
Abstract
This study examined surrogate women’s perceptions on the Indian ban on international surrogacy. In-depth interviews were conducted with 25 surrogate women at a fertility clinic in Gujarat, India. Three themes emerged: (1) perceptions of the ban; (2) impact of the ban on surrogates, international couples, and fertility clinics; and (3) long-term economic results of surrogacy. Women stated that international surrogacy should not be banned, because it provides substantial economic benefits. They also noted that the ban affects childless couples and clinics by cutting off a source of income. This research provides recommendations for social work action.
Until 2014, India was the primary global destination for commercial surrogacy. Over the past two decades, the Indian transnational surrogacy industry had grown into a thriving enterprise, as reproductive tourists (largely from the United States, Canada, and the United Kingdom) sought out the low costs, modernized medical infrastructure, lax regulations, and abundance of surrogate mothers offered in India (Chang, 2009). Reproductive tourism, an aspect of general, medical tourism, is defined as the “traveling of [intended parents] from their country of residence to another country in order to receive a specific treatment to exercise their personal reproductive choice” (Ferraretti, Pennings, Gianaroli, Natali, & Magli, 2010, p. 261). It is estimated that over 25,000 children have been born to Indian surrogates, primarily for intended parents (IPs) from high-income nations (Shetty, 2012).
The varying legal status of surrogacy between countries challenges international ethical norms and regulations (Crockin, 2013). It is well recognized by scholars that potential harms to all parties involved can be avoided through government regulation, rather than illegalization (Ekberg, 2014; Wilkinson, 2016). Yet, almost 15 years after India first legalized commercial surrogacy, the Indian Ministry of Health and Family Welfare, through its Department of Health Research, passed the Assisted Reproductive Technology (Regulation) Bill of 2014, making it illegal for women to become surrogate mothers for international IPs. While this legislation will impact the medical tourism industry of India, a more direct impact may be experienced by surrogate mothers (Perappadan, 2015). Further, adverse consequences, such as clandestine and/or harmful surrogacy arrangements, may place surrogate women at more risk than before (Shetty, 2012; Wilkinson, 2016).
Evolution of Commercial Surrogacy in India
India first legalized commercial surrogacy in 2002 (Chang, 2009). Over the course of 15 years, the Indian surrogacy industry had become a US$2.3 billion a year business (Shetty, 2012). It is estimated that over 600 artificial reproductive technology clinics are located throughout India, including both urban and rural areas (Deckha, 2015). Thousands of children have been born to Indian surrogates. In the United Kingdom alone, 1,000 children are born to Indian surrogates every year for IPs from the United Kingdom (Blyth, Crawshaw, & van den Akker, 2014).
India had become a “hot spot” for transnational surrogacy, in part due to the Indian government support for an unregulated surrogacy business. Since the 1990s, the Indian government had actively encouraged reproductive tourism to India as a way to increase gross domestic product growth. For example, the Indian government offered subsidies for clinics and hospitals treating overseas patients (Deckha, 2015). Medical services offered in India are quite attractive to IPs from highly developed countries. Not only does India have advanced medical technology and traditionally high standards of medical care, the cost of medical procedures is much lower than the cost of the same procedures in the United States or other high-income countries (Deckha, 2015). Further, no formal regulations existed on the commercial surrogacy industry (Shetty, 2012), and the processes of the industry were largely formed by market forces (Deckha, 2015). This is attractive to internationals who want to avoid legal hurdles and bureaucratic red tape, while saving money.
The lack of national oversight of the international surrogacy business had put the power to define guidelines in the hands of fertility clinicians who could potentially put their financial needs over the health and safety of surrogates. Despite the push for medical tourism, the government never fully addressed the social, economic, and political conditions in which women function and make decisions about employment. For instance, fees, policies, and surrogacy contracts varied from clinic to clinic (Bailey, 2009). The Indian government failed to establish regulatory control over the surrogacy industry, resulting in a lack of consistency between clinics.
Ethical Issues Surrounding Transnational Surrogacy
Since the popularization of commercial surrogacy, stakeholders have voiced concerns about the possible exploitation and coercion of surrogate mothers (Deonandan, Green, & van Beinum, 2012; Pande, 2011). Specifically, researchers have highlighted several issues regarding transnational surrogacy involving relatively wealthy IPs from high-income countries and surrogate mothers from developing countries (Wilkinson, 2016). In these cases, exploitation of poor women is especially pressing, and payment for services is often scrutinized. Indian surrogates are paid, on average, between US$3,000 and US$5,000, compared to U.S. surrogates who make between US$20,000 and US$30,000 (AUTHOR et al., 2014; Bailey, 2009). However, the salary generated from commercial surrogacy is often equivalent to 10 years of typical salary among poor women in India (Shetty, 2012). This amount is drastically more than what a typical woman would make in full-time employment. Although the amount for services is justified, given the work required, it is of concern when it could mislead or coerce women to become surrogates.
