
Abstract
The aim of this study was to understand how women describe their relationship with their young son(s) in a context of and following intimate partner violence. Face-to-face interviews with eight women were conducted. The analysis suggested that women constructed violence as being a cycle and their relationship with their son was impacted by this in multiple ways. The paper critically draws on attachment, family systems and trauma literature to consider the data in context, and offers a range of clinical implications for practice, training and supervision.
Introduction
Intimate Partner Violence (IPV) is the most common form of violence worldwide and contributes substantially to the global burden of mental health problems (Oram et al., 2022). It has been defined as ‘Any incident of threatening behaviour, violence or abuse (psychological, physical, sexual, financial or emotional) between adults who are or have been intimate partners or family members, regardless of gender or sexuality’. (Sharpen, 2009). In the UK, it is estimated that 1 in 4 women has experienced IPV since the age of 16 (Department of Health, 2013).
It is now well recognised that IPV has a significant impact on all those affected, including children (Oram et al., 2022). In the UK, it is estimated that around a third of children are exposed to IPV (Department of health, 2013). These children are also more likely to be victims of violence themselves (Edelson, 1999), and IPV has been identified as a serious risk factor in child maltreatment and death (Brandon et al., 2008).
Exposure to IPV is increasingly seen as a form of child maltreatment, and it is associated with a range of psychological, social, emotional and behavioural problems (Wathen and MacMillan, 2013). These risk factors included being involved in IPV later in life, with children exposed to IPV being at greater risk of being victims of IPV themselves and, in some cases, is associated with increased risk of perpetration (Ehrensaft et al., 2003).
The current paper is based on a research study that interviewed women with boys in infancy and early childhood (0–5 years) who had experienced IPV from a UK community population. These women had been but were not at the time of interview in a violent relationship, and they and their sons had been exposed to varying levels of IPV. The research question was: ‘How do mothers describe their relationship with their young son(s) in a context of and following IPV?’ This paper presents some of the analysed data from those interviews, alongside a clinically informed commentary on points of alignment and complementarity with, as well as disjuncture from, existing systemic, attachment and trauma theory and empirical research.
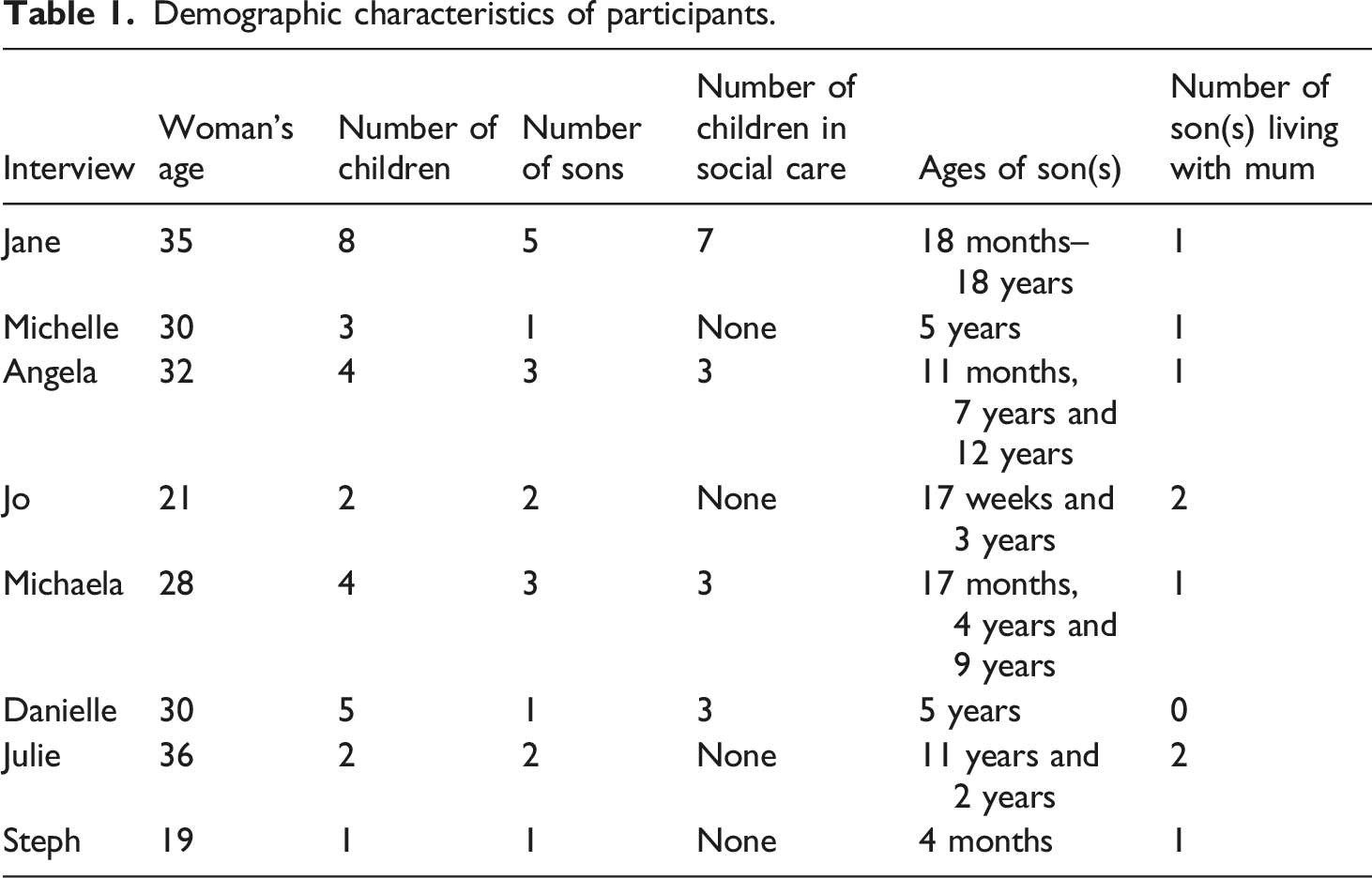
Participant information
Demographic characteristics of participants.
Findings
Violence as a ‘Cycle’ and the ‘Toxic Trio’
