
Abstract
In this qualitative study, in-depth interviews were conducted with 15 surrogates from India. Two themes are discussed: (1) motivations for becoming surrogates and (2) role of family and community in surrogacy. The respondents were illiterate women aged 21–30 years and had been surrogate mothers an average of 2 times. Motivations for surrogacy were financial in nature. Surrogates reported stigma from extended family and community forcing them to leave their homes and relocate after surrogacy. This study recommends counseling and psychosocial support services to women and change in policy to execute a stringent law to protect the rights of surrogates.
Keywords
Introduction and Literature Review
The number of people traveling abroad for medical tourism is a disputed number that varies from a relatively small proportion of the world population to upward of 2 million people per year. In recent decades, high-income people from the Global South have traveled to the Global North for procedures unavailable in their own country. However, recently the trend has reversed with people from the Global North traveling to the Global South for medical services. Often the medical tourists specifically cite the lower cost as a prime reason (Alleman, 2011). Overall, there is very little empirical data on this industry.
Infertility treatment is one of the most common medical procedures identified by medical tourism companies (Alleman, 2011). This infertility treatment includes transnational surrogacy, and the act of traveling to the Global South for this service is a relatively new phenomenon. Surrogacy refers to a contractual agreement wherein a woman agrees to carry and deliver a child for another individual or couple who will raise the child. For traditional surrogacy, the surrogate is the child’s genetic mother, whereas for gestational surrogacy, the surrogate is implanted with another woman’s fertilized egg (Pande, 2009). Moreover, surrogacy can be for either altruistic or commercial purposes. Due to the possibility of financial coercion, many countries have begun regulating the practices of assisted reproductive technologies to try and ensure a system that is nonexploitative. For instance, Australia allows for only altruistic surrogacy, and the surrogate cannot use her own eggs. Additionally, compensation can only take the form of medical expenses, legal advice, counseling, travel costs, loss of earnings, and premiums for health, disability, or life insurance (Hammarberg, 2011). In some countries, debate has ensued for decades about how to legally regulate surrogacy. Japan’s Society of Obstetrics and Gynecology, for instance, forbids surrogacy altogether. However, because this entity lacks legal authority, some obstetricians/gynecologists (OB-GYNs) perform the procedure for couples in an almost black market fashion. The majority of Japanese individuals experiencing reproductive challenges travel to other countries where surrogacy is legal, such as England, Canada, or the United States (Semba, 2010).
India regularly ranks among the most popular destinations for medical tourism with other popular locations including Costa Rica and Thailand (Alleman, 2011). In the last two decades, India has seen an entire industry created around its ability to provide medical services at low cost to a global consumer base (Parks, 2010). India legalized commercial surrogacy in 2002 and is the first country to have a thriving national and transnational commercial surrogacy industry (Chang, 2009). Specifically, a large number of U.S. citizens have traveled to India for infertility treatment (e.g., reproductive cell donation, surrogacy, birth, and delivery). Typically, individuals/couples travel from Global North countries (such as the United States and United Kingdom) to India for several reasons. First, commercial surrogacy is substantially cheaper in India. While the cost of commercial surrogacy may exceed US$100,000 in other parts of the world, the cost in India is a third of that amount (Pande, 2011). Additionally, India is more desirable than other Global South countries, because many Indians speak English, advanced medical technologies are available, and there are currently no laws regulating surrogacy in clinics (Chang, 2009; Pande, 2011).
Social science research on surrogacy has been conducted in the areas of depression, social support, and attitudes toward pregnancy. In the Global North, women have been found to occasionally regret their decision to become a surrogate (Blyth, 1994; Ciccarelli, 1997). Blyth’s study found that a significant minority of women (approximately 25%) reported experiencing significant emotional distress such as depression, stress, and anxiety in giving up the child. Ciccarelli (1997) found that surrogate mothers perceived the surrogacy experience to have a positive effect on close family members, including their own children. Half of the women in Ciccarelli’s study found that many women felt the surrogacy experience actually brought them closer to family members. However, extended family and friends were found to have mixed reactions to surrogacy. Over 40% of respondents in Ciccarelli’s study reported having lost a relationship as a result of surrogacy. In contrast, Hohman and Hagan (2001) found that husbands and partners were found to be generally supportive of surrogacy. However, these issues have not been examined in the Global South.
