
Abstract
The domestic violence (DV) field has long been known for its commitment to the integration of micro- and macro-level practice. This study explores the views of social workers providing clinical services within DV agencies in order to shed light on the ways in which they intellectually resolve the tensions inherent in carrying out the dual mission. Following the review of historical debates on professionalization of the field, the analysis focuses on clinical social workers’ efforts to construct integrated practices while responding to the historical context of feminism, which has shaped their agencies and the movement in the field.
Professions are distinguished, in part, by the roles and purposes they fill within society. The existence of a profession requires a unique purpose, a clear identity that makes it distinct from other occupations. For the social work profession, that unique purpose is a dual mission to simultaneously enhance social functioning and improve social conditions. This purpose is enumerated in a variety of the profession’s unifying texts, such as the NASW’s Code of Ethics (2008), the International Federation of Social Workers’ (IFSW) definition of social work (IFSW, 2012), and the Council on Social Work Education’s Educational Policy and Accreditation Standards (2012).
While carrying out the dual mission is central to our professional identity, doing so can be an intellectual, political, and practical challenge. Historically, the profession has struggled with maintaining a clear identity, and debates have taken place for over a century about which aspect of the profession’s dual mission is “authentic” social work (Haynes, 1998). Clinical social work, in particular, has been subjected to critique and has been accused of being overly focused on individual functioning, diagnoses, and a psychological view of human nature, while ignoring the social context of clients’ concerns (Specht & Courtney, 1994). Others have countered that clinical social work is firmly within the bounds of the profession’s mission and that the provision of psychotherapy can be seen as consistent with values of social justice (Swenson, 1998; Wakefield, 1988).
This article explores the views of social workers providing clinical services within domestic violence (DV) agencies, a field long known for its commitment to integrating micro and macro practice. The field is ideal for exploring practitioners’ views of the profession’s dual mission, as DV agencies have been rooted in traditions of both care provision and social movement work since their inception. Further, this field has traditionally been associated with feminist thought, which has maintained a strong critique of the dangers of treating abuse victims through psychotherapy. DV workers are in a unique position to inform a complex question, that is, how do clinical social workers provide psychotherapeutic services that incorporate attention to macro social work practice? This article explores the views of workers in DV organizations in order to shed light on ways in which they resolve the tensions inherent in carrying out social work’s dual mission. We begin with a literature review that explores the profession’s conceptualization of DV across time.
Social Work and DV: Historical Overview
The social work profession first encountered DV through child protection efforts that started in the late 19th century (Gordon, 1988). While addressing parental neglect and abuse, social caseworkers learned that often mothers were also victims of violence by their husbands. But child protection agencies avoided intervening in marriages. Abusers were viewed as ignorant or mentally deficient and physical abuse seen as “domestic disputes” caused by women’s improper housekeeping or unattractive appearance (Pleck, 1987, p. 125). These gender biases were also reflected in social work theory in the era of professionalization, which shaped the activities of family casework. For instance, Mary Richmond appeared to have a fixed idea of gender roles, claiming in her seminal book Social Diagnosis that the “the household speaks for the wife, answering unasked questions about her as it does not about the husband” (Richmond, 1917, p. 147).
In the absence of an organized women’s movement after the 1920s, this victim-blaming discourse was bolstered by the rise in psychiatric analyses of gender and DV. Although Freud never mentioned DV, Helen Deutsch, his former patient and disciple, applied his theory to the issue. Deutsch (1944) developed a comprehensive theory of female masochism to explain DV, arguing that women tended to remain with their assailant because they secretly enjoy the pain inflicted on them. With the prevalence of psychiatric social work, her theory had a significant impact on family social work practice in the 1940s and 1950s. Ignoring men’s behavior and gender inequality, caseworkers in family service agencies focused upon women’s sexuality and personalities. This perspective continued to influence social work practice until the 1970s.
