
Abstract
The study reported here determined that a national sample of single mothers had no health care coverage for an average of 9.35 months during a 32-month period during and after the Great Recession that began in December 2007 and ended in June 2009. Using comprehensively defined employment problems, it also found that adequately employed single mothers had the fewest months without health care coverage (M = 4.36), which more than doubled for those who experienced unemployment or involuntary gaps in employment, and tripled for those who experienced underemployment. The multivariate results confirm that employment problems place single mothers at a high risk of lacking health insurance. Implications for health care policy are discussed.
With the exception of elderly persons who primarily receive health insurance through Medicare, the majority of individuals in the United States depend on employment-based health insurance to pay for their health care needs (U.S. Census Bureau, 2011). As would be expected, when unemployment is high, such as during and after the “Great Recession” from December 2007 to June 2009, the uninsured rate among the nonelderly increases (Fronstin, 2010). Although this increase occurs primarily for adults (Holahan, 2011), variations in health care coverage among this group exist. For example, during 2009, 33% of single mothers had no health care coverage, compared with 19% of all men and 18% of married mothers (Hayes & Hartman, 2011). Unlike married mothers, when single mothers are unemployed, they cannot rely on husbands to provide health insurance. In addition, women receive lower wages and are more likely to be employed part time than are men, making it less likely that employers will provide health insurance benefits even when single mothers are employed (Joint Economic Committee, 2009). The aforementioned studies demonstrated that single mothers have an increased risk of lacking health insurance and the importance of examining relationships among multiple employment problems, such as unemployment, part-time employment, and low earnings and the lack of such coverage.
The research presented here explored the relationships among comprehensive measures of employment problems and the number of months that single mothers had no health care coverage for 32 months during and after the Great Recession. The findings provide important insights into the types of employment problems that are related to the lack of health insurance among this vulnerable population. Although the Supreme Court of the United States (2012) recently upheld the main provisions of the Patient Protection and Affordable Care Act (PPACA), which is expected to provide near universal health care coverage by 2014 (Doty, Collins, Robertson, & Garber, 2011), the House of Representatives passed a bill to repeal the PPACA 2 weeks later. In addition, political conservatives continue their efforts to repeal this legislation (Pear, 2012). These ongoing activities suggest the need for additional data to demonstrate the consequences of repealing this law for single mothers’ health insurance coverage, particularly during months of high unemployment.
Importance of Health Insurance Coverage
Compared with adults with health care coverage, adults without such coverage are at a greater risk of reporting barriers to health care, having no usual source of health care, postponing seeking health care because of its cost, and being unable to fill prescriptions (Kaiser Commission on Medicaid and the Uninsured, 2012b). Likewise, adults who lose health insurance after they lose their jobs report similar problems to those who continue coverage after their job loss (Doty et al., 2011). The lack of health care coverage also appears to increase the difficulty of receiving adequate medical care more for women than for men. For example, 39% of men compared to 52% of women have difficulty obtaining needed medical care. In addition, the ability to access health care varies by the length and adequacy of health care coverage. Only 9% of nonelderly women fail to obtain needed medical screenings because of the cost when they are insured all year, but not those who are underinsured. This rate increases to 23% for those who are insured all year, but underinsured, and 42% for those who are uninsured at any time during the year (Joint Economic Committee, 2009). Examining access to health care by marital status demonstrates the vulnerability of single mothers. Although 38% of married mothers fail to see a doctor because of the cost, 45% of single mothers fail to do so, and failing to fill a medical prescription is 33% higher for single mothers than for married mothers (Hayes & Hartman, 2011).
Because women have specific health needs that require them to seek more regular health care than do men, the consequences of inadequate health insurance coverage are more severe for women’s health, as well as for the health of their unborn children and infants. For example, women are more likely to have reproductive health issues, including those related to contraception, pregnancy, and childbirth, and to contract serious sexually transmitted diseases (Joint Economic Committee, 2009). Having health insurance is even more critical during recessions, since research has demonstrated that unemployment adversely affects the physical and mental health of adults (McKee-Ryan, Song, Wanberg, & Kinicki, 2005). In addition, inadequately employed or underemployed adults (such as those who earn poverty wages and those who are involuntarily working part time) are at an increased risk of experiencing health problems (Dooley & Prause, 2004).
