
Abstract
This quantitative and descriptive study investigated the quality of life (QOL) and attitudes toward aging of 270 older women in Sanliurfa Province, Turkey. The Turkish versions of the World Health Organization Quality of Life Instrument—Older Adults Module and the World Health Organization—Attitudes Toward Aging Questionnaire were administered to the participants. The results indicated that there was significant relationship between the women’s QOL and attitudes toward aging. Two dimensions of attitudes toward aging (physical change and psychological growth) were significant predictors of QOL in the women. It was also found that literacy and happiness affected some dimensions of the women’s QOL and some subscales of attitudes toward aging.
The increasing number of older people in the world, with higher expectations of a good quality and healthy life and with their high demands for health and social care, has led to international interest in the enhancement and measurement of quality of life (QOL) and attitudes toward aging in older age (Bowling, 2007). The world is experiencing a profound and irreversible demographic shift as older people are living longer and healthier than ever before (United Nations, 2001). In 2002, older people constituted 7% of the world’s population, and this figure is expected to rise to 17% globally by 2050 (U.S. Census Bureau, 2004). In Turkey, the percentage of the population aged 60 and older was 6.4% in 1985 and increased to 8.4% in 2000. The percentage was estimated to increase to approximately 9.5% by 2005 (7.4 million) in Turkey (Donmez, Gokkoca, & Dedeoglu, 2005; Hacettepe Institute of Population Studies, 2003). According to the Turkish Statistical Institute, the elderly population, counted as 3.9 million in the 2000 census, will represent 19% of the overall population by 2050 (State Planning Organization, 2007). Self-reported health status, QOL, and attitudes toward aging in Turkey are also increasing in importance for the elderly (Eser, Saatli, Eser, Baydur, & Fidaner, 2010).
QOL was defined by the World Health Organization Quality of Life Instrument group (WHOQOL, 1993, 1995) as “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” It is a broad-ranging concept affecting a person’s physical health, psychological state, level of independence, social relationships, and relationships with salient features of his or her environment (Bodur & Cingil, 2009).
There are significant relationships between QOL and attitudes toward aging in older adults. Eser, Saatli, Eser, Baydur, and Fidaner (2010) in Turkey; Low, Molzahn, and Kalfoss (2008) in Canada and Norway; and Fang et al. (2011) in some European countries found significant relationships between some subscales of QOL and attitudes toward aging in older people. Kalfoss, Low, and Molzahn (2010) found that all the subscales of the World Health Organization Quality of Life Instrument–Older Adults Module (WHOQOL-OLD) and the WHO-Attitudes Toward Aging Questionnaire (WHO-AAQ) correlations were significant in the Canadian and Norwegian samples, the lowest being between psychosocial loss and psychosocial growth for Canada (r = .363) and Norway (r = .132). Some studies and reports have confirmed that social support and independent living (autonomy) are strong determinants of the health-related QOL of older adults (Borg, Hallberg, & Blomqvist, 2006; Borglin, Jakobsson, Edberg, & Hallberg, 2006; Constança, Fonseca, Ignácio, & Amado, 2003; Eser et al., 2010; Hellstrom, Persson, & Hallberg, 2004).
The existence of charity institutions in all periods throughout Turkish history shows that elderly people were always assisted and protected in Turkish society (State Planning Organization, 2007). These services have been provided mainly by the Association of Social Services and Child Protection and, to a lesser extent, by local administrations, foundations, associations, some public organizations, and private individuals with the aim of helping many old people at the same time (Doğan & Değer, 2004). However, in Turkey, professional home care foundations and services for elderly people are insufficient and rare. Therefore, older people without access to family caregivers or who are incapable of self-care tend to live in assisted living facilities (Bodur & Cingil, 2009). There has been little research related to QOL and attitudes toward aging in older adults, especially women, in Turkey. Moreover, research related to happiness, well-being, health status, QOL, and the health-related QOL of elderly people in Turkey is still in its infancy for both older men and women. Research using the WHOQOL-OLD assessments with Turkish older people (Luleci, Hey, & Subasi, 2008) is currently lacking.
It is important to understand the significant determinants of QOL and attitudes toward aging in various subgroups of older adults (such as women) to support evidence-based policy guidelines, program development, and policy decisions in the Turkish health and social systems. The study presented here is the first study on the relationship between QOL and attitudes toward aging in older women in Turkey. The purpose of the study was to investigate the QOL and attitudes toward aging of elderly Turkish women in Sanliurfa Province, Turkey; to explain the relationship between QOL and attitudes toward aging; and to analyze differences in QOL and attitudes toward aging in these elderly women by levels of happiness and literacy. This article reports on an analysis of the factors that influence QOL and attitudes toward aging among women aged 60 or older who were living in low-income urban neighborhoods in Sanliurfa, Turkey.
Method
The study investigated the QOL and attitudes toward aging of older women in Turkey using a quantitative research design. QOL and attitudes toward aging were used as dependent variables, and happiness and educational status were used as independent variables. Also, when determining the predictors of QOL, the dimensions of attitudes toward aging were used as independent variables. The dimensions of QOL and two dimensions of attitudes toward aging were used as independent variables to analyze the predictors of psychosocial loss. The hypotheses were as follows:
Hypothesis 1. There are significant relationships between QOL and attitudes toward aging in older women.
Hypothesis 2. The subscales of attitudes toward aging (psychosocial loss, physical change, and psychological growth) significantly regress with the QOL of older women.
Hypothesis 3. Physical change; psychological growth; sensory abilities; autonomy; past, present, and future activities; social participation; (thoughts on) death and dying; and intimacy significantly regress with psychosocial loss in older women.
Hypothesis 4. The QOL and attitudes toward aging of older women significantly vary with the women’s level of happiness.
Hypothesis 5. The QOL and attitudes toward aging of older women significantly vary with the women’s level of literacy.
Participants
A cross-sectional study was conducted in two neighborhoods in Şanliurfa, Turkey, with legal permission from the Governor’s Office and the Health Authority Management of Sanliurfa. The field trial was conducted with 270 older women aged 60 and older who were living at home without community health care. A list of these women and their information and addresses was obtained from the Governor’s Office and the Health Authority Management of Sanliurfa.