When the second-wave women’s movement reframed the issue of “battered wives” as both a social and a political problem, survivors and feminists came together with scathing criticisms of social work’s distorted perspectives on women’s sexuality and “victim blaming” (Fleming, 1979). Here, the term “feminists” is broadly defined as the participants in the women’s movement in 1960s and 1970s, a collective effort to challenge dominant gender ideology and to bring about social change for gender equality (Kemp & Brandwein, 2010). The Battered Women’s Movement (BWM) can be seen as an effort for consumers to advocate for themselves in alliance with feminists, whose approach to DV was on challenging a violence prone patriarchy that condones DV rather than on blaming and changing women (Schechter, 1982). The BWM created its own practices and programs based on feminist principles, including legal services and shelters. Participants in the BWM also espoused progressive organizational principles, such as nonhierarchical and nonbureaucratic structures. They organized team leadership instead of a single director system and tried to eliminate a hierarchy between professionals and nonprofessionals as well as between activists and women victims who sought help (Galper & Washburne, 1977).
Over time, though, many voluntary organizations of the movement evolved to function as social service agencies for battered women. Issues of cooptation and professionalization were raised, causing heated discussions among participants in the movement (Ahrens, 1980; Morgan, 1981). This trend toward professionalization raised concerns among feminist social workers and lay advocates that incorporating social work practitioners into organizations would again shift the focus of the movement away from social change to focus on individuals (Markowitz & Tice, 2002). For instance, Ferraro (1983) concluded that professionalization ushered a therapeutic ideology into the shelter, ultimately diminishing the feminist practice principle of equal relationships between workers and women (Ferraro, 1983). A recent ethnographic study conducted by Dewey and St. Germain (2014) also showed that federal funds and professional staffing transformed the nature of relationships between staff and women into one between “experts” and “clients.” This unequal relationship, along with other requirements from funders, including increased needs for paperwork and documentation, led to a phenomenon called “social service fatigue” among survivors (Dewey & St. Germain, 2014). Due to this shift in nature of DV organizations from peer-to-peer advocacy to professional services, some participants in the BWM concluded that the BWM lost its identity as a social change movement. In their recent qualitative research with workers in 16 DV organizations in Midwestern states, Lehrner and Allen (2009) confirmed that professionalization and therapeutically oriented social service agendas were replacing the social change orientation of the organizations (Lehrner & Allen, 2009). Quoting the lament of one state advocate, “the Battered Women’s Movement went downhill when the MSW took over” (Danis & Lockhart, 2003, p. 215).
Because of the prevalence and persistence of this view of social workers as “apolitical” psychotherapists, there has been an ambivalence and caution toward a clinical approach among social workers in the field. Chong (2000) observed a deeply embedded conflict between social activism and clinical orientation from her in-depth interviews with 31 Master’s Degree in Social Work (MSW)-level social workers who have worked with DV survivors at community service centers and local shelters in New York City. Some participants expressed opposition to psychotherapy while others complained of misconceptions about clinical work and a tendency in the field to view psychotherapy as victim blaming, arguing for its merits as a tool to help survivors with trauma. Similarly, Conroy (1994) emphasized the critical role of clinical social work in the BWM, arguing that politics and clinical intervention are not necessarily incompatible, stating “to teach that the lives of battered women exist on the same continuum as those of other women, a continuum from mentally healthy to mentally ill, does not eradicate the political message that no women deserves to be hit … It merely says they battered women … should be assessed and served appropriately” (Conroy, 1994, ¶ 8).
This historical overview suggests that social work practice in this field of practice is one where the tension between individual services and social change has been particularly salient. However, there has been a dearth of research that pays particular attention to how clinical social workers negotiate these micro and macro practice tensions. This study explores how DV clinical social workers integrate micro- and macro-level practice. More specifically, the study examines how clinical social workers have evaluated and adopted therapeutic models and theories in a practice setting where clinical interventions have been criticized for depoliticizing violence against women.
Research Methods
A semistructured interview guide was developed to help explore the study’s key research questions. The guide included a number of topical areas related to the integration of macro- and micro-level practice. This article presents respondents’ perceptions regarding three of our topical areas, namely, (1) use of theoretical approaches and diagnostic tools in practice, (2) the concept of power and its implications for practice, and (3) efforts (intellectual or pragmatic) used to integrate micro and macro practice concerns. During the interviews, we did not attempt to limit the ways in which respondents discussed macro practice, instead letting them present their views as openly as possible in order to facilitate an authentic sharing of their practice perspectives. Our goal was to explore whether key ideas related to macro practice including empowerment, social change, feminist practice, and similar related topics would emerge, and to learn more about how practitioners integrated these ideas with their clinical duties.