Another concern is the treatment of India surrogates during pregnancy. Several accounts have detailed “surrogate hostels” in which women are housed in clinical compounds (Panitch, 2013; Shetty, 2012). In these hostels, women’s meals, activities, and health are closely monitored. Surrogates’ contact with their families and own children is often controlled as well. Complaints of poor food and water quality, overcrowding, sanitation, and hygiene have been conveyed to several researchers and journalists. However, because there are no regulations, some hostels are worse than others, and clinics often deviate from their roles as solely health-care providers to become “surrogacy agencies” (Shetty, 2012).
Similar to other pregnant women, obstetric risk and possibility of complications are present (Dar et al., 2015; Parkinson et al., 1998). Unlike other pregnant women, surrogate mothers may face increased risk of adverse psychological effects (FIGO Committee for Ethical Aspects of Human Reproduction and Women’s Health, 2008; Soderstron-Antilla et al., 2016). Further, even when clinicians inform surrogates about the risks of surrogate pregnancies, many neither comprehend nor remember the information (Tanderup, Reddy, Patel, & Nielsen, 2015). Primary motives for becoming a surrogate differ between contexts. In western setting, surrogate mothers’ motivations are often altruistic (Imrie & Jadva, 2014; Jadva, Murray, Lycett, MacCallum, & Golombok, 2003). Among India surrogates, however, financial factors are often the primary motivation for surrogacy (AUTHOR et al., 2014), which may add to the context of exploitation.
Assisted Reproductive Technology Regulation Bill of 2014
The Assisted Reproductive Technology (Regulation) Bill of 2014 was passed in response to growing concerns of ethical exploitation of surrogate mothers and was designed to provide comprehensive regulation of the industry for the first time (Dey, 2015). However, it instead banned the use of surrogacy for one of the largest consumer groups (international IPs) and directly affected women who benefited financially from surrogacy. Scholars have warned against banning commercial surrogacy for fears that it will send the industry “underground” (Wilkinson, 2016). In places where commercial surrogacy is illegal, there are problems with the legal status of children, more opportunities exist for organized crime, and adverse effects occur to surrogate women (Gamble, 2009). Despite these warnings, the Indian government criminalized transnational surrogacy.
Indian news outlets report that the bill came as a shock to doctors who believe the bill will be detrimental to the surrogacy business (Dey, 2015; Perappadan, 2015); however, little is known regarding surrogate mothers’ reactions to this bill and how they perceive it affecting their lives. The majority of the surrogate mothers in India have become surrogates multiple times and relied solely on the income generated by surrogacy for themselves and their family’s well-being (AUTHOR et al., 2014). After the ban, it is not known if these women have explored alternate solutions to income generation and the impact of the sudden ban on their economic livelihoods. The purpose of the current study was to highlight surrogate mothers’ perceptions regarding the ban on international surrogacy instituted by the Indian Assisted Reproductive Technology (Regulation) Bill of 2014. Our objective was to explore surrogates’ thoughts and understanding of the ban, its impact on the livelihood of surrogate mothers, and its impact on international IPs and clinics across India.
Methodology
Study Setting
Gujarat, a western Indian state of approximately 60.8 million people (India Vital Statistics Division, Ministry of Home Affairs, 2013), is home to a booming transnational surrogacy industry. As described by media outlets and investigative journalists, Gujarat has become known throughout India and the world as the country’s “surrogacy capital” (Ajay, 2014; Bindel, 2016; Doshi, 2016; Tagnik, 2013). We partnered with one fertility clinic in Gujarat that has been attributed with delivering over 1,000 babies created through surrogacy. The clinic, set in a small, somewhat rural location, operates a state-of-the-art hospital (with an adjoining surrogate hostel) and hires approximately 75 surrogates at any given time.
In the past 10 years, Gujarat has seen substantial growth in standards of living. For example, the percentage of households with electricity grew from 89% to 96%, the percentage of households using improved sanitation facilities grew from 44% to 64%, and the percentage of households using clean fuel for cooking grew from 40% to 53% (Ministry of Health and Family Welfare, Government of India, 2016). However, women continued to experience low levels of literacy throughout the region (73%)—compared to men at 90% (Ministry of Health and Family Welfare, Government of India, 2016). Further, less than three fourths of the female population aged 6 years or older have ever attended school, and less than one fourth of women have 10 or more years of schooling (Ministry of Health and Family Welfare, Government of India, 2016). In sum, despite increases in economic development throughout the region, women and girls operate within a state of systemic inequality and gender oppression.
