Abstract
A growing number of programs promoted by planners and others have aimed to foster communities that support older people. Do such programs make a substantial difference? Through a scoping review of research evaluating WHO-style age-friendly community initiatives (AFCIs), we investigate what kind of outcomes such initiatives have achieved and factors facilitating or hindering them. Elements affecting implementation varied by geographies. They included external resources (e.g., government support, funding, consultants), local resources (e.g., community size, demographics, staff, infrastructure), engaged local participants (e.g., partnerships, champions, older people), and effective strategies to build support (e.g., quick wins, awareness building, cultural sensitivity).
Keywords
Introduction
The world's population is aging and with that comes a need to make places that can better support older people (United Nations 2019). Over the past decades, multiple organizations have developed models and published guides to stimulate creating age-friendly cities and communities, such as Livable Communities by the AARP (formerly the American Association of Retired Persons), the AdvantAge Initiative by New York Visiting Nurses Association, Healthy Communities for Active Aging by the US Environmental Protection Agency, and the Global Age-Friendly Cities by the World Health Organization (WHO) (Glicksman et al. 2014; Gonyea and Hudson 2015; Winick and Jaffe 2015). 1 Among these models, the WHO age-friendly community approach, typically focusing on eight domains, has been widely used in practice in part because it has been adopted in many countries (World Health Organization n.d.). Its eight domains include outdoor spaces and buildings, transportation, housing, social participation, respect and social inclusion, civic participation and employment, communication and information, and community support and health services (World Health Organization 2007).
This paper synthesizes research evaluating such age-friendly community initiatives (AFCIs) to answer the question: do AFCIs work? More specifically, have they produced positive outcomes and what factors helped or hindered these outcomes? This matters for planners as these programs provide important models for creating comprehensively age-friendly communities that bring expertise from a variety of partners to the endeavor (Winick and Jaffe 2015). They are also important examples of cross-sectoral and community engagement used in planning and their lessons can be important to planning more generally, for example in planning for healthy communities or climate action planning.
Assessing AFCI effectiveness has been more complex than it might seem, however (Torku, Chan and Yung 2021; Steels 2015). Relatively few studies have gone beyond describing what various AFCI programs do and drawing some lessons (Greenfield et al. 2015). The programs themselves are hard to compare as they vary by the scale of implementation (e.g., district, city, metropolitan area) and the region of the world. Further, existing studies emphasize different topical issues. Even where there are evaluations, they tend to focus on the initial process of implementing an AFCI project and early outputs like reports and events rather than longer-term outcomes such as improved health well-being, or quality of life (Torku, Chan and Yung 2021; Steels 2015).
In this paper, we address those AFCIs using versions of the widely applied WHO age-friendly model or framework. Many AFCIs start by assessing the age-friendliness of places as part of a needs assessment. The focus of this review, however, is on synthesizing evaluations of outcomes of comprehensive programs designed to promote age-friendliness. We first define the inputs, outputs, and outcomes of an AFCI program, then examine outcomes AFCIs have achieved. Those that are more effective tend to have more resources (political, funding, technical, infrastructural, locational, social), engaged participants (collaborators, leaders, champions, and older people themselves), and use effective strategies to build support (quick wins, awareness raising, and cultural sensitivity). We also pay attention to the uniqueness of AFCI implementation in different geographic and economic settings, a key interest for planners. The WHO Age-Friendly Communities program has been around for much more than a decade, and at this stage, more rigorous and diverse evaluations are needed to build the knowledge base.
Background
What Is an Age-Friendly City or Community Initiative?
The WHO defines an age-friendly city as a place that “encourages active aging by optimizing opportunities for health, participation, and security in order to enhance quality of life as people age” (World Health Organization 2007, 1). Similarly, drawing from an ecological perspective, Alley et al. (2007, 4) define an “elder-friendly community” as “a place where older people are actively involved, valued, and supported with infrastructure and services that effectively accommodate their needs.” More recently, AARP, formerly the American Association of Retired Persons, has focused on livable communities with intergenerational links to “allow residents to age in place…[where] people of all ages can … make their city, town, or neighborhood a lifelong home” (Binette 2018).
As programs, AFCIs are “deliberate and distinct efforts across stakeholders from multiple sectors within a defined and typically local geographical area to make social and/or physical environments more conducive to older adults’ health, well-being, and ability to age in place and in the community” (Greenfield et al. 2015, 192). Communities represent geographical settlements at any scale—cities, regions, towns, or villages (Menec et al. 2011). As well as the WHO program, Lifetime Neighborhood in UK and AARP Livable Communities in the United States take a similar approach, integrating the physical and social environments typically using a model of collaborative governance and bottom-up participation, though they structured the physical and social domains differently (Lui et al. 2009).
To be classed as AFCIs in this review, then, programs did not need to be officially part of the WHO AFC network. However, as we describe later, they did need to share certain features including commitment to improving age-friendliness in multiple domains and largely as defined by the WHO, along with partnerships among multiple stakeholders. In this sense, programs were not AFCIs if they did not target age-friendliness, if they focused on one domain rather than overall age-friendliness, and if served by one single organization.
Histories of WHO AFCs
In 2006, the WHO accelerated age-friendly efforts by initiating a bottom-up participatory project to investigate features of age-friendliness, as conceived at the World Congress of Gerontology and Geriatrics in Brazil in 2005 (World Health Organization 2007; Neal and DeLaTorre 2009). Built on the WHO's Active Aging framework and other existing age-friendly approaches, the WHO developed a more comprehensive framework covering the eight domains of age-friendliness (World Health Organization 2007). The Public Health Agency of Canada funded the WHO to conduct a worldwide consultation with older people under this framework (Plouffe et al. 2013). Facilitated by the Ministry of Health in British Columbia and in collaboration with governments, researchers, and non-governmental organizations (NGOs) around the world, the WHO led focus group research with older people and caregivers in 33 cities in 22 countries, covering both urban and rural, developed and less developed, areas in 2006–2007 (Neal and DeLaTorre 2009; World Health Organization 2007).
Based on this work, in 2007 the WHO published Global Age-friendly Cities: A Guide, aiming to help cities to identify how to become more age-friendly (World Health Organization 2007). In 2010, the WHO established its Global Network for Age-friendly Cities and Communities. Since then, over 1,000 cities and communities in more than 40 countries have joined this network (World Health Organization n.d.). Individual countries have also promoted the concept, for example, the Canadian government produced an early guide for AFCIs in rural and remote areas (Gallagher, Menec and Keefe 2006).
Research on Age-Friendly Community Initiatives and Contexts
In parallel to the age-friendly movement is a small but significant field of academic research on AFCIs. One part of that literature is focused on defining and categorizing AFCIs. Some studies have drawn on theory to review elements of AFCIs, identifying key elements of AFCIs, describing examples, and proposing broad challenges (e.g., Fitzgerald and Caro 2014; Jeste et al. 2016; Buffel and Phillipson 2016). For example, Menec et al. (2011) conceptualized AFCIs based on the WHO framework and ecological theory. Both Lui et al. (2009) and Steels (2015) reviewed key features of AFCIs defined by different AFCI models and frameworks such as WHO Active Ageing or AdvantAge. Greenfield et al. (2015) conceptualized AFCIs regarding what they are, how they work, who they involve, in what geographic scale, with what rationales, and using which approaches.
Other work has addressed how to measure the age-friendliness of places. Such measurement is typically a first stage in creating an initiative but can also be done to assess the general state of age friendliness of an area in terms of physical, social, and organizational dimensions (Lehning 2014; Plouffe, Kalache and Voelcker 2015; Orpana et al. 2016; Buckner et al. 2019; Torku, Chan and Yung 2021; Xiang et al. 2021; Dabelko-Schoeny et al. 2020; Zhang, Warner and Wethington 2020; Brossoie et al. 2022).
Another body of work addresses general planning and policy-making for age-friendliness often using literature reviews or large surveys to examine what has been done or what could be proposed (Keating, Eales and Phillips 2013; Warner and Rukus 2013; American Planning Association 2014; Warner, Homsy and Morken 2017; Warner, Xu and Morken 2017; Zhang, Warner and Firestone 2019; Forsyth, Molinsky and Kan 2019; Keyes and Benavides 2019; Warner and Zhang 2021). Such work has both drawn on and contributed to debates about the wide range of approaches to age-friendliness and ideas for innovations. While not specifically about comprehensive initiatives, work on age-friendly places, and general planning and policy making, provided useful background for this paper when considering the types of outcomes AFCIs might create.