Several of the women viewed violence as a ‘cycle’ often based on their own experiences of witnessing IPV as a child and also being abused by caregivers and other adults. They thought that violence and abuse was normal and feared that their son’s would become perpetrators of domestic violence. “But yeah I think that was through learnt behaviour my dad used to hit my mum erm so obviously I’d grown grown up with that and it was normalised behaviour.I know that basically it’s a cycle and a perpetrator erm if a person if a child sees that then it’s going to become normalised and it will make them think that’s normal for them to be witnessing or having that done to them which obviously it’s not and I’d like to stop that cycle.” Danielle “And because I was so young my mum didn’t really give me the attention I wanted, she didn’t give me the proper love I wanted, erm so yeh I turned to him (partner) for that. And me and my mum we’re ok, but we’re not brilliant. My dad was an alcoholic for 35 years, and I’ve seen him going through some rough things. He’s battered his wife.... I’ve seen that.” Angela
The belief expressed here by Danielle reflects a wider discourse around intergenerational patterns of violence, a view that is often also espoused by practitioners and communicated to parents. However the intergenerational transmission of IPV and other forms of familial violence are complex (Renner and Slack, 2006), with proposed mechanisms such as social learning theory being described as too simplistic to have sufficient explanatory power to inform prevention and intervention (Wagner et al., 2019). Family systems theory offers a more ecologically informed, less linear, understanding of violence within families. This includes an analysis of the function of violence in a particular family, as well as how the complex patterns of communication, narratives and feedback loops perpetuates and maintains violent behaviour between different parts of the system (Sammut Scerri et al., 2017). A recent systematic review found evidence to support the use of family therapy in the reduction of IPV (Stith et al., 2022). Ecological models can also take wider social factors into account, linking immediate familial risk factors with the poverty, mental health problems and substance misuse problems that underpin family and community level violence (Hisham et al., 2021). Julie below illustrates the importance of these wider factors that influence mother-child relational development. “Through my pregnancy I was still drinking cos I thought that it would go away (laughs) and I didn’t tell my mum and dad and I was just messed up you know mentally and I think from postnatal depression from (older sons name) and all the stuff that had gone wrong with (older sons name) and (sons name) dad I just didn’t want to believe I was pregnant.” Julie
What Julie also helps us understand, is that while what has been described as the ‘toxic trio’ of safeguarding practice; IPV, mental health problems and substance misuse, all feature in her story, it is important to think of them as coping strategies that have complex interlocking relationships to one another. A recent literature review found that the evidence base for the toxic trio to be ‘alarmingly weak’ despite their ubiquity in policy and frontline practice (Skinner et al., 2021). In Julie’s words, her drinking developed in response to an unwanted pregnancy and interpersonal isolation following a period of mental ill health and earlier relationship difficulties. Crucially, it helps us make sense of her functional problems as it places them in context. However a superficial reading of ‘risk factors’ might lead us to a self-fulfilling bias that neglects other factors, such as Julie’s ability to reflect on her circumstances, and which may offer a more hopeful entry point for intervention.