Other studies have demonstrated that the lack of health insurance can also have economic repercussions, such as damage to a family’s financial situation after paying health care costs (Joint Economic Committee, 2009). Economic problems are particularly important for single mothers, since approximately 32.6% of female-headed families live in poverty, compared with only 6.2% of married-couple families (U.S. Census Bureau, 2011). In addition to employment increasing access to health care coverage, such coverage can enhance employment, which is particularly important for single mothers who frequently depend on their own earnings to support their families. Since Temporary Assistance to Needy Families (TANF) was established in 1996, obtaining employment is even more important, particularly for low-income, single mothers. Although most welfare leavers and other low-wage workers become employed, many lose their jobs and experience long periods of unemployment (Lee, 2007). Lee’s research indicated that having a health problem reduces job retention, and access to employer-provided health insurance is critical for retaining a job and becoming upwardly mobile, particularly for low-income mothers.
Employment Problems and Health Care Coverage
When the Great Recession began in December 2007, the unemployment rate was only 5%, which rose to 9.5% when the recession officially ended in June 2009 (U.S. Department of Labor, 2013). Unfortunately, this rate remained fairly stable in 2010 and decreased to only 8.9% the following year (U.S. Department of Labor, 2011). In 2010, 42% of single mothers, compared to 26% of married mothers, had been unemployed for at least 1 month in the previous 2 years (Hayes & Hartman, 2011). As might be expected, the uninsured rate grew during the Great Recession from 12.3% in May 2007 to 16.4% in July 2009, and workers with the lowest earnings experienced the largest decline in coverage (Fronstin, 2010). Other studies have directly connected health care coverage to employment status. In 2010, for working-aged adults, 15% of those working full time, year round; 19.5% of those working some time; and 28.6% of those working less than full time, year round lacked health care coverage the entire year (U.S. Census Bureau, 2011). In addition, in 2011, more than 70% of the uninsured went without health care coverage for more than 1 year, and 51% for more than 3 years (Kaiser Commission on Medicaid and the Uninsured, 2012b).
Hayes and Hartman (2011) also confirmed the relationship between health care coverage and employment status among women. In 2010, 37% of unemployed women, 34% of nonretired women not in the labor force, 25% of women employed part time, but only 11% of women employed full time reported no health care coverage some time during the previous year. Research on a sample of low-income, working women indicated that job changes decrease stable health care coverage, while working more hours increases such coverage (Anderson & Eamon, 2005). However, another study with past and current welfare recipients (Danziger, Corcoran, Danziger, & Heflin, 2000) found that a higher percentage of mothers who worked in all 12 months had no health insurance (20%) compared with mothers who did not work in any month (7.5%).
The Study
The literature review demonstrated that single mothers are particularly vulnerable to experiencing unemployment and lacking health insurance, particularly during periods of economic downturns. Our study makes two main contributions to this body of knowledge. First, we used national data for 32 months during and after the Great Recession when unemployment was exceptionally high to determine the number of months that single mothers lacked health care coverage. Second, we investigated whether comprehensively defined employment problems—unemployment or involuntary gaps in employment and underemployment—compared with adequate employment are related to the number of months that these mothers had no health insurance. In this article, we use the results of our study to address the consequences to single mothers’ health care coverage in the absence of the PPACA provisions.
Method
Data and Sample
For this study, we used the Survey of Income and Program Participation (SIPP), a longitudinal survey that interviews nationally representative samples of noninstitutionalized U.S. households every 4 months (referred to as a wave). To examine the relationships among employment hardships and a variety of sociodemographic characteristics and health insurance coverage 32 months during and after the Great Recession, we took data from the 2008 panel, which interviewed respondents between August 2008 and March 2011.
We began with a sample of 455 single mothers aged 18–65 who were heads of households and had at least one related child each under age 18 living in their households at the first wave. We then restricted the sample to those with completed interviews in all eight waves during the 32 months (N = 349). To address the concern that there might be some differences in individual and family characteristics between single mothers who completed all the waves of the survey and those who failed to complete all the waves, we compared our sample to the excluded cases. The bivariate results indicated no statistically significant differences between the two groups in any of the covariates described in the next section.
