
Abstract
For survivors of intimate partner violence (IPV), safe, affordable, long-term housing is a critical aspect of establishing a life free from abuse. New permanent housing models for IPV survivors, which are emerging across the United States, are designed to meet the basic need of shelter and must at the same time be focused on meeting the needs of survivors of IPV. Using an in-depth qualitative case study of a new supportive housing program serving 10 IPV survivors and their children, our research project examines how housing helps residents heal from trauma. We use constructivist grounded theory and a feminist perspective to give voice to the women and construct an in-depth understanding of their perspectives. Data collection spanned 7 months and included two rounds of individual interviews and four focus groups. Data analysis utilized open-ended coding and constant comparison to inform theories on trauma and trauma-informed care. Our findings indicate that safe, affordable housing is related to the ability of IPV survivors to recover from past trauma. Based on our findings, theories and practice frameworks should consider housing stability as an integral component in the healing process. We also discuss policy and practice implications to incorporate trauma-informed practices in housing models.
Keywords
For survivors of intimate partner violence (IPV), safe, affordable, and long-term housing is a critical aspect of establishing a life free from abuse. IPV survivors often face inadequate housing options after leaving an abusive relationship, forcing them to choose among retraumatizing options, such as cycling through temporary shelters, becoming homeless, or returning to an abuser (Clough, Draughon, Njie-Carr, Rollins, & Glass, 2014; Menard, 2001; National Network to End Domestic Violence [NNEDV], 2017; Wilson & Laughon, 2015). Although an extensive network of domestic violence emergency shelters across the United States address the immediate need of safe shelter, demand is greater than supply. A point-in-time survey found that in 1 day in 2016, over 41,000 individuals were provided shelter by a domestic violence agency, but that close to 12,000 were turned away due to lack of availability (NNEDV, 2017). Even survivors who find shelter in the domestic violence system often face time limits and subsequent challenges in locating long-term housing options (Botein & Hetling, 2016). Viable housing options in the private market are often unaffordable for low- and moderate-income families (Joint Center for Housing Studies, 2014), and public housing can have long wait lists in most urban areas.
In response to this crisis, an increasing number of domestic violence agencies are examining, developing, and growing programs aimed at helping survivors find and keep long-term affordable housing (Botein & Hetling, 2016). Based in the philosophy of housing first, which posits that people are better served when settled in a permanent housing arrangement as opposed to a temporary shelter, such programs are designed to meet the long-term need of housing as opposed to addressing a short-term emergency. This change from offering emergency shelter on a time-limited basis to providing affordable housing on a permanent basis marks a philosophical shift in service-provision for domestic violence agencies (Botein & Hetling, 2010). The change also echoes a growing recognition of the long-term impact of trauma and the field’s shift to trauma-informed care (TIC; Wilson, Fauci, & Goodman, 2015). While new program evaluations are currently examining various models and assessing survivor outcomes in terms of safety and housing stability (Sullivan, 2017), questions remain about the connections between housing and recovering from trauma.
Our research question asked how can long-term housing support journeys to healing and recovery from IPV. Very little research exists that directly examines the voices of women affected by or experiencing these newly developing programs. Using a case study of a new supportive housing program for survivors of IPV, we examined the residents’ perspectives on the model as related to their efforts to move past their traumatic experiences with IPV. We asked about their definitions of healing and how living in supportive housing has helped them with their journeys toward healing from abuse in order to understand whether and how the model matches survivors’ needs.
Background
IPV is a pervasive public health and social problem that impacts millions of women in the United States (Clough et al., 2014; García-Moreno, Jansen, Watts, Ellsberg, & Heise, 2005). While the use of a gender-neutral framework for understanding IPV has gained ground in recent years (Reed, Raj, Miller, & Silverman, 2010), evidence consistently demonstrates that IPV is a gender-based issue, as women are more likely than men to experience IPV and its negative effects (García-Moreno et al., 2005; Reed et al., 2010; Tjaden & Thoennes, 1998). Researchers have pointed to traditional masculine gender role ideologies and embedded gender inequities as some of the broader, societal reasons underlying the continual perpetration of IPV (Murnen, Wright, & Kaluzny, 2002; Reed et al., 2010; Santana, Raj, Decker, La Marche, & Silverman, 2006).
