations and institutions. They were invited to reflect on what fostered those relationships, what constrained them, and how they understood them as contributing to their field of practice. Finally, interviewees were asked about the future they saw for social work and feminist movement engagement with the problem of IPV.
Admittedly, the number of completed interviews is small, but that data are supplemented by content analysis of the organizational mission statements, websites, and publicly available tax information. Mission statements are the face that organizations turn toward the public world in an intentional display of their goals, priorities, and motivations. While they may not always directly reflect the organization’s practices and structure, mission statements are often the clearest articulation of an organization’s idea of itself, of its goals, and the influence it strives to affect. The analysis of the mission statements also included examination of recent publicly available income tax Form-990s of these organizations and the documents of the state procurement process for funds, administered by the state Department of Public Health. The state procurement of services for prevention and treatment of DV and sexual assault is the process by which organizations apply for grant contracts. The mission statements and financial reports established a snapshot of the organizations’ present financial state and sense of organizational identity.
The author transcribed and coded all interviews and organization mission statements using the qualitative data analysis software Atlas.ti (version 8.4.2). Coding was an iterative, multistage process that pursued an abductive analysis (Timmermans & Tavoy, 2012) of the interviews and mission statements. Codes were drawn from the analysis of the organizations’ mission statements and financial documents, as well as the theoretical entrance to the project. I began by coding the organizations’ mission statements, which involved two rounds of coding. The first was a rough code for patterns between the mission statements, while the second round of coding drew from these emerging patterns as well as concepts from the review of the literature. I established a set of codes from the analysis of these mission statements. This was used in the first wave of coding the interviews. This then informed the revision of the set of codes, which was finally used to code the interviews and mission statements as a cohesive set of data. As already stated, this was an iterative and abductive process, drawing on “the cultivation of anomalous and surprising empirical findings against a background of multiple existing sociological theories and through systematic methodological analysis” (Timmermans & Tavory, 2012, p. 169).
As a feminist sociologist, I practice an engaged reflexivity on my position in the field. This position includes both my individual social location and my engagement with the movement. I am a white, cis-gendered woman and with that positionality has come important privileges in my experiences with IPV as an individual, advocate, and researcher. My involvement in the IPV movement includes experiences as a crisis hotline volunteer, student, employed counselor-advocate, qualitative sociologist, teacher, and activist. The initial questions of this project—“What is the work? And with whom are we working?”—come from my own experiences working with community-based organizations that support survivors of DV and sexual assault. These questions also come from reflecting on my positionality, as I sought to incorporate black feminist critiques of the carceralization of the movement into my own understanding of IPV. I’ve worked at organizations that identified gender as central to their analyses of DV and the provision of services. Many of those organizations also recognized the intersection of gender with race, class, sexuality, and citizenship. These experiences provide me with a certain insight to these organizations, but I am also mindful of the biases I hold toward certain practices and approaches that make me sensitive to identifying spaces and moments in which individuals practice everyday resistance within institutions.
Data
Of the more than 60 DV service and advocacy organizations in Massachusetts, 18 are located in the Boston metropolitan area. In comparison, the central and Metrowest region contains 9, the southeastern region contains 10, the western region contains 5, and the northeast region contains 6 organizations (Jane Doe Inc, 2016). While the Boston metropolitan area is the smallest geographic area, it contains the largest number of community-based DV service providers. This is likely due to the concentration of Massachusetts’ population in the metropolitan area. It is also the home of Jane Doe, Inc., the state coalition, and eight statewide programs. Despite the field’s initial grounding in a grassroots social movement, the mainstream tenor of the work has developed practices that split the everyday activity of contact with and service for the survivors of DV from the political practice of policy and state advocacy. This split between the everyday activity of service delivery and the public, state-focused work of advocacy is reminiscent of the continued challenge to recognize the everyday (private) problem of intimate violence as a consequence of macrosocial, structural processes as translated through individual, relational interactions.