Measures
Dependent Variable
The lack of health insurance was measured by the number of months (ranging from 0 to 32) in which the mothers reported having no type of health insurance (including Medicare, Medicaid, and other public health insurance; private health insurance; and military-related health care) during the 32 months.
Independent Variables
Informed by other research (e.g., Dooley & Prause, 2004; Kalil & Ziol-Guest, 2005, 2008), we measured three employment variables during the 32-month period: unemployment/involuntary gaps in employment, underemployment, and adequate employment (the reference group). Adequate employment is defined as full-time employment or voluntarily part-time employment and earning above 125% of the poverty level. It includes continuous adequate employment, transitions to stable adequate employment, and voluntary gaps in employment in which the number of months of adequate employment is greater than the number of months of underemployment. Unemployment/involuntary gaps in employment includes continuous involuntarily unemployment (e.g., the loss of or layoffs from jobs), continuous voluntary unemployment (e.g., staying home to take care of children, being retired, attending school), and involuntary separations or gaps in employment. Underemployment is defined as being employed full time but earning less than 125% of the poverty line or being involuntarily employed part time. This category includes continuous underemployment, transitions to stable or unstable underemployment, and voluntary gaps in employment in which the number of months of underemployment was greater than the number of months of adequate employment. (For a more detailed description of these employment variables, see Wu & Eamon, 2011.)
Informed by prior research (e.g., Fronstin, 2010; Holahan, 2011), we included a number of covariates (see Table 1 for the detailed categories of the covariates). Mothers’ characteristics were age, education, and race/ethnicity measured at the first wave and if ever was a U.S. citizen and had a work disability during any of the 32 months. The household characteristics, which were averaged across the 32 months, included the number of mothers’ children aged 18 or younger in the home, number of months being single, number of months receiving any means-tested public benefits (TANF cash benefits, general assistance, Supplemental Security Income, food stamps, and Women, Infants, and Children Program), and the log of total monthly family income. Finally, region of the country was measured at the first wave.
Data Analysis