Assessing Age-Friendly Community Initiatives—Evaluation Issues
While substantial attention has focused on assessing places and general policy making, much less has addressed age-friendly initiative effectiveness, perhaps due to the complexity of outcomes and the different ways AFCIs benefit individuals and communities (Greenfield et al. 2015). Those assessment tools have often focused on the initial process of implementation. Among the process evaluation tools, AARP released a manual that defined AFCI program inputs, outputs, and outcomes, providing step-by-step guidance (Neal and Wernher 2014). To facilitate establishing baselines and monitoring progress, WHO released a guide to core indicators of age-friendliness (World Health Organization 2015). In addition, the Public Health Agency of Canada published a guide on AFCI evaluation (Public Health Agency of Canada 2015).
In assessing AFCIs, the line between inputs, outputs, and outcomes of such initiatives is not always clear, however. The AARP evaluation guide defines inputs as “resources that are put into a program or factors that facilitate its success.” Outputs include the “type and amount of program-related activities.” Outcomes are “changes, or results, that are hoped to be achieved through program activities” (Neal and Wernher 2014, 3; also refer to World Health Organization 2015, 12–13). For example, involving older people is often an input, but an initiative may also have an aim to involve older people, so the number involved may be an output or short-term outcome (Neal and Wernher 2014, 5).
Our focus on outcomes included long-term outcomes like improved health and short- and medium-term outcomes like completing an age-friendly urban plan, increasing participation, or improving walkability (Neal and Wernher 2014, 5). This raises some issues. For example, is helping shape an urban, city, or town plan an output (a program activity) or a short-term outcome (a change or result)? The line between outputs and short-term outcomes can be challenging to identify so we erred on the side of inclusion. For example, we consider developing an ordinance as a short-term outcome, providing an ongoing governmental framework for actions. Another tricky issue was deciding whether sustaining an AFCI in itself is an outcome. We suggest it is a short-term outcome. Finally, most AFCIs ultimately aimed to improve health and well-being but measured these long-term outcomes, presumably due to a lack of resources and difficulties disentangling the outcomes of an AFCI from other initiatives and trends (Table 1).
Examples of Outcomes and Other Activities for Age-Friendly Community Initiatives.
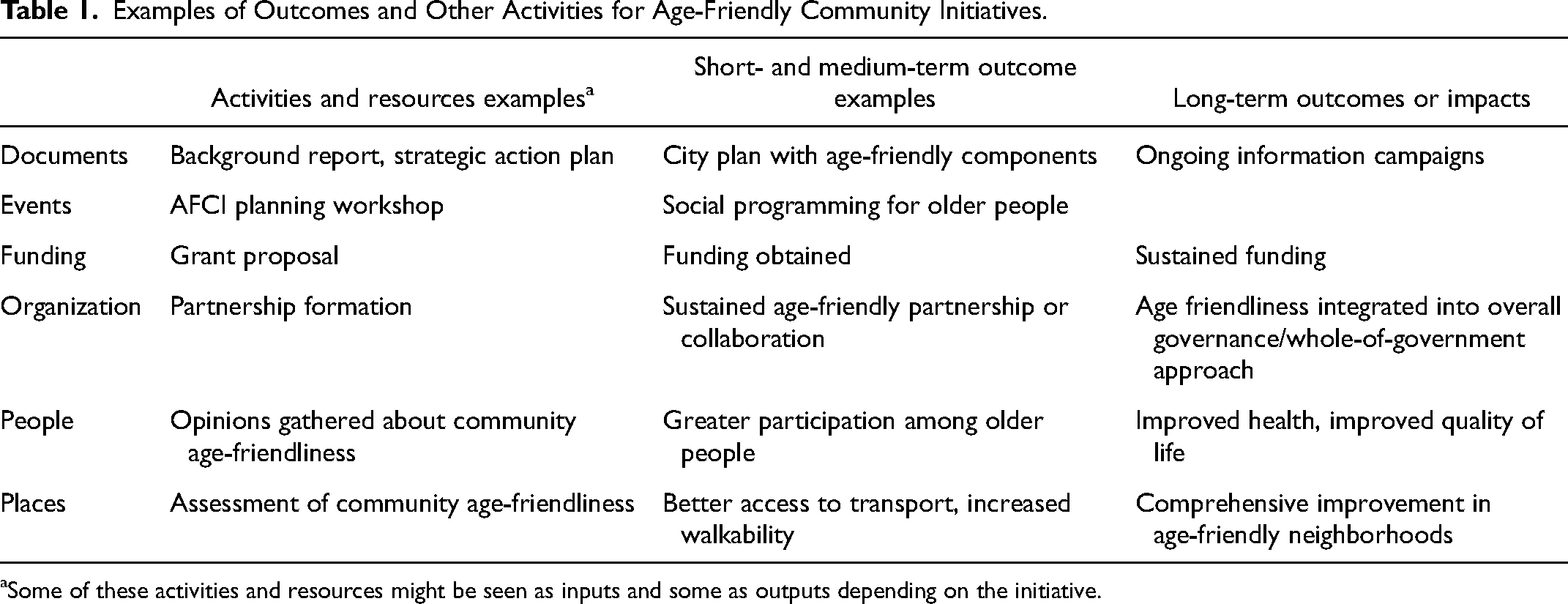
Some of these activities and resources might be seen as inputs and some as outputs depending on the initiative.
Several earlier reviews have attempted to summarize existing assessments of AFCI practices. Based on 13 studies of AFCI cases, Menec and Brown (2018) identified common facilitators and barriers including (1) elements that enabled forming AFCIs such as leadership and partnerships; (2) factors that influenced process such as funding and resources, integrating with other initiatives, and raising awareness; and (3) contexts that affected implementation, for example, supportive government, rural or urban settings, and fiscal factors. Their review covered both formation and implementation, though it did not focus on effectiveness in achieving outcomes.
Some reviews have explored multiple stages, including outcomes of AFCIs. Lehning and Greenfield (2017) examined conceptual and empirical knowledge regarding AFCIs’ activities (e.g., process of community change), outputs (e.g., community change), and outcomes (e.g., change in health and well-being of older adults). However, they mostly addressed conceptual knowledge because the existing empirical research on the evaluation of outputs and outcomes was rare (Lehning and Greenfield 2017). Reviewing the international literature, Lui et al. (2009) also found limited documentation evaluating AFCI approaches and outcomes. Similarly, Jeste et al. (2016) pointed out that a lack of evaluation was a major problem in understanding whether AFCIs work. Montayre et al. (2022) did not find any substantial evaluations of branded age-friendly interventions in rural and remote communities; they did find many narrow assessments of single interventions such as health education or exercise promotion.
Our work built on these earlier reviews, extending them by focusing on relatively detailed studies of AFCI outcomes and allowing some assessment of AFCI effectiveness. We investigated what kind of outcomes AFCIs have achieved and factors facilitating or hindering them, using an urban planning and policy lens to draw lessons for practice.
Of course, a large number of AFCI progress reports are available on municipal websites or the WHO website (e.g., NYC and The New York Academy of Medicine 2011; Innovations in Aging Collaborative and Age-Friendly Colorado Springs 2018). These reports, often written for funding bodies, typically describe the strategies and/or actions of the AFCI initiatives and their current status. However, in this paper, we review documents that are either peer-reviewed or by scholarly third-party evaluators. Such publications mean to contribute to knowledge rather than promote a program, typically involving more in-depth analysis of AFCI practices.
Methods
Review Methods
Given the emerging literature on AFCI program evaluation is highly diverse in terms of research questions, methods, and types of publications, we searched widely in academic research (e.g., journal articles, reports, book chapters, dissertations) that dealt with outcomes of AFCI programs. We used a form of scoping review methodology to map the evidence on how AFCIs work and identify the gaps where more research is needed (Munn et al. 2018). Scoping reviews identify the range and types of evidence and map them to identify knowledge gaps. They deal with broader issues than systematic reviews and do not need to address study quality, while still being structured (Booth, Papaioannou and Sutton 2012). Our protocol included clarifying search approaches and inclusion criteria, using multiple reviewers to reduce errors, and charting information and data from the reviewed studies in a structured way (Tricco et al. 2018; Munn et al. 2018). Though scoping reviews do not address the quality of included articles, we examined the study designs. The study design of each reviewed document, including research question and data collection methods, was reviewed by one author and checked by the other (Munn et al. 2018; Tricco et al. 2018). The complete list of included studies is in Appendix 1.