Several studies have found that surrogates tend to form a relationship with the commissioning couple rather than the fetus (Baslington, 2002; Ciccarelli, 1997; Hohman & Hagan, 2001; Ragone, 1996). Hohman and Hagan (2001) found that surrogate satisfaction was determinant on relationship with the couple. Interestingly, surrogates have been found to feel less attached to the fetus during pregnancy than nonsurrogates (Fischer & Gillman, 1991; Ragone, 1996) and to experience different attitudes toward pregnancy than nonsurrogates (Baslington, 2002; Ciccarelli, 1997; Hohman & Hagan, 2001; Ragone, 1996). Again, studies have not been conducted to examine level of attachment and attitudes among surrogates in the Global South.
Inquiry into this growing industry has remained on the journalistic level up until now. Very little empirical evidence exists around the effects of surrogacy on the woman’s health, family, and other social contexts. Similarly, very little research has examined Indian women’s decision-making process to become surrogates (Palattiyil, 2010). This research study examined surrogate women in one fertility clinic in Anand, India. The specific objectives of this research were (1) to understand women’s motivations for surrogacy and (2) to explore the role of family and community in the woman’s decision to become a surrogate mother.
Methodology
In-depth interviews were used to explore participants’ motivation, attitudes, and experiences of transnational surrogacy. These in-depth interviews were conducted in one fertility clinic in Anand, India, during December 2012. A staff member from the clinic provided contacts of women who had previously been surrogates for international couples, and a verbal script was utilized to recruit participants. The first author of this article conducted the interviews in Gujarati and Hindi and an interpreter was present to assist with translation when needed. Interviews were recorded upon the participant’s consent and translated from Gujarati/Hindi to English. A total of 16 women were interviewed; however, one interview was terminated after the participant indicated that she was currently pregnant. Therefore, results from 15 interviews will be presented here. Each woman was interviewed for between 40 and 50 min.
Due to the high rate of illiteracy among participants and cultural norms, it was not appropriate nor a standard of practice to require participants to sign actual consent forms. Consent was established through verbal communications and subsequent participation in the study. This informed consent technique revealed that participants had a clear understanding of the study, an appreciation for the invasiveness of the questions, and were willing to proceed despite minimal risks involved with discussing sensitive information about themselves. Recruitment continued until saturation was reached. Each surrogate was compensated Indian rupees (Rs.) 500 as travel reimbursement for participating in the study. The above study procedures were approved by the Institutional Review Board (IRB) at The Ohio State University and the University of Utah. In India, the social sciences’ IRB is not formalized yet, and there are no official approvals given. However, as social scientists, we are concerned about the protection of human subjects, and we attend to this as an important element of conducting our research. Since this topic is relatively new and exploratory in nature, qualitative methodology seemed appropriate to conduct this research. This methodology brought out in-depth understanding of the issue and highlighted the voices of surrogate mothers.
An interview guide (in English) was developed for this research study and subsequently as translated into Hindi and Gujarati. The interview guide contained several questions on demographics (i.e., age, marital status, number of children, education, and place of origin), entry into surrogacy, motivations for being a surrogate, as well as questions about experiences as a surrogate. The interviews were semistructured and the participants could choose to speak on any area of particular relevance to them.
For the purpose of analysis, the researchers translated and transcribed each interview. The analysis consisted of reading the qualitative data line by line, identifying themes, coding categories, and developing matrices to uncover relationships between themes and categories (Straus & Corbin, 1990; 1997). All participants were assigned pseudonyms for research purposes. In the results, participants’ comments are introduced or followed by one of these assigned pseudonyms.