Percentages or means were calculated to examine the number of months that the single mothers lacked health insurance, the employment variables, and the individual and household characteristics. Because the dependent variable was continuous, we estimated an ordinary least squares (OLS) linear regression model to examine the relationships among employment hardships and the other variables in the model and the number of months these mothers had no health insurance coverage. With regard to the skewness of the dependent variable, the number of months without health insurance was .93, which was less than 1.0. This skewness suggests that the distribution of the dependent variable was not highly skewed. Therefore, it was appropriate to use the OLS regression model.
In addition, we used standardized coefficients to determine which variables had the strongest relationships with the number of months without health insurance coverage. Sample weights, which generate unbiased estimates of parameters and standard errors for the U.S. population, were used in all the analyses (U.S. Census Bureau, 2001).
Results
Descriptive Results
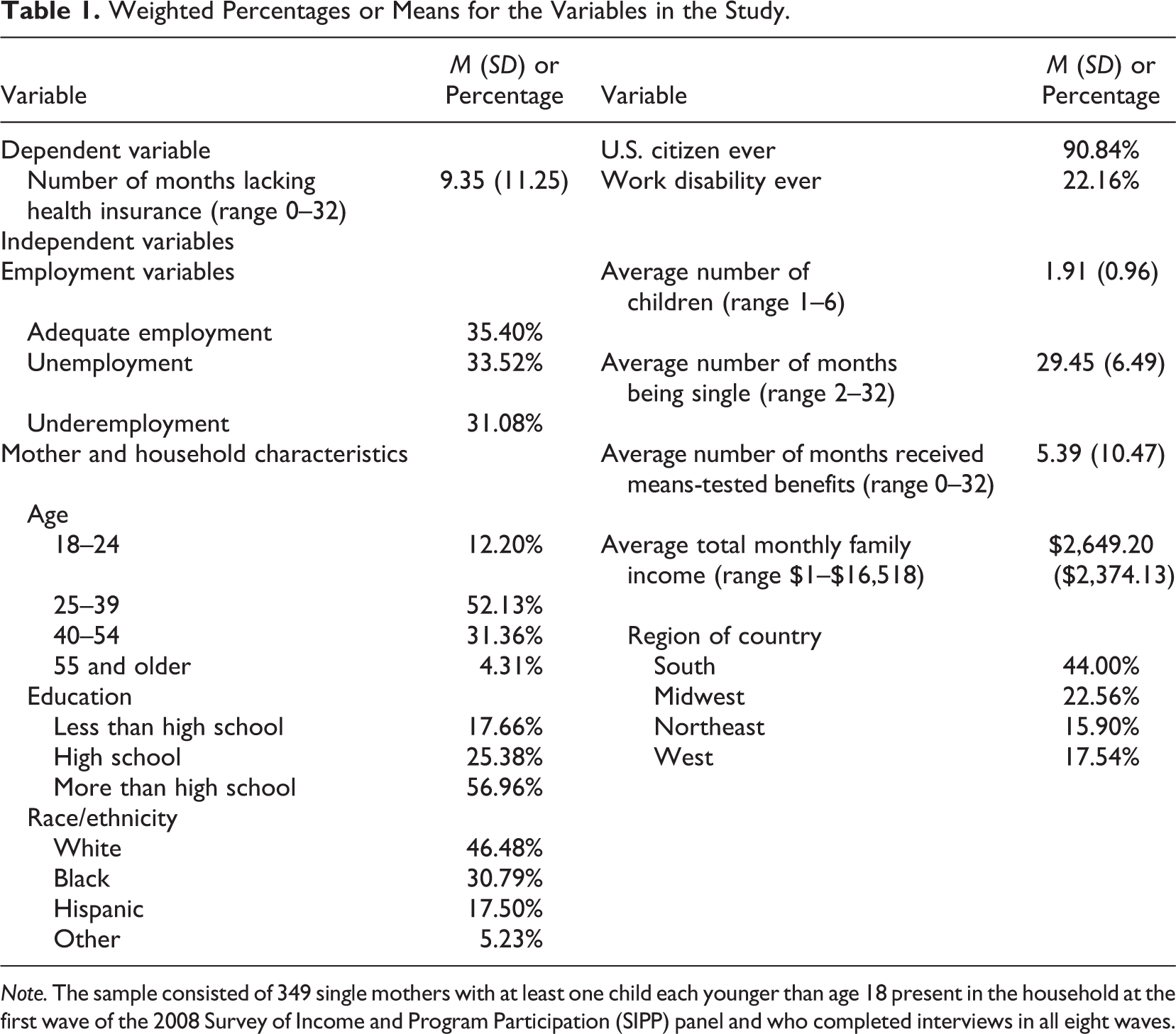
Table 1 presents the weighted percentages or means for the variables that were used in the study. The results indicate that during the 32 months, the single mothers had an average of 9.35 months without health care insurance, and only a little over one third of them were adequately employed. Moreover, the majority (65%) of these mothers either experienced unemployment/involuntary gaps in employment (33.52%) or underemployment (31.08%). As is also demonstrated in this table, more than half the sample were aged 25–39 (52.13%) and had more than a high school education (56.96%). A plurality of the sample was white (46.48%) and resided in the South (44.0%). At some time during the 32 months, 90.84% of the mothers were U.S. citizens, and approximately 22% had a work disability. During these months, the mothers had an average of two children, remained single for almost all the months (M = 29.45), received means-tested benefits for an average of 5.39 months, and had an average monthly family income of $2,649.
Weighted Percentages or Means for the Variables in the Study.
Note. The sample consisted of 349 single mothers with at least one child each younger than age 18 present in the household at the first wave of the 2008 Survey of Income and Program Participation (SIPP) panel and who completed interviews in all eight waves.
Figure 1 displays the average number of months in which all the single mothers lacked health insurance and the single mothers’ employment status during the 32 months. Single mothers with adequate employment had the fewest months (M = 4.36) without health insurance, which increased to an average of 10.06 months for those who experienced unemployment/involuntary gaps in employment and increased once again for single mothers who were underemployed (M = 13.44).