Search Strategy
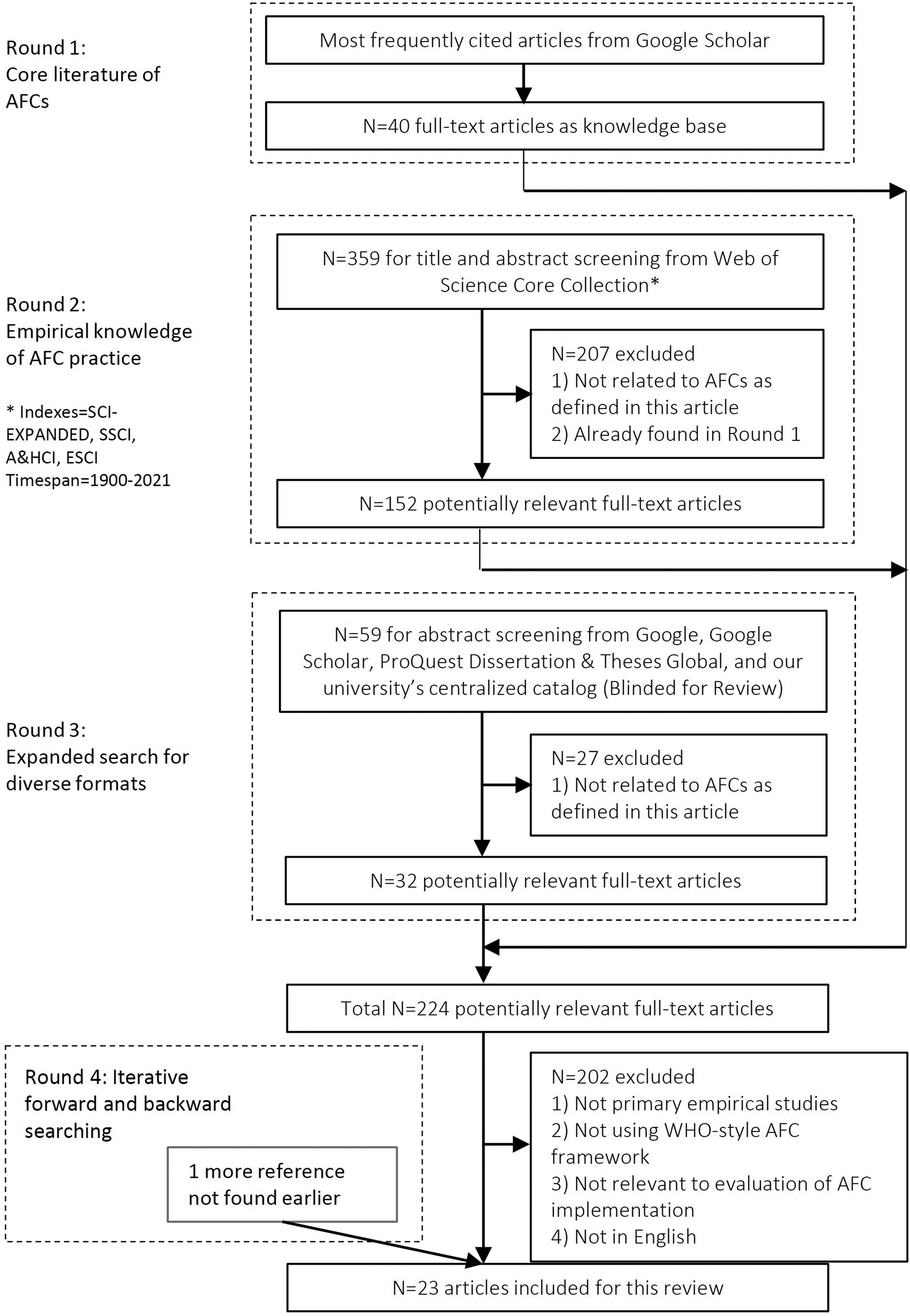
We took multiple approaches to searching the literature using diverse digital databases and forward and backward searches from identified materials. An exploratory search was performed using Google Scholar in March 2021 to identify 40 frequently cited documents on AFCI topics using key words ‘Age-friendly’ AND (‘evaluation’ OR ‘survey’ OR ‘review’). Informed by those documents, we then searched for more detailed topics in Web of Science using a variety of search terms (May 2021). 2 We then attempted to go beyond Web of Science using Google, Google Scholar, ProQuest Dissertation & Theses Global, and our university's centralized catalog, HOLLIS (https://hollis.harvard.edu/). To break beyond key words, we also searched for materials cited in documents we located and searched forward to those citing key references. We updated the forward and backward review in 2022 including articles published online up to 2021 (some were published in paper in 2022). We ultimately included 23 articles in our main listing (Appendix 2).
Inclusion/Exclusion Criteria
All the documents obtained for full-text review were examined by both authors independently. We used the following inclusion criteria: (1) primary empirical studies; (2) focused on AFCIs using something akin to the WHO AFCI framework for neighborhoods, cities, and regions looking at multiple dimensions; (3) examining AFCI implementation after needs assessment and early implementation, involving outcomes; (4) addressing places in context, and (5) in the English language. The included studies cover a range of AFCIs of diverse scales from different countries, though concentrated in North America, Australasia, and Europe (see Appendix 1).
We had several dilemmas when assessing whether to include papers. One issue was assessments of failures documenting a lack of outcomes; we included some that more clearly addressed this issue of outcomes. Some age-friendly programs focused on systems and individual facilities, such as home care systems or aged care facilities, and these were not included. As noted above, evaluations of general age friendliness unrelated to an AFCI were also not included. Large surveys of professionals working in the field were helpful background but not the focus of this review.
Covering programs with multiple dimensions relevant to planners, the best of the included studies provides rich qualitative or (sometimes) quantitative evidence. Most used standard evaluation methods from policy, planning, and public health drawing on interviews, surveys, document analysis, and readily available indicators. Evaluations varied in quality, however—reflecting the resource constraints inherent in implementing innovative projects on modest budgets. Some were based on small numbers of interviews, short time periods, and few research designs had controls. We were not sure about the level of review in the dissertations, chapters, the report, and one journal article with a fast acceptance time. We have indicated these issues in Appendix 1 and taken them into account in our analysis.
Ultimately, the 23 key documents included for the review included 18 journal articles, two book chapters, two dissertations, and one report. We also highlight two other issues in Appendix 1. Eight of the 23 documents focused more on the lessons learned from implementation, briefly mentioning outcomes. We have indicated them with an asterisk. These were helpful papers that might not have been included with more stringent inclusion criteria. In addition, only four documents included substantial direct evidence obtained from older people themselves. Rather, most relied on information from AFCI committee members and staff.
Analysis
As a scoping review, we mapped out what is known about the effectiveness of AFCIs, where more research is needed, as well as implications for practice. As noted earlier, short- and medium-term outcomes include such phenomena as implemented urban plans, increased walkability, better access to transport, greater participation in neighborhood events among older people, and improved community understanding of the value of older adults. Long-term outcome examples include improved health and quality of life of individuals (Neal and Wernher 2014). As shown in Appendix 1, we extracted outcomes from the included studies.
W
Factors Supporting or Hindering Implementing Age-Friendly Community Initiatives.