Results
Although several topics and themes emerged from these interviews, the researchers limited the results to two critical themes: (1) motivations of surrogate mothers; and (2) the role of family and community in surrogacy. However, before elaborating on the themes, the researchers would like to provide a brief background of the participants of this study.
Identifying the Surrogate Mothers
The following discussion describes the characteristics of the surrogate mothers who participated in the study. All 15 women who participated in the study were married and had given birth to at least one biological child prior to becoming surrogate mothers. Participants were referred to the surrogate clinic by agents hired by the doctor or by husbands and close relatives. A majority of the participants reported to be from very low socioeconomic background and had little to no formal education. Also, participants reported that their husbands were unable to earn sufficient income for the family due to employment status, and surrogacy was seen as a way to alleviate poverty. The commissioning parents were from the United States, Japan, Canada, Australia, England, Japan, India, and Madagascar. Please refer to Table 1 to review the demographic details of the participants of this study.
Demographics of Sample.
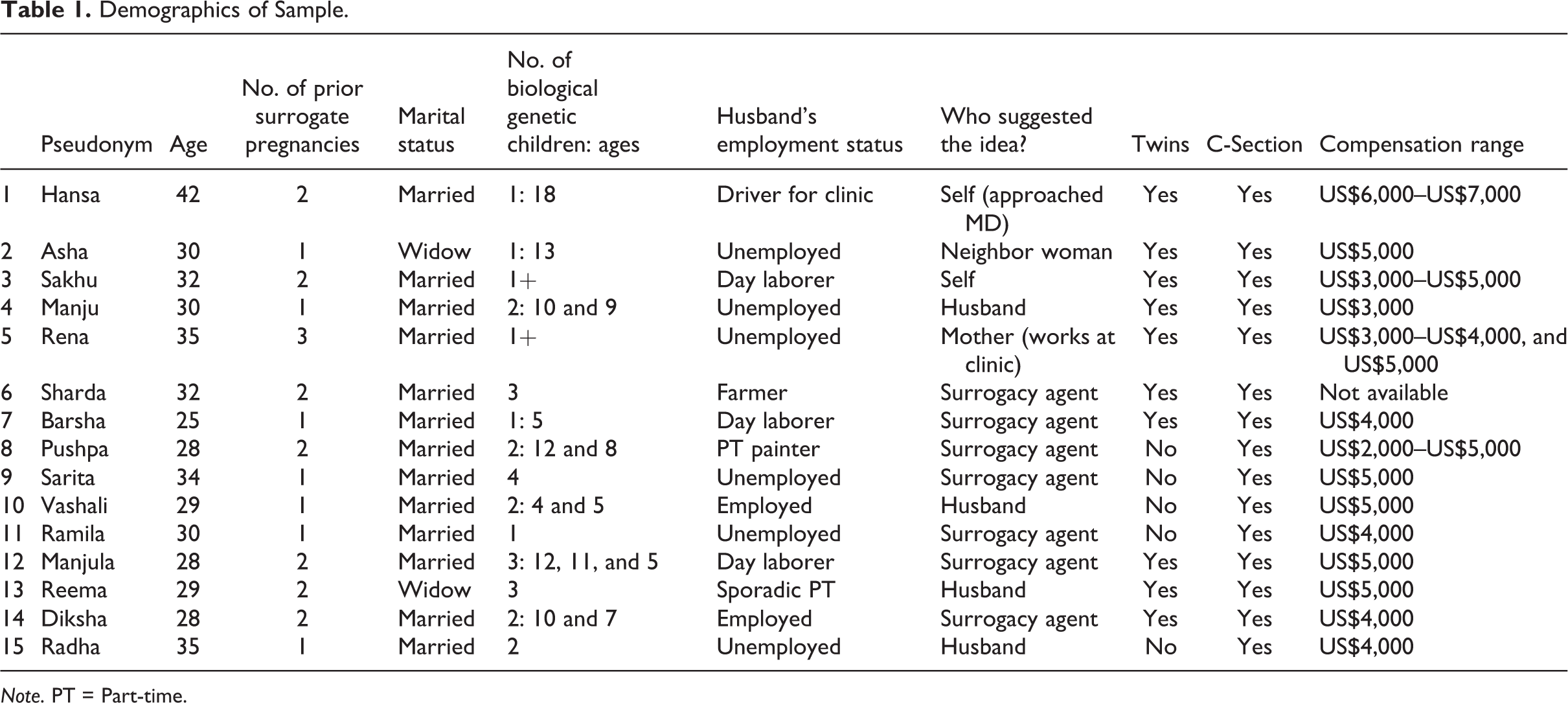
Note. PT = Part-time.