Trauma responses as adaptive but distracting coping strategies
A central characteristic of traumatic presentations is hyper-vigilance for threat, and in the context of IPV this focus is often on the communication and subtle cues that precede an argument, escalation and attack (Hebenstreit et al., 2015). In the below excerpts Danielle, Jo and Jane illustrate how they attempted to manage their partner’s needs but this distracted them from their children’s needs. “It was just that I was so bogged down with the emotional stress of what’s going to come next erm is he going to be, is he going to hit me? Are they going to want their dinner on the table for this time or that time? Or if I don’t do something right then I was constantly focusing on the actual man instead of the children.” Danielle “It was easier [to be a mother] when he wasn’t there cos I was on my own. I could do what I want; you know I could go by my routine. I didn’t have to worry about him coming in and arguing with me in front of him. I knew that, he [her son] was more settled when he was with me on his own.” Jo “And when he was in it was like shut up, don’t make a noise, don’t play, don’t move, basically don’t breathe or do anything. Er and things like that It was like he was the baby, he had to have the attention and the kids got put to the side, until he had enough attention and he was happy with it.” Jane
The experience of being distracted from the children in the context of fear in the parental relationship was pervasive across the sample, and highlights an important area for practitioners to consider. There is something of a fixation on the ‘maternal gaze’ in early years child policy and practice (Vandenbroeck et al., 2017) that can divert the focus away from wider systemic factors. This can become another burden imposed upon the mother by practitioners, the need to focus on the child without taking adequate account of their context. What is interesting in the above quotes however is that these women are expressing desire to be in relationship to their children, and they find their partner relationship as a distraction. So perhaps it is this adult relationship that needs working with, or at least a structural change to the system, before the maternal preoccupation can be expected to flourish.
Trauma theory emphasises the establishment of emotional and physical safety before trauma processing work can begin (Courtois and Ford, 2016), and similarly here before the mother can be expected to open herself up to her own projections around her child, some environmental stability needs to be put in place. Of course, the difficulty with this is that the assurance of safety is not always easy or even possible for these families, and policy and practice is often focused on working with the mother-child dyad in the environment we would like to see rather than the one there actually is. Perhaps part of this is due to the theories of change they are based on, which are often rarefied, modernist therapeutic approaches that assume a degree of privilege and a secure therapeutic frame. Systemic theory and practice can be helpful in these cases as there is recognition of the practitioner becoming part of the family system, and needing to not try to exercise control over it’s functioning but to, ‘participate in systems in a way that promotes systemic self-control’. (Atkinson and Heath, 1990: 146). This pragmatism, coupled with complex systems thinking, enables practitioners to engage with the family as they are functioning. However the dilemma around families that are managing IPV is, how much can you work with a system that is actively dangerous and where the practitioner has ethical and statutory responsibilities to keep people safe alongside a therapeutic task? Some of the nuances of holding this position are addressed in systemic work that directly addresses IPV (Sammut Scerri et al., 2017) and a fuller discussion of the need for a both/and flexible approach to practice will be elucidated in the implications section. In cases of extreme unpredictability and endangerment however, anything other than functional parenting may be impossible, and professionals are duty bound to act in these circumstances.
Analysis of the data suggested that for some mothers, the trauma related hyper-vigilance described above extended to their sons, both in their relationship and in their maternal representations. “I hated (sons name) when he was born…. I hardly ever cuddled him where as (daughters name) I would. Erm I’d do the necessities but then I wouldn’t even really enjoy doing that erm and I just like… it feels horrible to say you never bonded with your own child when he turned 2 I, I did start loving him but up until then it’s hard to say but I did hate him.” Michaela “did worry me for a little while that it might come between me and him or I might not bond with him as well as what I could be because of what I’d been through with him being a male as well….. In a way it does sort of affect your relationship a little bit with him because I don’t want him to turn out how he was....” Jo
While it is important to note that the two responses are different, Jo is more hesitant about any impacts while Michaela is emphatic, this is an important feature of a trauma response that inadvertently colours the mother-son relationship. When under threat, we respond by generalising and simplifying as our capacity to think reflectively is diminished. When this capacity interferes with our ability to accurately mentalise our child’s needs, it can have a detrimental impact on the dyadic relationship (Ensink et al., 2014). Extending this difficulty to the wider system, IPV has a pervasive negative impact on patterns of relating in general (Cooper and Vetere, 2008), and so we would expect the struggle 'to mentalise is common across the system as well as residing with the mother.