Women experiencing IPV face a range of often overwhelming concerns, including but not limited to physical injuries, negative mental health consequences, limited financial resources, barriers to meeting basic needs, precarious situations for their children, and feelings of shame and isolation (Jasinski, Wesely, Mustaine, & Wright, 2005; Pavao, Alvarez, Baumrind, Induni, & Kimerling, 2007; Wilson & Laughon, 2015). Contemporary trauma theory provides a framework to understand how experiences of trauma can have long-lasting psychological and physiological impacts on individuals (Herman, 1992; Van der Kolk, 2014). According to the theory, IPV matches a form of human-caused trauma that results in disconnection and powerlessness (Herman, 1992). Although the application of trauma theory to IPV often begins with this psychological foundation, feminist explanations of IPV force a consideration of macro- or societal-level factors in addition to individual-level barriers and how trauma theory might be adapted (Anyikwa, 2016). Similarly, feminist scholars have cautioned that applications of trauma theory to service provision, if limited in focus on only psychological and physiological impacts, might limit practice to focusing on individual rather than societal solutions (Tseris, 2013).
Homelessness is a societal-level factor that often interacts and complicates individual experiences of IPV. IPV is now recognized as one of the leading causes of homelessness among women in the United States (Baker, Billhardt, Warren, Rollins, & Glass, 2010; Rollins et al., 2012; U.S. Conference of Mayors, 2005). Studies have documented how IPV is associated with episodic stays in homeless shelters (Metraux & Culhane, 1999) and concerns about housing instability (Pavao et al., 2007). Women experience housing instability when they face conditions such as frequent unwanted moves, eviction threats, challenges in securing housing due to credit or rental problems, difficulties in paying rent or mortgages, and the need to double up with friends or family (O’Campo, Daoud, Hamilton-Wright, & Dunn, 2016; Rollins et al., 2012). When coupled with the obstacles associated with navigating the social service agency bureaucracy or interfacing with underresourced service providers (Clough et al., 2014), housing instability can lead to women accepting unstable and unsafe housing options, including returning to or staying in abusive relationships (Clough et al., 2014; Menard, 2001; NNEDV, 2017; Wilson & Laughon, 2015). The documented lack of housing services and affordable housing units (Baker et al., 2010; NNEDV, 2017) also contributes to situations of housing instability and highlights the critical need to identify viable housing solutions that adequately meet survivors’ needs, ensure their safety, and facilitate their pathways toward healthy, independent lives.
In light of the multiple barriers that IPV survivors face, as the result of both individual trauma and patriarchal or inadequate social systems, the permanent supportive housing model, with its linkage of affordable rental housing with a range of supportive services based on resident needs, holds potential as a solution (Botein & Hetling, 2016). Permanent supportive housing (PSH) gained popularity in the 1980s as a new solution to chronic homelessness among individuals with mental health or substance use issues. The model is closely related to the housing first philosophy, which posits that individuals are better positioned to succeed when they are living in a permanent home as opposed to an emergency shelter. In contrast to the previous approach, which asked individuals to address all barriers, like substance use, before qualifying for housing, PSH is designed to allow residents to pursue treatment and other options while in a permanent residence. The four key principles of PSH are affordability, safety and comfort, accessible and flexible support services, and empowerment and independence (Hannigan & Wagner, 2006). Services provided by PSH programs can include employment training, job placement assistance, career counseling, mental health counseling, peer support groups, and legal advocacy (Shegos, 2001). The philosophy of PSH emphasizes independence and empowerment; thus, services are voluntary and residents have choice in the extent and manner to which they participate. In this way, PSH becomes “a place to call one’s own that makes a person feel safe and secure in the world” (Bird, Rhoades, Lahey, Cederbaum, & Wenzel, 2017, p. 13). Evaluations of the model indicate positive outcomes for individuals and cost–benefit savings as the cost of PSH is less expensive than serving emergency needs through public services like emergency shelters, hospital emergency rooms, and jails (e.g., Culhane, Metraux, & Hadley, 2002).
Efforts to adapt PSH and other long-term housing models to the needs of IPV survivors are more recent. The agencies that have pursued this strategy have integrated TIC practices to better match PSH to the needs of survivors. TIC is a foundational element in the provision of services to IPV survivors and is based on trauma theory, which refocuses service provision from the question of “what is wrong with you?” to a question of “what happened to you?” The five key principles of TIC are safety, trust, choice, collaboration, and empowerment (Harris & Fallot, 2001). Hales, Kusmual, and Nochajski (2017) quantitatively assessed these five dimensions using structural equation modeling and found that they are both unique and complementary, supporting their theoretical strength. Wilson and colleagues (2015), however, found that the five principles have been defined and implemented differently at different domestic violence agencies, indicating that agencies have chosen to adapt rather than adopt the principles. TIC is now also being applied to homelessness services and housing models outside of the IPV field. TIC principles align well with principles of PSH (DeCandia, Beach, & Clervil, 2013; Hopper, Bassuk, & Olivet, 2009). When adapted to address the needs of women who have experienced both abuse and the trauma associated with homelessness and housing instability, TIC emphasizes trauma awareness, safety, opportunities to rebuild control, and the use of a strengths-based approach (Hopper et al., 2009). While practice has demonstrated the alignment and compatibility of the approaches, theoretical developments have not followed as quickly. The role of housing stability remains absent from theoretical frameworks of TIC, and best practice models consider only how to integrate TIC into housing and not the possible role housing might play in recovering from trauma.
