
Abstract
Objective
We sought to determine the patency of normal arterial branches from the covered segments of an artery after stenting.
Background
Most intracranial aneurysms occur at arterial branching points (bifurcations, side-branches, or perforators). The post-stenting patency of normal arterial branches from the covered segments of the artery is important. We have previously developed a hybrid stent with micropores to prevent early parent artery occlusion by more early endothelialization, and mid- to long-term parent artery stenosis by control of intimal hyperplasia after aneurysm occlusion.
Methods
We created aneurysms in 10 rabbits by distal ligation and intraluminal incubation of elastase within an endovascularly trapped proximal segment of the common carotid artery. All animals were treated with hybrid stents having micropores. Four animals were observed for one month and three each for three and 12 months. The patency of the side-branches of the subclavian artery was evaluated angiographically and in some cases, histologically.
Results
Aneurysms were completely occluded at all time points other than 12 months. The subclavian artery and brachiocephalic artery were patent, without significant stenosis. All the side-branches of the subclavian artery detected on the preoperative angiogram remained patent at the final assessment.
Conclusion
The use of hybrid stents for aneurysm repair and side-branch patency seems to be effective, as per the long-term results obtained in an animal model.
Introduction
Most intracranial aneurysms occur at arterial branching points (bifurcations, side-branches, or perforators). Simple covered stents are associated with the highest rate of complete aneurysm occlusion. However, their use in the human intracranial circulation is limited by access issues and the possibility of occluding small perforating end-arteries. It is important to assess the patency of normal arterial branches arising from the covered segments of the artery after implantation of simple covered stents. We established rabbit carotid aneurysms by intraluminal incubation of elastase within an endovascularly trapped segment of the proximal common carotid artery (CCA),1,2 and we implanted hybrid stents equipped with micropores in these aneurysms. 3 Besides studying the occlusive effect of the hybrid stents in the aneurysms, we examined the patency of the side-branches arising from the right subclavian artery (SA), both angiographically and histologically.
Materials and methods
All experiments were performed on Japanese white rabbits (3.5–4.2 kg) and conducted in accordance with the Principles of Laboratory Animal Care (formulated by the National Society for Medical Research, Chicago, IL) and the Guide for the Care and Use of Laboratory Animals (NIH publication no. 86–23, revised 1985; National Institute of Health, Bethesda, MD). The research protocol (no. 12010) was approved by the ethics committee of the National Cerebral and Cardiovascular Center Research Institute.
The aneurysms were first created and then subjected to stent implantation two to four weeks later under general anesthesia, which was induced by the intramuscular injection of 0.2 ml/kg ketamine chloride (10%) and 0.3 ml/kg xylazine, and additional dosage was determined on the basis of the animal’s movements.
Fabrication of hybrid stents (Figure 1)
A stainless mold (diameter, 1 mm) was dipped in a tetrahydrofuran solution and allowed to dry. Subsequently, a balloon-expandable coronary-artery bare stent (Momo stent: diameter, 3 mm; length, 20 mm; Japan Stent Technology, Okayama, Japan) was mounted on the cover film of the mold, and again, it was dipped in the solution and dried. The thickness of the cover film was restricted to approximately 30 µm. Micropores were then made in the cover film using a KrF excimer laser apparatus (L4500; Hamamatsu Photonics, Shizuoka, Japan). Micropores are circular, with a pore diameter and interpore distance of 100 µm and 250 µm, respectively, such that they achieve an opening ratio of 23.6% (calculated) after full expansion. 3 The uncoated stent was a bare stent with an opening ratio of 86%. The outer surface of the film of the microporous stent grafts was coated with argatroban (500 µg/cm 2 ), which was applied using a methanol solution (1% w/v); the solvent was subsequently volatilized for physical adsorption. The fabricated hybrid stent was then remounted on the delivery balloon system (Thrill Slalom PTA dilatation balloon catheter; diameter, 3 mm; length, 2 cm; Cordis, J & J, Europa, N. V., Netherlands).