However Michaela and Jo are doing more than making links between the trauma and their ability to attend to their sons, they are also suggesting that they felt differently about them as a result of their gender. Maternal representations of their babies are important in the development of attachment security, and are influenced by the mother’s own relational history (Stern, 1995). They can also be influenced by traumatic events and concurrent stress, in particular IPV, which has been found to affect prenatal representations, their stability over time and the infant’s consequential attachment strategies (Levendosky et al., 2013). The seminal paper on maternal representations, ‘Ghosts in the nursery’ paper describes how a mother’s own trauma experiences can be ‘projected’ into her relationship with her children, potentially leading to an intergenerational cycle of abuse (Fraiberg et al., 1975). A more recent study found that IPV triggers fear and helplessness in mothers, meaning that a child’s ordinary demands can be a traumatic reminder of violence increasing the level of stress in the mother and impacting her responses to the child (Levendosky et al., 2011). The role of the abuser can be ‘projected’ onto the child who is subsequently perceived as being abusive and found that women who experienced IPV were more likely to have non-balanced perceptions of their child as measured by a semi-structured interview (Huth-Bocks et al., 2004). Non-balanced perceptions are characterised by a sense that the parent does not really know the child or the child is seen as serving to meet the parent’s own needs. In attachment theory terms, we might think of this as the parent being both frightening to the child, while frightened themselves (Lyons-Ruth et al., 1999).
While the above research-based formulation fits with the data presented, there is a mechanistic and deterministic quality that needs to be critiqued. While it is helpful for us all to think about our projective processes that shape our internal working models and influence how we relate to other people, there is a pathologising quality here that is othering of these parents. Part of the benefits of a trauma focused approach to understanding the lack of ‘balance’ described above is that it emphasises the adaptive, survival oriented quality of trauma responses even if they are also maladaptive in other contexts (Sweeney and Taggart, 2018). This recognition of the necessary distraction the IPV has created, provides a platform for the mother to have her own experiences and responses validated which can then create a space to think about their representations of the child. This is very much in line with Patricia Crittenden’s attachment based approaches to working with parents, which prioritises the need to acknowledge and validate the parent’s needs before expecting them to do the same for their children (Crittenden, 2008). For practitioners working with a family where there are active risks of IPV however, the time needed for such delicate work to happen and take root is often lacking and this is one reason that parental history and current needs are neglected in the face of immediate concerns about child safety.
Other aggression in the family
Some of the women noticed an increase in aggression from their sons and wondered about this being linked to their exposure to IPV. The women reported that this aggression was directed towards them, siblings and peers at school. “Erm, the main problem we had with him at first was his behaviour, erm a lot of like hitting other children, snatching, shouting, you know trashing toys and stuff.” Jo “Sort of or I’d send him to his room cos he would kick me, bite me, pinch me, pull my hair and you couldn’t say no to that boy.” Michaela
The mothers perspective on this broadly fits with the evidence base, exposure to IPV in preschool children more than doubles the risk a child will have significantly aggressive behaviour by the time they start school (Bowen, 2017). While part of using aggression to meet needs and communicate demands is developmentally appropriate for young children, exposure to IPV makes it more likely to persist into school years and result in particular difficulties in expressing remorse, uncaring behaviours and a struggle to express emotions (Oram et al., 2022). While there is reasonable evidence that parenting interventions can help alleviate these difficulties, the families who most need these interventions are the least likely to access them (Minnis, 2019). Service access was certainly an issue in the community these women were from, and this has likely got worse in subsequent years of cuts to early years provision. An additional layer of complexity for practitioners to consider is, given the trauma hyper-vigilance we explored above, how easy will it be for parents to engage in an educational programme like the Incredible Years which requires concentration, attention and emotional engagement, all things that might be difficult characteristics to muster in the context of IPV.