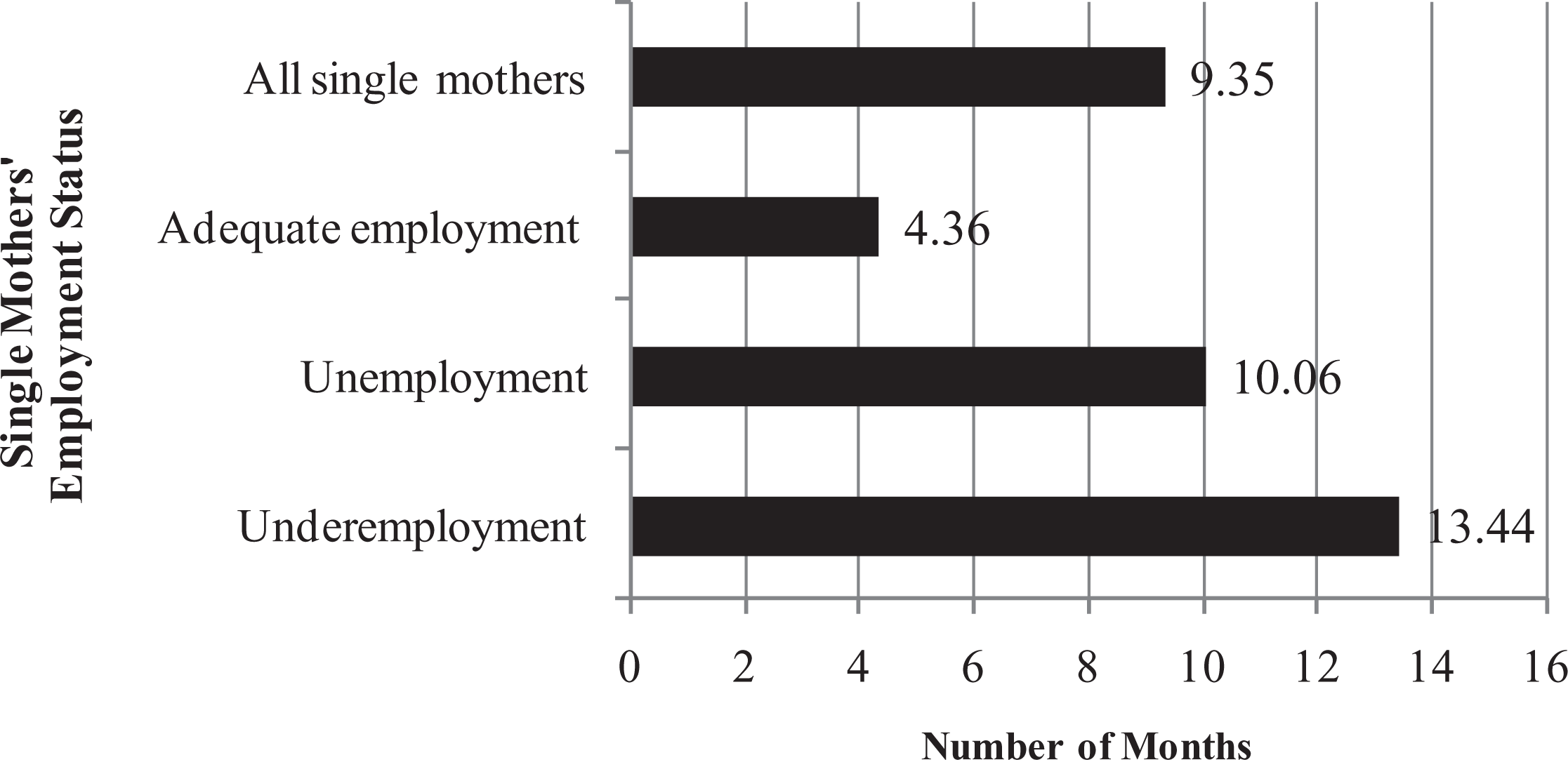
Average number of months without health insurance during the 32-month period, by the single mothers’ employment status. Note. The sample consisted of 349 single mothers with at least one child each who was younger than age 18 and was present in the household at the first wave of the 2008 SIPP panel and completed interviews in all eight waves. SIPP = Survey of Income and Program Participation.