Preparation of aneurysms in rabbits (Figure 2(a))
Aneurysms were constructed in 10 female rabbits by employing a previously described method,1,2 with a few simple modifications. The right CCA was surgically isolated, ligated distally, and controlled proximally with 2.0 silk sutures before a 5-Fr detachable sheath introducer (Medikit, Tokyo, Japan) was induced and passed retrograde to the midportion of the CCA (approximately 3 cm cephalad to the origin of the CCA). A hemostatic valve of the sheath (Medikit, Tokyo, Japan) was detached, and a rotational and hemostatic triple connecter was connected to the sheath placed in the CCA. Through the sheath, an occlusive microballoon (Naviballoon; Kaneka, Tokyo, Japan) (Titan percutaneous transluminal coronal angioplasty (PTCA) dilatation balloon catheter: diameter, 4.0 mm; length, 9 mm; Cordis, J & J, Miami, Florida, USA) and subsequently a microcatheter (Excelsior SL10; Striker, Tokyo, Japan) were advanced near the CCA origin (Figure 2(b)). Porcine elastase (Sigma, Tokyo, Japan) was mixed with nonionic contrast medium to obtain a 25% dilution. Elastase (6.8 units/mg/0.25 cc) was injected and incubated in the isolated CCA for 20 min, while the balloon was inflated at the origin of the right CCA. Next, the microcatheter and deflated microballoon were removed. Angiography was performed to confirm the dilation of the affected CCA. The CCA was ligated with a 2.0 silk thread after sheath removal, and the skin was closed by discontinuous knots with a similar thread.
Endovascular technique
No drugs, such as antiplatelets, were administered during the study. Endovascular treatment was performed via the right femoral artery, at two to four weeks after the creation of the aneurysm. The femoral artery was exposed and ligated distally with a 2.0 silk thread. After pharmacological dilation of the artery with 8 mg of papaverine chloride, a 19-G puncture needle was used to introduce the 0.032″ mandrel; then, a 4-Fr 10-cm sheath (Clinical Supply, Tokyo, Japan) was advanced into the right femoral artery under fluoroscopic guidance.
The 4-Fr catheter was navigated into the brachiocephalic artery (BCA) with a 0.035″ guidewire. Digital subtraction angiography (DSA) showed the BCA, SA, and aneurysm. A balloon catheter (Thrill Slalom PTA dilatation balloon catheter; diameter, 3 mm; length, 2 cm; Cordis, J & J, Europa, N.V., Netherlands) crimped with our hybrid stent was passed through the sheath and navigated into the BCA. Using fluoroscopy and road mapping, we advanced the hybrid stent over the balloon catheter across the aneurysmal neck and inflated the balloon. Post-procedural DSA was performed. The balloon catheter was removed, leaving the hybrid stent in place. Subsequently, the sheath introducer was carefully and slowly pulled out. The femoral artery was ligated with two sutures of a 2.0 silk thread previously placed around the artery, and the skin was closed discontinuously with a similar thread.
Final angiography and harvesting
After the observation period, angiography was performed using a 4-Fr sheath placed at the left CCA in all animals. The left CCA was exposed and ligated distally. A 19-G puncture needle was used to introduce the 0.032″ mandrel; then, a 4-Fr, 10-cm long sheath (Clinical Supply, Tokyo, Japan) was advanced to the left proximal CCA under fluoroscopic guidance. A DSA series was performed to evaluate the final angiographic result. Occlusion of the aneurysms and patency of preoperatively detected side-branches of the artery was evaluated angiographically. Thereafter, the animals were subjected to euthanasia by intravenous injection of potassium chloride. The BCA, the right SA, vertebral artery (VA), some other arterial branches, and the treated aneurysm were resected en bloc and placed directly in a 4% paraformaldehyde phosphate-buffered saline solution for rapid fixation. Some of the samples were evaluated histologically to determine the patency of the branches.
Histology
Histological examination was performed in some cases, by using a cross-sectional sample (hematoxylin and eosin (H&E) stain) obtained from the stented portion of the aneurysm to confirm the patency of the side-branches.
Results
A balloon catheter crimped with our hybrid stent was easily and smoothly passed through the sheath, navigated into the BCA and right SA via the aorta, and inflated at the neck of the aneurysm. The hybrid stent covered and occluded the aneurysm instantly or after a few minutes. All the side-branches of the right SA observed preoperatively appeared patent (without any significant stenosis) on the angiograms obtained at one, six, and 12 months.