Qualitative research on IPV and housing, however, indicates an important connection between housing and well-being. According to O’Campo, Daoud, Hamilton-Wright, and Dunn (2016), studies that explore this topic are generally more concerned with the financial rather than psychological elements of housing instability. While there is less attention paid to how women conceptualize the link between housing and emotional healing, Zufferey, Chung, Franzway, Wendt, and Moulding (2016) conclude in their recent study that “access to safe and affordable housing, respect, recognition…and feelings of belonging to a safe home are fundamental to women’s well-being” (p. 473). Additionally, while there are many qualitative studies that look at women’s voices and lived experiences in homeless and domestic violence shelters as well as emergency and transitional housing programs (Melbin, Sullivan, & Cain, 2003; Williams, 1998; Wilson & Laughon, 2015), few studies directly examine how women IPV survivors perceive and experience newly developed PSH programs (Botein & Hetling, 2010; Centers for Disease Control and Prevention, 2010). Filling this gap in the literature is essential to understanding how IPV survivors view and value a possible connection between housing and recovering from trauma and how this connection might be applied to both theory and practice.
Method
Study Setting and Research Design
In March 2016, the Town Clock Community Development Corporation (CDC) opened the doors of Dina’s Dwellings, 10 newly renovated apartment units in a previously underused section of the First Reformed Church of New Brunswick, NJ. Dina’s Dwellings provides affordable permanent housing with supportive services for women survivors of IPV and their children. To qualify for the housing, survivors must be coming from emergency or temporary shelter, meet income criteria, and have a documented physical or mental disability, which includes depression, anxiety, posttraumatic stress disorder, and other mental health conditions that are commonly associated with experiences of abuse. Dina’s Dwellings also provides supportive services and referrals. The space includes 10 apartment units on the first two floors: 2 two-bedroom units, 1 one-bedroom unit, and 7 studios. On the third floor, there is a community space with couches, a television, and a library; a conference room; a utility room; laundry facilities; a room with clothes and food donations; and the offices of the case manager and Executive Director. A second floor sitting area with a bookshelf and plants overlooks the front walk of the facility. The development of Dina’s Dwellings was a lengthy process with initial brainstorming beginning in 2009, ground breaking in 2014, and the welcoming of residents in early 2016.
During the later stages of the planning phase, the lead author met with the executive director to learn about the project. In collaboration, they decided to engage in a research partnership and designed a project grounded in a longitudinal, qualitative investigation of residents’ experiences at Dina’s Dwellings during its first year of operation. The overall goal was to offer insights about how women conceptualize residence at the site and participation in the supportive programs as related to their lives, specifically their individual journeys toward healing and stability. Additionally, the project aimed to offer concrete suggestions to Town Clock CDC staff and board to ensure that policies and procedures are in line with providing a safe, supportive, and positive space for residents. The research project received a Community–University Research Partnership Grant from the lead author’s institution and as such followed best practice guidelines of clear communication, reciprocity, trust, and shared authority as put forth by the university.
The research team consisted of four female faculty and students with research interests and practice backgrounds in the field of violence against women. Two of the team members had previously worked as staff at domestic violence agencies in other states. The other two team members had worked at Dina’s Dwellings as interns. Our ages ranged from early 20s to mid-40s. All members had completed formal training in domestic violence to work with survivors. We grounded the project in a feminist approach that prioritizes the voices of those most impacted by and knowledgeable about the new housing model. Specifically, our methodological approach was based in feminist grounded theory (Keddy, Sims, & Stern, 1995; Wuest, 1995), with specific analytical and coding decisions that matched with constructionist grounded theory (Charmaz, 2006). Following the constructivist grounded theory approach, we sought to understand the differences in perspectives and experiences of the women and coconstruct meaning with them, acknowledging our own perspectives and biases (Plummer & Young, 2010). As a Community–University Research Partnership, we worked closely with Dina’s Dwellings staff, discussing preliminary findings at monthly meetings and gathering feedback on all written documents. In this way, the staff served an important collaborative research role, validating themes, raising new questions throughout the process, and adding another set of views and values to our emerging understanding. The research project was reviewed and approved by the university institutional review board.