Motivations of Surrogate Mothers
Each of the participants of this study was asked about her motivation and reasons for becoming a surrogate mother. All the participants stated that their primary motivation was the financial compensation that was offered to them. Each participant stated that she received about US$3,000–5,000 for successfully delivering a baby through surrogacy. The compensation for carrying twins ranged between US$4,000 and US$6,000. However, the received compensation was different for each pregnancy and depended upon the commissioning parents’ economic background as well as the contracts that were signed between the parents and the clinic. The difference in compensation offered to each surrogate in the study can be seen in Table 1. In describing the motivation for surrogacy, one of the participants, Rena, a 3-time surrogate stated: I could not get the house even though I wanted to after the first time because there was always some family things. My father in law had cancer. Husband had loans. So all money went there. So it became a natural decision even though second time I had C-section and didn’t feel up to doing it a third time.
This quote clearly states that there was a pressing financial need that resulted in Rena’s decision to become a surrogate mother 3 times.
Another participant, Reema stated: I am a widow and I live with my mother-in-law and son. I was not able to make ends meet, and lived in extreme poverty—house was leaking all the time. There was a woman from the clinic who came to my house and talked to me about surrogacy. I really needed money and she made it sound so easy. She had done it three times. So only for the money I decided to listen to the woman and come to the clinic.
Sakhu said: My husband and I had lots of financial problems. We had to vacate our rental home. My husband offered to sell kidney and I told him that instead of doing that I can become a surrogate. We had no other choice.
The above-mentioned quotes indicate that participants became surrogates to support their families. Of the 15 participants, 10 mentioned that their husbands were unemployed and they had no other choice but to become surrogates. Five participants stated that their husband’s employment was inadequate and did not provide enough for their families, and they had to become surrogates because there was “no other choice.”
Sarita stated: With all my children, and a husband with no work—I had to do it all myself and it is very difficult. There was no other choice in the matter.
Radha mentioned: My husband’s job is not very good. There are lots of problems. Months will pass with no money from him. So he was very interested in a way out of our situation. He even tells me to become an egg donor from time to time.
The surrogate mothers in this research reported a low socioeconomic background and had a compelling need to make money for supporting themselves and their families. The participants’ motivations for becoming surrogate mothers were clearly financial in nature. They did not state primary motivation to help an infertile couple or to be of service to the community or society, which are often times reasons cited by surrogate mothers in the literature (Blyth, 1994; Ciccarelli, 1997).
Role of family and community in surrogacy
The role of the family in relation to the gestational surrogate was complex. The role of the husband in making the decision to become a surrogate was mentioned by 10 of the 15 participants. Three women mentioned that their husband was supportive of the idea, four explained that their husband insisted that they consider it, and three said that their husband needed to be convinced before the decision to become a surrogate could be made.
My husband is the one that insisted that I should become a surrogate. He read the article and then brought me to the clinic. I didn’t want to really do it but when I thought about the money I had no other choice.
My husband is the one that motivated me to come here. He came and talked to the doctor and then made sure I became a surrogate. Months will pass with no money from him. So he was very interested in a way out of our situation. He even tells me to become an egg donor from time to time.
I came here with my husband and the clinic convinced him that nothing happens between the man and me, it is only medicines that make the baby.
I … told my husband and my own family and they were supportive.
Apart from the husband’s role in surrogacy, the role of other family members was also considered to be important. Often times parents of the surrogate, siblings and even in-laws participated in the surrogacy process. They either helped and supported the surrogate, or acted indifferently and even criticized her for becoming a surrogate.