Stent graft and its remounting
The stent struts were completely embedded within the cover film, thereby indicating that the luminal surface of the stent graft was smooth and flat (Figure 1(a) and (b)). It was possible to shrink the stent grafts by using a hand-held crimping device, without any damage to the cover film. Stenting procedures were performed using standard endoscopic procedures without difficulty.3,4 A hybrid stent is shown. Micropores (with a pore diameter and interpore distance of 100 µm and 250 µm, respectively, to accomplish an opening ratio of 23.6% after full expansion) are placed in a polyurethane membrane of approximately 30-µm thickness on a bare coronary stent (a coronary Momo stent, Japan Stent Technology). (a) Macroscopic image and (b) scanning electron microscopic image.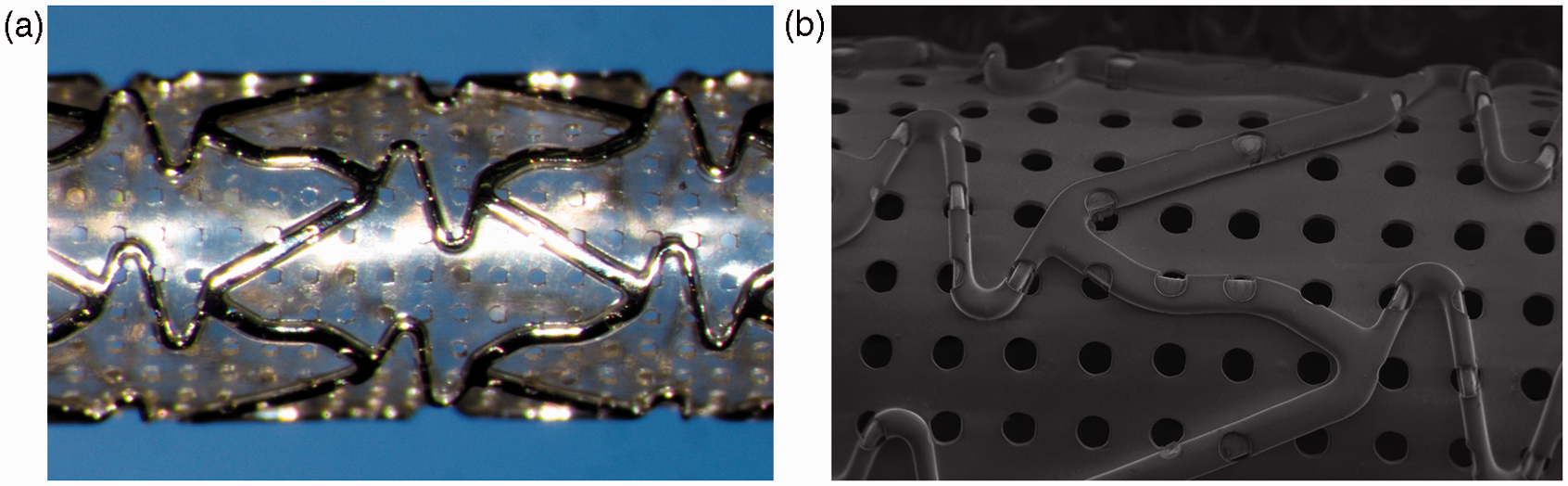
Fabrication of carotid aneurysms (Figure 2(c))
All aneurysms were systematically and easily created by our modified method. A 5-Fr detachable sheath introducer, later connected with a rotational and hemostatic triple connector, was easily inserted into the affected CCA. An occlusive balloon and microcatheter were navigated into the CCA origin without difficulty. The size and shape of the aneurysms were variable, although they were originally funnel-shaped.