The International Institute of Boston is the oldest organization in the Boston metropolitan area to provide services to survivors of DV—established in 1935, its predominant focuses are the economic and citizenship needs of recent immigrants (International Institute of New England, 2016). The newest organization to the Boston metropolitan area is the Boston Medical Center’s Domestic Violence program, established in 2007 (Boston Medical Center, 2016). In between, five of the organizations were founded between 1974 and 1979, three between 1980 and 1989, eight between 1990 and1999, and two between 2000 and 2007 (see Figure 2). These organizations are mostly community-based or hospital-based programs, and as one employee described, with this, “the field itself has kind of split along funding lines, along, maybe slightly philosophical differences.” The splits across the arena of DV service and advocacy fall along funding lines, ideological differences, and institutional partnerships, as well across historical periods of the DV movement.
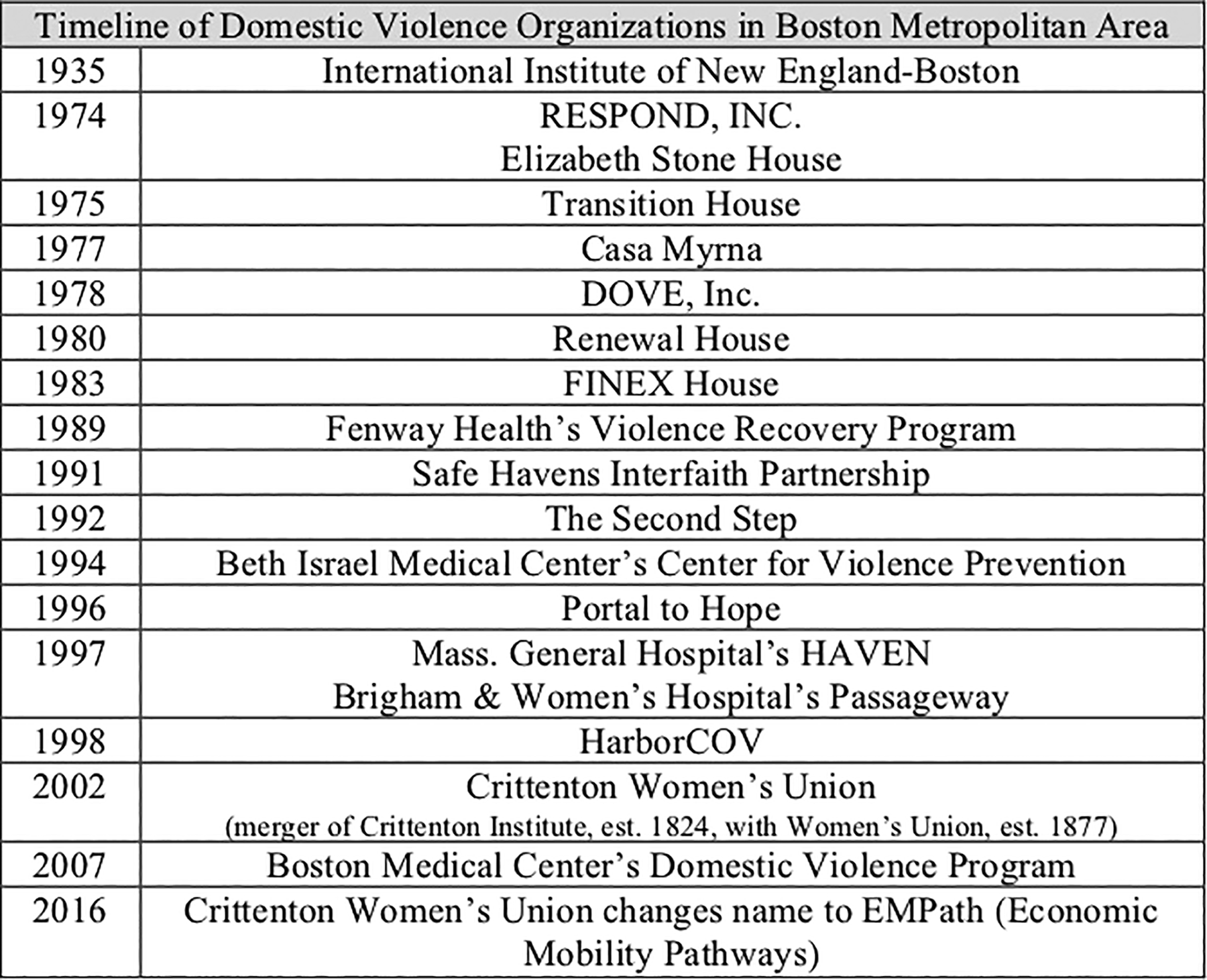
Time line of establishment of domestic violence organizations in the Boston metropolitan area.