My mother in law helped out at home. There was no other support and she did the cooking and looked after everything in my absence.
A contrasting view was presented by Sarita, she stated: I had no support from my in-laws. They criticized us and we left the village and started living separately.
Commonly, after pregnancy was confirmed, participants lived in a surrogacy hostel for the duration of the pregnancy. Surrogates chose whether or not to reside in the hostel. More often than not, surrogates chose to live in the hostel to avoid stigma at home. Because the agency only allowed women who had previously successfully given birth to become surrogates, all the participants had biological children who were forced to remain at home while the surrogates lived in the surrogacy hostel. Typically, the surrogate’s family home was located far from the surrogacy hostel, which resulted in limited contact with family members. Other family members, such as a mother-in-law or husband, stepped in during this time to take on the participant’s responsibilities such as child rearing and cooking meals.
I am worried about this second time. Staying in the surrogate home will be hard and I don’t know who will take care of my child. But the 9 months will go fast and then we will have the money we need.
I did not like staying in the surrogate home. I constantly wanted to go back home to my children. But the poverty of our house would have been bad for my pregnancy. It was safer to stay in the surrogate house.
For many of the participants, some or most of her family members did not know she was a surrogate. If the family members did know, they tended to protect her secret to shield others from the truth. In other cases, the women mentioned reluctance to tell their family members about the surrogacy. Five of the participants mentioned that some members of their family or community did not know that they had become a surrogate.
My extended family still does not know about what I did. They are very conservative and would not accept me if they were to come to know.
I have not told my parents about it. Or my extended family because if they come to know such things they would kill me. They live in the village so they do not understand the process.
It’s very difficult to stay without family for so long. And also keeping it secret from them.
While family members’ reactions to the surrogacy varied from negative to relatively supportive, community members’ reactions were always negative. Surrogate mothers were typically stigmatized if community members became aware of the surrogacy. This resulted in ostracism and one participant was even forced to move away from her village.
There are so many people that talk badly about what we do. There is much stigma, and people say things like she is after money … and things.
I am Christian. When the church folks came to know of the surrogacy, they stopped talking to me, and stopped admitting me in the church.
I lived in one village and once people found out about the surrogacy we had to move. And so now we are in a different village. When I came to the surrogate house, I told people that I was taking a job for one year away from home. But then people started asking a lot of questions and then they started talking about me badly so I had to move again.
Surrogate mothers employed various strategies to avoid stigma and ostracism. These included living in the surrogacy hostel while engaging in false claims of alternative employment or even lying about the result of the pregnancy.
I had to stay in surrogacy home because people in village would ask about how I got pregnant, especially with no husband.
Because there was no surrogacy home, I had to stay in own house. I told everyone that it was our child. When the child was born we told them the baby did not survive.
While the major incentive cited for the creation of the surrogate hostel was the maintenance of the surrogate’s health, the information mentioned above points to an additional reason: To maintain seclusion of the pregnant surrogate, thus shielding her from the eyes of a disapproving community. By providing a means of isolation, the surrogacy clinic is both meeting their own need for supervision of the pregnancy and meeting the need of the women to keep the surrogacy private. A third stakeholder in this arrangement is the community itself. By quarantining the practice of gestational surrogacy out of public view, it is a way to maintain the social norms of traditional reproduction, even as surrogacy becomes more and more common.
Discussion
In this section, we will first discuss the motivating factors that the surrogate mothers described in their interviews. The main motivator was financial, with a secondary factor being altruism. Additional headings of “deciding to become a surrogate and “recruitment” are also included in order to better describe and explore the decision-making process of surrogate mothers. Second, we will discuss the role that the family and the community played in the decision-making and surrogacy processes. The husband’s role, the support of children and family during the surrogate mother’s absence, and the community’s role in surrogacy will each be explored.