Instruments
WHOQOL-OLD
The WHOQOL-OLD was originally developed by the WHOQOL Group for investigating the QOL of older adults (Power, Quinn, Schmidt, & WHOQOL-OLD Group, 2005). The WHOQOL-OLD (Fleck, Chachamovich, & Trentini, 2006; Power et al., 2005; WHO, 2006) consists of 24 items (rated on a 5-point Likert-type scale) divided into six facets or subscales. Facet 1 evaluates sensory abilities on the basis of the following items: sensory impairment (taste, smell, sight, hearing, and touch) affecting daily life, a loss of sensory abilities that affects participation in activities, problems with sensory functioning affecting social interaction, and rating of sensory functioning. Facet 2 evaluates autonomy on the basis of the following items: freedom to make decision, feeling in control of one’s future, people around oneself being respectful of one’s freedom, and the ability to do things one would like to do. Facet 3 includes questions regarding past, present, and future activities to determine the following: satisfaction with the current availability of opportunities to achieve goals, satisfaction with having received the recognition one deserves in life, satisfaction with what one has achieved in life, and confidence that one has things to look forward to. Aspects of social participation are evaluated in Facet 4: the perception that one has a sufficient number of activities to perform each day, satisfaction with the way in which one is using one’s time, the perception of an appropriate activity level, and satisfaction with the number of opportunities one has to participate in community activities. Facet 5 evaluates the attitudes an individual has toward death and dying, concerns about the way in which one will die, the fear of not being able to control one's death, the fear of dying itself, and the fear of a painful death. Facet 6 includes questions related to intimacy to determine the following: feeling a sense of companionship in life, experiencing love in life, having opportunities to love, and having opportunities to be loved. Higher scores indicate a better QOL in each domain.
This questionnaire was administered on a face-to-face basis, and the period assessed was the previous 2 weeks. Possible scores on the facets ranged from 4 to 20. A total score could also be calculated by summing the values of the individual items. For positively worded items, higher scores indicated a higher QOL; for negatively worded items, the score had to be recoded (Eser et al., 2010; WHO, 2006). The WHOQOL-OLD was validated for use in Turkey by Eser et al. (2010). In this study, the internal consistency reliability of WHOQOL-OLD was .745.
The AAQ
The AAQ is a self-report measure with which older people can express their attitudes toward the process of aging. The development of the AAQ followed a coherent, logical, and empirical process that took full account of relevant gerontological knowledge and modern and classical psychometric analytical methods (Laidlaw, Power, Schmidt, & the WHOQOL-OLD Group, 2007). The scale consists of 24 items (rated on a 5-point Likert-type scale) in 3 domains (psychosocial loss, physical change, and psychological growth) with 8 items each (a minimum of 8 and a maximum of 40). The AAQ was validated for use in Turkey by Eser et al. (2011). In this study, the internal consistency reliability of the AAQ was .782.
Data Collection
The study was conducted between January 2 and January 27, 2012. All the instruments were administered to the older women in person by 67 students at the Department of Nursing, Harran University, Ankara. The students, who had taken courses in subjects related to the elderly, received specific instruction in the objectives of the study, the QOL of older people, and the research measurement tools. Each instrument could take 10 to 30 min to complete, depending on the speed of a participant’s response. We used the convenience sampling method and the following selection criteria: aged 60 and older and having no illness that was likely to cause death within the next year, such as cancer and dementia, or any other significant cognitive impairment. Older women who had acute complaints, psychiatric disorders, or severe hearing problems were included. Of the 650 eligible respondents, 260 refused to participate and 120 could not be contacted. Ultimately, 270 interviews were completed, for a response rate of 41.53%. Assistance was provided by a coresearcher if a participant requested or required help with the questionnaire. Informed consent forms were received from all the participants, and permission was obtained from provincial officials.
Data Analysis
All data were checked and analyzed using SPSS version 15.0. Descriptive statistics were used to identify the characteristics of the participants and the distribution of the subscale scores. The evaluation of internal consistency and intercorrelations were based on Cronbach’s α and bivariate correlations, respectively. The means, standard deviations, ranges, and minimum and maximum scores for QOL and attitudes toward aging were calculated. The Kolmogorov-Simirnov test was used for normality analysis. Pearson’s correlations between QOL and attitudes toward aging were performed for the total group of participants to determine the degrees of the relationships among the variables. Scores for the QOL and attitudes toward aging subscales were calculated, and reliability, correlation (for Hypothesis 1), multiple linear regression (for Hypotheses 2 and 3), and Student t (for Hypotheses 4 and 5) analyses were then conducted.
Results
Table 1 presents some of the sociodemographic characteristics of the older women in the study. The participants ranged in age from 60 to 98 (mean age: 67) and 80.10% were married. Of the 270 participants, 173 (64.08%) were illiterate. The majority of participants (83.70%) considered themselves to be happy.