Women with both sons and daughters described how witnessing IPV appeared to affect their children’s behaviour differently with boys responding in an external way and girls responding by avoiding violence or taking on a caring role. “See I, I,I do think it is different the way it impacts on girls and boys because obviously (daughter) saw that as well and being female I think it is different between a girl and boy because (daughter) she will totally like if she sees something violent or something like that she’ll shy away from it.” Michaela “Yeh because with the boys like when, when, when I had the 5 youngest ones with me and I used to go to the park or somewhere, if a bloke looked at me like in a nice way, (son) would say don’t fucking look at my mum. I’d fucking hit ya and, and you know, you know and I’d be like (son)! Don’t swear there’s no need for that, you know.” Jane
Sometimes the women described their son’s behaviour using wording that was directly linked to the perpetrators’ behaviour. “Being verbally abusive to me…Smacking his sister, pushing me er if I asked him to do something er instead of him going ‘Yes mummy’ like he normally did. He’d be like no, so he’d become quite verbal(ly) abusive to me.” Michelle “He knows how to hurt me you know mentally I think [her 11 year old son].” Julie
Again, the mother’s descriptions here broadly echo the population level research evidence in gender differences in response to exposure to IPV when combined with other forms of childhood maltreatment. Exposure to IPV and/or direct physical or sexual abuse doubles the risk of men perpetrating IPV and of experiencing IPV for women (Whitfield et al., 2003). The cited study is one of the hugely influential Adverse Childhood Experiences Studies (ACEs) and is based on associations between different forms of early adversity and adult outcomes. The ACEs research has been helpful in drawing attention in mental health to the psychosocial context of distress, but has been roundly critiqued as an overly deterministic and crude measure of life chances that ignores social context and blames parents for societal problems (White et al., 2019). Part of the difficulty with the application of this research evidence, is not the actual science itself, but the enormous claims it has made about the origins of a host of complex social problems and the influence ACEs research has had on policy and practice.
In the case of this study, an uncritical acceptance of ACEs research on IPV would be to identify ‘at risk’ boys in a way that could be deterministic and create a harmful family script around their development, which sees them as miniature versions of dangerous men. This creates a risk of stigma and offering these young boys limited other life scripts they can follow, meaning aggression, when it occurs can become pathologised and a self-fulfilling prophecy. While the sample of mothers and children in this study were all white, this type of stereotyping and prejudice is something young black boys are at particular risk of (Goff et al., 2014). So while the research might present itself as ethically neutral, there is a labelling effect when it is applied to individuals that mirrors the longstanding problems with certain forms of psychiatric diagnosis such as Borderline Personality Disorder, whereby it can impact prognostic optimism and is therefore counterproductive (Lomani et al., 2022).
Change to the system creates new struggles
Intimate partner violence is the primary concern in around half of all Children in Need in the England (National Statistics, 2021). Half of the women had previously had children taken into care, although all had at least one child living with them at the time of interview. In most of the cases where the women had their children taken into care this occurred after they had left the relationship. The women discussed the pressure from social services to leave the abusive relationship and all of the women there mentioned social services involvement. However, once they had left the abusive relationship, their relationship with their son(s) did not always improve. As Jane describes, it led to a shift in the family system but not the disappearance of violence as a way of establishing control. “Yeh the first time (son) ever touched me cos normally, if the kids got out of hand like that and they raised their hand to me or their voice or anything then [dad] would give them a crack up the head…. And put em back, knock em back down to size, sort of thing you know. He wouldn’t let them disrespect me…But because he wasn’t there, he thought well I’m the man of the house; I can do what I wanna do now [her 13 year old son].” Jane
From a systemic perspective Jane’s description makes sense as a way that the system finds a form of homeostasis that brings with it balance and consistency. Another way to think about this is that as the father leaves the family in the wake of IPV, a triangulating function for the oldest child is to increase his level of aggression to attempt to pull the father back in again to regulate the system (Dallos and Vetere, 2012). This is a way of seeing the older boys aggression as functioning not as a form of social learning, nor merely as an enactment of a family script, but rather as an expression both of his own complex attachment strategy to manage danger (Crittenden, 2008), and intervening indirectly in the parental relationship. The complexity of this belies the understandable but misguided belief that removing the father will result in a peaceful home. For practitioners working in the context of IPV making structural changes to the system to promote safety, a key question is, when you take someone away, what needs to be put in place to manage the gap they leave?
A number of other mothers also identified the point of departure of the father in the wake of IPV as the beginning of other difficulties for the family. “Yeh erm I lost all my confidence, I didn’t want to go out, I couldn’t make any friends, erm I was stressed all the time, I was worried, I was getting paranoid. And er, yeah yeah it did have a massive impact on me…. And erm because I was diagnosed with depression as well I thought that would go against me [fear of social services].”” Michelle
The collapse that Michelle describes here will be familiar to people who have survived chronically stressful life experiences, only to find themselves crash at the point where the immediate danger diminishes (Courtois and Ford, 2016). It adds further weight to the argument we make above that while removal of the male partner might be important in cases of IPV, it does not follow that this will resolve the challenges the family faces. The fact that several of these mothers had their children taken into care after the departure of the father is an indication that there were additional pressures once they had complied with the advice of social care practitioners. It also represents something of a betrayal of trust for mothers if they had been told they should break off their relationship with the father in order to prioritise the children’s needs leaving them with nothing in the end to show for it.