These are three key periods in the history of DV advocacy and service delivery in the Boston metropolitan area. These periods, however, bleed together and are not wholly stable. The first (1974–1979) coincides with the initial grassroots flowering of the movement; the second (1980–1994) represents a period of both growth and decline with important state and federal policy successes alongside challenges brought on by neoliberalism and professionalization (Bumiller, 2008), and the third (1994–2007) as post-VAWA, with all its benefits and limitations, and increasing collaboration with health-care institutions. The years between 2007 and the present may come to be another key decade in the history of the movement, as indicated by the merging of some organizations (Crittenton, Inc. with the Women’s Union in 2006 into the Crittenton Women’s Union), organizational name changes (the Crittenton Women’s Union to EMPath in 2016), and significant state policy changes (especially changes to MGL 209a. regarding custody of pets, as well as the 2015 Act Relative to Domestic Violence and criminalization of strangulation). In the historical development of the interstitial space of Boston DV service and advocacy, certain institutions and models of organizational behavior and collaboration have structured the movement’s capacity to both deliver services and act for social change.
Mission Statements
As previously mentioned, all 18 organizations present a statement of their goals and principles on their websites. Of these mission statements, 15 mention domestic or IPV specifically. The three organizations that do not mention domestic or IPV in their mission statements are the International Institute of New England-Boston, Fenway Health’s Violence Recovery Program, and EMPath. Interestingly, none of the organizations mention feminism or the feminist movement directly in their mission statements. However, the centrality of gender, if not the feminist movement, continues to emerge from the interviews. As the organizations define their goals through their mission statements, they mark the boundaries of their practices and intersections with neighboring institutions.
As a social movement, the contemporary DV movement ostensibly has two primary goals: first, to provide immediate services and resources to survivors of DV; and second, to advocate for the broader social change required for liberation from the oppressive systemic causes of violence. The first goal may be rephrased as a goal of “treatment” for survivors (and perpetrators) of domestic and IPV. The second goal may be simplified to “prevention” of the cultural and structural framework that allows violence to occur. Of the 18 organizations in this analysis, 16 identified their “treatment” practices and goals in their mission statement. The three organizations that do not identify a “treatment” goal are the same three organizations that do not mention domestic or IPV in their mission statements.
Only eight organizations identified “prevention” services or used “prevention” discourse to describe their goals and vision in their mission statements. Of those eight organizations, four were founded between 1974 and 1978 in the first years of the DV movement. The other four organizations that included “prevention” services or discourse in their mission statements were founded between 1992 and 1998, a period during which the state and health-care institutions became more intimately involved with DV service and advocacy, most notably through VAWA in 1994. Survivors of domestic and IPV initiated 5 of the 18 organizations; of those 5, 3 include “prevention” services or discourse in their mission statements.
Who Are They Working With?
Of the 18 organizations in the Boston metropolitan area, 5 are directly affiliated with a hospital or medical institution. Seven of the organizations directly mention medical or health services in their mission statements. Eight organizations highlight legal services in their mission statement and description of provided services. Of those eight, three organizations also mention their collaborative relationships with other community institutions including law enforcement. Four organizations define themselves as community based directly in their mission statements; of those four, all four use “treatment” discourse, two use “prevention” discourse, and three were founded by survivors of domestic and IPV. Three organizations mention religion, spirituality, or faith in their mission statements. Two organizations (Safe Haven Interfaith Partnership and Renewal House) are directly affiliated with religious institutions. Through these mission statements, the organizations signal their primary institutional relationships, indicating not only the influence of those institutions on their practice and discourse but suggesting their own impact on their institutional collaborators.