Occlusion of the aneurysm (Table 1)
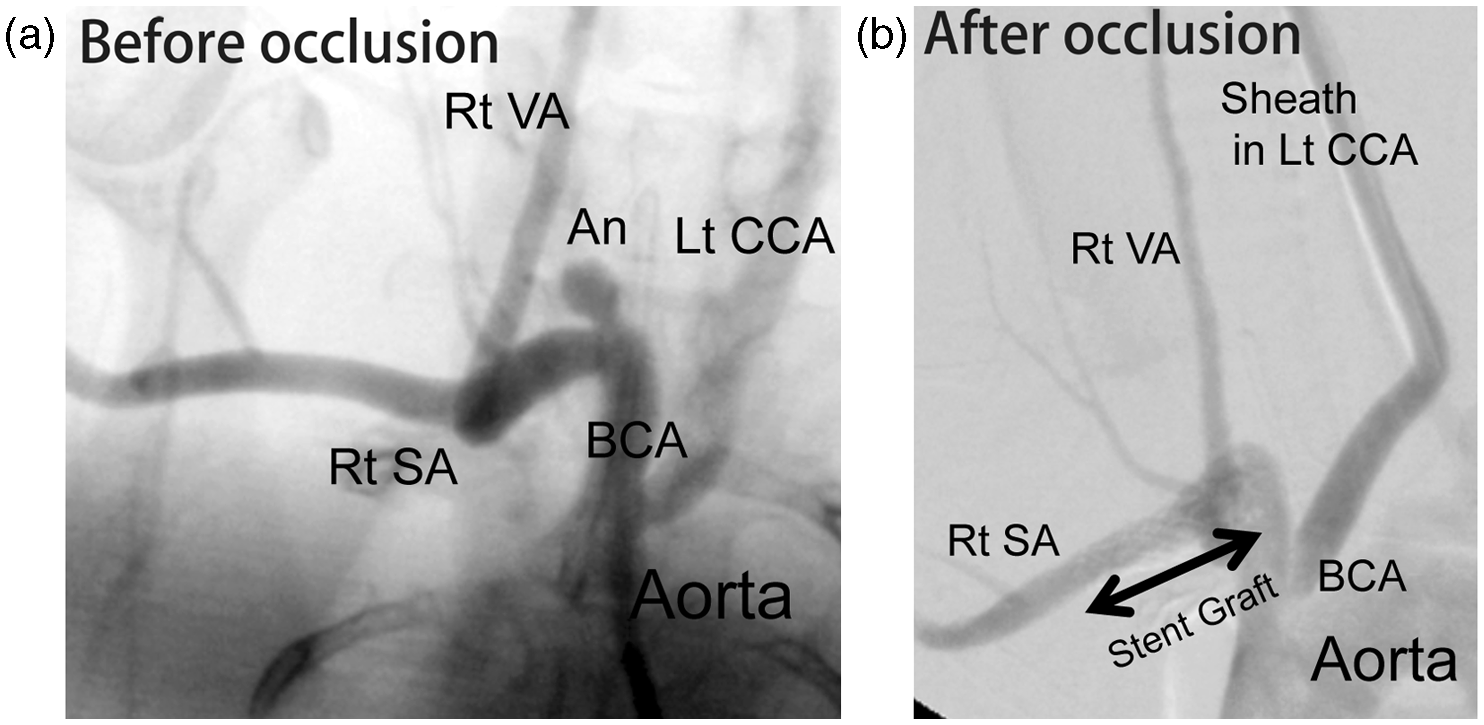
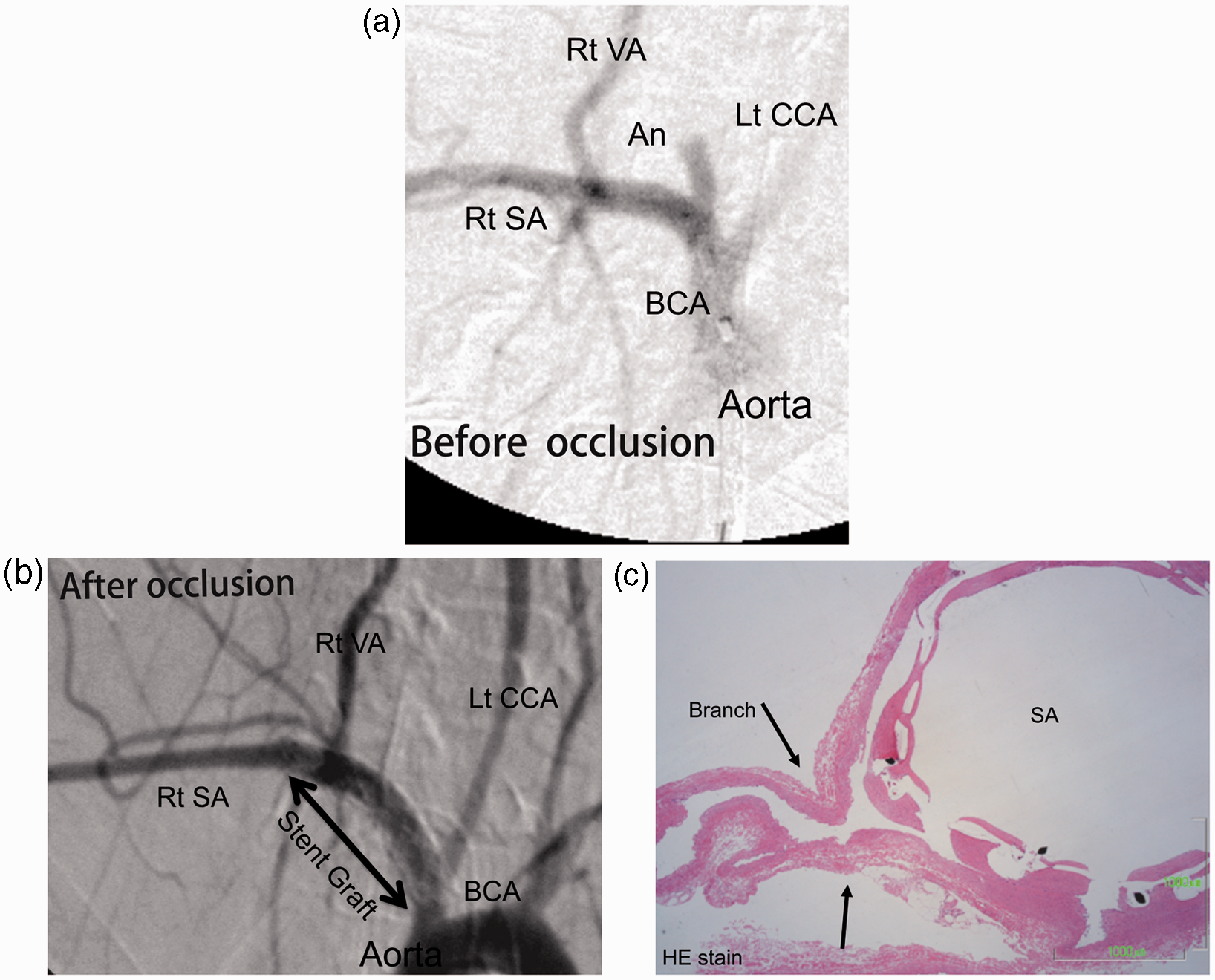
At 12 months, all aneurysms but one were completely occluded, with four aneurysms being occluded at one month; three, at three months (Figure 3(a) and (b)); and two, at 12 months (Figure 4(a) and (b)). At the 12-month follow-up, one aneurysm remained patent because of distal movement of the hybrid stent itself from the aneurysm neck. A schema of the aneurysm occlusion in the rabbit using a hybrid stent (arrows) implanted through the femoral artery. Branches such as the vertebral artery, internal thoracic artery, and costocervical artery are indicated (a). Approach to the right CCA via a rotational and hemostatic triple connector. A microcatheter and microballoon are inserted from each hemostatic valve (b). Entrapment system in the right CCA. A microballoon and microcatheter through a 5-Fr detachable sheath (c). CCA: common carotid artery; VA: vertebral artery; ITA: internal thoracic artery; SA: subclavian artery. At three months after occlusion, the aneurysm was still occluded (before (a) and after (b)). Side-branches, such as the vertebral artery and costocervical artery, were patent. An arrow shows a stent graft placed a cross the aneurysmal neck (b). CCA: common carotid artery; VA: vertebral artery; BCA: brachiocephalic artery; SA: subclavian artery. At 12 months after occlusion, the aneurysm was completely occluded (pre (a) and post (b)), while the vertebral artery, internal thoracic artery, and