Study Participants
All 10 residents of Dina’s Dwellings were invited to participate in the project. An initial meeting with the residents was held one evening in September 2016, about 5 months after most women had moved into the building. At this meeting, which was held in the community room of Dina’s Dwellings, the research team introduced themselves and the project. Flyers with key information and the phone number of the principal investigator were also posted in the building.
Of the 10 residents, eight women volunteered to participate in various sessions. The women ranged in age from their early 20s to early 50s, and some had children in their care. We spoke with eight women whose races and ethnicities included Caucasian, African American, Latina, and South Asian. About half the women were working at least part-time, but all had incomes low enough to allow them to qualify for low-income housing. All had documented mental health disabilities as stipulated by the program. Although most of the documented disabilities were related to depression and anxiety, the Dina’s Dwellings case manager reported that some women were also dealing with more challenging issues such as past substance use and more serious psychiatric conditions. All but one of the women had moved into the building during the first months of operation. The remaining resident moved into the building about halfway through the research project and joined the project immediately after her arrival. The later addition of this participant helped validate themes emerging throughout the data collection and coding process. Participation by residents in the research project was completely voluntary, and the identity of participants is confidential. We refer to residents with pseudonyms in this article.
Procedure
Data collection included four focus groups and two rounds of individual in-depth interviews. The timing of data collection and volunteer participation are summarized in Table 1. Of the eight residents of Dina’s Dwellings who participated in the project, three women participated in all four focus groups and both interviews. Two women participated in all data collection meetings except one focus group. One women participated in the first half of the project, while another joined later and participated in the second half. The final participant attended only one focus group.
Sample Members and Data Collection.
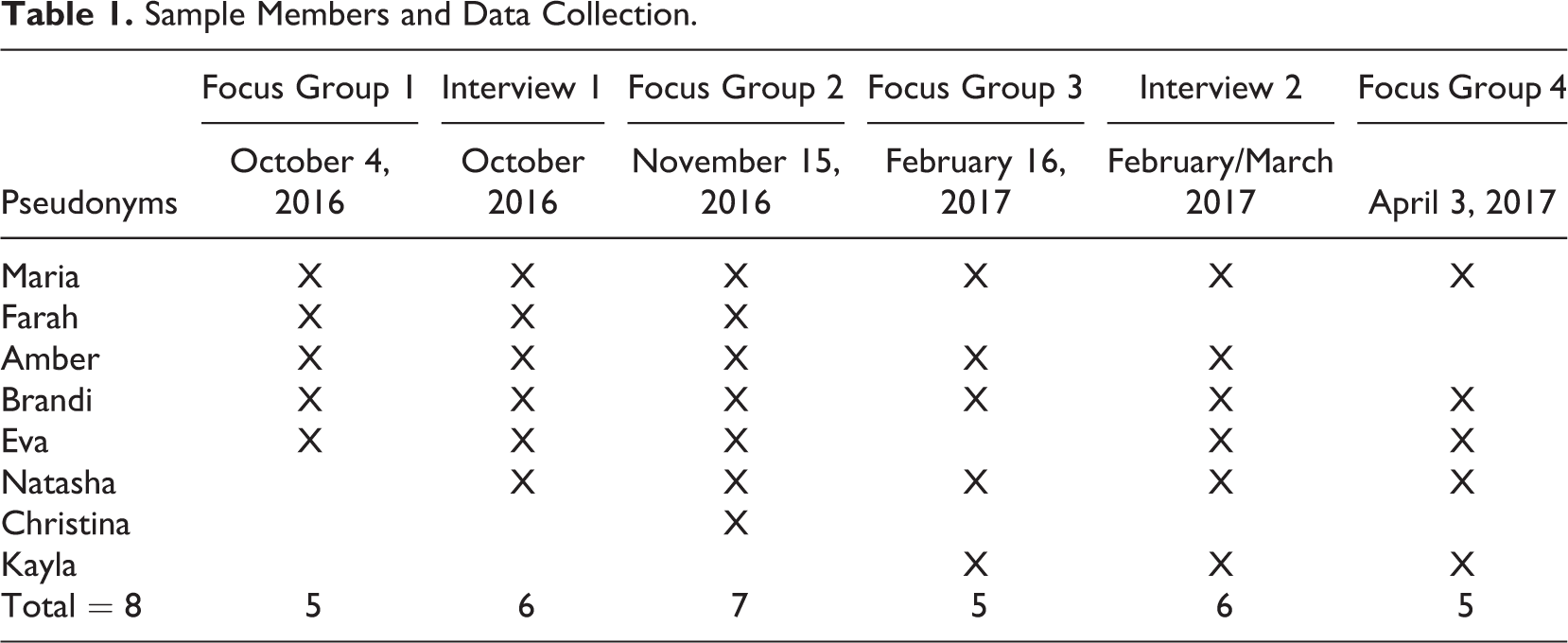
Data collection began with a focus group discussion. The purpose of the focus groups was to hear women talk as a group about their shared experiences participating in programs and sharing the space. The primary purpose of the first focus group was to develop a trusting relationship between the research team and the participants. It also allowed the researchers to learn about the terms and words women used among themselves to discuss the topic, the “women talk” Devault (1990) emphasizes for feminist research. Hearing and listening to this language helped the research team edit the individual interview instrument. The conversation focused on the purpose of the project and women’s descriptions of their experiences and opinions of Dina’s Dwellings as new residents. The focus of the second focus groups evolved to include more detailed discussions on shared experiences and efforts to find work and social supports. The final two focus groups included additional questions on emerging categories and themes and incorporated member checking to validate emerging findings. Guiding questions at the final focus group included a discussion of healing and how housing relates to their journeys to healing. Attendance at focus groups ranged from five to seven women at each session.