Sociodemographic Properties of the Study Population (n = 270)
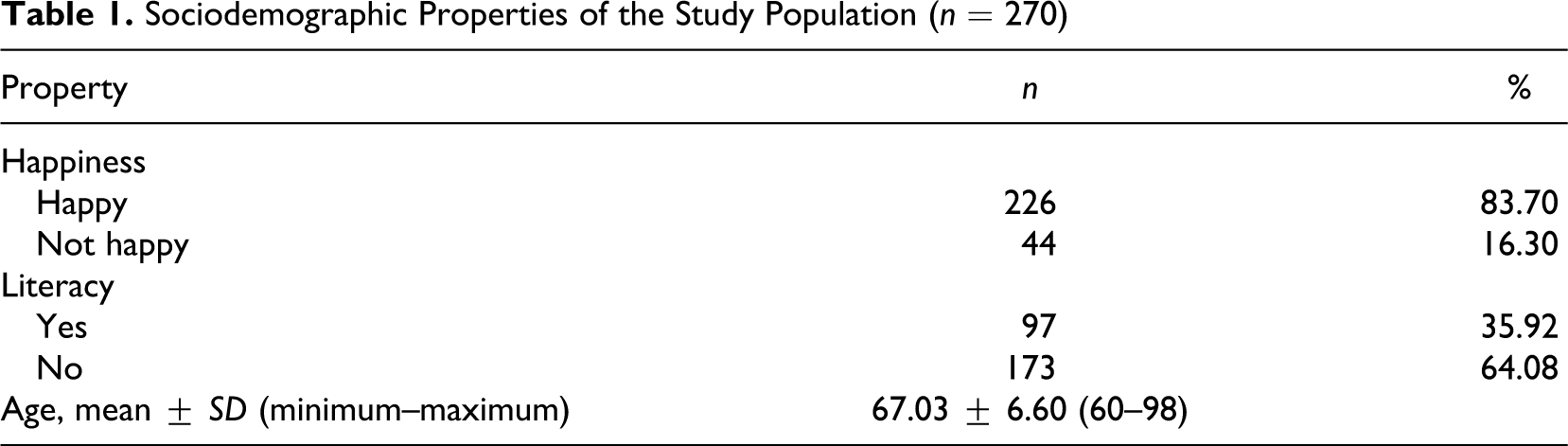
Table 2 shows the descriptive statistics (including the means, standard deviations, and range) for overall QOL, attitudes toward aging, and subscales of QOL and attitudes toward aging. The mean overall QOL score for the entire sample (270 participants) was 75.64 ± 10.75. The theoretical maximum score of the overall QOL was 120. This mean score indicated that the participants’ QOL was at the medium-high level. In addition, the mean scores for the subscales of QOL were slightly above the medium level. The highest subscale score for QOL was for sensory abilities (13.81), followed by intimacy (13.21) and (thoughts on) death and dying (12.86). The lowest domain score of QOL was social participation (11.36), followed by autonomy (12.15). The participants had medium-level scores for attitudes toward aging. The psychological loss subscale of attitudes toward aging had the highest mean score among the subscales of attitudes toward aging. In this study, the older women believed that they had experienced serious psychosocial loss. The mean overall attitudes toward aging score for the 270 participants was 76.23 ± 8.49. The theoretical maximum score for overall attitudes toward aging was 120. This indicated that the participants’ mean score for overall attitudes toward aging was at the medium-high level.
Scores and Descriptive Statistics for QOL and Attitudes Toward Aging
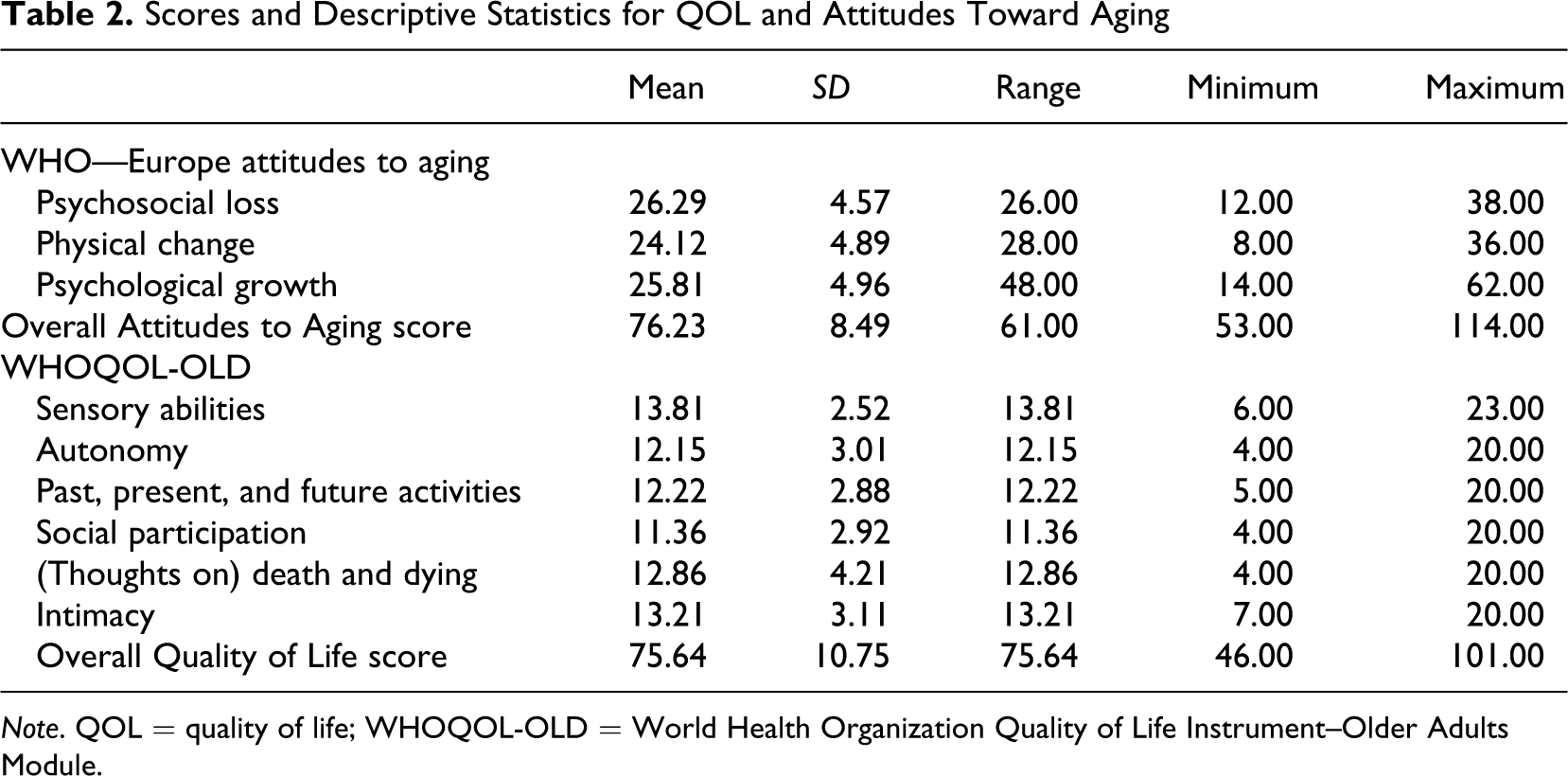
Note. QOL = quality of life; WHOQOL-OLD = World Health Organization Quality of Life Instrument–Older Adults Module.