Study Population
We used purposive theoretical sampling to identify women from an existing database of previous commercial surrogates who had been hired as surrogates for international IPs. The second author of the article had a previous collaborative relationship with the clinic who assisted with participant recruitment. Eligibility criteria included being a surrogate for an international IP at least once, older than age 18, and able to give informed consent. Women were contacted by clinical staff, provided details about the study, and scheduled for an interview, if they were willing and interested in the study. Oral informed consent was obtained prior to the start of the interview, because most women are illiterate. The institutional review board at The Ohio State University approved the research protocols. The aim of the study was explained to participants and each participant was compensated 1,000 Indian Rupees (INR; equivalent to US$15.00) for participation. In total, 25 women were recruited and interviewed for this study.
Data Collection
Data collection occurred throughout June 2016. The second author conducted all data collection through semistructured interviews in Hindi or Gujarati, which lasted approximately 45 min. The second author is Indian, fluent in Hindi and Gujarati, has extensive training in qualitative interviewing techniques, and has prior experience conducting qualitative studies in India. The second author recorded, transcribed verbatim, and translated interviews to English for analysis. The second author is familiar with the cultural context and was able to include indigenous constructs in the translations. No issues arose in the ability to effectively translate the interviews from Hindi/Gujarati to English. On the basis of a review of the literature and previous experiences, six topics were identified for exploration. Women were asked about their motivations to become a surrogate, experience as a surrogate, perceptions of the ban of transnational surrogacy, including the cause and impact, the result of surrogacy in their lives, social consequences of surrogacy, and background information. A semistructured interview guide with open-ended questions and follow-up prompts was utilized to guide the discussion, but participants were free to speak on any matter they deemed important (Creswell, 2009).
Data Analysis
We used a qualitative, phenomenological approach called narrative analysis, with the goal of assessing participants’ perceptions and meanings of phenomena through the way in which they discuss their lived experiences (Creswell, 2009). We wished to stay close to the participants’ words and understand how participants’ stories were shaped by the political context in which they live (Moustakas, 1994). This allows for deeper meanings of a phenomenon to be observed (Padgett, 2008). Participants were able to describe their experiences and have their stories be the focal point of the analysis.
Data analysis focused on discovering common themes in participants’ experiences and the conditions of those experiences (Padgett, 2008). To accomplish this goal, we followed the Stevick-Colaizzi-Keen method of phenomenological analysis (as citied in Moustakas, 1994). First, verbatim transcripts were read line by line several times, with the goal of understanding the opinions of women on the surrogacy ban. Next, all relevant statements were coded and recorded. All nonrepetitive statements were listed. Then, each statement was clustered into categories. Categories of statements were grouped into themes with similar meanings of the experience. Finally, themes were synthesized into a description, and verbatim excerpts were used to highlight each theme. All participants were assigned pseudonyms for research purposes. In the results, participants’ comments are introduced or followed by one of these assigned pseudonyms.
Results
Participant Characteristics
On average, the 25 women included in the analysis had been surrogates about 1.3 times, resulting in 32 reported surrogate pregnancies (Table 1). The age of the participants ranged from 26 to 45 years (M = 32), and the vast majority were married. The women had, on average, about 1.9 biological children, primarily conceived before surrogacy work. Of the women who reported mode of delivery for each surrogate pregnancy (N = 26), almost all had a cesarean section (89%), even though most biological children were delivered vaginally. In addition to surrogacy, eight women (32%) had worked as paid egg donors. Most women were homemakers or unemployed; although, some had found employment at the fertility clinic in which they participated as a paid surrogate. Employment at the fertility clinic often included positions as surrogacy recruiters and domestic helpers for cleaning and cooking at the surrogate hostel and the hospital.
Participant Characteristics.