Individual interviews were based on an open-ended and conversational approach that allowed the resident to share her experiences in her own words and to expand on individual thoughts, feelings, and ideas (Rubin & Rubin, 2005). The interviews allowed women to discuss experiences and thoughts they were uncomfortable with sharing at the focus group settings and allowed the researchers to ask about unique individual values and opinions. We conducted two rounds of individual interviews: one in October 2016 and one in February/March 2017. Interview instruments were semistructured, with main questions and follow-up probes but allowed for interviewers to focus on supporting a conversational style interview led by each resident. The main questions for the first round of interviews focused on experiences with Dina’s Dwellings, personal and family well-being, goals and how Dina’s Dwellings provides supports in reaching their goals, and their housing future. The second round of interviews focused again on overall well-being, goal-setting, and experiences with Dina’s Dwellings, but in order to examine how women experienced Dina’s Dwellings as related to their ability to recover from trauma, the interview protocol was edited to include questions on how women defined healing from abuse.
Interviews and focus groups were conducted in a private room at Dina’s Dwellings, and information about additional services was available if the need arose. Informed consent was obtained before each interview and focus group, and confidentiality was stressed. Women were given Visa gift cards for their participation in the focus groups (US$20) and individual interviews (US$25). Interviews and focus groups were audio recorded, transcribed, and uploaded to NVivo Version 11.4 for data management and coding. All data were stored in a locked private office at the university and on a password protected server.
Analytic Approach
Data analysis was based in feminist grounded theory with an emphasis on reflection (Keddy et al., 1995; Wuest, 1995) and was a collaborative effort among the research team. While feminist grounded research is compatible with various approaches to grounded theory (Evans, 2013), the research team depended solely on constructivist grounded theory to avoid mixing approaches. The goal of the analysis was to develop an in-depth understanding of residents’ experiences with Dina’s Dwellings and how, if at all, they saw housing as related to their healing process. Data collection and data analysis were conducted simultaneous by three members of the research team and followed the procedures of constructivist grounded coding (Charmaz, 2006). The main research question of how housing is related to healing guided both data collection and analysis. Open-ended line-by-line coding of transcribed interviews were conducted in NVivo individually by the researchers. Notes and memos were kept during the data collection period and regular discussions among the research team focused on the creation of categories from open codes, the emergence of possible themes, and revisions to the semistructured interview and focus group guides. Later interviews and focus groups were altered to include questions focused on emerging themes. Relationships among the initial open codes were reexamined and using constant comparison, these were categorized through focused coding. During the last stage of analysis, theoretical coding, the research team worked collaboratively to review categories and synthesize memos to finalize themes and theoretical concepts. Because the number of participants was bounded by the study site, we were unable to follow closely the pursuit of theoretical sampling as suggested by most grounded researchers. As noted previously, the addition of a late volunteer helped in verifying emerging themes and the longitudinal nature of the project added to our ability to clarify our understandings of women’s views and meanings through later interviews and discussions. In this way, our approach follows the guidance of feminist grounded researchers who consider the method to be “evolving and creative” (Keddy et al., 1995, p. 453).
The project was designed to ensure the credibility of our qualitative results through four primary strategies: prolonged engagement, triangulation, peer debriefing, and member checking. First, interviews and focus groups were scheduled to allow for prolonged engagement with the women (Oleson, 1998). All meetings were conducted at the building so in addition to formal conversations, we were also able to observe interactions and engage in small talk with many residents. Because two of the researchers were also interns at the site, they were able to observe additional interactions. Second, we used two data collection strategies, focus groups and interviews, to allow for triangulation of data (Oleson, 1998). Third, conversations within the research team as well as meetings with Dina’s Dwellings staff allowed for peer debriefing (Rager, 2005). Meetings with staff aided in understanding context and validated researcher perspectives. Finally, member checking was an integral part of the research process (Keddy et al., 1995). The third focus group was solely dedicated to reviewing an interim report written for the agency, clarifying quotes presented in that document and eliciting feedback on preliminary codes and findings to help us move forward to the second round of interviews and the final focus group.