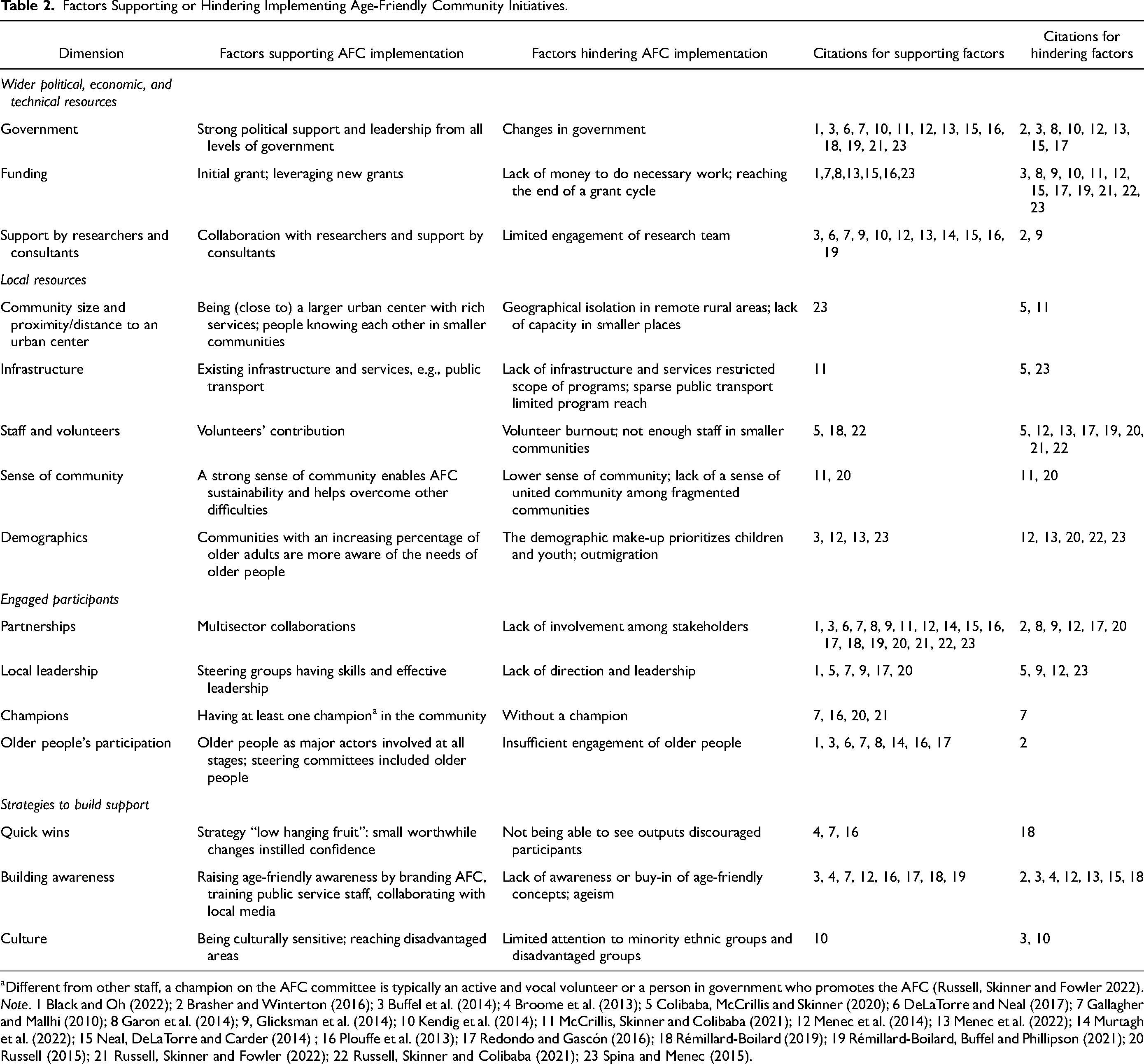
Different from other staff, a champion on the AFC committee is typically an active and vocal volunteer or a person in government who promotes the AFC (Russell, Skinner and Fowler 2022).
Note. 1 Black and Oh (2022); 2 Brasher and Winterton (2016); 3 Buffel et al. (2014); 4 Broome et al. (2013); 5 Colibaba, McCrillis and Skinner (2020); 6 DeLaTorre and Neal (2017); 7 Gallagher and Mallhi (2010); 8 Garon et al. (2014); 9, Glicksman et al. (2014); 10 Kendig et al. (2014); 11 McCrillis, Skinner and Colibaba (2021); 12 Menec et al. (2014); 13 Menec et al. (2022); 14 Murtagh et al. (2022); 15 Neal, DeLaTorre and Carder (2014) ; 16 Plouffe et al. (2013); 17 Redondo and Gascón (2016); 18 Rémillard-Boilard (2019); 19 Rémillard-Boilard, Buffel and Phillipson (2021); 20 Russell (2015); 21 Russell, Skinner and Fowler (2022); 22 Russell, Skinner and Colibaba (2021); 23 Spina and Menec (2015).
Limitations
We have already discussed difficulties defining outcomes as well as differences in the research methods of reviewed papers. Some papers with richer lessons had weaker outcome measures. While some papers compared different initiatives, few had controls comparing places with and without initiatives. Given the high level of convergence in terms of the findings of all the articles, we are, however, confident in the overall direction of the results.
Do AFCIs Achieve Positive Outcomes?
Not All AFCIs Thrive Enough to Have Outcomes
Many AFCI programs have struggled to have meaningful achievements, even in terms of sustaining ongoing partnerships (Menec et al. 2022; Neville et al. 2021). For example, Menec et al. (2022) explored AFCI sustainability in Manitoba, Canada, finding that seven of the 52 investigated AFCIs were fully sustainable, with an active committee and strong champions, while the other 45 AFCIs were in hiatus, reorganized, or never got off the ground. Russell, Skinner, and Colibaba (2021) interviewed 11 informants from 11 rural AFCIs in the Newfoundland and Labrador Provinces, Canada, among which eight were likely to become sustainable and three were about to cease operations. Representatives of 10 more eligible AFCIs were not available likely because they had been dissolved.
Outcomes of AFCIs—Short-Term
AFCIs that have been studied in the literature have documented a variety of short-term outcomes. Collaborative partnerships are regarded as an essential step, and a potential outcome, leading to the long-term sustainability of AFCIs (e.g., Russell, Skinner and Colibaba 2021). Garon et al. (2014) compared two AFCIs in a pilot project in Quebec, Canada, drawing on focus groups, surveys, log books, and other documents over four years. One case led by a group of older-adult associations was less effective in institutionalizing age-friendly approaches than another where the steering committee collaborated across sectors with strong municipal representation and consultation with older people. Among the 44 rural and urban AFCIs in Manitoba, Canada, studied by Menec et al. (2014), leaders from about half of the AFCIs had developed new collaborations and partnerships with organizations such as local businesses, senior centers, schools, and other governmental and NGOs. These partnerships helped to establish capacity, promote awareness about the AFCIs, execute age-friendly projects, and facilitate access to public spaces (Menec et al. 2014). Smaller communities, however, can lack the capacity to leverage new partnerships (Menec et al. 2014).
Though AFCIs are often supported and guided by higher level policies, AFCI implementation can also produce new local policies and detailed action plans, leading to activities that benefit older people and prepare for and sustain new age-friendly projects. For example, the AFCI initiative of Portland and Multnomah County (Oregon, US) contributed to long-term city plans and policies related to housing, transportation, urban form, and design and development (DeLaTorre and Neal 2017). Murtagh et al. (2022) described Belfast's AFCI creating datasets and indicators that shaped debates and influenced various urban plans. Glicksman et al. (2014) documented how Philadelphia adopted a more age-friendly accessory dwelling unit ordinance.
Outcomes of AFCIs—Ongoing Programs and Completed Projects
Ongoing programs and completed projects can improve age-friendliness of multiple domains such as outdoor spaces, transportation, social inclusion, health service, and access to local business (e.g., Neville et al. 2018; Russell 2015; Plouffe et al. 2013). Among the 44 rural and urban AFCIs studied by Menec et al. (2014) in Manitoba, Canada, 77% had implemented one or more new projects by the time of research, tackling issues in outdoor spaces and buildings, social participation, and communication. However, these AFCIs were less successful in implementing projects to address transportation, housing, and community support. In addition, 45% of these AFCIs managed events and activities to promote awareness of age-friendliness. The AFCI of Manchester used many “age-friendly demonstrator” sites to promote age-friendly outdoor spaces and buildings, though how well they worked was not yet clear (Buffel et al. 2014, 66). Similarly, in British Columbia, 80% of 30 AFCIs studied reported undertaking local actions on identified priorities (Gallagher and Mallhi 2010). Studies indicated that programs in rural AFCIs mostly focused on social and recreational activities that required fewer resources (Colibaba, McCrillis and Skinner 2020; Russell, Skinner and Colibaba 2021).
Outcomes of AFCIs—Medium and Longer Term
A limited number of studies have investigated the medium-term outcomes of AFCI implementation, such as providing more age-friendly outdoor space or improving perceptions of aging (Broome et al. 2013; Plouffe et al. 2013; Redondo and Gascón 2016; Rémillard-Boilard, Buffel and Phillipson 2021). Broome et al. (2013) evaluated how the AFCI in Hervey Bay, Queensland, Australia, influenced bus usage and social participation. They used Brisbane, with no AFCI intervention, as a control site. They conducted satisfaction surveys with older bus users (n = 335) and a repeated measures cohort study with older residents (n = 100) in both sites immediately before and after the 2-year intervention. They found that AFCI implementation in Hervey Bay improved satisfaction and perceived usability of the bus system and helped maintain the level of bus use and social activities among older people. In contrast, bus use and social activities declined in the Brisbane sample. Murtagh et al. (2022) reported on surveys cited by Age-Friendly Belfast showing improvement in physical activity, park access, safety, volunteering, and other factors over the period of their first plan from 2014 to 2017. It was not clear how much was directly due to the initiative, but the trends were all positive.