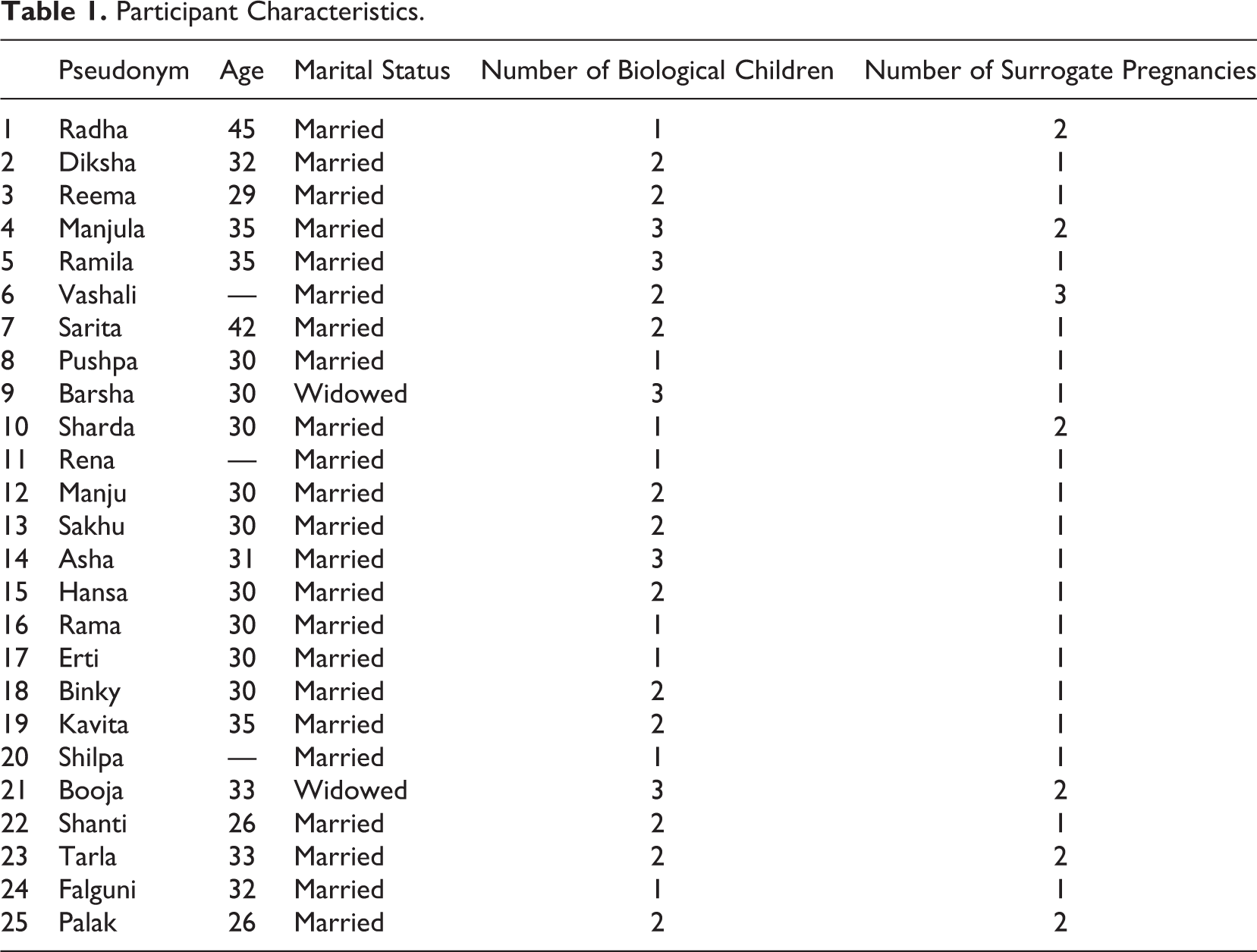
On average, women reported that they had been paid approximately 492,000 INR (with a range of 253,000–1,000,000 INR) for surrogacy work for international couples. These values are equivalent an average of US$7,230.00 and a range of US$3,750.00–14,800.00. In contrast, for surrogacy work for domestic couples, women reported having been compensated an average of about 490,000 INR, with a range of 375,000–650,000 INR. Corresponding USD amounts are US$7,200.00 and US$5,560.00–9,640.00, respectively. Country of origin of international IPs included America, Japan, Canada, South Korea, Ireland, United Kingdom, Singapore, and Iraq. Additionally, four women reported being a surrogate for Indian IPs.
Narrative Themes
The main themes in the women’s narrative were (1) surrogate mothers’ perceptions of the surrogacy ban; (2) impact of the ban on surrogate mothers, international IPs, and fertility clinics; and (3) long-term economic results of surrogacy.
Perceptions of surrogacy ban
Every participant resoundingly expressed her disdain for the ban on international surrogacy. The women voiced that the ban should be lifted so that international IPs could come for surrogacy services in India. Women reported that the practice is mutually beneficial: the IPs get children, the surrogates get payment, and the doctor gets business. Examples of comments related to this theme are below:
I think that the government should lift the ban and give a chance to these women, as well as the others, involved in this process…because it’s for a good cause. Everybody is benefited by this, the doctors who are involved, the couples who cannot have their own children, and women like us who cannot earn enough to feed our own children.
…The government should lift this ban. Everybody is mutually benefited from this practice. We come from a small village where there is no source of major income. By the means of this practice, we earn a large amount and can look after our financial needs.
Other participants expressed altruistic reasons for opposition to the ban. Radha, a 45-year-old woman who had been a surrogate twice (both Radha and her husband work at the fertility clinic), said, “This practice should have been continued. I feel bad for all the foreigners who cannot have kids because having children makes all parents happy.” However, the vast majority of women were economically motivated to participate in surrogacy and, thus, felt the ban restricted their economic potentials.
…We strongly feel that foreign couples should be allowed to come into the country for surrogacy. I would request the government to lift the ban so that women like us, who have no source of income in their lives, can be helped financially.
I would just say that the ban should be lifted because it will be a huge help for other women like me who are in need…and would be benefited by this practice.