The issue of trust in these relationships is a cogent one, as lack of parental engagement is the most commonly referred to difficulty in Children’s Services case files (Mason et al., 2020). Given that a high proportion of these mothers also have histories of interpersonal violence, often from attachment figures, and we can anticipate low levels of epistemic trust in a toxic combination with institutional untrustworthiness, making good working relationships very difficult (Mason et al., 2020). The tension at the heart of much social work practice, that of the need for care and control, can result in intra-psychic and organisational splits whereby the care is all devoted to the ‘innocent’ children while the ‘guilty’ parents are subjected to controlling demands to change. This is an understandable reaction to the at times unbearable pressure these practitioners are under, the lack of reflective supervision and support in many services, as well as the material reality of the serious risks children face in some families. However it does represent a psychological defence that cannot keep in mind the fact that many of these parents were once innocent children themselves and were often failed by the very legal structures designed to protect children and which they now experience as coercive. While it would be hubristic to pretend here that there is an easy solution to these tensions, it is important to acknowledge the centrality of relationships in this work and that in the absence of trust it is very difficult for parents to meaningfully engage in the painful work that is needed to restore safety.
The interview as a process of reflection
This final section concerns the process of conducting the interviews themselves. They all took place after leaving the relationship but it appeared that some of the women were able to reflect more than others on what the experience of IPV might have been like for their son(s) and how this impacted on the mother-son relationship. It appeared that realisation of the impact of domestic violence on the son(s) and further reflection on this occurred as women were ending the cycle of violence (often in response to spending time thinking and talking in therapy or with friends and family) and is likely to be a process that continues. Some of the interview material suggested that the women were continuing to reflect in the context of the interviews. It is likely that this process of reflection is not linear and some of the women appeared to oscillate between denying any impact to a realisation of the impact along with feelings of guilt. These variations in insight into the impacts of IPV on themselves and their children can be understood in a range of ways, as failures of mentalisation and reflective functioning as described earlier in the paper (Fonagy and Allison, 2012), but also as psychological defences designed to manage the shame of failing to adequately protect their children form harm. There is also the interpersonal context of the interview itself, where the women were justifying what has happened to another professional (the researcher) asking them questions about a difficult and private area of their lives. In the Meaning of the Child to the Parent Interview, which assesses parent-child relationships through a semi-structured interview with parents, contains a facility to code for the influence the parent attempts to have on the interviewer (Grey and Farnfield, 2017). While parental behaviour in assessment settings lacks ecological validity, it can be a useful way to think about how defended the parent feels the need to be in how they present their family life.
For some there is still a ‘denial’ or a wish that their son was protected from witnessed anything. It appeared that it was difficult for some of the women to recognise the experience as potentially traumatic for their son(s). “I don’t think he’ll be affected by it too much cos I don’t think you have any memories until you’re about 3 anyway do you so erm hopefully he’s not affected by it too much. Hopefully he won’t be a perpetrator of domestic violence.” Danielle “I don’t think so because I tried to hide my feelings from him.” Julie
In the excerpts from Julie and Danielle, we can see the uncertainty and anxiety in their defensive reaction to considering the impacts IPV might have had upon them. The memory issue is a commonly cited one by parents whose children have suffered adversity; that it does not matter because they will not consciously remember them. Beyond the well-established evidence presented throughout the paper that exposure to IPV in infancy and early childhood does have a detrimental impact on psychosocial development (Oram et al., 2022), it is helpful for practitioners to be curious about what functions this defensiveness serves. This can also help us avoid getting into theoretical debates about parenting and child development with parents that impedes the work of establishing trustworthy working relationships. One possibility is that it is borne of a strategy to manage feelings of shame at having failed as mothers. It has been argued that parents in Child Protection proceedings face profoundly shaming experiences that lead to a range of acting our behaviours, including angry denial and minimisation of difficulties (Gibson, 2015). In a sociological piece on mothers who lose their children in the court arena, Lisa (Morriss, 2018) describes them as ‘abject figures’, deeply stigmatised, and not seen as legitimate mourners due to their perceived failures as parents. In response to this stigmatised identity (what in our society is less revered than a failed mother?), it is necessary to find external sources of responsibility and to minimise the harm caused, in order to maintain an acceptable identity. The lack of conviction in the quotes presented above are reminiscent of another study interviewing mothers who had children taken into care, where there was an attempted expression of an ‘unspeakable shame’, that resulted in the research participants tailing off in their speech mid-sentence and emotionally shutting down in reaction to the pain of it (Siverns and Morgan, 2021). One implication of this is the need for services to reduce the burden of shame these parents are exposed to (Gibson, 2015), possibly through the implementation of dignity conferring processes which have been presented as the affective opposite and therefore one antidote to shaming institutional responses (Salter and Hall, 2021). It has been argued that the current vogue for trauma informed approaches, often critiqued for lacking theoretical specificity (Sweeney and Taggart, 2018), needs to be more focused on shame sensitivity in order to effectively engage people with interpersonal trauma histories (Dolezal and Gibson, 2022).