Pearson’s correlation was used to determine whether a relationship existed among the categories and subcategories of QOL, attitudes toward aging, and physical disorder. The correlation coefficients ranged from −.012 to .729 (see Table 3). Significant correlations were found between QOL and attitudes toward aging. Negative relationships were found between physical disorder and QOL (r = −.129; p < .05). Overall QOL and overall attitudes toward aging had a significant and positive relationship (r = .382; p < .01). The sensory abilities and death and dying domains had weak relationships with the other domains, whereas the autonomy domain score was strongly correlated with all the other domains, except the death and dying domain. The psychosocial loss subcale of attitudes toward aging did not significantly affect overall QOL. However, psychosocial loss negatively affected some subscales of QOL (especially social participation). The sensory abilities and death and dying domains had weak relationships with the other domains, while the autonomy domain score was strongly correlated with all the other domains except death and dying. Hypothesis 1 was supported.
The Correlations Among QOL, Attitudes Toward Aging, and Physical Disorder
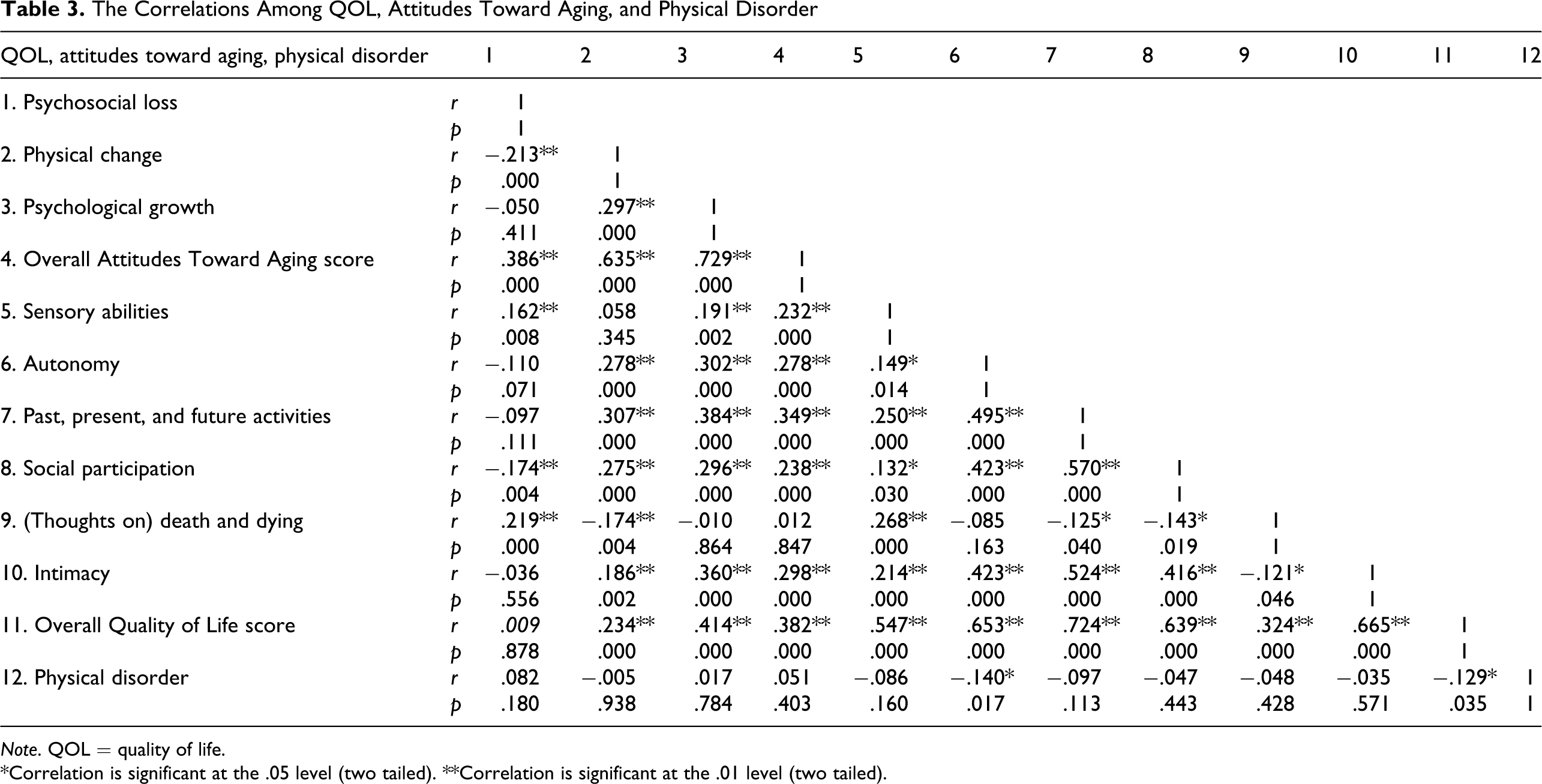
Note. QOL = quality of life.
*Correlation is significant at the .05 level (two tailed). **Correlation is significant at the .01 level (two tailed).
Table 4 shows that 17% (adjusted R 2 = .16, F = 20.505; p < .001) of the variance in the dependent variable (overall QOL) was explained by the independent variables (psychosocial loss, physical change, and psychological growth). The Durbin-Watson statistic was 1.52 (below 2.50), which did not reveal autocorrelation among residuals, confirming the suitability of using regression for analysis. Furthermore, the variance inflation factors (VIFs) were all below 10 (1.048 and 1.146), indicating the absence of multicolinearity (Hair, Anderson, Tatham, & Black, 1998). Two independent variables, physical change (β = .296; t = 2.280; p < .05) and psychological growth (β = .815; t = 6.505; p < .01), had significant effects on the dependent variable. Psychological growth was a more significant regressor of the overall QOL than the other subscales of attitudes toward aging. However, the psychosocial loss subscale of attitudes toward aging was not a significant regressor for QOL in the older women in this study. Hypothesis 2, then, was accepted for physical change and psychological growth but was rejected for psychosocial loss (see Table 4).