Most women who participate as a commercial surrogate are in financial need and did not describe any women participating in surrogacy for anything other than economic reasons. Women’s opinions of the ban are largely influenced by this economic context. While all women said that the government should reverse the ban, only one woman, Diksha, provided alternative solutions: I feel that this is completely wrong on the government’s part and that surrogacy should not have been banned. I feel that there should be rules and regulations pertaining to it but it shouldn’t be banned altogether.…The government should reconsider their decision about the ban since there are women who are being affected by this, such as the widows, divorced, uneducated women…and they are at a loss because the standard of living is increasing every day and by the means of surrogacy they can at least assist themselves financially.…They can certainly enforce rules and restrictions to regulate this practice but they should lift the ban.
I just know that foreigners are not allowed now, I don’t really know why.
That I am not aware of, but I would only come again if this ban is lifted for foreigners
I am not aware of that; I am not educated. If the ban is lifted, it will be beneficial for everybody.
Two women briefly mentioned that the government may have put the ban in place because of negative misperceptions or bad practices but quickly dismissed those thoughts and could not elaborate further. Most women were not aware of any “wrongdoings” at other clinics throughout India; although, they did have some awareness of rumors surrounding surrogacy.
…People often say that women here become surrogates for less money and therefore are being exploited. There are various things that people say…I don’t think that is the truth, because there are so many women who resort to wrong or unethical work to survive and this work is definitely better than that.
I don’t know why the government chose to impose this ban. If this practice increased foreign investment in the country, what problem could the government possibly have? I don’t understand…I think it is because the society and community members talk ill about it that is what I feel.
Some women diverted their attention to the “good” that was done at the hospital in which they participated as a surrogate as justification for the practice. These women often mentioned how the doctor at this particular fertility clinic provides each woman with economic opportunities that she otherwise would be without and the gratefulness they feel for this.
The government might have some misconceptions.…They must think this practice is wrong, but it is actually beneficial for us. The doctor is doing a good job, because we come from a poor background with no house of our own and it takes our sorrows away. So what the doctor madam does is good.
…I feel it should not have been banned.…I have never heard any such incident wherein a surrogate mother has been harmed. Our doctor madam is so genuine that she helps women in need even if they do not wish to become surrogate mothers. She provides schoolbags, books, scholarships, and so on to children in need.
Many of the women spoke highly of the work being done by the doctor at the clinic in which they worked. So much so that they could not see how surrogacy could be harmful to women in other clinics. For example, Radha said, “I don’t think that [women are victimized by surrogacy]. That does not happen here.” Binky also shared these sentiments: I would just like to say that the ban should be lifted. There are so many other women like me, who work as servant maids and are exploited at their work places. This is a better practice wherein they can earn well and look after their families.…The person who imposed this ban, should have come here at this hospital for inspection and seen for himself how it is practiced here and how is it different from other places where malpractices occur.
Impact of the ban on surrogate mothers, international IPs, and fertility clinics
The women described three parties who are impacted the most by this ban: surrogates, IPs, and doctors.
Impact on surrogates
For surrogates, the impact of the ban was felt in terms of economic impact and impact on their livelihood. Economic impact pertained to the lack of financial benefits and compensation that surrogacy offers. Most women felt that the lack of opportunity to earn substantial amounts of money was the most harmful aspect of this ban
Poor people like us have been most affected. We have no major source of income. With the surrogate money, we can buy a house for ourselves; invest in our children’s future.
We would be the ones being most affected by it naturally. We are benefited it financially, we are able to invest in our houses, our children’s future, and other things by the doctor’s grace.
While international IPs may not come to India for surrogacy services, Indian couples can hire a commercial surrogate. Although, there is some discussion among lawmakers in India on banning commercial surrogacy for Indian couples. However, when this study was conducted, women could still become surrogates for Indian couples. There was a general perception among the women that foreign IPs paid substantially more money for services. The women agreed that the effort put into surrogacy work is not worth the money for Indian IPs, as they pay less compared to international IPs.
We are the ones who have been affected by the ban. We don’t get enough payment from the Indian couples. Foreign couples naturally pay more. They also pay us additionally, and they keep in touch and help us in need.
This ban should not have been imposed, because we are being affected by that as we receive minimum payment. The foreign couples would always give extra money when they felt happy. Both the parties were benefited equally.
Although the women said that international IPs pay more money for services, Binky said that payment for surrogacy is constant across surrogates. Therefore, some of the women’s narratives suggest that international IPs “tip” more for services more than Indian IPs. In addition, women are not aware if this tipping will actually occur and, if so, how much it may be. Sakhu said “The couple gives additional money when they are happy but that is uncertain and we come to know in the end.” Interestingly enough, women’s reports of their payments do not support this argument. On average, women who had been surrogates for international IPs only earned about 2,000 INR (equivalent to US$29.50) per surrogate pregnancy more than surrogate pregnancies carried for Indian IPs. This practice of international IPs “tipping” surrogate women may represent cultural differences between the IPs and surrogate women. Tipping for services is often the norm in high-income nations, such as the United States, and international IPs may be tipping surrogate women or providing gifts as a means to show their gratitude or a sense of duty to the woman. The same tipping culture may not be present among Indian IPs.