costocervical artery remained patent. An arrow shows a stent graft placed across the aneurysmal neck (b). A cross-sectional specimen (H&E stain) showed that the origin of the branch (arrows) from the subclavian artery was patent at 12 months (c). CCA: common carotid artery; VA: vertebral artery; BCA: brachiocephalic artery; SA: subclavian artery; H&E stain: hematoxylin and eosin stain.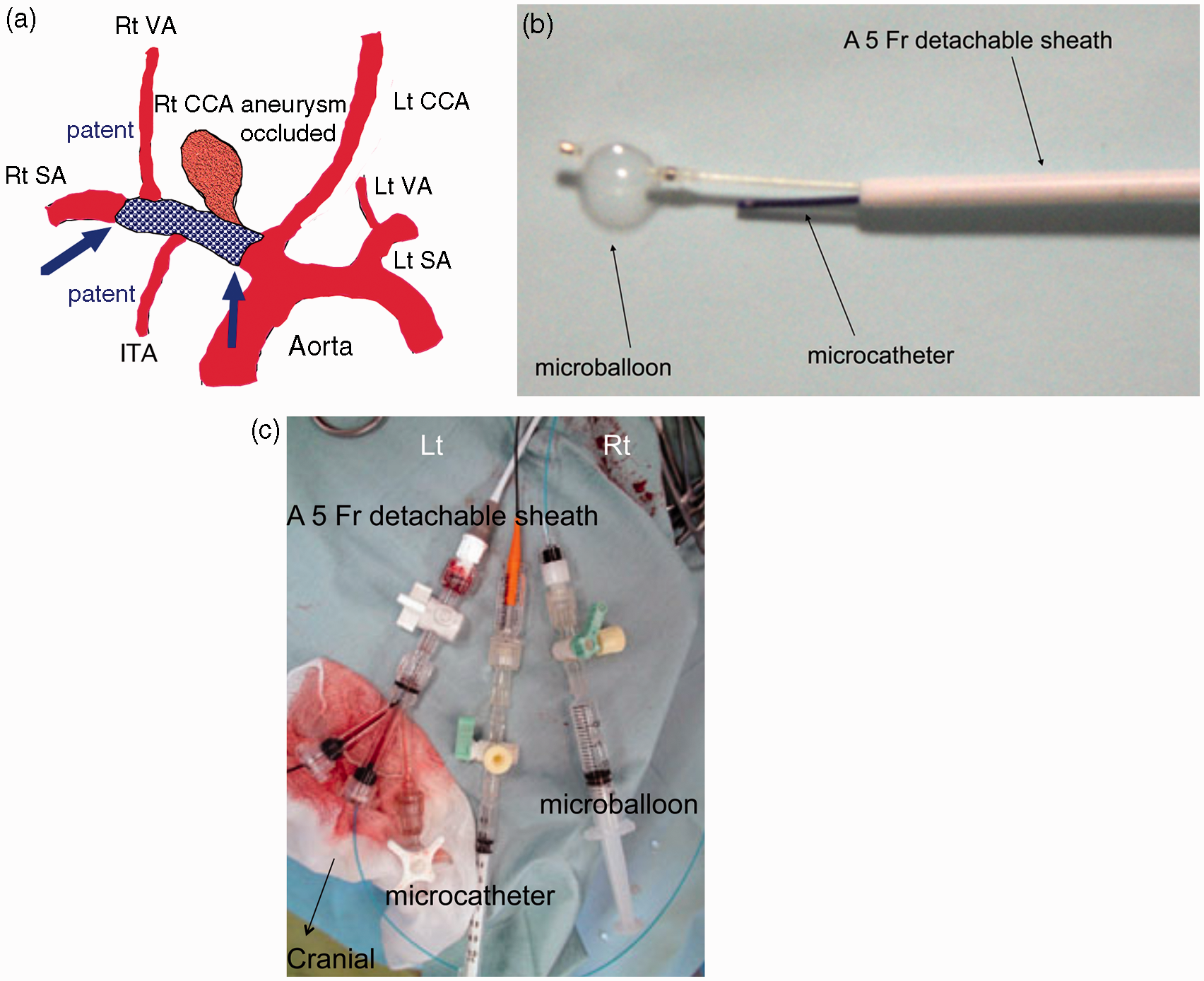
Preservation of side-branches
Results.
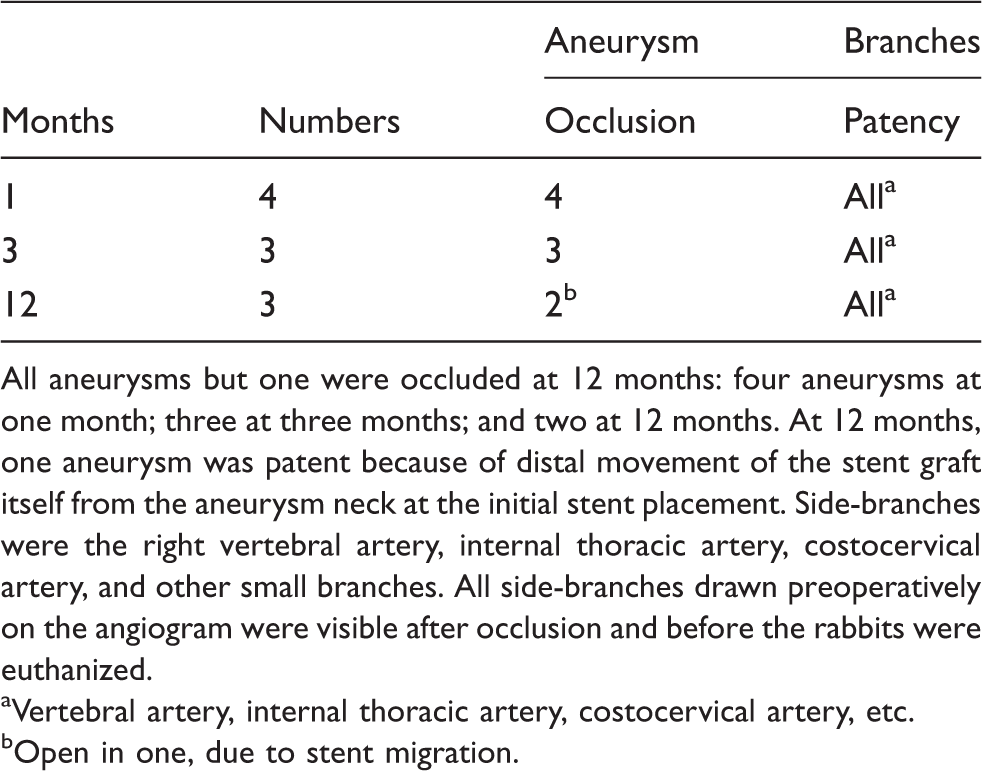
All aneurysms but one were occluded at 12 months: four aneurysms at one month; three at three months; and two at 12 months. At 12 months, one aneurysm was patent because of distal movement of the stent graft itself from the aneurysm neck at the initial stent placement. Side-branches were the right vertebral artery, internal thoracic artery, costocervical artery, and other small branches. All side-branches drawn preoperatively on the angiogram were visible after occlusion and before the rabbits were euthanized.
aVertebral artery, internal thoracic artery, costocervical artery, etc.
bOpen in one, due to stent migration.
Discussion
Although Guglielmi detachable coil systems (GDC coils) have been widely accepted and used in the treatment of intracranial aneurysms, primary stenting of aneurysms by using porous stents 5 or stent grafts 6 and implantation of coils after stenting7–10 are emerging techniques in endovascular treatment.