Some have documented AFCI outcomes qualitatively. In AFCIs in Quebec, Canada, implementation teams observed positive outcomes such as increased sense of belonging, greater older people's participation in recreational activities, and stronger awareness of older people's needs among local services and politicians (Plouffe et al. 2013). The city of La Plata, Argentina, assessed AFCI actions in 2013. Results based on focus groups with 95 people showed age-friendly improvements had been implemented in outdoor spaces, public transport, and safety from traffic and crime (Redondo and Gascón 2016). Rémillard-Boilard, Buffel and Phillipson (2021) studied 11 AFCIs at the city level from 11 countries based on questionnaires (N = 11), interviews (N = 5), and document reviews. The AFCI representatives reported varying outcomes including improved services for older people, communities becoming overall better place to age, more positive images of aging, and increased awareness of older people's views and needs.
Finally, a few studies have examined broader outcomes of AFCIs, such as improved older people's physical, mental, and social health and quality of life. Russell (2015) conducted interviews and focus groups with 35 committee members and 43 older residents from 11 AFCIs in Newfoundland and Labrador, Canada, evaluating the impacts of AFCI implementation through one-time grants. Findings were mixed. On one hand, respondents described increased respect for older people, sense of community, and improved health through recreational and social activities designed to increase fitness and healthy eating. These social programs also ameliorated isolation and loneliness, providing new social support resources. However, due to resource constraints, the programs could reach only a small number of people and did “little to reduce the experience of being stuck in place” (Russell, Skinner and Colibaba 2021, 222; Murtagh et al. 2022).
Evaluation Methods
As discussed above, evaluations of AFCI effectiveness have often simply assessed whether or not partnerships were established and projects executed relying on committee member and older resident interviews. We had expected more diverse evaluation methods. As guided by WHO, the evaluation of AFCI progress could be done by comparing indicators of multiple domains before and after the implementation period (World Health Organization 2015). However, only Murtagh et al. (2022, 67) cited such work, and it came from “different surveys with a range of populations, participants, and methods.” More pre-post intervention studies could contribute to the evidence of the AFCI effectiveness (e.g., Broome et al. 2013).
Whose Perspectives?
Most survey-based studies explored the perspectives of AFCI committee members or government officials, while four investigated the viewpoints of older residents (Appendix 1). Other studies drew on progress reports, action reports, minutes, and public documents, which also generally represented perspectives of the AFCI committees or local governments (e.g., Kendig et al. 2014). Though all the results were generally positive if mixed, the results from the committee members were often more optimistic than those from older residents (Colibaba, McCrillis and Skinner 2020; McCrillis, Skinner and Colibaba 2021).
Why Did Some AFCIs Achieve More Than Others?
Common Factors That Supported or Hindered Implementing AFCIs
While AFCI programs are diverse, there have been some common factors that have contributed to the making of more age-friendly communities and vice versa. Our findings on common facilitators and barriers of AFCIs were consistent with earlier reviews (e.g., Menec and Brown 2018). Our updated review focused on the factors that influenced outcomes rather than the initial phases of an AFCI, however, and suggests some new themes.
As shown in Table 2, the factors that supported or hindered implementing AFCIs centered around four main topics and 15 sub-topics related to who was involved and what they did. Wider external resources included government support, grants, and technical assistance. Local resources such as distance to other communities, existing infrastructure and services, a sense of community, and demographics could affect age friendliness. Engaged local participants included multiple stakeholders, specific champions, as well as older people themselves. Strategies to build support included quick wins, increasing awareness of age-friendliness, but also addressing issues of inclusion such as cultural sensitivity and tackling ageism.
Wider Political, Economic, and Technical Resources
Government
Strong government support at all levels was identified as a key facilitating factor for AFCI implementation, providing sources of leadership, funding, and policy and technical support (Menec et al. 2014; Plouffe et al. 2013). Though having less power than upper-level governments, city or municipal governments provided strong political support by adopting age-friendly policies and action plans, allotting staffing and local funds, and building the capacity of AFCIs (Black and Oh 2022; Rémillard-Boilard, Buffel and Phillipson 2021; Rémillard-Boilard 2019; Russell, Skinner and Fowler 2022). More effective AFCIs included such features as having a dedicated municipal government staff on the AFCI committee (Menec et al. 2014; 2022; Buffel et al. 2014; Plouffe et al. 2013).
In contrast, a lack of government support and changes in government could impede AFCI implementation (Brasher and Winterton 2016). In less effective AFCIs, municipal participation was minimal, with no council members sitting on the committee and few decisions made by the council to help AFCIs (Menec et al. 2014; 2022; Redondo and Gascón 2016; Garon et al. 2014). Further, government turnover frequently interrupted or slowed public policies and action plans (Menec et al. 2022; Redondo and Gascón 2016; Kendig et al. 2014; Neal, DeLaTorre and Carder 2014). Information might not be transferred to new officials, though there were chances to obtain support from new staff (Menec et al. 2014; Neal, DeLaTorre and Carder 2014). Murtagh et al. (2022) identified problems resulting from a lack of involvement by urban planners. Kendig et al. (2014) pointed out that the best opportunity would be to align the actions of governments at all levels.
Funding
The more effective AFCIs often leveraged additional funds from various sources (Menec et al. 2022; Garon et al. 2014; Plouffe et al. 2013; Gallagher and Mallhi 2010). Montreal's case showed that having an age-friendly action plan adopted by the city government encouraged most projects to consider older people's needs and provide resources (Rémillard-Boilard 2019). By integrating age-friendly considerations as central part of policy making, resources could be more consistent (Buffel et al. 2014).
Meanwhile, insufficient funds challenged the sustainability of AFCIs and limited the capacity of AFCIs to address larger issues (E. Russell, Skinner and Colibaba 2021; Rémillard-Boilard, Buffel and Phillipson 2021; Russell, Skinner and Fowler 2022; Redondo and Gascón 2016; Menec et al. 2014). Finances were especially challenging for rural AFCIs given fragmented locations (McCrillis, Skinner and Colibaba 2021). Conflicting priorities such as social inclusion and economic growth were also issues (Buffel et al. 2014). One solution was using the initial grant to build capacity to obtain additional funds, as well as achieving worthwhile changes with limited resources (Plouffe et al. 2013).
Support by Researchers and Consultants
Research work and researchers have played a critical role in moving AFCIs forward, though given our emphasis on academic literature it may be biased toward seeing such work positively. Obviously, the WHO has provided many technical resources on its web site; organizations like the US AARP do too. Research teams from universities and institutes have frequently collaborated with provincial and city governments (Buffel et al. 2014; Menec et al. 2014; Neal, DeLaTorre and Carder 2014; Plouffe et al. 2013). Such groups have performed baseline studies to help improve programs, for example, by paying more attention to disadvantaged groups (Buffel et al. 2014; Kendig et al. 2014). Researchers have joined AFCI advisory groups and provided guides and ongoing support, collaborating with the provincial and city governments and other technical groups (e.g., NGOs) (DeLaTorre and Neal 2017; Menec et al. 2014; Plouffe et al. 2013). Such participation by universities and researchers has increased the stability and continuity in implementing AFCIs (DeLaTorre and Neal 2017). Further, researchers have conducted implementation evaluations (Plouffe et al. 2013). Moreover, knowledge exchange in general could benefit all AFCIs at different stages, which could be catalyzed by research reports and publications (Rémillard-Boilard, Buffel and Phillipson 2021). However, Glicksman et al. (2014) have warned that not all collaborations with researchers are positive, outlining points of potential misunderstanding around political practices and academic culture.
Local Resources
Community Size and Proximity to an Urban Center
Proximity to other communities has made age-friendliness easier to achieve, providing an urban advantage (Spina and Menec 2015). In contrast in regional AFCIs which involved multiple discrete communities, distance between communities has challenged program attendance and communications (Colibaba, McCrillis and Skinner 2020). Additional problems included incompatible self-identities and needs in disconnected communities (McCrillis, Skinner and Colibaba 2021).
However, the small size of rural communities could be an advantage where AFCI actions could easily reach and directly benefit older residents (McCrillis, Skinner and Colibaba 2021). Menec et al. (2014) also found that the progress in larger urban AFCIs tended to be slower, compared to small rural communities where there was less bureaucracy and people knew each other. Similarly, the case of Pinawa town in Manitoba, Canada (population 1,450), showed that small size is not a barrier to age-friendly improvement (Plouffe et al. 2013).
Infrastructure
Poor existing infrastructure and services (e.g., public transport and local businesses) and human resources could make implementing AFCI actions and projects more challenging in remote, geographically isolated villages (Menec and Brown 2018). For example, older participants in a study in rural Canada described how a lack of facilities such as activity venues and transport services, as well as a lack of internet access, limited the programs in their AFCI (Colibaba, McCrillis and Skinner 2020). In contrast, AFCI leaders in another study of rural AFCIs reported that partnerships enabled them to draw upon existing infrastructure such as senior centers (McCrillis, Skinner and Colibaba 2021).