Findings
Journeys to Healing
An analysis of the connection between housing and healing depends in part on understanding how residents defined healing from abuse and the specific approaches or actions they valued in helping them heal from their experiences of trauma. Each of the women living at Dina’s Dwellings explained that they are on their own individual journeys to healing and recovering from their past trauma. In the first round of focus groups, we found that women spoke more comfortably and easily about the types of services, referrals, programs, or other supports that helped them as opposed to the ways in which these supports helped them. This discovery and our emerging construction of healing yielded changes to questions and data collection approaches throughout the project. Although their stories were different, four themes or categories of healing emerged: recognizing the impact of trauma and developing coping mechanisms, understanding the time and differences inherent in the healing process, refocusing on and building confidence, and moving on.
Women firstly vocalized that healing meant addressing the impact that trauma has on their lives and learning better coping mechanisms. A few women expressed that in the past they had trouble confronting or admitting the trauma and did not realize how large of an impact it had on their lives. Kayla spoke extensively about coping with her past. In her words, “I just didn’t realize how much the trauma aspect has been affecting my life…[Before] my way of dealing with things was to escape and that is not helpful.” Many women talked about how they are now focusing on addressing the impact of trauma and identifying better ways to cope when problems do arise. Kayla explained further, Healing is also…for me anyway, is finding better coping mechanisms, too. Because [before] I mean I just shut down and you know then I don’t do anything, and everything turns out the way that it has and here I am. Because I went from having my own house and a great job and making great money and you know my own car, I had custody of my child, the whole nine yards and then I just let it all go, you know. And I didn’t care, I just ran away. Because everyone’s situations are different, some people have been through trauma and you can’t take care of a trauma case in 30 days, or 60 days, or 90 days. Sometimes the trauma case could be permanent, you know. So everyone heals differently. Give yourself time, taking one day at a time, don’t put too much pressure on yourself because pressure brings pain too you know so one day at a time, smile more, you know even if you have a bill and you can’t pay it, smile more, you know. Yeah I mean you have to give yourself time to heal, healing takes time, it takes a lot of time.
Finally, a few women expressed that healing also encompassed moving on and that healing would happen when they could move on and accept where they are in their lives. Natasha articulated that moving on is a sign of healing, That’s when I know I’m healed but it’s like…when I can look at the person that hurt me and they don’t faze me or they don’t make me emotional…like feel any type of emotion then I know I have healed from the situation or if I talk about the situation and I don’t show any emotion towards it. I think healing means just being able to move on from the past and find stability and I guess forgiveness, you know forgiveness of situations, people, I mean you don’t forget but you can forgive, which enables you to move on and become stable and accept.
Housing as the Foundation of Healing
When asked how living at Dina’s Dwellings helps them on their journeys to healing, women unanimously agreed on the critical importance of housing. Women were comfortable explaining this relationship from the beginning of the project, allowing for ample dialogue in later groups about the meaning behind their descriptions. All women articulated and connected that having their own long-term affordable residence is a necessity and directly related to their ability to recover from abuse and build independent lives. In this way, Dina’s Dwellings addresses a universal need of all survivors through the provision of affordable, permanent housing.
Residents described how housing gives them a place to call home, a stable and affordable foundation, and a safe refuge to heal. All residents used the word, “home,” to describe their residence at Dina’s Dwellings. In her first interview with us, Natasha explained, I mean the fact that I can call this our home, you know. I don’t see anything wrong with it. I’m comfortable here. I feel safe here. My child’s healthy…safe. We have a place to finally live after the traumatic situation. I mean I pretty much have not had a home for almost four months.
First, the stability of affordable long-term housing, of having a home, was described as an immediate relief from stress and worry. Many women contrasted their current situation with the instability of their recent past. Eva also explained in her first interview, “Because…we have, you know, a roof. Before we used to live in shelters and we experienced a lot of traumas. But until we lived here we finally have a place to live. A place to move.” Some women specifically noted the short time limits of temporary shelters. Many agreed during the final focus group discussion that Dina’s Dwellings relieved the worry of “where am I going to live?” Maria elaborated on the point, And knowing that you can stay…. I mean because 30 days [in a temporary shelter], in my mind I’m like all I’ve got is 30 days! And you’re stressing out. I mean that is paralyzing. [Dina’s Dwellings] opens your mind to where you can sit…almost be able to make plans now. I’m stable so I don’t have to worry about where I am going to live. I’ve been here a year so I feel comfortable now, so now let me start making plans towards the future. It is wonderful, I feel more safe…. I feel so safe. So before when I went to sleep…. I was not sleeping well because I’m thinking somebody will come attack me, especially my abuser. So now I feel so comfortable in here because you know we have cameras, we have a safe place, safe doors, you know, things like that.