Following approval by a University Institutional Review Board, data were collected from November 2010 to September 2011 through qualitative interviews with clinical social workers who formerly or currently have provided therapeutic services to DV survivors within DV agencies. The sample was drawn from DV agencies located in two Midwestern states and one Northeastern state. In order to be eligible for involvement in the study, participants had to have been formerly or currently employed in clinical positions by DV organizations, either as therapists at shelters or community outreach programs. All participants were required to have at least a MSW as a minimum professional degree. Since the licensed clinical social work credential is not always required for entry-level social work therapist positions in DV organizations, the participants did not have to hold a clinical license. Network sampling was used as the sampling method.
In-depth interviews were conducted with 13 participants representing five DV organizations. This relatively small sample size was due to the limited number of DV organizations that had the financial resources to hire clinical social workers as “in-house” therapists. The average age of the participants was 40 years old, and 2 of 13 participants were non-white. All respondents had an MSW and eight of them held a clinical license. On average, respondents had worked in the DV field for 11 years and previously or currently worked as therapists at the DV agencies that had shelters. Three participants were working at the shelter as in-house therapists, while the rest of them were providing therapy services to survivors in the communities. Table 1 shows the participants’ demographic characteristics, work positions, and the number of years they had worked in the DV field. Pseudonyms were used to ensure the confidentiality of the information provided by each participant.
Participants’ Demographic Characteristics and Work Experiences.
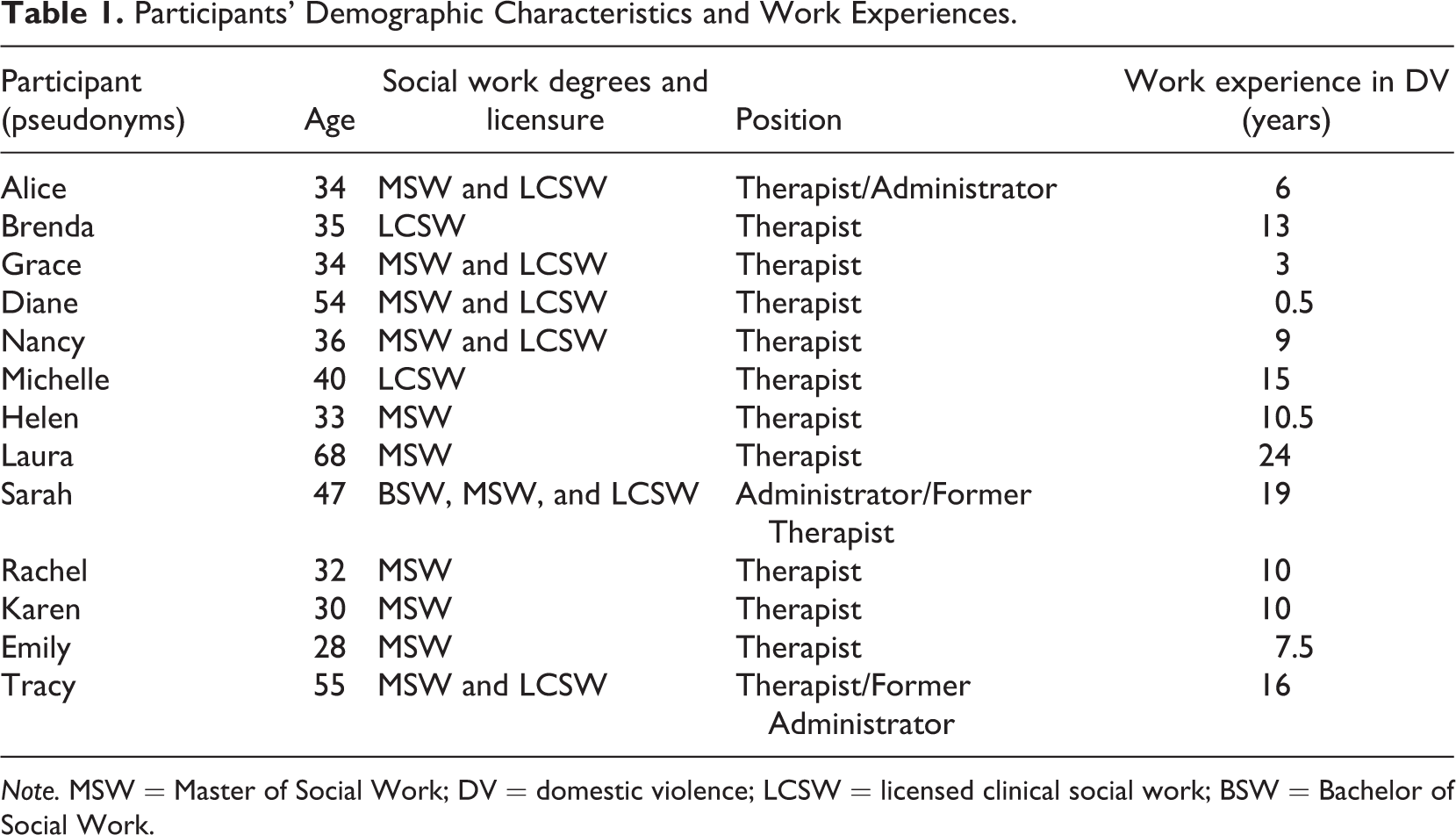
Note. MSW = Master of Social Work; DV = domestic violence; LCSW = licensed clinical social work; BSW = Bachelor of Social Work.