Staff and Volunteers
Local human resources, including staff and volunteers, were essential for AFCI implementation and sustainability. Local volunteers contributed to AFCIs by applying for grants, providing diverse expertise, and connecting older residents with AFCI services (Russell, Skinner and Colibaba 2021; Colibaba, McCrillis and Skinner 2020; Rémillard-Boilard 2019). However, many AFCIs, especially in smaller communities, experienced insufficient staff and volunteers and volunteer burnout (Colibaba, McCrillis and Skinner 2020; Menec et al. 2014; 2022). Reasons included lack of funds, outmigration, and low awareness of older people’s needs (Menec et al. 2022; Rémillard-Boilard, Buffel and Phillipson 2021; Redondo and Gascón 2016; Russell 2015).
Sense of Community
Studies showed that rural AFCIs had some advantages such as sense of community, rapport, or a sense that “everyone helps everyone” (McCrillis, Skinner and Colibaba 2021, 339). McCrillis, Skinner and Colibaba (2021) investigated five rural AFCIs in Ontario, Canada; two had difficulties in implementation. Based on interviews with 46 AFCI committee members, a robust sense of community and pre-existing connections supported the more effective AFCIs. People were willing to help each other, gathering volunteers, raising funds, and getting local clubs to serve the community (also Russell 2015). In contrast, lack of a united sense of community impeded AFCI implementation in fragmented communities (McCrillis, Skinner and Colibaba 2021).
Demographics
The demographic features of communities influenced priorities and social capital (Spina and Menec 2015; Russell 2015). When there was a greater concern for other population groups such as young adults or immigrants, the communities paid less attention to age-friendly efforts (Spina and Menec 2015). Menec et al. (2022)'s study of 52 AFCIs in Manitoba, Canada, showed that six out of the seven most sustainable AFCIs were in locations with increasing percentages of older people, while the four least sustainable AFCIs had no such increase. Further, interviewees’ comments from 11 mostly rural and remote AFCIs showed that outmigration had negative effects on social capital, which made it difficult to sustain active volunteerism levels, though many of these AFCIs had a large proportion of older residents (Russell 2015).
Meanwhile, demographics did not always prevent the AFCIs moving forward. Buffel et al. (2014) compared AFCI cases in the City of Brussels, Belgium, and the City of Manchester, UK. Manchester had a much lower percentage of older people than the rest of England and Wales due to both lower life expectancy and outmigration. Brussels also had a continuous decrease in the older population in the prior 15 years. Both cities became the first to join the WHO Global Network in their countries. In addition, among their activities, intergenerational projects linked the needs of younger and older people, an emphasis of WHO's European office (World Health Organization 2017). These achievements demonstrate how to cope with competing priorities (also Menec et al. 2014; Spina and Menec 2015).
Engaged Participants
Partnerships
AFCI studies consistently found that strategic partnerships with a wide range of stakeholders were essential to implementing and sustaining AFCIs (Rémillard-Boilard, Buffel and Phillipson 2021; Rémillard-Boilard 2019; Russell, Skinner and Fowler 2022; Russell 2015; Spina and Menec 2015; Plouffe et al. 2013; Gallagher and Mallhi 2010). These stakeholders included older people, youth, local government representatives (including planners), businesses, universities and schools, health services, media, non-profit organizations, and volunteer groups (Rémillard-Boilard, Buffel and Phillipson 2021; Russell, Skinner and Colibaba 2021; Spina and Menec 2015; Gallagher and Mallhi 2010). In contrast, those without new partnerships were less successful in implementing their programs (Russell 2015).
AFCIs used multiple approaches to build strategic multi-sector partnerships in their AFCI process. AFCI steering committees or advisory councils involved a wide range of stakeholders (Neal, DeLaTorre and Carder 2014; Plouffe et al. 2013; Gallagher and Mallhi 2010). AFCIs also built external partnerships by drawing upon pre-established local connections linking to other relevant initiatives (DeLaTorre and Neal 2017; McCrillis, Skinner and Colibaba 2021; Menec et al. 2014; Rémillard-Boilard, Buffel and Phillipson 2021). Moreover, some cities built innovative mechanisms and published strategic statements that encouraged collaborations (Rémillard-Boilard, Buffel and Phillipson 2021; Buffel et al. 2014). Partnerships and collaborations are a core feature of planning for healthy communities and that is no different for AFCIs (American Planning Association 2017). Surveys and cases of general planning for age friendliness have also found engagement and partnerships to be important (Keyes et al. 2014; Warner and Zhang 2021).
Local Leadership
It was both critical and challenging to have the right people lead AFCIs (Menec et al. 2014; Pestine-Stevens 2019). The improvement of age-friendliness in La Plata, Argentina, was largely attributed to the steering group who took strong leadership to promote the AFCI project (Redondo and Gascón 2016). In Russell's (2015) study, informants claimed that intrinsic motivations among the AFCI committee members were equally important, compared to municipal support. Conversely, a lack of leadership from the local government and the AFCI community affected other factors such as new partnerships (Menec et al. 2014). Leadership required not only motivation but also capabilities and skills (Spina and Menec 2015). Knowledge exchange, technical consulting, and especially having a dedicated municipal staff person in the AFCI community could support local AFCI leaders, as mentioned previously.
Champions
Different from other staff, a champion on the AFCI committee is typically an active and vocal volunteer or a person in government who promotes the AFCI (Russell, Skinner and Fowler 2022). The champions were important to AFCI progress because they had critical leadership in applying for new grants, organizing the committee, and transforming the proposal into action (Russell, Skinner and Fowler 2022; Russell 2015; Gallagher and Mallhi 2010). Studies found that AFCIs had better progress with at least one champion in the community, while some communities lost the impetus and failed to complete their projects without a champion (Gallagher and Mallhi 2010; Plouffe et al. 2013).
Involving Older People
As the core stakeholders, older people's perspectives and participation were particularly important in the AFCI implementation. Studies showed that more effective AFCIs included older people in the steering committee or advisory group (Elaine Gallagher and Mallhi 2010; Plouffe et al. 2013; DeLaTorre and Neal 2017). Some effective AFCIs involved older adults as active actors and leaders at all stages including developing a policy plan (Buffel et al. 2014; Garon et al. 2014). Many studies found insufficient participation. Brasher and Winterton (2016) examining AFCIs in Victoria, Australia, found less than two thirds of the 31 demonstration projects had older adults in the steering groups. Similarly, Black and Oh (2022) found moderate evidence of involving older people in AFCI processes based on progress reports of 30 AFCIs in the US. AFCIs could benefit more from actively engaging older people at all stages; indeed, it is part of the AFCI model.
Strategies to Build Support
Quick Wins
A few additional strategies were found essential in AFCI implementation, one of which was quick wins. The British Columbia experience showed that more effective AFCIs started with “low hanging fruit” to achieve worthwhile changes with limited resources. (Elaine Gallagher and Mallhi 2010, 11; Plouffe et al. 2013). Small but useful changes established confidence and raised awareness in the communities (Gallagher and Mallhi 2010). Small changes, such as adding a bus service with flexible routes, could improve bus usage and satisfaction among older people (Broome et al. 2013). On the contrary, when AFCI participants could not see the outcomes, they could be disappointed and discouraged (Rémillard-Boilard 2019).
Awareness
Ageism was identified as a barrier for implementing AFCIs (Buffel et al. 2014). Addressing ageism and raising awareness of age-friendliness in the public were useful strategies for AFCI to obtain support (Gallagher and Mallhi 2010; Menec et al. 2014; Plouffe et al. 2013). In contrast, lack of awareness of older people's needs led to low engagement of stakeholders (Menec et al. 2014). AFCIs promoted public awareness of age-friendliness in partnerships (Gallagher and Mallhi 2010; Plouffe et al. 2013). Branding age-friendly efforts at public events was useful for increasing awareness as well as identifying the AFCI outcomes (Buffel et al. 2014; Rémillard-Boilard 2019).
Culture
Another observed challenge hindering the effectiveness of AFCIs was insufficient connection to indigenous, marginalized, and disadvantaged population, though some AFCIs targeted diverse economic and cultural backgrounds (Buffel et al. 2014; Kendig et al. 2014). In Buffel et al. (2014) study, Manchester's AFCI interventions targeted ethnic minority older people, but Brussels did not seem to. In rural contexts, social and recreational programs were often limited to a small group of older people (Russell, Skinner and Colibaba 2021). Colibaba, McCrillis, and Skinner (2020) investigated a Canadian rural AFCI based on semi-structured interviews with 10 older AFCI participants. Responses showed that the initiative was limited to small-scale social and physical activity programs and with limited bilingual support. Those homebound due to physical condition or geographical isolation benefited little (Colibaba, McCrillis and Skinner 2020).