Housing as a Platform for Service Provision and Community Building
In contrast to women’s descriptions of having permanent affordable housing, which met a universal need, women did not describe the role of services in similar ways. Healing, as articulated by the residents, is a personal journey. Women discussed the role of case management, programs, and community in supporting their journeys to healing but explained that these supports met individual needs. Thus, needs, preferences, and opinions of service provision and community building were often different for residents and common themes or shared meaning did not emerge from the data. Case management, material support, health services, and community support were coded, but agreement among the women was not strong.
Dina’s Dwellings provides formal supports and referrals for residents with individual case management provided by the case manager, an on-site part-time staff member with an master of social work degree. Women described individual help and support they received from the case manager as supporting their journeys to healing. Eva described,
She [the case manager] is always concerned, and she always tries to help. She always…you know she is the kind of person who…like how are you doing guys, how is school,…how is your child doing?
When asked about specific aspects of Dina’s Dwellings that support their journeys to healing, women mentioned various programs. Some women focused on material support, which then enabled them to focus on their own challenges and not have to worry about meeting basic needs. Maria, who had a young child explained, Not just housing, like she [other focus group participant] said diapers, come get paper towels, you know stuff like that it can be stressful because it…getting it, you can come upstairs and almost go shopping to a certain degree. You know that’s good. This place is beneficial because there is so much that I can do that I can get involved with healing. It’s like when something is going on you know like that soothing or whatever, like get involved with it, kind of like the meditation, like the yoga.
Finally, some women saw Dina’s Dwellings as supporting their healing by meeting emotional and social needs through community building. Dina’s Dwellings aims to facilitate informal supports by building a sense of community and friendship among the residents. Women saw and appreciated the importance of community building activities and programs like resident dinners. Maria explained, “I like all of that. I like the dinners that they have, this way it helps morale in the—where we live and everything here and we get to know each other a little bit more.”
Perhaps based on the unique and individualized needs of the residents, and in contrast to the universality of the need for housing, women discussed concerns and criticisms of some of the support services and community building efforts. A couple women expressed disappointment with the limited nature of case management and programming, mentioning specific, and often individual unmet needs related to employment or education, for example. In this way, detailed descriptions of formal and informal supports were sometimes conflicting, with some residents praising supports while others criticized them. The longitudinal nature of the research also revealed changes across time for the same women. Some of these inconsistences seemed to be related to the unpredictable nature of crises related to IPV experiences such as court appearances, child support disputes, and mental health issues. Such barriers can result in intensive times of needs and the inability to support others. Amber explained, “I try. Each of us, I think, has our own story, our own problems. It’s kind of hard for me, you know, with other people.” Women expressed challenges to forming friendships with other women who are also trying to navigate their own journeys to healing. Brandi explained during her individual interview, Yeah it’s hard because you don’t know what they are going through, you know, you don’t know what is going on with them. They might talk to you, they might not…so I just limit the things I have to say. If I see them I will be happy to see them and that’s it. You can come to the third floor and there is somebody there to talk to you when you’re just like having a mental breakdown, there is always someone that you can speak to, like when…. I’ve never had that until I moved here. So it is kind of like I’m not like so bottled up with so much emotion. Like I used to be very emotional and now I feel free to talk about my life without feeling oh my God it has to be crazy. The housing provides, you know,…it’s a main source of stability. There are stressors and sometimes, you know, there are things that…it’s a new project so there are wrinkles. We’re guinea pigs you know, and sometimes I want to throw my hands up and be like this is ridiculous and too stressful but at the same time I am better off than where I was.
Discussion
Our findings indicate that safe, affordable, and long-term housing is related to the ability of IPV survivors to recover from past trauma and supports journeys to healing. Women in our study describe healing from trauma as possible because of the stability offered by having affordable long-term housing. Residents consider their housing at Dina’s Dwellings to be their foundation, and the constructed subthemes of relief from stress and worry, time to think about the future, feeling safe, and the ability to focus on self-care reflect women’s descriptions of healing and coping. Our findings go beyond past research that establishes the role of housing as related to safety and financial stability. Women in our study experience a strong relationship between housing and recovering and healing from trauma in a more holistic way. Thus, our research pushes us to consider existing trauma and TIC theories and the absence of stability as a variable or aspect in those frameworks. Our case study indicates that housing and the stable foundation housing provides should be incorporated into trauma and TIC theories. Our findings support a broader understanding of trauma theory as espoused by Tseris (2013). Safety as conceptualized in current TIC frameworks is a concept related to security and feelings of safety from harm; the description of safety does not include feeling safe from uncertainty. Our findings suggest that stability is a core component of coping and recovery and should be added to TIC models as either a separate principle or included as an element of safety.