All interviews were recorded and transcribed verbatim. Analysis of all data was based on the principles and techniques of grounded theory (Corbin & Strauss, 2008). With the assistance of a qualitative data analysis program (ATLAS.ti7), a range of codes was created; themes emerged out of codes through a process of constant comparison.
Findings
In the following, we present respondents’ perspectives on the challenges of promoting the profession’s dual mission. Overall, the interviews suggested that, in order to effectively negotiate both the clinical and the political, social workers engage in intellectual and pragmatic strategies to promote well-being and to minimize potential risks to clients. Three broad themes emerged which centered upon (1) workers’ conscious struggles with the use of mental health diagnostic systems and their attempts to use diagnoses in order to promote empowerment and well-being; (2) a process of critically evaluating practice theories and methods based on their inclusion of concepts of power, control, and oppression, and their utility in promoting healing and empowerment; and (3) a varied, and at times, unclear view of the usefulness of feminist social work theory and practice as a tool for promoting the professions’ dual mission.
The Politics of Mental Health Diagnosis
Mental health diagnosis emerged as an important topic that involves considerations of social meanings and power relations. None of the participants’ agencies required therapists to have a diagnosis for the clients. In fact, a “no diagnosis policy” is seen as having a positive effect on DV survivors who have been manipulated by their abusers into thinking that there is something wrong with them. One participant specifically mentioned the labeling effect of diagnosing clients as the reason why they do not agree with the practice of mental health diagnosis. Instead of diagnosis, they try to focus only on symptoms or behaviors, especially when those are related to facilitating the healing process for their clients. I’m not really big on labeling people because then they kind of hang their hat on that, ‘Well I’m bipolar so that’s just what I do’ … As far as really being beneficial to the client, I think just ‘What are your symptoms? How are these interfering with the goals that you want to get to and what do we need to do about it?’ To me it’s much more valuable than label, label, label. (Diane) Another thing that we do is we talk about the ways in which we document, the language that we use, how we are framing what’s going on. Not omitting anything, but often it’s the way you describe you know and how you document that ends up hurting someone in court down the line. And there are a lot of misdiagnoses out (there). So it’s another way that we try to conduct outreach … to train medical professionals to understand trauma and what it looks like. And let’s not be so quick to put a diagnosis on someone for a mental health disorder, if actually a lot of the symptoms maybe are masking trauma. It’s looking like a bi-polar disorder, or paranoid personality disorder, but actually it’s a trauma symptom. (Alice) If a woman comes in and says I’m having severe mania, I mean, and the speech is pressured as we’re talking. How do you ignore that? You’ve got to deal with that, and I don’t think you’re labeling when you do that. I know there’s a lot of discussion in literature about labeling. But you have to deal with people’s psychiatric issues. (Tracy)
Therapeutic Interventions and Sociopolitical Contexts
A second theme that emerged concerns the ways in which DV workers assess, choose, and implement therapeutic models and techniques. We were curious whether workers prioritized particular models or theories and whether they would see specific practice models as more helpful in integrating the personal and social aspects of clients presenting concerns. Our respondents approach this work with a high degree of pragmatism, gravitating to an eclectic mix of methods, and an awareness of targeting needs specific to clients’ individual stages of recovery. What is more, these social workers do attempt to consider the ways in which models allow for the inclusion of macro-oriented concepts such as power and oppression, thus suggesting again an effort to incorporate macro concerns into direct practice interventions.