From the interview data, themes emerge related to this question of exactly with whom these organizations are working. One point that has emerged is that community-based DV organizations do not work substantively with other DV organizations.
Their executive directors and CEOs are in communication, and advocates on the frontline do communicate with other organizations in order to procure housing or specific referrals for their clients. They do not, however, frequently and regularly come together to discuss their observations—or those of survivors—and to build solidary incentives. This weakness of the arrangement of the organizations has emerged through interviews and confirms some of the critiques of the movement as increasingly co-opted through professionalization processes. As one employee remarked, “sometimes I think, you know, when people are doing their shelter search or depending on the individual relationship that staff have with other folks at different organizations, sometimes I think that we’re doing to this work together. But I also feel like we’re doing it alone.” However, it is clear from these organization’s histories, mission statements, and financials that there are strong ties with other institutional fields. All of the employees interviewed commented on their partnerships with other organizations and institutions, with one employee of a suburban community-based organization commenting that “it’s all about connections. It’s all about relationships in our work,” speaking to both their relationships with survivors and their institutional partnerships. These include academic institutions, hospitals, state agencies, community police departments, and religious institutions. These connections suggest that the interstitial space of the DV movement contains competing, heterodox logics of prevention and treatment of IPV.
Several questions remain. These include what particular qualities of individual organizations allow for their alliance with which institutional fields, as well as which of these neighboring institutions may establish control of the interstitial space, how that control continues to be challenged, and what new institutional fields may be drawn into the interstitial space of action. As Hahn and Scanlon (2016) note, DV service providers and advocates integrate micro with macro practices such that the space of action is never wholly controlled from the top via institutional influences. While one employee at one organization claims “I have to say that the longer that I have been in the field, the more that I have learned from the different survivors that we’ve served, and I’m just humbled by the stories that I’ve heard and inspired by the situations that survivors have founded themselves in, and most of that has informed the work that we’ve done going forward,” another employee of a different organization laments “the road blocks are still with the government there and Section 8 and housing authorities and all the hoops you have to jump through.” There is still space for the work to be informed by survivors’ experiences and for noninstitutional knowledge to be valued, even as the struggle continues against the contradictory logics of the state and other institutions.
Discussion
The Movement in an Interstitial Field
These DV organizations work to define themselves, their work, and the boundaries of their interstitial space through the definition of their mission and goals. Their missions revolve around the treatment and prevention of DV between individuals and across communities. There is some consensus across both community-based and hospital-based organizations on the definition of domestic and IPV: that it “is probably the same one that’s on Jane Doe’s website or you know is kind of the, you know, known as battering or a pattern of behavior where one person is using power and control over another person through different types of tactics like fear or intimidation or threats of violence.” There is, in both their organization’s formal mission statements and in employee’s informal definitions, the recognition that IPV includes a dynamic of power and control and may include physical, sexual, psychological, emotional, and financial violence. The church-affiliated organizations emphasize that spiritual and religious abuse is also possible. The tentative agreement over the definition of DV marks out these organizations and their work as distinct from other programs that may deal with survivors including hospitals and the Department of Children and Families.
In the Boston metropolitan area, the open, interstitial space of IPV advocacy and activism is most dominated by its relations with the fields of the feminist movement field, the medical institution, educational institution, and the legal/penal institution. In the section that follows, I illustrate how these relations constrain and enable the practices and orientations of individuals working in intimate partner organizations. Below is the diagram of the honeycomb arrangement of their space of practice, with the spheres of the feminist movement, medical institution, educational institution, and the legal/penal institution now highlighted (see Figure 3).