In something of a contrast, four of the women were able to reflect in detail on their son’s experience of witnessing domestic violence. These women were also potentially further along on their journey of making sense of IPV. “Erm he hasn’t said anything about it, erm but I think he is aware. I think he does realise because of how his behaviour was up until we started working with him. Erm so I think he does know, I think he’s seen what’s gone on and he’s thought that that’s ok. Erm yeah even though he hasn’t said nothing I don’t think he forgets I think he knows.” Jo “And it’s made me think like that as well and especially I’m determined to get this over before he understands anything that’s going on and I hope to think I’d never tell him until he’s old enough to, I don’t know I might not tell him I’m not too sure about that yet. I’m just going to see what sort of little boy he is when he grows up that understands that sort of stuff I just don’t want him being that sort of person.” Steph
These women also recognised their son’s confusion that they would have experienced when witnessing IPV but being expected to behave in a different way. “So and he er refused to say sorry and I had to explain to him that that sort of behaviour isn’t normal so but it must be hard for him to explain… like to understand that rather when that’s what he’s seen as he’s grown up…It was hard for me to let him know that hitting his sister or hitting me was not the right thing to do because the next day or hour (ex-partner) would come round and do exactly the same thing that he was doing. So it was really hard for me to try and tell him that you know it’s wrong.” Michaela
One of the most pertinent clinical questions arising from this contrast between different mothers, is what are the personal characteristics, contextual factors and variations in experience of IPV that lead to contrasting ability to reflect on its impacts? While the current study was not designed to directly answer that, it is worth considering the wider literature. In one study that looked at maternal representations in the context of IPV, it was found that the personality traits of openness and agreeableness increased the chances of balanced representations at 1 year (Lannert, Levondosky & Bogat, 2013). While intra-psychic measures such as these are important in understanding what characteristics and qualities need to be encouraged to enable mothers to represent their child’s experience in the context of IPV, they are limited through the lack of systemic focus. The value in a systemic approach to understanding IPV, is in its broader focus, not only on the family dynamics, but on the social, political and economic contexts in which it occurs (Sammut Scerri et al., 2017). While this multi-dimensional, ecological focus can lead to a divergence in views around how best to respond to IPV, it does mean that the inclusion of mother’s individual traits can be mitigated through a socio-political perspective, which undermines the development of victim blaming narratives (Morriss, 2018). A final note on the differences is related to the time since they left the abusive relationship and the help they have received. While these were not included in the analysis, it is important to note their importance in the recovery of reflective functioning.
A note on fathers
While we attempted to take a broadly systemic focus in our understanding of what these women told us, we have also left an important perspective out of our paper, that of fathers. Recent systemic theory has written about the need to work with parental dyads in the aftermath of IPV, once a cessation of violence has been secured (Sammut Scerri et al., 2017; Lawick and Groen, 2009). This better reflects the clinical reality that these families are often bound by complex bonds that are not easily breakable through state intervention or social engineering, even when professionals or the courts feel that is the safest outcome. This also brings to the fore of our minds a practice question that is often not asked; who are these fathers and what has led them to hurt their families?