Financial Motivators
Earlier in the article, several studies were mentioned that showed how richer countries had outlawed the practice of paying women to be surrogates due to the danger that the large financial transaction would serve as a coercive factor in the decision to become a surrogate. When considering that gestational surrogacy has been labeled as potentially financially exploitative to birth mothers in the Global North, should surrogacy then be alternately interpreted as liberating for Indian women because they have no other sources of income?
When this idea of financial transactions in surrogacy was explored in this study, it became apparent that severe financial hardship was the main reason that the participants chose to become gestational surrogates at the clinic. There was an overarching theme of choosing surrogacy as an attractive last resort for poorly educated women with few choices to earn enough money to support their family. Several women used the Hindi word, “majburi,” in their explanation of why they chose to become surrogates. This word translates into English as being “compelled” to do something. Additional aspects of the translation further elaborate on the definition, including the terms obligated, constrained, and helpless. By using this concept, the women communicated how they felt reluctant to refuse the opportunity to become a surrogate due to the overwhelming life burdens they were experiencing. Thus, women chose to participate in surrogacy as a result of poverty regardless of the stigma associated with the practice. This phenomenon has been supported by Pande (2009) and Rotabi and Bromfield (2012).
A Noble Cause
Although financial gain was the main motivation for pursuing gestational surrogacy among the participants, many women also indicated that they were doing something noble. They went further in making the distinction between sex work and their work as surrogates. Sex work on one hand was perceived as a dishonorable means of acquiring financial resources for a family in poverty. Surrogacy on the other hand was seen as a way to get much more money and was not seen by the surrogates themselves as being degrading in the same way as sex work. A quote from Ramila sums up the sentiment of many of the surrogates well: Earlier women didn’t know this was an option so they were prostitutes. This is such a noble cause and we get money also. Even after that people still don’t recognize this as a good thing. They still think it’s a bad thing. My husband talked to me about all these things and explains why this is better than the other things women do for fast money.
Although the idea of serving as a surrogate for a couple who were otherwise unable to have children was mentioned as a noble act by the participants, it was not mentioned as the primary motivator. Financial gain was the predominant initial response when women discussed their motivation for pursuing surrogacy. The inclusion of surrogacy as a noble act can be viewed as a moral justification for a decision already made for financial reasons. There is cultural stigma against gestational surrogacy (Pande, 2009, 2010; Twine, 2011), thus conceiving of surrogacy in this way may legitimize the woman’s role in the process.
Deciding to Become a Surrogate
While the main motivation for becoming a surrogate was financial, surrogacy was not a widely known or understood procedure in this community at the time of these interviews. Because of this, multiple factors were at play in the woman’s ultimate decision to become a surrogate. The woman must first have been made aware of the option of surrogacy. She must then understand the procedure and its implications. She must seek approval, active or tacit, from her husband and close members of her family. Additionally, because these gestational surrogates spent the duration of their pregnancy in an alternate location, she must make arrangements for the care of her family and household in her absence. In order for the woman to make the final decision to be a surrogate, all of these areas were addressed.
Recruitment
The majority of women in the study did not seek out surrogacy. Rather, they were approached by someone else with the idea. Of the 15 participants, 7 had been approached by an agent of the surrogacy clinic. Four had been told about surrogacy by their spouse. Only two said that they had been the one to initiate the surrogacy process. This speaks to the practice of recruitment for gestational surrogates in this community. Because prior surrogates were given a “finder’s fee” of up to Rs. 5,000 (US$100) for each woman they brought in to be a surrogate, there was motivation for past surrogates to promote the practice positively to other women in the community. This initial external pressure to consider surrogacy may legitimize surrogacy as a noble act and reduce the stigma associated with the practice—the women were not on the whole personally drawn to surrogacy and thus may rationalize their decision to participate by relying on the altruistic aspects of providing a baby to an otherwise infertile couple. That is to say, although the primary motivation for surrogacy was financial, further conceptualizing surrogacy as a noble act may allow the woman to more easily legitimize her decision to herself and her family.