Implications and Research Gaps
This paper has investigated AFCI outcomes and the factors helping or hindering them from achieving positive results. Several factors are important for achieving more substantial positive outcomes: external resources (e.g., funding, consultants), local resources (e.g., community size, demographics, staff, infrastructure), engaged local participants (e.g., partnerships, champions, older people), and effective strategies to build support (e.g., quick wins, awareness building, cultural sensitivity).
This review raises several implications for practice. These include the special needs of rural areas, leadership, and institutionalizing age friendliness.
Practical Lessons for AFCIs
Rural and urban areas faced a mix of challenges and opportunities; however, studies examining rural AFCIs indicated a general lack of resources (e.g., staff, volunteers, and transport services). This limited the scope of the initiatives, particularly for broader issues such as housing and transport, and their longevity (Russell, Skinner and Colibaba 2021). These findings echo those of Warner and Zhang (2022) who studied how well U.S. communities conducted comprehensive planning and zoning to meet the needs of children and older people, finding rural areas struggled.
Russell, Skinner, and Colibaba (2021, 222) asked “whether it is realistic to expect small committees to develop programs that meet the challenges of aging in rural regions.” The more sustainable rural AFCIs drew upon a sense of community, using pre-existing local partnerships to fill budget gaps, and engaging older residents as leaders, volunteers, and participants. However, to achieve bigger goals, rural AFCIs need more support.
Vision and leadership are particularly important for AFCI effectiveness given limited funding and competing local priorities. Many cases mentioned champions. The cases of Brussels and Manchester showed that both cities’ vision and strategies influenced AFCI implementation, overcoming demographic disadvantages (Buffel et al. 2014). However, compared to Brussels, Manchester had a broader vision of age-friendliness in terms of targeting those in deprived areas or from minority ethnic groups (Buffel et al. 2014).
Many AFCI programs emphasized special multi-sector partnerships; however, integrating age-friendliness and social inclusion into general policy making and urban development seemed to enhance sustainability. Age-friendly projects can work better as part of more comprehensive projects such as intergenerational housing (Menec et al. 2014; Spina and Menec 2015).
Another challenge is who is to be involved. It seems clear that actively engaging older people and targeting disadvantaged groups are beneficial. Dedicated staff are also important, though how many would depend on the design of the program. Researchers can help with evaluation to build confidence in the program, increase visibility in the public, as well as provide guidance for moving forward.
Research Gaps
With relatively few evaluations, more research on AFCIs could expand the diversity of users engaged, outcomes assessed, and geographical areas, deepening these results and addressing urban planning.
Many studies interviewed knowledgeable informants who were often leaders and members of AFCI committees. As noted earlier, only four of the documents included interviews or focus groups with older users. However, evaluation from a wider range of users’ perspectives, as well as older residents who did not or could not participate in the AFCI projects, would help broaden understanding. More importantly, more research is needed to explore the needs of underrepresented older populations, such as indigenous populations, ethnic minorities, and those in deprived areas, evaluating how the AFCIs had or had not benefited them. This could support more culturally sensitive strategies and action plans.
Few studies have focused on the long-term outcomes of AFCIs such as improvements to health. Most AFCI evaluations have analyzed documents and interviews. These studies produced valuable insights on what AFCIs have achieved and whether they are sustainable. However, more diverse studies could contribute to a more comprehensive understanding of the effectiveness of AFCIs in achieving longer-term outcomes. They could also deepen understandings of how local and external resources help AFCI success.
Most studies related to AFCI evaluations have focused on North America, Europe, and Australia. It may be because the cities involved in the earliest WHO AFCI efforts were mostly distributed in these areas. More studies from diverse locations could help understand how WHO-style age-friendly framework works in different geographic, economic, political, and cultural contexts.
One motivation for this paper was that the lessons from such assessments matter for urban planners and while planners can learn from more general AFCI programs there is a need for more evaluations to engage urban planning (Murtagh et al. 2022; DeLaTorre and Neal 2017; Neal, DeLaTorre and Carder 2014). Given the likely public and political interest in aging, taking a more active role in AFCIs could bring allies to planners. Planners are adept at the kind of generalist, cross-sectoral thinking needed in AFCIs. Alternatively, they can also learn lessons from these initiatives about the kinds of external and local resources, participants, and support-building strategies that have worked. They include issues such as champions, quick wins, and cultural sensitivity that can add nuance to planning ideas about effective implementation in multiple areas of planning.
Given the coming challenges of aging societies globally, much more could be done to learn from programs that put aging front and center. We hope urban planners embrace this challenge.
Footnotes
Acknowledgments
We are grateful to Jennifer Molinsky, Bailey Hu, and Ashley Tannebaum for comments on the draft manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is supported by the Social Technology for Global Aging Research Initiative at Harvard University.
Notes
Included Studies.
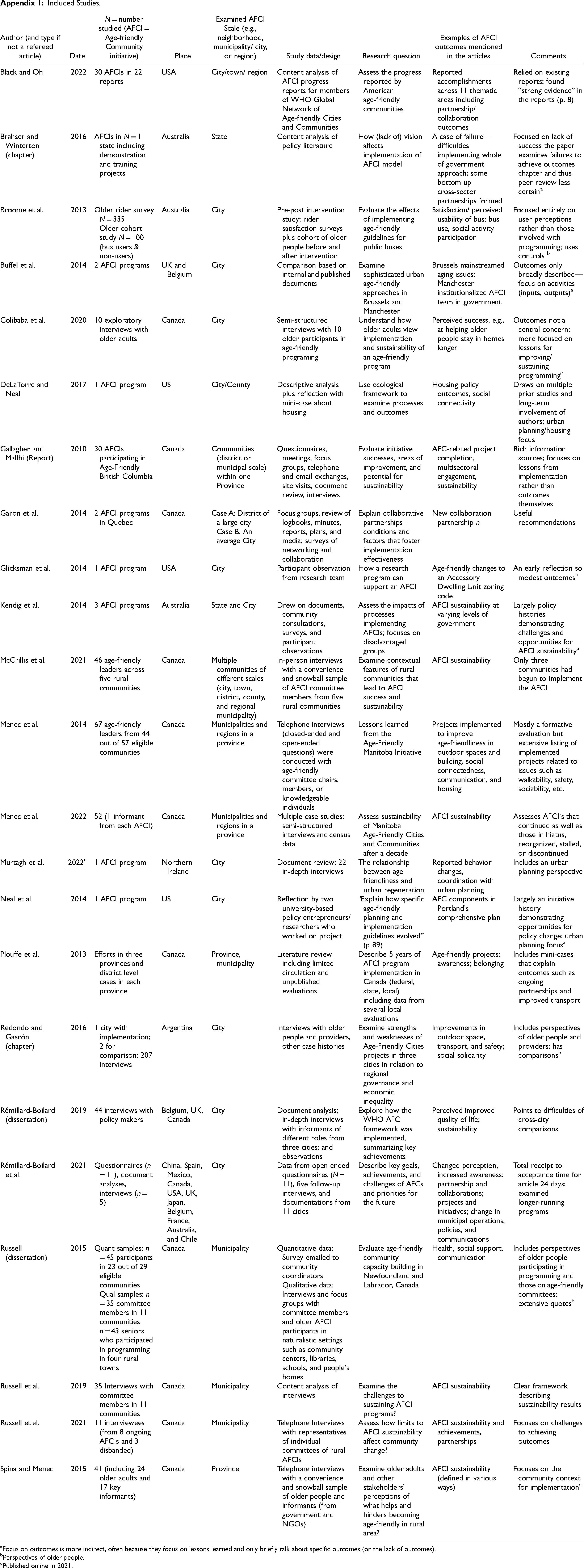
| Author (and type if not a refereed article) | Date | N = number studied (AFCI = Age-friendly Community initiative) | Place | Examined AFCI Scale (e.g., neighborhood, municipality/ city, or region) | Study data/design | Research question | Examples of AFCI outcomes mentioned in the articles | Comments |
|---|---|---|---|---|---|---|---|---|
| Black and Oh | 2022 | 30 AFCIs in 22 reports | USA | City/town/ region | Content analysis of AFCI progress reports for members of WHO Global Network of Age-friendly Cities and Communities | Assess the progress reported by American age-friendly communities | Reported accomplishments across 11 thematic areas including partnership/collaboration outcomes | Relied on existing reports; found “strong evidence” in the reports (p. 8) |
| Brahser and Winterton (chapter) | 2016 | AFCIs in N = 1 state including demonstration and training projects | Australia | State | Content analysis of policy literature | How (lack of) vision affects implementation of AFCI model | A case of failure—difficulties implementing whole of government approach; some bottom up cross-sector partnerships formed | Focused on lack of success the paper examines failures to achieve outcomes chapter and thus peer review less certaina |
| Broome et al. | 2013 | Older rider survey N = 335 Older cohort study N = 100 (bus users & non-users) |
Australia | City | Pre-post intervention study; rider satisfaction surveys plus cohort of older people before and after intervention | Evaluate the effects of implementing age-friendly guidelines for public buses | Satisfaction/ perceived usability of bus; bus use, social activity participation | Focused entirely on user perceptions rather than those involved with programming; uses controls b |
| Buffel et al. | 2014 | 2 AFCI programs | UK and Belgium | City | Comparison based on internal and published documents | Examine sophisticated urban age-friendly approaches in Brussels and Manchester | Brussels mainstreamed aging issues; Manchester institutionalized AFCI team in government | Outcomes only broadly described—focus on activities (inputs, outputs)a |