Considering the complex reality of women’s lives in their experiences of trauma, healing, and housing, our findings also relate to the integration of TIC into housing and IPV work. Although we did not directly ask the women about the principles of TIC or PSH, their descriptions of the role Dina’s Dwellings played in their healing journeys reveals many of the TIC and PSH principles already stressed in homelessness services, including trauma awareness, safety, opportunities to rebuild control, and the use of a strengths-based approach (Hopper et al., 2009). The connection between housing stability and recovery from IPV underscores the critical importance of strengthening and expanding trauma-informed practices in housing models. The proper delivery of TIC can facilitate IPV survivors’ pathways toward healing in a safe and stable housing setting, and our findings align with this theory.
Conclusion and Implications
Before considering the implications of our findings, we note the limitations and scope of our research design and make suggestions for future research directions. Our findings are drawn from a small qualitative research project and thus are not generalizable to the experiences of other survivors. Our findings are site and case specific. This lack of generalizability is often expressed as a limitation of qualitative work, but qualitative research makes a different contribution to knowledge building. The goal of this project was to uncover theoretical insights and generate possible hypotheses to be investigated by other researchers. The body of literature on housing and IPV is relatively new. Our findings suggest the need for additional research on the applicability of specific PSH principles and trauma-informed practices to housing for IPV survivors. As discussed above, future research on trauma and TIC should also explore and assess the efficacy of adding stability and housing to their theoretical frameworks. We also did not explore how our findings relate to coping theories outside of the TIC framework, yet we believe this would be enlightening. Finally, although we had regular interactions with the Executive Director and the case manager, we did not formally interview them. A second suggestion for future research is to include their perspectives and insights on model development in this area.
Despite these limitations, we cautiously draw two specific practice implications and one critical policy implication from our findings. First, we suggest that programs focus on casework and advocacy that is designed to meet individual needs. Residents were in agreement that their needs and situations differ from each other. While all residents shared a common identity as IPV survivors, the specific services and supports that each individual woman felt she needed sometimes differed. The small number of women at Dina’s Dwellings and the diversity of their experiences and needs present a programmatic challenge for staff. It is often not feasible for agencies to offer programs or workshops for only two or three women, even if that number comprises a full third of residents. Moreover, many women seemed to benefit from the referrals and connections made by the case manager with outside organizations, particularly in terms of mental health, that more closely matched the unique individualized needs of residents. We thus recommend that small programs in particular focus on providing advocacy and casework to women individually, instead of designing programming that attempts to match the needs of all residents.
Second and more urgently, our findings underscore the critical need to train on and adopt trauma-informed practices. Many domestic violence agencies and shelters are currently adapting procedures with a focus on TIC and beginning to train all staff that might have a need to interact with survivors. For example, maintenance staff who need to enter apartments should understand the impact of trauma and residents’ need for space, and they should be trained on respectful interactions and how to respond ethically to unique circumstances. Trainings should be ongoing or periodic to ensure direct service staff and others including student interns, volunteers, and board members have continued access to and knowledge of best practices and changes in the field. The ability of organizations to remain relevant and supportive of the residents’ journeys to healing depends on everyone, from interns to board members, understanding and working toward best practices that meet the very challenging and diverse needs of the residents.
Finally, as way of a broader policy implication, the central role of housing in supporting healthy and independent lives as indicated by our research underscores the need to address the crisis of affordable housing in the United States. Our findings directly emphasize the need to develop more long-term housing options for IPV survivors. We applaud the efforts of domestic violence advocates in recognizing and developing models that meet this need. However, given that such programs are only open to survivors who have chosen to disclose their experiences and that our findings strongly indicate a positive benefit of long-term affordable housing for all residents, we urge scholars and policymakers to explore and consider the connection between housing and well-being more broadly.
Footnotes
Acknowledgments
The authors thank the women of Dina’s Dwellings, staff and residents, for their willingness to support and participate in the project and for their honest thoughts and opinions. The trust of the leadership of Dina’s Dwellings in the research project is indicative of their desire to improve the program, and we hope the findings gleaned by our research are helpful in the near and far term.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Community–University Research Partnership Grant from the Rutgers Office of Community Affairs.