The Predictors of QOL
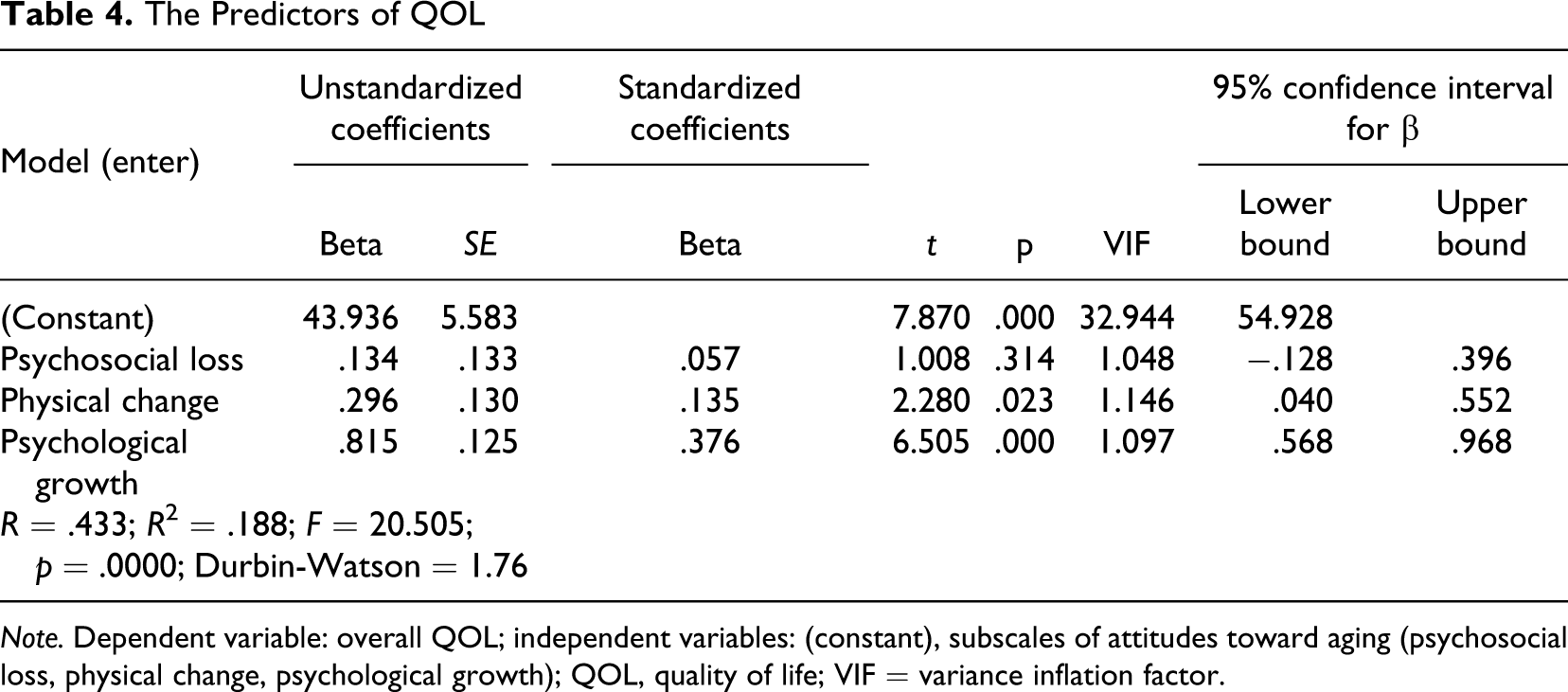
Note. Dependent variable: overall QOL; independent variables: (constant), subscales of attitudes toward aging (psychosocial loss, physical change, psychological growth); QOL, quality of life; VIF = variance inflation factor.
Table 5 shows that 11.4% (adjusted R 2 = .10, F = 4.178; p < .001) of the variance in the dependent variable (psychosocial loss) was explained by the independent variables (physical change; psychological growth; sensory abilities; autonomy; past, present, and future activities; social participation; [thoughts on] death and dying; and intimacy). The Durbin-Watson statistic was 1.68 (below 2.50), which did not reveal autocorrelation among residuals, confirming the suitability of using regression for analysis. Furthermore, the VIFs were all below 10 (minimum 1.169 and maximum 1.983), indicating the absence of multicolinearity (Hair et al., 1998). Three independent variables—physical change (β = −.150; t = −2.502; p < .05), sensory abilities (β = .265; t = 2.286; p < .05), and (thoughts on) death and dying (β = .147; t = 2.153; p < .05)—had a significant effect on the dependent variable. In this study, sensory abilities were more significant regressor of psychosocial loss than were the other independent variables. Hypothesis 3, then, was accepted for physical change, sensory abilities, and (thoughts on) death and dying but was rejected for psychological growth; autonomy; past, present, and future activities; social participation; and intimacy.
The Predictors of Psychosocial Loss