Less compensation for services was not the only complaint made against Indian IPs. Women reported that international IPs maintain relationships with their surrogates and oftentimes provide “gifts” to the surrogates and their children. Indian IPs, on the other hand, are perceived to only come for the surrogacy process and not to get to know the surrogate.
…The foreign couples pay more, which is naturally more beneficial for us because we are in need. The foreign couples also maintain relationships with the surrogate mothers after delivery which is not the case with the Indian couples, simply because the Indian couples are scared of the societal norms and what will people think.…So the foreign couples not only maintain their relations but also pay more, which is naturally a better option for us.
There’s no particular problem [with Indian couples] but definitely the money will be less and they don’t really want to maintain relations such as the couple from Ireland who specially came to India to meet me.
Again, counterevidence suggests that perhaps the women only perceive that international IPs “care” more than Indian IPs. Some surrogates reported that they did not maintain any type of relationship with the international IPs that hired them besides when they initially met. For example, when probed Barsha said:
It will be good if foreigners can come.…Women can earn more money; the couple also gets what they want.
So, are you in touch with the couple?
No, they never call me.
Likewise, Manju said, “They met me. They did not say much. They saw the report, they were happy with it, and then they went.” Furthermore, this enthusiasm for a relationship by IPs may fade over time. Rama said, “The [Americans] used to stay in touch earlier but not now.”
While some surrogates reported not knowing how much of a “tip” they will receive for their work, some surrogates reported that they do not know how much they will make beforehand, regardless of the tip. For instance, a couple of women were in the process of becoming surrogate mothers for a second or third time. When asked about the amount they will receive, they stated:
I don’t know about that. They will give me the payment when I will be leaving for home…. Ultimately, we receive what we are destined to receive.
They will be paying me in dollars.…I don’t know the exact amount, but they will decide and give me the money when I am ready to leave the hospital…. They know what financial needs I have, like I need a house, so they will pay me around 5–6 lakhs (equivalent to approximately US$7,700–9,200) approximately according to my need, decide with the authorities, and give me my payment.
From the importance that is placed on payment for services, one would think that the women would be not only involved with the negotiation of payment but would have their own financial criteria to be met before agreeing to the arrangement. However, not one surrogate, including those who had been a surrogate both internationals and Indian, reported the payment as being unsatisfactory. Rama, who was in the process of being a surrogate, said, “I haven’t thought much about [the payment], but I will be happy with the amount I receive.”
Impact on IPs and clinics
The impact of the ban for international IPs and clinics/fertility physicians was also described. Women reported that IPs are at a lost, because in India, the cost of surrogacy is less, IPs can be assured to receive a child, and the standards of care are high.
…The couples who come here for surrogacy have to pay way less for surrogacy here so it is beneficial for them as well plus in this particular clinic, the doctor assures them a 100% guarantee of getting a child so they are definitely affected.
This is a major loss for women. Everybody related to this practice has been affected by this ban.…Surrogate mothers here, I feel have healthier habits than the surrogates in the foreign countries as they abstain from alcohol consumption.
The hospital and its employees are definitely at a loss, but the foreign couples who cannot have children are also largely impacted by this because they are in a helpless situation. They are the ones most impacted because they have money and no children. What is the use of all the money, if you have no children?
The doctor who ran the fertility clinic was also described as being at a loss but not as much as the surrogates and the IPs. A large proportion of the fertility clinics revenue is derived from international IPs. Without foreigners seeking surrogacy services in India, clinics will begin to loose profits.
The foreign couples naturally pay more money and to run this hospital one definitely needs funds. She has worked hard for so many years over this, she will definitely face difficulty.
If we are being affected, the doctor also has been affected. The foreign couples made payments to the hospitals as well.
Long-term economic results of surrogacy
Throughout the interviews, women emphasized their positive experiences of the surrogacy process. In particular, women highlighted their time in surrogate hostels. The women also commented on the skills they were able to learn, such as stitching, as helpful. The women emphasized what they perceived to be as a high quality of care at the hostel and did not report any loneliness, depression, or social isolation.
They used to give us training for various vocational courses like stitching, henna art, and so on, for our own benefit…I did not feel [lonely] because there were other women and we used to all talk to each other.…They give us periods off if we are facing any problems otherwise families used to come to visit every Sunday. If we ever faced any problem, they used to send us home for a few days. They used to send cars to pick and drop us.
It was very good.…The doctor madam took care of us in every way. There was no pressure of any kind; we were free to do whatever we wanted to. The doctor here was almost like a mother to us. She assisted us in every problem we had. Our family members came to visit us every Sunday; we could go visit them whenever we wanted to.