In terms of therapeutic models and techniques, most respondents shared that eclecticism is more helpful than adherence to a specific approach; no single therapy method can address all of the issues related to DV. As one participant noted, this is because “domestic violence is not a mental health problem, but a social problem that can exacerbate mental health issues.” Respondents noted that the helpfulness of a therapy technique or model depends on individualized situations and contexts as well as the stage at which clients are at in the process of recovery. For example, the use of solution-focused therapy might be premature for clients with severe trauma. If the client has just been admitted to the shelter, crisis intervention should come before introducing other therapy models.
Although individual symptoms can be addressed through a specific therapy technique, several therapists noted that one should always be mindful of environmental causal factors that may severely impair clients’ abilities to address the symptoms of the trauma. For example, therapists noted that there are a variety of tactics utilized by the abusers to control the women who they victimize; this has to be considered as part of the social context of any clinical work. An awareness of such social factors creates a critical consciousness for DV social workers who must adapt and modify clinical approaches to prevent victim blaming or a simplified view of DV. For instance, cognitive behavioral therapy (CBT) is cited by many participants as one of the most helpful therapeutic techniques, as many DV survivors may suffer from distorted cognitive processes due to years of control and oppression experienced at the hands of their abusers. However, participants shared that one of the risks of using CBT techniques is that this can send a message to clients that all of their concerns, such as the existence of DV or relationship problems, can be managed through a change in cognition. This may minimize the effects of external factors and ignore the abuser’s responsibility for initiating violence. Considering environmental factors is also critical because of the person–environment perspective is central to the role of social work. In the DV context, clinicians note that the ongoing presence of abuse in client’s life should be considered as the most important factor in adopting any therapy technique. Like with CBT because someone who is living a very simple life might be able to do the homework, whereas my clients, you don’t know sometimes where they’re going to be the next week, like for writing in a notebook about your feelings. So I feel like the clients who either are still with the abuser or are dealing with the abuser in like a co-parenting happening, but I think something like CBT or DBT, they don’t have control over a lot and so they, with emotion regulation, like how can you do that when someone is threatening you? (Karen) What I really like about the model in our field, it wasn’t the retrofitting a survivor’s experience into an old model or a prior model. It was truly taking survivors’ experiences, and trying to look at what the common thread was. So it came from their stories, from their experiences, and it actually reframes even the process of going in and out of the relationship as a part of the healing process, as a critical part of the healing process, not seen as relapse, like in a medical model or disease model. It’s not seen as a relapse, because that would insinuate it’s her fault, there is something wrong with her. It’s just about her readiness to change, and we know that there are so many more factors that are preventing her from moving along healing process and really getting to safety. Factors that are really out of her control. (Alice)
Ambivalence Toward Feminism
When participants were asked a question about their use of theoretical approaches to assess the situation of clients and practice methods to help clients, feminism arose as one of the most frequent topics throughout the interviews, even though they were not specifically asked to comment on feminism and its relation to their practice. Thus, a third theme that emerged in our study was the divergent ways in which workers thought about feminism and its capacity to serve as an overarching theory to ground micro to macro DV work.