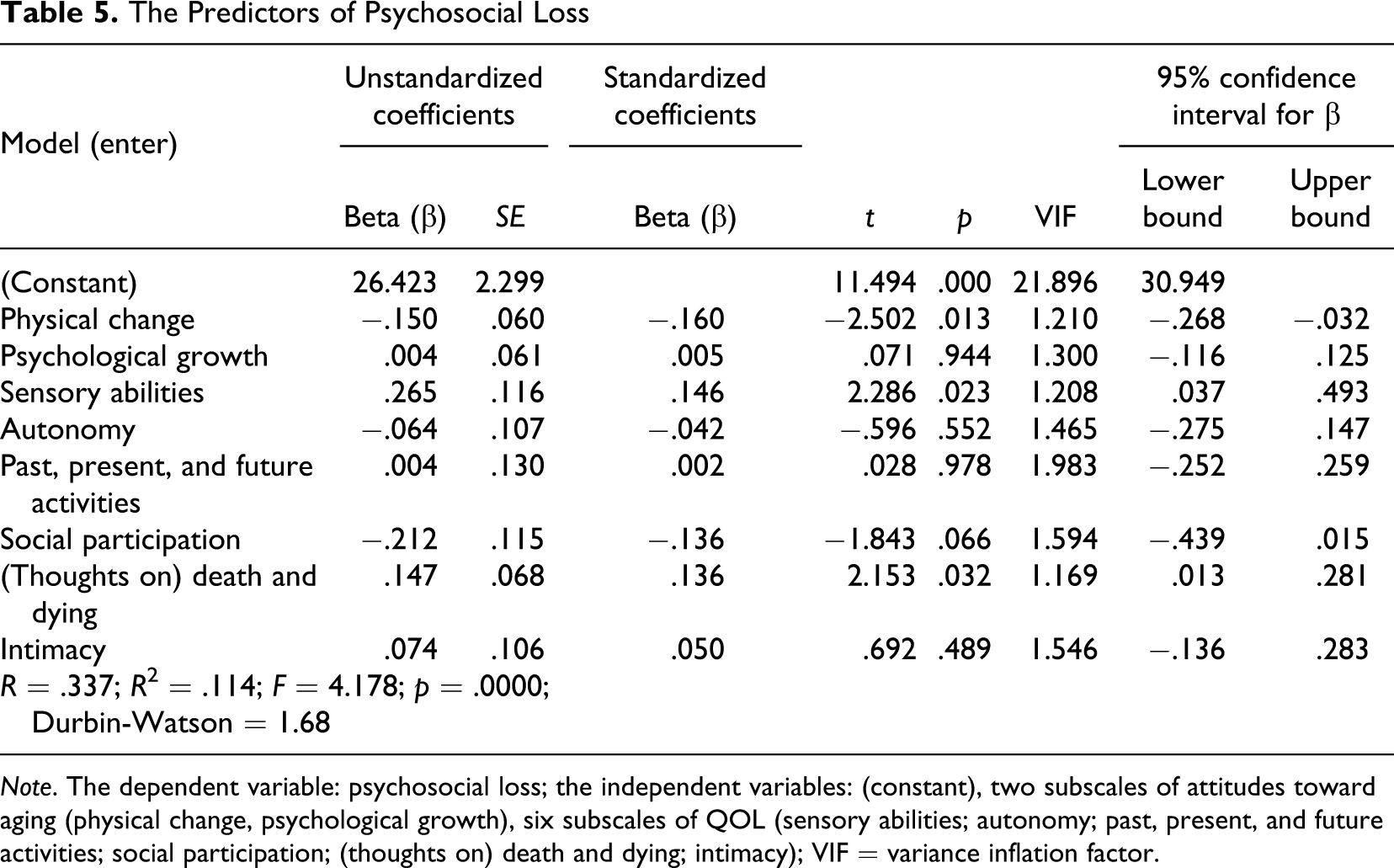
Note. The dependent variable: psychosocial loss; the independent variables: (constant), two subscales of attitudes toward aging (physical change, psychological growth), six subscales of QOL (sensory abilities; autonomy; past, present, and future activities; social participation; (thoughts on) death and dying; intimacy); VIF = variance inflation factor.
The scores for psychosocial loss, physical change, psychological growth, and overall attitudes toward aging did not change significantly in terms of the existence of happiness (p >.05). The scores for autonomy (t = 2.316); past, present, and future activities (t = 3.296); intimacy (t = 3.082); and overall QOL (t = 2.558) for the participants changed significantly in terms of the existence of happiness (p < .05). The happy participants had higher mean scores than did the unhappy participants according to autonomy; past, present, and future activities; social participation; intimacy; and overall QOL. However, the unhappy participants had higher scores for psychosocial loss, physical change, psychological growth, and overall attitudes toward aging than did the happy participants. These differences in attitudes toward aging are not statistically significant. The findings revealed that happiness significantly affects overall QOL in older women. Hypothesis 4, then, was accepted for autonomy; past, present, and future activities; intimacy; and overall QOL (see Table 6).
QOL and Attitudes Toward Aging and According to Happiness
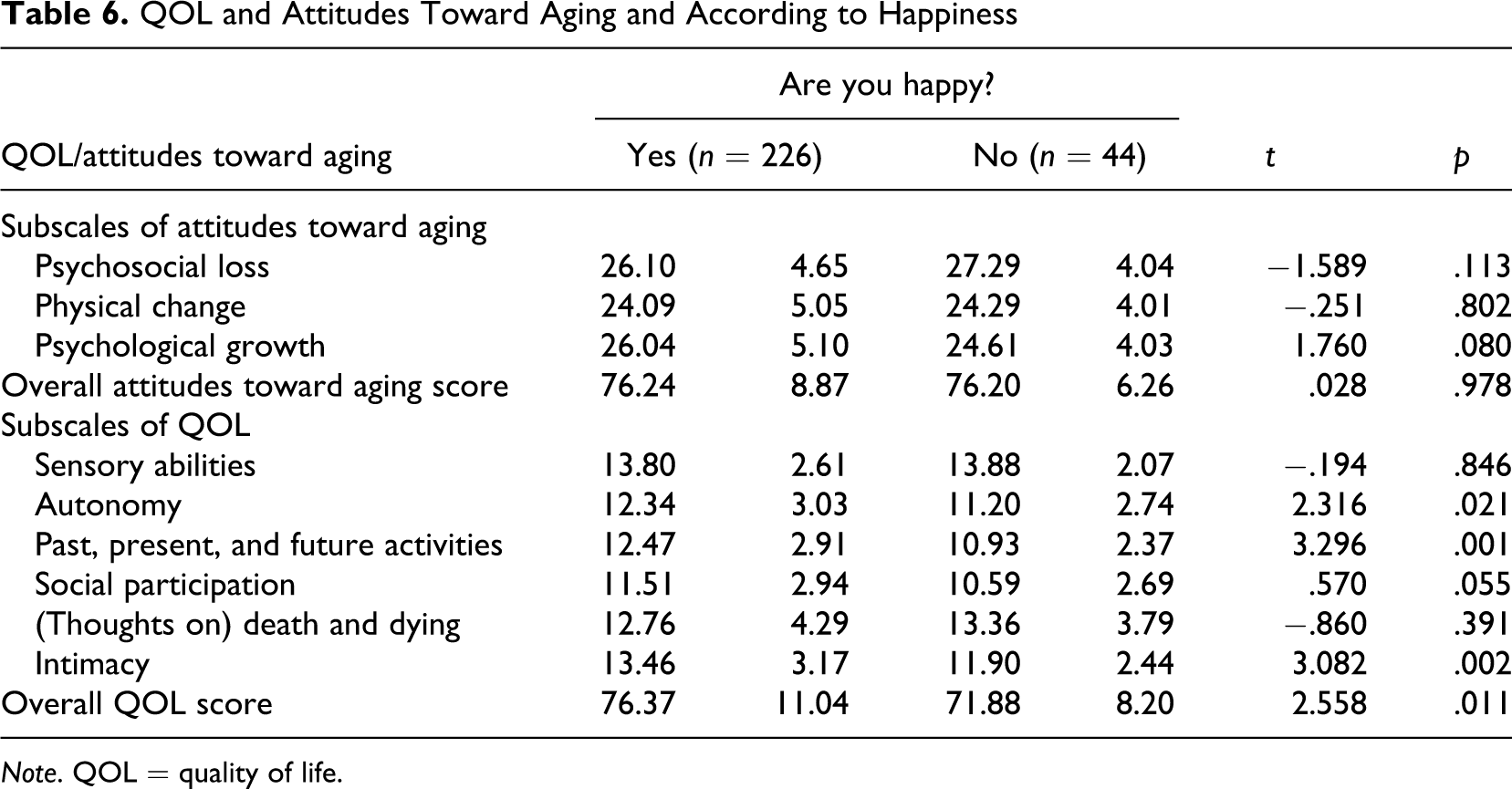
Note. QOL = quality of life.