Multivariate Results
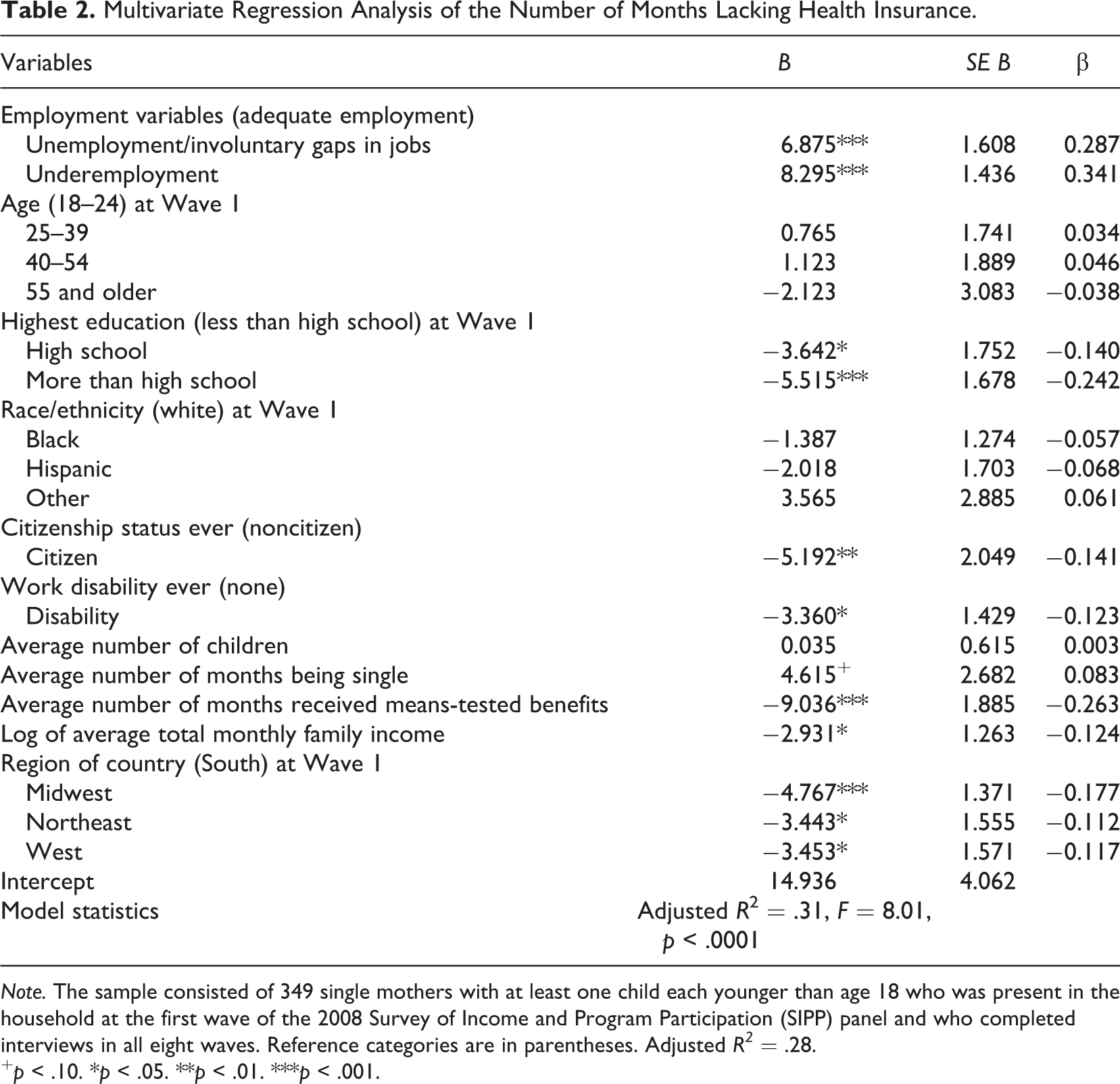
The multivariate results (see Table 2) demonstrate that compared to the single mothers who were adequately employed, those who were unemployed or had involuntary gaps in employment experienced more months without health insurance coverage (B = 6.87, p < .001), than did the underemployed single mothers (B = 8.29, p < .001). A number of the covariates demonstrate significant negative relationships with the number of months that the single mothers lacked health insurance. These single mothers had a high school education (B = −3.64, p < .05) or more than a high school education (B = −5.52, p < .001) during Wave 1, compared with less than a high school education, and were U.S. citizens at some time during the study period (B = −5.19, p < .01). Moreover, those who ever had a work disability (B = −3.36, p < .05) received means-tested benefits for more months (B = −9.04, p < .001); had higher average family incomes (B = −2.93, p < .05); and resided in the Midwest (B = −4.77, p < .001), Northeast (B = −3.44, p < .05), or West (B = −3.45, p < .05), compared with the South, also had fewer months without health care coverage. The standardized coefficients indicate that the most important factors associated with the number of months without health insurance are underemployment (β = .34) and unemployment/involuntary gaps in employment (β = .29). The F statistic indicated a highly statistically significant model fit (adjusted R2 = .31, F = 8.01, p < .0001).