Given the strong historical influence of the feminist movement, it is perhaps no surprise that feminism would organically emerge in the discussion of practice perspectives. It was more surprising, however, to see such divergent views these participants had on feminism, in terms of their understanding of what it is and how useful it is for their practice with DV survivors. For some, feminism was the most important framework in evaluating their practice as well as to understanding the problems confronted by their clients. For these respondents, the key question they asked in evaluating their practice was whether it was consistent with feminist principles. But not all participants mentioned feminism as their primary theoretical and practice framework. These participants perceived feminism as having too narrow of a focus to explain the complexity of DV, capturing only a partial picture of the problem. For example, feminism was seen as putting too much emphasis on gender socialization; in their practices, these clinicians also saw psychological and individual characteristics playing a significant role. Truthfully, I don’t believe that it’s all learned behavior. I think everybody that participates in domestic violence has got personal pain and there are some people that are sociopaths and psychopaths. So you can’t just put them all in one category and say they learned that because they watched dad shove mom and that’s how I’m going to do it. The pain level of the people that are participating in DV is greater than just saying something as trite as it’s learned behavior. And if you only offer it from that place, you’re not going to help everybody. (Laura) I think sometimes my experience is that, like it can only take clients so far sometimes. Like it doesn’t necessarily heal some of the trauma that they’ve experienced because of the feminist framework and where we see some of these issues coming from in our society. So I think it’s an important perspective to bring into it but I don’t think that can be the only perspective. (Helen)
There is also a concern that a feminist approach may alienate some clients. One participant stated that some clients feel intimidated or scared by feminist thinking because of the stereotypical image of feminist as a “radical or militant.” Therefore, this worker believed that taking the feminist approach to engage women who are experiencing severe trauma is not always effective. In social work the first thing you have to do is engage. And that’s crucial. And having worked with the mandated clients, if you don’t engage, you’ve lost them. And so what I’ve learned is that the feminist approach for me wouldn’t work, because from what I’ve seen, for example, we get a new person here. I go into the cafeteria and I use the softest voice I have and I say, ‘Hi, I’m the women’s therapist. What’s your name?’ And they’ll say ‘Oh, okay. I heard about you.’ Very nonthreatening, because that person’s been traumatized. And I think, from what I’ve observed, sometimes feminists, they come on pretty strong and that scares people. (Tracy) If you look at the research on domestic violence and know it’s still an issue, it’s still an issue of violence against women. It’s not gender neutral. So, like for example for me in the child protection world, a lot of times when I train on domestic violence, I talk about the fact that the majority of batterers are male and the majority of survivors are female We can’t just say because we have a simple assault charge on both people that that means that the violence is bidirectional. It means that we have to ask a lot more questions. We need to understand who is controlling who and more often than not, there’s the social male. (Emily)
Discussion and Implications
The findings of this study suggest that psychology and politics were intertwined in clinical social workers’ daily intellectual practices. In other words, the participants in this research study have evaluated the political implications of their clinical practice in terms of diagnosing practices of mental disorders and through the selection of practice theories for working with DV survivors. These social workers are aware of, and address, issues of domination and power imbalances between abusers and victims. Based on their appraisals of these issues, they attempt to create new systems of care and practice approaches tailored to address the issue of DV in the work with survivors. More specifically, the study’s participants attempted to redefine mental health services as a tool to empower survivors who have been traumatized by the power and control tactics used by abusers, assuaging deep-rooted suspicion toward the provision of mental health services for DV survivors.
Although our respondents agreed that mental health issues must be given proper attention, they were ambivalent about diagnosing clients with a mental disorder and about using the DSM. On one hand, they were concerned about the stigmatizing effect of diagnosing a client with a mental disorder as it may send the message that there is “something wrong with them.” Moreover, in the context of DV, where a mental disorder diagnosis may be used against the victim in the legal system, a cautious approach to mental health diagnosis and the use of the DSM is regarded as a necessary measure to protect women’s interests and prevent further abuse (Meier, 2009). Out of these concerns, they created alternative service systems where clinicians are not required to diagnose clients in order to seek reimbursement. This freedom from the managed care system has helped clinicians to avoid the clinical trap of the medical model espoused by the DSM, enabling them to focus on interpersonal and environmental factors. This might have been possible because clinicians in the DV field assessed their services within a social change framework, which led to collective efforts to create a system that aims to achieve client wellbeing within the political economy of mental health care systems.
However, clinical social workers did not completely discount the usefulness of the DSM, noting its normalizing effect on survivors. They recognized the reality of the current mental health system where the DSM is widely used. This mixed attitude among clinical social workers toward mental health diagnosis in general, and the DSM in particular, may reflect the bifurcated positions on this issue in the social work profession itself. While the majority of social work scholars and practitioners have advocated for the use of the DSM as a primary assessment tool for mental disorders, some of the strongest critics of the DSM have also come from social work (Gomory, Wong, & Lacasse, 2011; Kutchins & Kirk, 1997). Kutchins and Kirk, for instance, have criticized the DSM for its lack of reliability and validity. Further, they have questioned whether it is able to be used to accurately diagnose the mental disorders of oppressed social groups, noting that is has stigmatized these populations by labeling them as mentally ill (Kutchins & Kirk, 1997). Because of this ambivalent position toward the DSM and the psychiatric approach within the field, clinical social workers might be trained to use the DSM for their practice while critiquing it at the same time (Frazer, Westhuis, Daley, & Phillips, 2009).