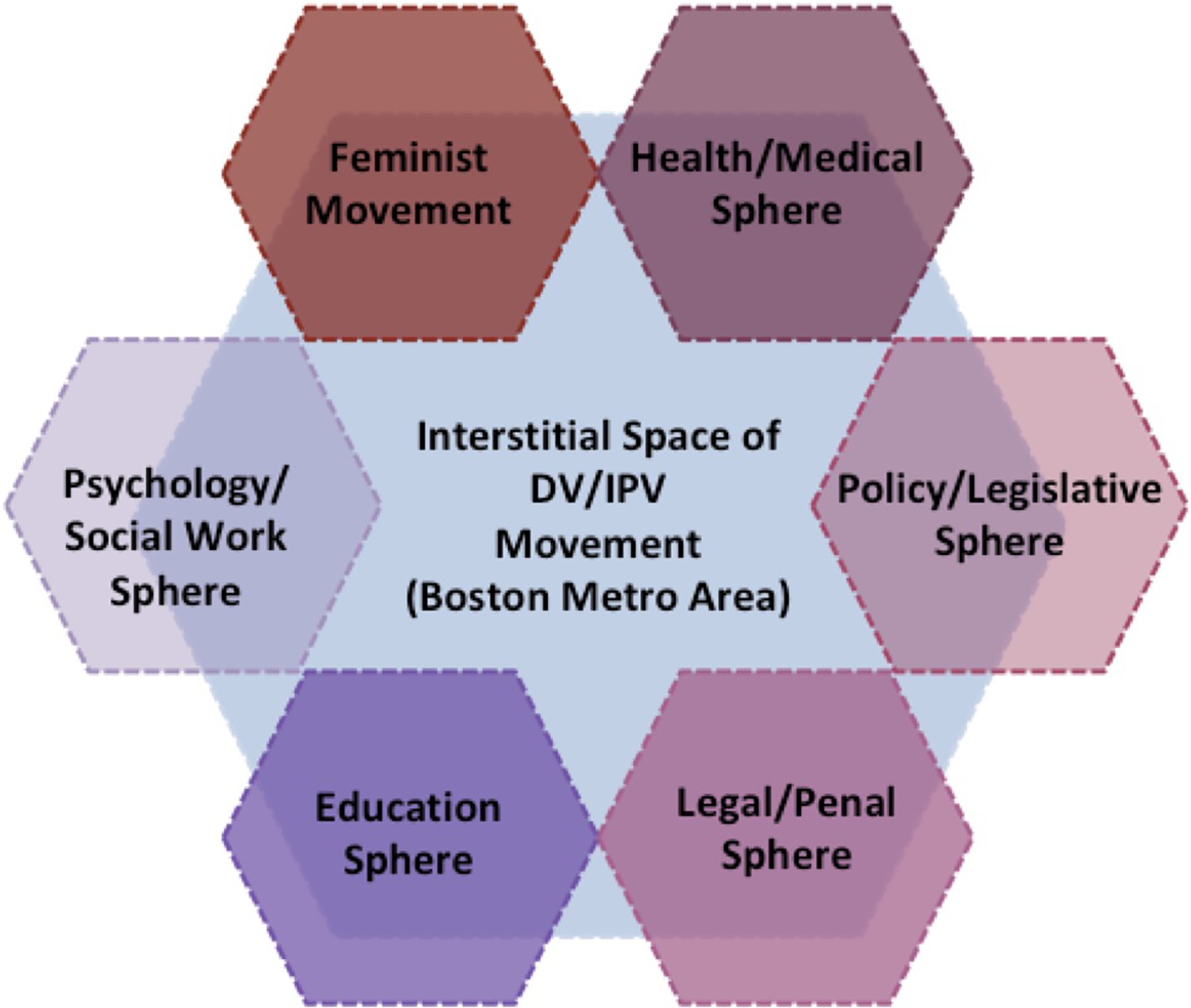
Focusing on the relationship between the Feminist Movement, Health/Medical, Education, and Legal/Penal spheres in the interstitial space of the domestic violence/intimate partner violence Movement.