Although the women were provided with vocational trainings, relatively few reported to be using that training to earn a stable income. In fact, most of the women were still unemployed. Other women had found odd jobs around the fertility clinic, such as babysitting or maid service, or currently searching for employment at the clinic.
I did not really do anything concrete but I babysit here at the hospital.…We used to take care of the children that were delivered by the surrogate mothers.…I am not doing anything currently, but 6–7 months ago, there was one child that we raised up to 4 and a half months until the couple came.…The doctor madam here always gives us work, whenever we come to her with a request.
Other women worked for the clinic, not in a full-time capacity, but rather for commission as surrogate and egg donor recruiters. These women receive payment from the fertility clinic when they bring in women to become a surrogate or donate their eggs. Indeed, most of the women we interviewed had heard about surrogacy through similar means.
I am a cook at two houses.…I also help the hospital in bringing women to donate their eggs.…There is a hospital in Vadodara city wherein I take women to donate their eggs, whichever is a convenient option for them. I approach women who are suffering financially and encourage them to do this good deed rather than doing something wrong. This is at least for a good cause. I encourage women to become surrogates, for which I get my commission as well. All these things have helped me become financially stable.
I also encourage and bring other women to do surrogacy because it is a good practice. I bring such cases to the hospital here…. Currently, I got two women. I get around 20,000 INR.
Although the women are no longer surrogates, they attempt to maintain their connection with the fertility clinic and the doctor as much as possible. The doctor of the clinic may be a primary motivation for this desire. Many women spoke very highly of her, often attributing the economic results of surrogacy to her, rather than their own work. Indeed, the surrogate women often refer to the head physician as “doctor madam” signaling respect and admiration for her. This affection may complicate women’s decision-making regarding surrogacy, health procedures, and payment.
The doctor madam has offered jobs to all the women who want to work here at the hospital.…The doctor madam really takes care of us.…The doctor has asked us to come here if we or our children face any problems.
I work here at the hospital as an attendant. I really appreciate what the doctor does here, and I worship her for everything she has done for me.
While the women may not have stable employment after surrogacy, the payment from the previous surrogacy work has provided many with homes and education for their children that, they report, has eased their difficult financial situations.
I was in dire need of money because of my poor condition. Being a surrogate mother, changed my situation and I don’t know what would have I done if the doctor was not there to support me.…I definitely couldn’t save the money because the standard of living has been increasing and this was a longtime back so the money has been spent of course but because of that money, we were able to stand on our feet and become financially stable.
Discussion
Surrogate women did not support the ban on international surrogacy, because they perceived financial benefits of the work. Most of the women were able to build permanent cement homes and/or save money for their children’s education with the help of the income they received through surrogacy. While women discussed the financial loss they would suffer due to the ban, the majority stated that they had no idea how they will sustain themselves any longer. The Indian government’s ban comes with no alternate plan for supporting livelihoods of women who rely on surrogacy. On one hand, the ban seems to be unfair for women who were clearly dependent upon surrogacy; however, upon further reflection, we are urged to think about the nature of surrogacy in India and whether it was truly economically sustaining to women who were surrogate mothers.
Overall, surrogacy services are much cheaper in India, and surrogates are not compensated according to any standard guidelines. The context of poverty is exploited by international IPs, because it keeps their costs low (Wilkinson, 2016) and ensures that surrogate women must place the child with the IPs (Shetty, 2012), as they do not have the means to care for the child. Similar to other studies conducted in the region (e.g., AUTHOR et al., 2014), most of the women in this study were from socially and economically disadvantaged backgrounds and were driven by desires for economic advancement. Yet, as reflected in the narrative of the women in our study, payment for surrogacy is often dependent on IPs, and gifts/favors are given to the women at IPs’ discretion. Regulation of surrogacy has been advocated as the most viable option to reduce discrepancies in payment (Wilkinson, 2016), because standardized payment for services can ensure that all women receive “equal pay for equal work.” However, the Indian government lacked clear protections for surrogate women.
In this study, international IPs seem to have great control over whether and/or when they will contact the surrogates; surrogate women have no control over these aspects. Pande (2015) describes the importance that surrogate mothers place on developing “kinship ties” with the surrogate fetus and intended mothers. In particular, forging emotional ties with the intended mother allows the surrogate to challenge “the medical construction of their relationships as merely contractual and easily disposable” (Pande, 2015, p. 58). Other studies have noted the importance of the relationship between the surrogate and IPs in the surrogacy experience (Baslington, 2002; Imrie & Jadva, 2014). Some surrogate women whom we interviewed placed an emphasis on being a surrogate to international IPs, because international IPs show more kindness, provide more money and gifts, and want to have and/or maintain a relationship with the surrogate. Although, no evidence suggested that actual, meaningful relationships are maintained between surrogates and international IPs, unlike the ones described between surrogates and Indian IPs in Pande (2015). Jadva, Blake, Casey, and Golombok (2012) and Imrie and Jadva (2014) found that in the United Kingdom contact between surrogate and intended mothers was harmonious, but the frequency and quality of the relationship decreased over time. We also found that the frequency and the quality of the surrogates’ relationships with IPs declined after surrogacy services.