A recent study of fathers who have lost their children following court proceedings in the UK, found that the backgrounds of these men had much in common with the mothers they partner with (Brandon et al., 2017). A large minority had been through the care system themselves, and almost all had suffered significant childhood adversity and exposure to IPV. Perhaps more surprisingly, they were also likely to remain with the same partner even after the children were removed, challenging the stereotype of absent fathers, moving from partner to partner and leaving mothers to pick up the pieces. Crucially for this study, some of them had been violent and IPV was a risk factor in several cases, but they did not present as ‘pure’ perpetrators and in the research transcripts were able to express remorse and shame for their acts of violence (Brandon et al., 2017). The risk of IPV also appeared to be linked to the sorts of feelings of shame and humiliation that appeared to drive defensive reactions in some of the mothers accounts quoted above. While this is not an equivalent risk factor, it does point to the relevance of shame sensitive practice for fathers too in the prevention and treatment of IPV (Dolezal and Gibson, 2022). Suffice to say, their absence from this study is an omission that risks increasing their marginalisation in this area and research asking about their views on their sons in relation to IPV could act as a useful adjunct to this study. The issue of reintegration of fathers to the system once IPV has ceased is delicately handled in the systemic literature (Sammut Scerri et al., 2017), and reflects an important reality, that in spite of our phantasies of ridding the family of the aggressor, these men are still around in the community and so exert influence even in their absence from the home.
Implications
While we have discussed a range of implications throughout the paper, we wanted to conclude by offering some further practical applications for practice, as well as for the training and supervision of practitioners. We intend to be inclusive in our suggestions, hoping this will be of relevance and value to social care and health practitioners, as well as those with formal psychotherapeutic training.
The social policies that have been enacted in the years since this research was conducted have further eroded the community resources and value placed on families with young children. The closure of Children’s Centres and other forms of austerity, in communities like this one, can be understood as a form of state violence enacted upon families struggling with intergenerational adversity and disadvantage (Taggart et al., 2017). It is difficult to credit that this societal level violence, described by the late Scottish community activist Cathy McCormack (Fryer and McCormack, 2012) as the ‘war without bullets’, is unconnected to the violence that occurs in communities and family homes. As research has shown IPV and parent-child violence (Tsai, 2012), is an illness of poverty as much as individual pathology, and it is important practitioners do not lose sight of this in the desire to focus on a part of the system they have influence over.
From a practice perspective, one of the skills needed to work with mothers and sons in the context of IPV is the ability to understand problems in the relationship in a trauma context. Focussing on the adaptive function of hyper-vigilance, preoccupation and emotional lability, can prevent clinical pessimism about parenting capacity, by instead recognising that the trauma reactions can change as safety increases. We would encourage practitioners to use theories such as mentalisation, maternal representation and reflective function in a way that recognises their state dependence rather than stable traits. Furthermore, the research evidence and the accounts of the women in this study would suggest that there may be some basis for their concerns about son’s acting out aggressively in the wake of IPV. However, here again, a systemic perspective that emphasises the dynamic nature of this strategy in managing the needs of the system, and as a possible expression of attachment need is more helpful than a deterministic philosophy that engenders prognostic pessimism (Dallos & Vetere, 2012; Cooper & Vetere, 2008).
Creating shame sensitive service contexts can be helpful in enabling parents to acknowledge the losses and harm they have all faced as a result of IPV. The promotion of dignity conferring processes in practitioner-parent relationships, can encourage parental engagement and enable therapeutic work around delicate topics such as responsibility for childhood maltreatment to occur without overwhelming narratives of blame taking hold.
Finally, in order for any of the above to happen, practitioners themselves need to be well supported, with regular reflective supervision and training. Rates of childhood adversity have been found to be higher among health and social care professionals, when compared to the general population (Esaki and Larkin, 2013). One psychological mechanism that may bring practitioners into the field is their own experiences of IPV, as children or adults. It is important this possibility is taken into account when recruiting and training practitioners, not as a red flag but rather as another systemic factor to be considered when teaching and supervising on the topic of IPV and exposing practitioners to this work post-qualifying. While reflective practice in training and supervision can create conditions whereby practitioner disclosure can be safely managed and thought about in terms of practice, there is still stigma within services about staff vulnerability (Horsfall et al., 2010), and it should not be left up to the individual to take responsibility for raising it. Creating training and service cultures where the ‘us and them’ of systemic practice is challenged can both destigmatise families who are struggling with IPV, while also making it possible for practitioners to consider their own family histories and to think openly and reflexively about how this might influence their own positions.
In conclusion, we hope that the generosity of the women in this study to offer their stories can add further layers of complexity to the field of IPV. We particularly want to conclude by drawing attention to their commitment to try to parent as best they could in challenging circumstances, and that they continued to try to make sense of their experiences in the research interview itself. The process of writing the paper has led us to reflect on our own family relationships and we hope we have represented the struggles of these families in a spirit of humility and solidarity. We feel this ongoing meaning making provides grounds for cautious clinical optimism that if well engaged, therapeutic change for families is achievable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.