Multivariate Regression Analysis of the Number of Months Lacking Health Insurance.
Note. The sample consisted of 349 single mothers with at least one child each younger than age 18 who was present in the household at the first wave of the 2008 Survey of Income and Program Participation (SIPP) panel and who completed interviews in all eight waves. Reference categories are in parentheses. Adjusted R2 = .28.
+ p < .10. *p < .05. **p < .01. ***p < .001.
To address the possibility of multicollinearity among the different independent variables, we assessed the variance inflation factors, which showed that none was greater than 3 (range: 1.11–2.89). This finding suggests that the covariates are not highly correlated with the predictors (employment variables), and multicollinearity may not be a concern.
Discussion
The study found that single mothers had no health insurance for an average of 9.35 months, or approximately 29% of the 32 months during and after the Great Recession. Even adequately employed single mothers had an average of 4.36 months without health care coverage during these months. Moreover, compared with the adequately employed single mothers, the average number of months without health insurance was about 2.5 times higher for those experiencing unemployment/involuntary gaps in employment and slightly more than 3 times higher for those facing underemployment. Our results highlight that the underemployed single mothers had more months without health insurance than did those who were unemployed or had involuntary gaps in jobs. The multivariate results confirm these relationships, and compared with the other variables, the employment variables have the strongest relationships with the lack of health insurance. On the other hand, single mothers who had fewer months without health insurance were more educated, were U.S. citizens, had a work disability, received means-tested benefits for more months, had higher family incomes, and resided in areas of the country other than the South.
Since the majority of nonelderly individuals in this country receive health insurance coverage from their employers (U.S. Census Bureau, 2011), when single mothers experience unemployment/involuntary gaps in employment, insurance coverage would be expected to decrease. Our results are also consistent with past research that indicated that even when individuals are employed but work in part-time or low-wage jobs, they are less likely to receive employment-based health insurance (Kaiser Commission on Medicaid and the Uninsured, 2012b). The finding that the underemployed single mothers had more months without health insurance than those who experienced unemployment/involuntary gaps in employment is likely due to health care policies that provide at least two advantages to people who are unemployed. First, some unemployed workers can benefit from the Consolidated Omnibus Budget Reconciliation Act (COBRA), which mandates that employers that sponsor health care coverage and have at least 20 workers make coverage available for up to 18 months under certain circumstances, such as job loss (Doty et al., 2011). Second, state eligibility guidelines for Medicaid usually require individuals who are employed to meet higher income thresholds than those who are unemployed (Kaiser Commission on Medicaid and the Uninsured, 2012a). As a result, underemployed single mothers can earn similar incomes as those who are unemployed who receive unemployment compensation, yet not qualify for Medicaid benefits.
The statistically significant negative relationships that were found among the covariates in our study and the number of months with no health care insurance were difficult to compare with past research because the samples and insurance measures were inconsistent. Nonetheless, the results are not unexpected. More educated single mothers likely have fewer months without health insurance because they are better able to obtain jobs that provide health care benefits. These mothers also may have greater knowledge of alternative sources of insurance coverage. The findings that single mothers who were U.S. citizens and had a work disability experienced fewer months without insurance coverage are not surprising. Noncitizens are frequently excluded from both public and employment-based health care plans (Kaiser Commission on Medicaid and the Uninsured, 2012b), and many single mothers with a work disability likely qualify for Medicaid. Single mothers who receive means-tested benefits for more months likely have fewer months without health care insurance because they also meet eligibility guidelines for public health insurance. In addition, applying for one type of means-tested benefit may increase the tendency to apply for and receive other types. Single mothers with higher household incomes can have fewer months without health insurance because they use the income to purchase private insurance, pay copremiums, or participate in COBRA. Finally, the finding that residence in the South places these mothers at risk of having more months without health care coverage could be due to lower rates of employment-based health insurance (Holahan, 2011) and lower Medicaid eligibility thresholds in the southern states (Kaiser Commission on Medicaid and the Uninsured, 2012a) compared to other regions of the country.