Past, present, and future activities (t = 2.820) and social participation (t = 2.761) changed significantly in terms of literacy status (p < .05). That is, the participants who were literate had higher mean scores for overall QOL than did those who were illiterate. However, literacy status did not significantly affect overall attitudes toward aging and overall QOL. Hypothesis 5 was accepted for past, present, and future activities and for social participation (see Table 7).
QOL and Attitudes Toward Aging According to Literacy
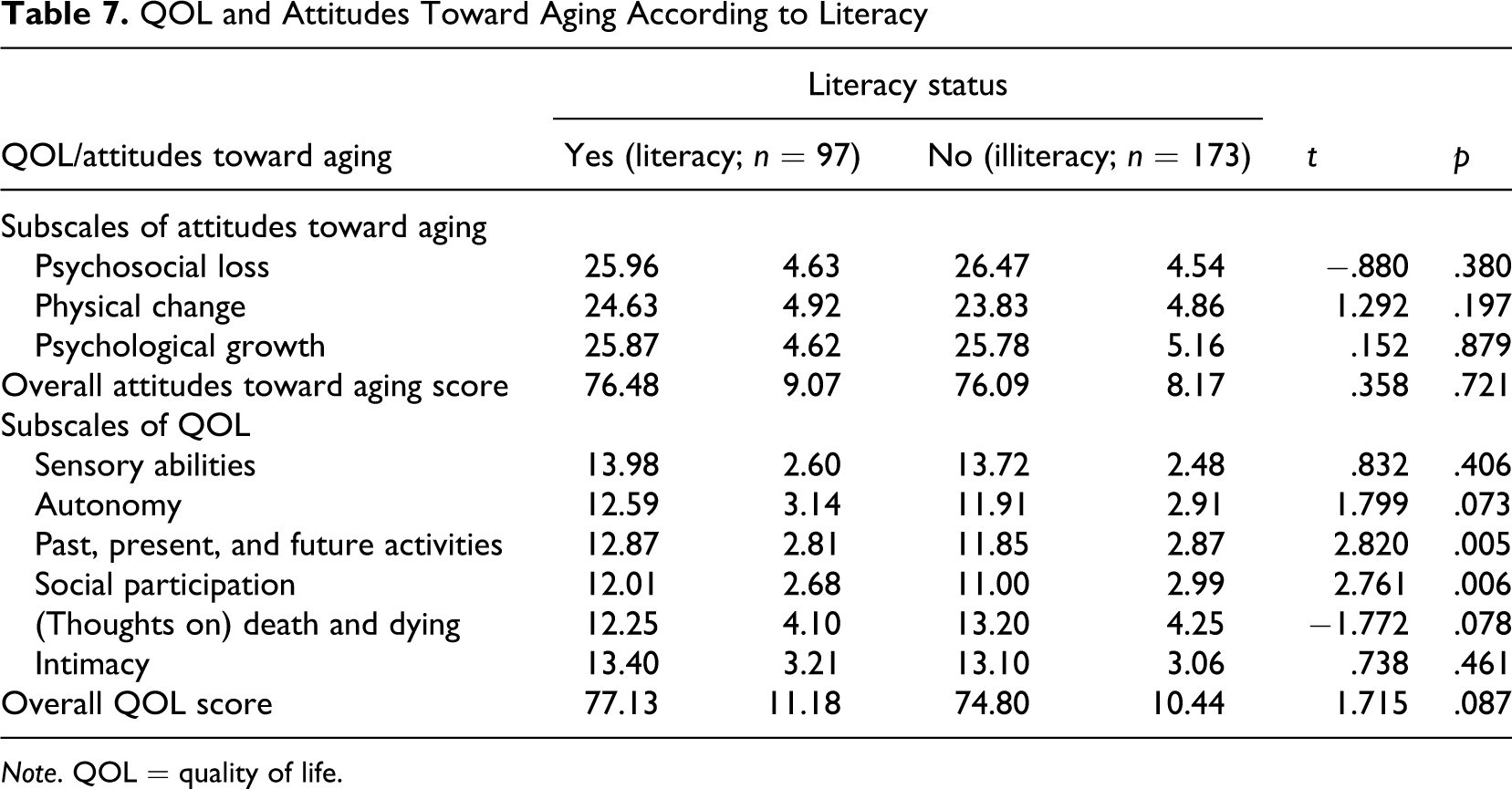
Note. QOL = quality of life.
Discussion
The results indicated that there was a significant relationship between QOL and attitudes toward aging of older Turkish women in one city of Turkey. The dimensions of attitudes toward aging (physical change and psychological growth) were significant predictors of QOL in the participants. The women had medium-level scores for attitudes toward aging. The psychological loss subscale of attitudes toward aging had the highest mean score among the subscales of attitudes toward aging; that is, the women believed that they had suffered severe psychosocial loss. These results are consistent with the results of previous studies (Eser et al., 2010) in Turkey and (Low, Molzahn, & Kalfoss, 2008) in Canada and Norway as well as in other countries (Fang et al., 2011; Shrestha, 2010). Eser et al. (2010) found out that three domains of QOL in Turkish older adults—autonomy; past, present, and future activities; and social participation—had correlation coefficients with an overall score >0.7. The sensory abilities and death and dying domains had weak relationships with the other domains, whereas the autonomy domain score was strongly correlated with those of all the other domains, except the death and dying domain (Eser et al., 2010). Kalfoss, Low, & Molzahn (2010) found that the correlations of all the subscales of WHOQOLF-OLD and WHO-AAQ were significant in the Canadian and Norwegian samples (p < .01), the lowest being between psychosocial loss and psychosocial growth for Canada (r = .363) and Norway (r = .132).