Our study clearly indicates that women depend upon surrogacy for financial benefits and better livelihoods. However, their lack of agency to negotiate payment or maintain relationships with IPs was explicitly evident. Surrogate women may be perceived to “choose” whether to become a surrogate or not. Yet, their choices become restricted throughout the surrogacy process, including limited ability or inability to negotiate contracts and/or payment and to make their own health decisions with regard to methods of delivering the baby and types of medications that they receive. Their accommodation arrangements over the course of pregnancy and diet and nutrition regulations were all decided by the clinic. The surrogate mother’s ability to partake in shared decision-making was largely controlled by doctors who ran the fertility clinics. The doctor acted as a mediator between the surrogate and IPs and controlled the relationship between the two parties. The doctor choose the surrogate mother for the IPs and the whether or not the two parties had a relationship was decided by the doctor or the IP. Finally, women’s social networks were influential in women’s decisions. Husbands must “allow” women to become surrogates, and other relatives and peers of the woman recruit and influence women to seek out surrogacy. Considering all of these factors, we question the notion of free choice among women when they opt for surrogacy.
The ban on surrogacy seems to be the Indian government’s response to stopping exploitative practices involved in surrogacy. However, there are no alternate solutions for economic independence and livelihood options for women who either were surrogate mothers or wanted to be surrogate mothers in the future. The ban is currently imposed only on international couples, while Indian couples are still able to hire surrogate mothers in India. Therefore, commercial surrogacy continues and women get paid less than they did by international couples. At the same time, the law does not make any attempts to offer social services to surrogate mothers before, during, or after surrogacy, and the surrogate’s agency still remains in the hands of the doctors or the IPs.
Limitations
The views expressed in this study only represent the experiences of surrogates employed at one fertility clinic in India. The fact that the interviews were conducted inside the clinic premises and the women’s feelings of respect for the doctors’ authority and social class may have influenced women’s responses. Additionally, most of the women continued to have a relationship with the doctor of the clinic. Some of them worked within the clinic and some had desire to be selected as surrogate mothers again. It may be possible that women’s responses were influenced due to this. Lastly, this clinic has been open to several academic studies and investigative pieces portraying relatively good transparency in their procedures. Therefore, the perceptions of women who participated in our study may be substantially different from surrogates at other clinics, especially clinics with unfavorable track records or those that engage in illegal practices.
Implications for Social Work and Research
In western countries in which commercial surrogacy is legal, risks (both physical and psychological) of surrogacy have been largely mitigated by intensive counseling and support for surrogate mothers and IPs (Soderstrom-Antilla et al., 2016). Social workers should employ a woman-centered approach to surrogacy to implement real changes in how surrogates are hired, informed of the health procedures and risks, treated throughout the surrogacy process, and cope with postsurrogacy effects. Employment counseling and connecting surrogates with opportunities for paid employment outside of surrogacy and fertility clinics can help women create economic sustainability for themselves and their families. Social workers can be involved in reviewing contracts, informed consent procedures, and reviewing health information with surrogates so that they may truly be “fully informed” for decision-making.
We urge social workers to advocate for laws and programs that represent the desires of surrogate women. Surrogacy is a heavily contested policy topic; however, analyses often focus on bioethics, rather than what surrogates want. Social workers should advocate for comprehensive legislation to regulate, rather than restrict surrogacy in India and throughout Asia. An evidence-based policy for Indian surrogates may include an equitable and uniformly applied compensation structure; establishment of surrogates’ rights over their body; medical procedures; and relationships with IPs and surrogate children, education about the surrogacy process for the surrogate (including comprehensive informed consent procedures), and social service programs. Social workers should challenge unjust policies and promote the voices of surrogate women who are affected by these policy changes.
Scholars have noted the importance of keeping surrogacy under strict regulation to avoid creating a surrogacy “black market” (Caamano, 2016; Wilkinson, 2016). Indeed, other countries, such as Thailand and Nepal, have banned international surrogacy—evidence that reforms and regulations are needed for this industry (Caamano, 2016). Social workers can monitor and report illegal surrogacy situations in India among surrogates and in western contexts among IPs. Social workers assisting IPs in high-income countries should make IPs aware of the benefits and drawbacks of transnational surrogacy.
Given the inherent exploitation that is present in transnational surrogacy, research efforts should focus on understanding the decision-making abilities and empowerment of women in this context. Empirical evaluations of social, psychological, and health outcomes among surrogate women can provide foundations for evidence-based interventions. Additionally, interventional studies should be employed to increase the autonomy of women. For example, empowerment-focused interventions may be appropriate to help surrogate women negotiate pay and terms of their contracts, while increasing their confidence and decision-making abilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.