This study had a number of limitations, including the inability to establish a causal order between the employment variables and health care coverage over the 32 months. We also failed to control for important changes over time (e.g., education and area of residence), and the results may be biased because of the omitted variables, such as mothers’ health problems and other job characteristics that are related to both employment hardships and health insurance coverage. Possible biases may also exist from sample attrition across the eight waves.
Despite these limitations, our findings provide important information for social workers, legislators, and others to advocate for continuing the PPACA policies. These findings, in conjunction with past research, indicate that in the absence of the PPACA provisions, employment, governmental programs, and private purchase will not increase health care coverage for vulnerable groups such as single mothers. As our literature review indicated, the lack of health care coverage has both health and financial consequences for these mothers and their children. Mothers without health insurance have difficulty obtaining adequate medical care, which can adversely affect the health of their unborn children and their ability to parent their children. The lack of health care coverage and related health care problems also increase health care costs and interfere with employment, which only intensify the financial hardships that single-mother families disproportionately face. Moreover, the finding that underemployed single mothers face a higher risk of lacking health insurance than unemployed single mothers has implications for TANF and social work. Single mothers who are expected to and do enter the workforce to provide for their children, yet are able to find only low-paying and part-time jobs that provide less access to health care coverage than their unemployed counterparts, is a social justice issue that should attract the attention of social work advocates. Furthermore, the U.S. Department of Health and Human Services (2012) recently announced that it will allow states to develop demonstration projects to identify more effective strategies for improving employment outcomes for TANF recipients. Our findings demonstrate the need for such waivers to assist welfare recipients (particularly single mothers) to obtain not only employment but “adequate” employment.
Since the 1980s, employment-based health insurance has been decreasing (Glied, Jack, & Rachlin, 2008). Even when employers provide health insurance, it is not available to all employees, such as part-time and low-wage workers, those recently hired, and those who cannot afford the shared premiums (Kaiser Commission on Medicaid and the Uninsured, 2012b). In addition, when workers are eligible to participate in COBRA, the cost is frequently unaffordable (Doty et al., 2011). This is likely the case even with the American Recovery and Reinvestment Act of 2009, which provides a maximum subsidy to cover 65% of the cost of COBRA (Fronstin, 2010).
Although all the states currently make full or partial public health insurance available to parents who meet income and other guidelines, states vary in their income thresholds and copayment premiums, which can prevent single mothers from accessing public health insurance. As we discussed previously, almost all the states have higher income thresholds for unemployed parents than for working parents. In January 2012, only 18 states (and the District of Columbia) extended eligibility for Medicaid to parents with incomes that are at or above the federal poverty line, and the median Medicaid eligibility threshold for working parents is 63% of the federal poverty line (Kaiser Commission on Medicaid and the Uninsured, 2012a). Primarily because of the high cost, private insurance covers approximately only 5.5% of the individuals in this country (Kaiser Commission on Medicaid and the Uninsured, 2012b), and it is usually purchased for a short time to “bridge the gap” in employment-based coverage (Ziller, Coburn, McBride, & Andrews, 2004).
When fully enacted, the provisions of the PPACA should increase health care coverage for single mothers and other vulnerable groups. Currently, the provisions allow adults to remain on or join their parents’ insurance until age 26 and require insurance companies to cover those with preexisting conditions. By 2014, near-universal coverage should be achieved for the uninsured by subsidizing health insurance through public programs or by subsidizing private health insurance offered through new state insurance exchanges (Doty et al., 2011).
In conclusion, our results suggest that if the PPACA is repealed, single mothers will continue to be at risk of lacking health insurance regardless of their employment status. Our most notable finding is that single mothers who work involuntarily part time or for low wages are more likely to lack such coverage than are unemployed mothers. If society wants to “make work pay” and to ensure that single mothers are sufficiently healthy to pursue career goals and to care for their children, then Congress must continue the provisions that will provide coverage for universal health care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.