Husbands’ Role
It is worth noting that none of the married women interviewed said that they made the decision to be a surrogate without their husband’s approval. Husband’s approval was considered mandatory not only by the women but also by the surrogacy clinic. It was a requirement that the husband signs the paperwork providing permission for his wife to become a surrogate mother. This indicates that surrogacy was not the decision of the woman alone and her husband was surely involved in the decision-making process. Thus, the woman’s body belongs not to herself only but to her husband as well. However, the results of this study indicate that the husband’s role varied from being indifferent to being insistent for the wife to become a surrogate. Some of the husbands needed convincing while some were supportive by offering domestic help while their wife was away in surrogate homes.
Support of Children and Family
One of the main reasons the husband was involved in the decision-making process is because all of the surrogates had at least one prior successful pregnancy and thus at least one biological child that they were currently caring for. Because most of the women interviewed were in the surrogacy home for the duration of their pregnancies, other arrangements had to be made for the care of their home and their children. The participants stated that they missed their children while they were away and that other family members took care of the young children in their absence. Here, “family members” refer both to nuclear and to extended family members.
Community’s Role in Surrogacy
One theme that emerged from the interviews was that the community at large was opposed to gestational surrogacy. Many women reported apprehension to inform extended family members for fear of disapproval or retribution. Participants also reported having to relocate after community members (e.g., neighbors, fellow villagers, and church members) found out about the surrogacy. This lack of support from community is in one aspect unsurprising, as many Indians view surrogacy as comparable to sex work (Pande, 2009). Women’s roles as wife and mother are important in this community, and fidelity in a monogamous marriage is expected. The in vitro fertilization (IVF) process involved in gestational surrogacy was not understood by all members of the community, and even when it was, the idea of a married mother carrying another couple’s baby was not supported.
Even so, systems of support were necessary for the gestational surrogacy process to occur at all. As explained previously, clinic staff, surrogacy agents, husbands, and family members were all involved in the process. Furthermore, all of these stakeholders benefited financially from the woman’s gestational surrogacy. The genetic parents paid the clinic. The surrogacy brokers received a finder’s fee. The family members, such as children, husbands, or parents, went to school or at times bought a permanent home that was slightly better than the rental homes or temporary shanties that housed them prior to surrogacy. So, even though the larger community heavily stigmatizes surrogacy, various members of the community directly benefit financially from the practice of gestational surrogacy.
Conclusion
This work illustrates a number of implications for policy, practice, and future research. In terms of policy, this work implores the regulating bodies to begin to develop policy around a number of key concerns. The first is the importance of establishing a well-reasoned and uniformly applied compensation structure for the women that choose to serve as gestational surrogates. The system currently in place is administered on a case-by-case basis and increases the likelihood that some women may experience exploitation. Additionally, no governmental policy exists regarding the education of surrogate mothers. For example, Sarita stated, “After delivery there are some problems everyone has, but no one talks about them. But the doctor gives lots of painkillers.” Therefore, a policy is needed around the level of disclosure and education about the process itself, so that a woman can make a well-informed decision about engaging her body in this type of work.
It is important to note, that every participant’s surrogate pregnancy resulted in a Cesarean section, and many surrogates had undergone multiple Cesarean section procedures. Increased Cesarean sections are associated with increased risks, including morbidity (Clark & Silver, 2011; Silver, 2012). Although conditions associated with Cesarean sections are rare, many are serious and include pelvic pain, bowel injury, cystostomy, urethral injury, placenta accreta and previa, reduced fetal growth, preterm birth and possibly stillbirth, decreased fertility, increased risk of ectopic pregnancy and spontaneous abortion (Clark & Silver, 2011; Silver, 2012; Solheim et al., 2011). Thus, women need to be informed of these risks associated with Cesarean section delivery. Moreover, there should be a policy structured around the number of times that women may engage in this work and other reproductive services. Women we interviewed demonstrated a wide range of number of surrogate pregnancies.
In terms of practice, level of disclosure continues to be an important element. The women whom we interviewed often demonstrated a dire need for income caused by other systems of services either not being there at all or not being effective. Clear lines of obligation should be established from the professional organizations that oversee social workers employed in this line of work to ensure that the women and their families are advocated for in every possible way.