Previous studies confirmed that social interactions and independent living (autonomy) are strong determinants of health-related QOL (Borg et al., 2006; Borglin et al., 2006; Constança et al., 2003; Eser et al., 2010; Hellstrom et al., 2004). Luleci, Hey, and Subasi (2008) revealed that there was a significant difference between the QOL scores of older men and women in a nursing home in Turkey. The QOL of the women in Luleci et al.’s study might have been negatively affected by their new lifestyles. Their emotional bond with former experiences was more powerful, their memories were stronger, and their relationships with family members were greatly missed. Turkish women are very involved in all aspects of domestic life and are extremely dependant on their families. These factors may have led to a reduced QOL for Turkish women living in an assisted living facility. Relief programs and psychological interventions may improve their QOL (Bodur & Cingil, 2009; Fassino et al., 2002; Wang et al., 2000). Ng, Ballantyne, and Brenkel (2007) reported lower QOL scores before women had hip replacement surgery, although gender differences did not continue after the surgery.
QOL is related more to a personal sense of happiness and subjective life satisfaction than to objective problems, such as physical functioning (Cardona, 2010; Pinquart, 2001; Pinquart & Sorensen, 2000). Physical function/well-being and QOL in older adults have a significant correlation (r = .50; p < .01; Halvorsrud, Kalfoss, Diseth, & Kirkevold, 2012). Haas (1999) noted that QOL was usually measured with objective indicators, such as socioeconomic status, education, and housing, which accounted for only 15% of the variance in QOL compared to 50% of the variance accounted for by subjective indicators, such as happiness and life satisfaction. Molzahn and Skevington (2010) revealed that happiness was a significant regressor for overall QOL in older adults; that is, it could enhance the QOL of older adults. In addition, Altug, Yağci, Kitiş, Büker, and Cavlak (2009) reported that the QOL of older adults in Turkey is negatively affected by lower educational levels.
This article has addressed the QOL and attitudes toward aging of older women in a deprived urban area in Turkey. The QOL scores for these women were not very high. Thus, the Turkish government should take into account the importance of the subjective well-being, QOL, level of happiness, and level of education of older women in considering policies and programs in deprived areas in Turkey. The results of this study could be used to emphasize the importance of attitudes toward aging, education, happiness, and education for gaining a better understanding of the QOL of elderly Turkish women. It would also be useful to conduct comparable studies that explore aspects of the QOL of older women in different cities and nursing homes in Turkey to validate the results of the study. The results of our study suggest that QOL is a complex, multidimensional concept that should be studied at different levels of analysis in Turkey and other countries. We highlight the implications of the findings for the successful implementation of aging policy strategies with respect to individuals, families, businesses, public services, and communities.
This study had some limitations, primarily because it was conducted with older women in one city in Turkey. It was a cross-sectional one, illustrating the current predictive factors for the QOL of the participants, which may change over time and may not represent the entire population of elderly Turkish women. Other limitations of the study included the nonassessment of cognitive impairment, the use and side effects of medications, and the severity and comorbidity of diseases, all of which could have affected the results.
Future research should focus on specifying the directionality of the relationships among different domains of QOL as well as different levels of the QOL construct in older adults. Also, advanced quantitative methods, such as structural equation modeling, should be used to study the complex relationships between QOL-related factors in aging. Structural equation models, regression models, and factorial models provide an effective way of summarizing and validating research findings. In addition, QOL research may benefit the most from longitudinal studies and field research that are designed to test the causal implications of different dimensions of QOL and studying the effect of manipulating different dimension of QOL (Cardona, 2010).
A broader perspective on QOL is important for multisector policy evaluation and for gaining a better understanding of and enhancing QOL in later life (Bowling, 2007). The WHOQOL-OLD module and WHO Europe Attitudes toward Aging Questionnaire could provide researchers, clinicians, and policy makers with unique scales to measure the impact of successful interventions. They also provide a vehicle for measuring how individuals age across cultures and under different economic, political, and social circumstances. However, the field of QOL; attitudes toward aging; and happiness of older adults, especially women, require much more research, discussion, and methodological sophistication and, ultimately, more common sense in Turkey and other countries. Finally, the results of the study emphasize the importance of QOL in older adults who are living in their own homes in Turkey and the attitudes toward aging of nursing home residents in Turkey.
An understanding of the attitudes and QOL of older adults in Turkey and developing countries could assist policy makers in planning programs that are meaningful to older adults, contribute to their psychological growth, minimize their physical decline, and reduce their perceptions of psychological loss (Kalfoss et al., 2010; Tate, Leedline, & Cuddy, 2003). Attitudes also influence decisions that have an impact on health-promoting behaviors, as suggested in the WHO Active Ageing Policy Framework (WHO, 2002).
The aging of the population is one of the most important demographic facts that has come to the foreground in the 21st century. In the whole world, people live longer, birth rates decrease, and consequently the elderly population increases both numerically and pro rata. The aging of the population affects all facets of a society, including health, social security, environment-related issues, education, business opportunities, sociocultural activities, and family life. In Turkey, the State Planning Organization (2007, p. 1) declared that “policies and programs in Turkey on ageing focus on increasing the quality of life and health in general.”
Turkey is a society that looks after its elderly people with their traditions and customs. The large majority of elderly persons live with their children; the ones who live apart are in close contact. Because of this culture of harmony, family is important in elderly people’s problem solving. In hospitals, other than general health services, geriatric services are not sufficient to provide the help and special care that elderly people need to preserve their health.
An important goal for health systems and social services is to improve the QOL elderly men and women. It is therefore important to determine and analyze the factors that influence the QOL in these populations (Halvorsrud et al., 2012). However debate still continues on which dimensions of QOL are important to older adults (Bowling et al., 2003; Haywood, Garratt, Schmidt, Mackintosh, & Fitspatrick, 2004; Molzahn, Kalfoss, Makaroff, & Skevington, 2011). Relatively little research has been conducted on the QOL of older women across cultures and countries. The majority of recent QOL studies with older adults has focused on the validation of instruments and/or cultural adaptation (Paskulin & Molzahn, 2007). WHO (1998) suggested that populations in developing countries will become elderly before they become rich, while those in industrialized countries will become rich before they become elderly, emphasizing that all countries in the world need to be prepared to address the QOL, happiness, well-being, and health-related QOL of their aging populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.