The development of stent grafts for intracranial aneurysms is challenging. Most intracranial aneurysms occur at branch points (bifurcation, small side-branches, and perforating arteries). The maintenance of the patency of normal arterial branches originating from the covered segment of the artery after stenting across the lesion is a major concern. The salient issues influencing the use of stent grafting for aneurysms in humans include the delivery of the stent graft, degree of cover porosity, configuration of the aneurysm, curvature of the parent vessel, and presence or absence of perforating end-arteries. 2
A simple bare stent has no efficacious occlusive effect on aneurysms, although it raises a few concerns about the occlusion of side-branches. In contrast, a simple covered stent has sufficient occlusive effect on the aneurysms, but it can occlude the side-branches. To compensate for the disadvantages of simple covered stents, we have been developing a hybrid stent. This hybrid stent consists of the commercially available balloon-expandable coronary-artery stent with a thin SPU film (by dip-coating method) on which micropores have been created by the excimer laser ablation technique, followed by coating with argatroban. 4 We have developed a hybrid stent with micropores to prevent early parent artery occlusion by more early endothelialization and administration of argatroban, and mid- to long-term parent artery stenosis by control of intimal hyperplasia after aneurysm occlusion, compared with those in a simple covered stent.
In the current study, we established elastase-induced rabbit carotid aneurysms, all of which were occluded by our hybrid stents until 12 months, and all the small side-branches detected preoperatively remained patent without significant stenosis or occlusion even after implantation of the hybrid stents. The hybrid stent was smoothly navigated into the affected BCA and SA from the femoral artery, as easily as the bare stents.
Our microporous membrane induces early endothelialization capable of secreting tissue plasminogen 11 within one week of stent graft implantation, 3 thereby avoiding early thrombosis and controlling mid- to long-term hyperplasia. 12 Polyurethane has excellent elastomeric properties and is clinically used as a material for manufacturing blood pumps and arterial grafts; it also exhibits no toxicity or little biodegradation.13–15 Argatroban, an arginine-derived synthetic low-molecular-weight compound that binds to thrombin, competitively inhibits fibrinogen cleavage and the platelet activation stimulated by thrombin.16,17 It has been used for preparing antithrombogenic surfaces in percutaneous transluminal angioplasty (PTA) devices, including balloon catheters and stents.18,19
In this study, cerebral thromboembolic events were not evaluated using magnetic resonance imaging (MRI). Less intimal hyperplasia of the parent artery was focally noted in the group treated with hybrid stents without antiplatelets. If this device is clinically used, antiplatelet therapy with one or two drugs will be necessary for approximately one to three months, as per the conventional therapy after vascular stenting.