| Colibaba et al. | 2020 | 10 exploratory interviews with older adults | Canada | City | Semi-structured interviews with 10 older participants in age-friendly programing | Understand how older adults view implementation and sustainability of an age-friendly program | Perceived success, e.g., at helping older people stay in homes longer | Outcomes not a central concern; more focused on lessons for improving/ sustaining programmingc |
| DeLaTorre and Neal | 2017 | 1 AFCI program | US | City/County | Descriptive analysis plus reflection with mini-case about housing | Use ecological framework to examine processes and outcomes | Housing policy outcomes, social connectivity | Draws on multiple prior studies and long-term involvement of authors; urban planning/housing focus |
| Gallagher and Mallhi (Report) | 2010 | 30 AFCIs participating in Age-Friendly British Columbia | Canada | Communities (district or municipal scale) within one Province | Questionnaires, meetings, focus groups, telephone and email exchanges, site visits, document review, interviews | Evaluate initiative successes, areas of improvement, and potential for sustainability | AFC-related project completion, multisectoral engagement, sustainability | Rich information sources; focuses on lessons from implementation rather than outcomes themselves |
| Garon et al. | 2014 | 2 AFCI programs in Quebec | Canada | Case A: District of a large city Case B: An average City |
Focus groups, review of logbooks, minutes, reports, plans, and media; surveys of networking and collaboration | Explain collaborative partnerships conditions and factors that foster implementation effectiveness | New collaboration partnership n | Useful recommendations |
| Glicksman et al. | 2014 | 1 AFCI program | USA | City | Participant observation from research team | How a research program can support an AFCI | Age-friendly changes to an Accessory Dwelling Unit zoning code | An early reflection so modest outcomesa |
| Kendig et al. | 2014 | 3 AFCI programs | Australia | State and City | Drew on documents, community consultations, surveys, and participant observations | Assess the impacts of processes implementing AFCIs; focuses on disadvantaged groups | AFCI sustainability at varying levels of government | Largely policy histories demonstrating challenges and opportunities for AFCI sustainabilitya |
| McCrillis et al. | 2021 | 46 age-friendly leaders across five rural communities | Canada | Multiple communities of different scales (city, town, district, county, and regional municipality) | In-person interviews with a convenience and snowball sample of AFCI committee members from five rural communities | Examine contextual features of rural communities that lead to AFCI success and sustainability | AFCI sustainability | Only three communities had begun to implement the AFCI |
| Menec et al. | 2014 | 67 age-friendly leaders from 44 out of 57 eligible communities | Canada | Municipalities and regions in a province | Telephone interviews (closed-ended and open-ended questions) were conducted with age-friendly committee chairs, members, or knowledgeable individuals | Lessons learned from the Age-Friendly Manitoba Initiative | Projects implemented to improve age-friendliness in outdoor spaces and building, social connectedness, communication, and housing | Mostly a formative evaluation but extensive listing of implemented projects related to issues such as walkability, safety, sociability, etc. |
| Menec et al. | 2022 | 52 (1 informant from each AFCI) | Canada | Municipalities and regions in a province | Multiple case studies; semi-structured interviews and census data | Assess sustainability of Manitoba Age-Friendly Cities and Communities after a decade | AFCI sustainability | Assesses AFCI's that continued as well as those in hiatus, reorganized, stalled, or discontinued |
| Murtagh et al. | 2022c | 1 AFCI program | Northern Ireland | City | Document review; 22 in-depth interviews | The relationship between age friendliness and urban regeneration | Reported behavior changes, coordination with urban planning | Includes an urban planning perspective |
| Neal et al. | 2014 | 1 AFCI program | US | City | Reflection by two university-based policy entrepreneurs/ researchers who worked on project | "Explain how specific age-friendly planning and implementation guidelines evolved” (p 89) | AFC components in Portland's comprehensive plan | Largely an initiative history demonstrating opportunities for policy change; urban planning focusa |
| Plouffe et al. | 2013 | Efforts in three provinces and district level cases in each province | Canada | Province, municipality | Literature review including limited circulation and unpublished evaluations | Describe 5 years of AFCI program implementation in Canada (federal, state, local) including data from several local evaluations | Age-friendly projects; awareness; belonging | Includes mini-cases that explain outcomes such as ongoing partnerships and improved transport |
| Redondo and Gascón (chapter) |
2016 | 1 city with implementation; 2 for comparison; 207 interviews | Argentina | City | Interviews with older people and providers, other case histories | Examine strengths and weaknesses of Age-Friendly Cities projects in three cities in relation to regional governance and economic inequality | Improvements in outdoor space, transport, and safety; social solidarity | Includes perspectives of older people and providers; has comparisonsb |
| Rémillard-Boilard (dissertation) |
2019 | 44 interviews with policy makers | Belgium, UK, Canada | City | Document analysis; in-depth interviews with informants of different roles from three cities; and observations | Explore how the WHO AFC framework was implemented, summarizing key achievements | Perceived improved quality of life; sustainability | Points to difficulties of cross-city comparisons |
| Rémillard-Boilard et al. | 2021 | Questionnaires (n = 11), document analyses, interviews (n = 5) | China, Spain, Mexico, Canada, USA, UK, Japan, Belgium, France, Australia, and Chile | City | Data from open ended questionnaires (N = 11), five follow-up interviews, and documentations from 11 cities | Describe key goals, achievements, and challenges of AFCs and priorities for the future | Changed perception, increased awareness: partnership and collaborations; projects and initiatives; change in municipal operations, policies, and communications | Total receipt to acceptance time for article 24 days; examined longer-running programs |
| Russell (dissertation) |
2015 | Quant samples: n = 45 participants in 23 out of 29 eligible communities Qual samples: n = 35 committee members in 11 communities n = 43 seniors who participated in programming in four rural towns |
Canada | Municipality | Quantitative data: Survey emailed to community coordinators Qualitative data: Interviews and focus groups with committee members and older AFCI participants in naturalistic settings such as community centers, libraries, schools, and people's homes |
Evaluate age-friendly community capacity building in Newfoundland and Labrador, Canada | Health, social support, communication | Includes perspectives of older people participating in programming and those on age-friendly committees; extensive quotesb |
| Russell et al. | 2019 | 35 Interviews with committee members in 11 communities | Canada | Municipality | Content analysis of interviews | Examine the challenges to sustaining AFCI programs? | AFCI sustainability | Clear framework describing sustainability results |
| Russell et al. | 2021 | 11 interviewees (from 8 ongoing AFCIs and 3 disbanded) | Canada | Municipality | Telephone Interviews with representatives of individual committees of rural AFCIs | Assess how limits to AFCI sustainability affect community change? | AFCI sustainability and achievements, partnerships | Focuses on challenges to achieving outcomes |
| Spina and Menec | 2015 | 41 (including 24 older adults and 17 key informants) | Canada | Province | Telephone interviews with a convenience and snowball sample of older people and informants (from government and NGOs) | Examine older adults and other stakeholders’ perceptions of what helps and hinders becoming age-friendly in rural area? | AFCI sustainability (defined in various ways) | Focuses on the community context for implementationc |
Focus on outcomes is more indirect, often because they focus on lessons learned and only briefly talk about specific outcomes (or the lack of outcomes).
Perspectives of older people.
Published online in 2021.
Search Flow Diagram.