Relations with the feminist movement field
It remains important to reflect on how DV agencies operate (or can operate) as feminist social movement organizations for three reasons. The first is an empirical concern with the trajectories of social movements and the form of interstitial spaces; the second is an applied interest in the work of service delivery and advocacy; and the third is an ideological commitment to creating links between anti-violence praxis and thought. When most broadly defined, the feminist movement is a movement that examines the structural causes and channels of power, violence, and oppression in relation to gender, and works to transcend and transform them with a liberatory practice. The centering of women and gender in these analyses is the special province of feminist movements. Feminist organizations, therefore, are those that work for social justice, intervene against structural violence and oppression, and practice reflexive self-critique. Drawing from Armstrong’s cultural–institutional approach, DV organizations can also be understood as social movement organizations, for this approach justifies any collective challenge to any institutional arena as a potential social movement project (Armstrong, 2002, p. 11). I argue that IPV organizations are feminist social movement organizations that are embedded in an interstitial space that draws together neighboring institutional fields. Their varying capacity to act as feminist and/or social movement organizations is circuitously determined by their position within this arena.
The field of DV service and advocacy holds multiple definitions of domestic and IPV and includes various relationships to feminist ideologies or logics of praxis, all while holding to a dominant narrative that the field is rooted historically in feminist social movements. Social justice and feminist ideologies are not absent from the work, simply unevenly expressed. This uneven allegiance to feminist ideologies is reflected in the organizations’ mission statements and employees’ reflections. Almost all of the employees that I interviewed identified themselves as feminist or social justice oriented. They also suggested that the majority of their colleagues also identified as such. They were hesitant, however, to describe the organizations themselves as feminist, social justice oriented, or anti-racist, although all agreed that these were relevant projects to their work. One employee of a community-based organization shared that “clearly we don’t necessarily have a strong identity really as a feminist organization. I think a lot of people who work here are feminists, but I don’t know in terms of [our] identity, you know. That’s telling me something if I can’t necessarily say with 100% certainty exactly how we identify.” Yet, an employee at a different, hospital-based organization shared that “as often and in as many ways as we can, we certainly connect the dots with sexism and racism, between violence against women and violence against people of color or LGBT people, sort of the intersections of oppression and the ways that kind of dominant culture and dominant privilege contributes to these things.” These individual statements reflect the organizations’ own mission statements, few of which explicitly mentioned gender, women, or the feminist movement. Yet many of these mission statements communicate a message of feminist and/or social justice orientation by connecting their service provision to survivors with social change goals of community education and violence prevention.
While individual workers may hesitate to describe their organizations as feminist, they are very aware that the limits of the field of action for DV service and advocacy are defined by structural inequities. These inequities, especially around housing and financial resources, as well as penal and carceral consequences, disproportionately affect communities of color and populations in poverty. Individuals within these organizations do bring feminist ideologies to their work, even if they don’t always recognize their organizations as feminist or social justice organizations. Within the contested space of IPV services, these individual ideologies become muffled by relationships between organizations and neighboring institutions.
Workers are hesitant to speak for their organizations, to describe them as wholly feminist or social justice oriented, but it is not clear that this hesitancy comes from their own, or their colleagues’, refusal to think about the work in these terms. In many instances, their hesitancy to describe their work or the organization as feminist comes from a strong sense of the DV movement’s own failure to fully attend to issues of social justice and larger scale social change. As one hospital-based employee shares, they see “racism that pervades, so not only are racism and domestic violence connected, racism is largely to blame for why the movement, the field itself has become less of a movement.” This particular employee connects this issue to the segregation and professionalization of the movement, pointing also to the impact of organizations that recruit their executive directors from the business or corporate sectors. This employee identifies this as a problem because these individuals may not have trauma-informed or social justice backgrounds and therefore may pull DV organizations too closely into alliance with for-profit models.
This observation mirrors that of Mehrotra, Kimball, and Wahab (2016) who found that the impacts of neoliberalization, professionalization, and criminalization are intertwined in their effects on DV work. Constrained by these intertwined pressures, individual employees struggle to identify their organizations as part of a feminist social justice movement, even while they may identify their individual work in these terms. For example, an advocate at a community-based organization shared, So I don’t know if we see ourselves as activists, but I think we’re trying to push for a little bit more in terms of prevention education. I think that we, because we’re a really small organization, it feels like a lot of work that we do is kind of on the ground, putting out fires everyday, it’s a little difficult for us to see this from a more broad, kind of 30,000 feet up point of view and trying to really think about how we can, you know, make larger systemic changes when we’re still just trying to deal with the frontline.