It was also clear from the interviews that clinical social workers were constantly evaluating existing theories and therapeutic interventions as they applied them in their practice. One important criterion seemed to be how well the theories and interventions addressed the dynamics of DV and how helpful they were in healing survivors. Social workers selected or adapted theories based upon their acknowledgment of social factors such as the power and control of abusers and oppressive social forces, which can hinder survivors’ efforts to escape violence. Specifically, clinicians preferred to use models that can take into account the influence of an abuser’s use of power and control tactics (Burke, Gielen, McDonnell, O’Campo, & Maman, 2001).
The relevance of feminist thought to clinical work in a DV setting was a contested subject. With a few exceptions, the majority of participants were reluctant to fully endorse feminism as the most significant explanatory and practice framework for their work. Clinical social workers believed that other theories should be combined with feminism to fully understand the causes of DV, contending that psychological theories are needed to understand why certain men become abusive. Others admitted that feminism helped them to understand the etiology of DV but felt that it was inadequate as a framework to help heal survivors’ trauma. The same mixed views are also found in other research studies. McPhail, Busch, Kulkarni, and Rice (2007) also found inconsistencies and tensions between assumptions of the feminist model and the realities perceived among DV advocates (McPhail, Busch, Kulkarni, & Rice, 2007). Accordingly, these workers expressed a desire for a more flexible paradigm that allows the practitioner to “cherry pick” from various theories and practice models, combining feminist concepts of empowerment with knowledge from disciplines such as neurology and psychology.
It is also notable that almost no participants mentioned the iconic scholars who provided feminist analyses of mental disorders, trauma, and mental health practice (Worell & Remer, 2003). It is not clear why these historic thinkers were not mentioned, but we surmise that this omission may suggest a diminishing influence of feminist thought and practices within the broader profession. Recent investigations by scholars on feminism’s place in the profession concluded that, while feminist social work thrived under the influence of second wave feminism in the 1980s, these theorists failed to develop theories that recognized differences among women while sustaining a dynamic commitment to solidarity. Due to this lapse in theoretical development, recently trained social workers are unable to articulate the theoretical foundations of feminist practice and research (Gringeri, Wahab, & Anderson-Nathe, 2010; Kemp & Brandwein, 2010). In this regard, further research is needed to clarify our understanding of why feminism did not hold a greater appeal to social workers in DV settings, where one would assume that gender issues and concerns about patriarchy would be paramount. More research in this area will help to augment the recent efforts by scholars to revive feminism in social work as a way to reinvigorate the profession’s commitments to social justice and social change (Gringeri & Roche, 2010).
DV should be also more actively incorporated into social work education. The field has been considered as one of the most important topics by social work scholars and educators because of its prevalence across practice settings, including child welfare and public welfare settings (Hagen, 2001; Postmus & Ortega, 2005). However, with few exceptions, the history of the BWM is often not covered in social work education on DV or in U.S. social welfare history. Given its historical struggles and impacts on political consciousness, DV is a powerful example of how political and historical context affects our understanding of an issue. Therefore, the influence of the BWM and DV practice on the integration of micro and macro practice should be duly recognized in the profession.
Limitations and Conclusion
This study used a relatively small sample, so caution is advised in generalizing from the findings. The study’s relatively small sample size was partly due to the limited number of DV organizations that had the financial resources to hire clinical social work staff. For those organizations with a clinical program, the size of the program and number of clinical social workers varied depending on the agencies’ focus and the availability of funding. Also, the research questions were broad in nature, so not every question was explored with follow-up questions such as participants’ definition of feminism. More follow-up questions would have made it possible to provide deeper understanding of what feminism means to clinical social workers in the DV field. Despite these limitations, this study uncovered some ways in which clinical social workers attempt to intellectually and pragmatically integrate their micro practice and macro practice, which may provide empirical data for furthering the discussion on the subject in the profession.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.