There should also be an effort by practicing social workers in areas of high utilization for these services around awareness raising. A key function of the social work profession is to create awareness around issues, and the issue of gestational surrogacy, as our participants discussed, is a process not clearly understood and rife with stigma. Without identifying women who have engaged in the work, for fears of their safety when discovered, social workers could launch general awareness campaigns that could serve to increase women’s safety when they return to their villages, should their work as a gestational surrogate be discovered.
Future research is needed to continue exploring the experiences of surrogates, as well as the role of recruiting agents and husbands. Future research is needed that examines the mental well-being of surrogates in India. Constructs such as depression, self-esteem, attachment to the fetus, and attitudes toward pregnancy will provide a clearer understanding of the impact of surrogacy postdelivery. Longitudinal data are needed to understand the impact of this process on surrogates mentally, emotionally, physically, and financially in the long term.
Finally, future research should explore the roles that recruiting agents from the surrogacy clinic play in this process. Other research the team has conducted about the recruitment process suggest surrogacy may be portrayed only in a positive light to successfully recruit women, rather than disclosing the actual experience of the process. Our work illuminated that many other systems support the women in the endeavor to be gestational surrogates, so a further understanding of their level of satisfaction with the process is warranted.
Ross-Sheriff (2012) asked, “Should our professional work include advocacy and research on the ethics of commercialization of the human body, including women’s bodies and surrogacy?” (p. 127) We answer with a resounding, “yes.” Future research must continue to examine the ethics associated with the commodification of women’s bodies, especially those bodies in the Global South.
Finally we probe, is it ethical that marginalized and illiterate women are paid to bear children for relatively wealthy women within a larger globalized medical for-profit undertaking? Is it fair that their health is not insured on a long-term basis? Is it equitable that the amount of money they make is meager compared to what a surrogate mother would receive in the Global North? Are women’s rights being violated in practicing international gestational surrogacy? As social workers concerned about women’s issues, we have these challenges before us.
Understanding globalization and its impact on women’s bodies is critical and we need to advocate for the protection of women rights. We encourage dialogue among social workers to examine gestational surrogacy from the perspective of human rights and women’s rights. To do this, it is important to engage the Universal Declaration of Human Rights in this dialogue. In particular, Article 25 of the Universal Declaration of Human Rights (1948) states, “Everyone has the right to a standard of living adequate for the health and well-being of himself/herself and of his/her family, including food, clothing, housing and medical care and necessary social services…”. Additionally, Article 23 states “Everyone has the right to work, to free choice of employment, to just and favourable conditions of work…” (Universal Declaration of Human Rights, 1948). We recommend that the international social work organizations and networks openly discuss the human rights violations behind gestational surrogacy and strive toward spreading awareness about the issue. Finally, we feel that the global social work community needs to develop a protocol on ethical underpinnings of gestational surrogacy and advocate strongly for protecting the rights of women.
Limitations of the Study
Our work was impacted by limitations. The most important one to consider was the sampling method our team used to engage gestational surrogates. Our team conducted the work in the facility where women had been gestational surrogates, and in many cases the women still had relationships with the facility. In some cases, these relationships were income generating through performance of general housekeeping work, through other reproductive service engagement (i.e., reproductive egg donation); and in many other cases, they were maintaining close relations for potential future service selection. Therefore, it is possible that the participants did not speak freely, given their ongoing, financial relationship with the surrogacy clinic. Hence, surrogates who have not maintained a relationship with the clinic may describe the process in a more negative light. Thus, this study cannot be generalized to all surrogates seen at this facility.
Another limitation of our study was its cross-sectional nature. Our team interviewed women at one point in time about an experience that is likely to have a lasting and evolving contextual meaning to the woman over her lifetime. Therefore, this study cannot be generalized to the larger population of surrogate mothers. Future work should explore this role and its interpretation over time to understand the long-term impact on the women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.