In some cases, the way in which gender, women, and/or feminism are absent is more significant than the simple fact of their absence. For example, Transition House’s mission statement states: We reject the notion that domestic violence is inevitable. Instead, we strive to provide violence prevention education to children and adults, to educate the community about the realities of domestic and dating violence, and to offer viable and effective intervention strategies. (Transition House, 2016)
Relations with the medical institutional field
The inclusion of IPV programs within hospitals and health centers is one of the dominant patterns of collaboration with neighboring institutions of the interstitial space of DV/IPV advocacy. As demonstrated above in the discussion of employees grappling with their individual social justice orientations and the institutional constraints on their organizations, there is more to the current state of the U.S. DV movement and its space of practice than its vertical, top-down co-optation by the state and other institutions. Even in programs closely affiliated with the health-care institution, there is space for individual and organizational practices to challenge institutional logics that are in contradiction with the social justice and feminist logics of a social movement. Indeed, one employee historicized the Boston relationship between the DV movement and the medical institution by explaining “so we started, it was one of the first hospital-based programs, and I think it was started in ‘97, I’m pretty sure. Um, 1997. And that it came out of this need of feeling like, okay, we have these community-based organizations, and most of them are doing like shelter work, and what, feeling like the healthcare systems was a place that wasn’t being tapped into.” From this narrative standpoint, the IPV field itself drew in the medical field into its arena to better organize services, prevent violence, and affect change.
Some of the organizations’ mission statements label DV as a public health issue, implying that it is a disease to be treated, rather than a consequence of structural inequalities experienced through individual, intimate interactions. One example is Transition House, mentioned above; other instances of this intertwining of the medical field and IPV movement are apparent in the mission statements of both community-based and hospital-based organizations. For example, one program based at a local hospital states that its mission is “to improve the health and well-being of people impacted by multiple forms of violence, including domestic violence, sexual assault, community violence and homicide by providing trauma-informed services and programs.” Here the mission is both expanded and contracted—it is expanded to include multiple forms of violence but contracted to focus on the health and well-being of individuals.
Yet, as one employee at a hospital-based organization shared, a public health perspective aligns with her: Oppression standpoint, and like seeing the oppression of women, and having specific gender-based violence. I think also, from like a social justice point view of, this [is] an epidemic and that this is something that, you know, is not obviously confined to the U.S., but you know, around the world, and so I think that that was really, you know, I’m part of the solution, if you will, or part of the change or hope and education and all of that in like something that feels insurmountable at times.
The inclusion of IPV programs within hospitals and health centers is one of the dominant patterns of collaboration with neighboring institutions of the interstitial space of DV advocacy. It is a multidirectional relationship that pulls and pushes both institutional fields together to effect their definitions of where their work overlaps and with consequences for the definition and prevention of IPV.
Relations with the education institutional field
The organizations of the Boston metropolitan area also operate strongly in relation to the legal, criminal, and education institutional spheres. Many workers pointed to their collaborations with schools and universities as key to the prevention of DV. They also spoke more broadly to the education of other community-based programs, businesses, and the general public on the dynamics of domestic and IPV. The community outreach coordinator at a community-based program shared that one of her goals with education is “whether its students in the high school, or just in general community members, recognize and stand up for the victims.” This logic of education as prevention reflects the intersection of the feminist movement’s definition of IPV as a consequence of structural patterns, public health’s logic of community treatment through community education, and a social justice logic of collective responsibility for our neighbors. As organizations develop formal and informal collaborations with schools and universities, their field of action is expanded along with their repertoire of services and advocacy.