The aneurysms were created experimentally by intraluminal incubation of elastase within an endovascularly trapped segment of the proximal portion of the CCA, with slight modifications to the method. The CCA branches from the BCA of the rabbit, and it was ligated beyond the point of elastase incubation. Endoluminal digestion of the internal elastic lamina, with spreading of elastase up to the adventitia, results in a thin-walled aneurysm, as observed in humans. 20 Aneurysm formation occurred over a two-week period, after which the animals were treated with the respective therapies. The rabbit aneurysm model with elastase has some characteristic features: (1) long-term patency in untreated animals, (2) simulating aneurysm morphologies that place a high shear stress on the aneurysmal neck, (3) similar size in aneurysm diameter and parent artery diameter, (4) maintenance of the integrity of the endothelium of the aneurysmal cavity, and (5) short construction time and easy reproduction. 21 The rabbit aneurysm is histologically similar to the human saccular aneurysm and was useful for the current study.
Mechanisms of branch occlusion by stents include the longitudinal snow-plowing effect, stent jailing (early stage), and in-stent neointimal growth (late stage) during or after stent deployment. 22 Cerebral vessels with aneurysms tended to be minimally atherosclerotic. Radial force in the stent strut might be less than that in the intracranial PTA stent, which reduced the longitudinal redistribution of the plaque. Our hybrid stent had a porosity appropriate for the regulation of the in-stent neointima growth even at 12 months (personal communication). The arteriovenous pressure gradient is the driving force of the blood flow through the branches and perforators under normal conditions. Additionally, long-term remodeling of the artery and its lumen, in response to the presence of the intraluminal prosthesis, is less likely to result in complete occlusion of the jailed branch. 22 Experimental evidence in dogs showed that vessels (small muscular branches from the VA) comparable to human perforators tend to remain patent if less than 50% of the ostial diameter is covered with the stent strut. 23 If the diameter of struts is 100 µm, complete occlusion of the perforators may not occur, but the exposed stent wire covering the perforators will remain a potential source of thromboembolic complications in canine carotid aneurysm models. 24 The diameter of stent struts in our hybrid stent was less than 50 µm. Fibrotic tissue growth around the filaments extended into the origin of the branches (external arteries) without narrowing them significantly.
Intracranial self-expanding stents generate a radial force too weak to require coverage with cover materials, although some of them, such as Neuroform or Enterprise, are recommended. Therefore, we selected balloon-expandable coronary-artery stents for the preparation of hybrid stents.
The branch originating from the aneurysm sac, which is treated with a flow diverter (pipeline embolization device), is kept patent in the presence of a flow demand through it. 25 The significant shrinkage of the aneurysm gives the branch an “infundibular-like” appearance at its origin, or the branch is represented by a tortuous takeoff from the parent artery in place of the initial aneurysm. A slow occlusion process for the treatment of ruptured aneurysms is yet to be developed.
The stent developed by us is a hybrid of a bare stent and a simple covered stent; this hybrid nature helps regulate the porosity and enables early intraluminal endothelialization and late inhibition of the intimal hyperplasia. Experimentally fabricated canine carotid aneurysms were occluded with the placement of our hybrid, self-expanding, stent grafts at one, 4 six, and 12 months (personal communication). A porosity of 23.6% was found to be suitable in the presence of less neointimal hyperplasia. 4 On the basis of the porosity and demand of the blood flow by vessels, side-branches or perforating arteries can be protected if the stenotic area generated by the hybrid stents is less than 50%. 23
In this study, the patency of all the side-branches was maintained, along with the occlusion of the aneurysms, although the side-branches were not as narrow as the intracranial perforators. If the use of hybrid stents for aneurysmal occlusion is planned, the number of associated perforators should be less to ensure safety.
In the examined aneurysmal model using stent grafts, all small side-branches of the patent artery were patent without significant stenosis. Thus, our hybrid stent represents a step forward in the clinical management of aneurysms.
Conclusion
The long-term results obtained in an animal model indicate that hybrid stents may be effective for aneurysm repair while maintaining side-branch patency.
Footnotes
Acknowledgements
We appreciate the kindness of Shuzoh Yamashita, PhD, President of Japan Stent Technology Co. Ltd, in supplying the MoMo stent for our hybrid stents.