Relations with the legal and penal institutional fields
The DV movement’s interactions with the legal and penal institutions are one of its most complex bundles of relations. The criminalization, or carceralization, of domestic and IPV has been well critiqued (Bumiller, 2008; Sokoloff, 2005; Whittier, 2016), especially for its uneven and often destructive effects on already marginalized communities. That one of the standard services offered by DV organizations is legal advocacy, including accompaniment to court, assistance with filing police reports, and emotional support throughout court procedures is evidence for the criminalization of DV. Yet, that the problem of DV—and the space for advocacy and services around this problem—is intertwined with the legal and penal institutions is not evidence that the problem or the field of action has been wholly dominated by these institutions’ logics. One longtime employee at a community-based organization argues that it is important to facilitate those relationships because: There are certain police officers, there are domestic violence officers in the different towns that, some are trained more highly than others, but that we feel, we make a point to form a relationship with, because in that critical moment when you have somebody in danger, you need to be able to have the personal cellphone of the person you want to get to and you don’t have go through all the formalities.
These examples demonstrate how workers retain important critical logics of the feminist movement’s definition of DV in the face of health care, social work, legal, and other institutions that may pathologize, criminalize, and medicalize the experiences of survivors and perpetrators. Yet, as several employees shared, the work of DV advocates and counselors is necessary precisely because victims and survivors “were interfacing with other people and systems who weren’t hearing what they need.” The work can’t be separate from those other systems and institutions because the experiences and needs created by IPV are not confined to any one of those systems. The space of DV service and advocacy defines itself in interaction with and relation to these systems and institutions but maintains its separate interstitial space largely through individual practices within organizations. These individual practices continuously mark the boundaries of the space through definition of mission and collaboration with other organizations and institutions.
Conclusion
What is the work? And with whom are these organizations working? The answers to these questions are drawn from the analysis of the relations and collaborations between these organizations and surrounding institutional spheres. It is in the activity of these relations that the problem of DV is framed and collective action against the issue is defined and legitimized. The recognition of domestic and IPV as an issue of social justice and public health—rather than as an individual misfortune—was not possible before the mobilization of resources, ideology, and opportunity by the feminist movement. The present framing of IPV and legitimate modes of services and advocacy is likewise indebted to the both the internal and external context of the DV movement. The work of DV prevention and treatment and the recognition of legitimate partners in this work have been defined within an interstitial space.
The definition of this violence and abuse as DV or IPV has occurred through the relations and collaborations between grassroots organizations, a social change movement, and the surrounding institutional spheres. It has predominately been defined as a structural issue made visible as a problem between individuals. The legitimate response to this issue is recognized as policy advocacy, medical intervention, public health education, and collaborations with the criminal and civil court systems. This is not so much the result of a settled, dominant logic, but the consequence of interacting and interstitial bundles of logics that weave together the space of action for DV/IPV movement. This has occurred through the drawing together of these institutional spheres into the interstitial space of DV service provision by the magnetic pull of the feminist movement.
This definition of the legitimate activity, concerns, and stakes of this interstitial space was not inevitable, nor is it impervious to alteration. The contemporary DV movement could have evolved quite differently if it had created stronger ties to, perhaps, the anti-war or labor movements. It certainly appears differently, and acts in relation to different audiences, on the transnational stage. The inclusion of organizations like EMPath, Fenway Health, and the International Institute of New England-Boston as members of the state DV coalition may indicate that such an evolution of the interstitial space is ongoing. It may also indicate another successful consequence of the feminist DV movement—its steady infiltration into the strategic action fields of other social change movements and institutional spheres.
The feminist movement has not disappeared from DV service delivery organizations, nor have they been wholly co-opted by state funding and regulation. Rather, these organizations are positioned in an interstitial field, a space between the fields of the state, business, the courts, and so on, that has been drawn into the arena by the feminist social change movement. Partnerships between DV organizations and police departments, hospitals, judicial systems, and corporations are examples of this capacity to strategically practice heterodox engagements. The capacity of DV organizations to productively engage with and influence various institutional fields—to reframe their goals in terms of these fields’ stake and interests—is precisely because they exist in a space between and in relation to all.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.