
Abstract
Patients with advanced liver disease challenge anesthesiologists, especially those providing regional anesthesia for postoperative pain management. Coagulopathy, encephalopathy, sepsis and other comorbidities complicate care. Liver failure lowers albumin and α1-acid glycoprotein and slows hepatic clearance, increasing the unbound fraction and effective exposure to amide local anesthetics. Risks are magnified by acidosis, low cardiac output, low body mass index, sepsis, and concurrent renal dysfunction. Neuraxial options are often limited by coagulopathy and the risk of catastrophic neurologic complications while superficial, compressible peripheral blocks are generally considered safer than deep plexus targets. Safe practice includes the use of ultrasound guidance, incremental injection with frequent aspirations, avoidance of unnecessary high-dose multiple-site injections, and conservative dosing and infusion strategies. Regional anesthesia is feasible in patients with hepatic failure when dose and technique are adjusted to disease biology and when local anesthetic systemic toxicity (LAST) preparedness is routine. Catheters should run at lower concentrations and rates with scheduled reassessment and clearly communicated stop times. Teams should keep 20% lipid emulsion immediately available for treatment of neurologic or cardiovascular signs of LAST. We provide a practical pathway to select the block, choose the agent, and set doses that keep a reasonable safety margin for local anesthetics.
Introduction
Regional anesthesia has expanded rapidly over the past decade, driven by the routine availability of ultrasound and a growing number of fascial plane techniques. Used as part of multimodal analgesia, regional analgesia helps limit perioperative opioid exposure, decrease the complications of uncontrolled surgical pain, and when done well, can shorten recovery and improve patient experience. These benefits are especially attractive in patients with advanced liver disease who often are vulnerable to delirium, respiratory compromise, and prolonged hospitalization when pain is poorly controlled. 1 Ultrasound-guided peripheral nerve, neuraxial and fascial plane block techniques can provide targeted analgesia and reduce acute postsurgical pain. In everyday practice, catheter-based strategies and fascial plane blocks have made high-quality incisional analgesia manageable in a wide range of settings. Yet hepatic failure also narrows the safety window with local anesthetics. Coagulopathy, hemodynamic instability, pharmacokinetics, reduced protein binding and slower hepatic clearance raise the stakes for each milligram of local anesthetic and complicate decisions about regional techniques. Institutional culture and variable familiarity with newer blocks further influence whether regional anesthesia is offered at all.
High quality randomized trials in this population remain limited; most data come from liver surgery cohorts, including hepatectomy and transplantation, as well as observational studies, which clinicians must translate thoughtfully to cirrhosis and acute liver failure. As such, this article is a narrative non-systematic review intended to focus on clinically relevant and high-impact literature. We connect liver pathophysiology to practical choices in technique selection, dosing, catheter use, and monitoring for patients with hepatic failure, emphasizing approaches that favor compressible targets and conservative pharmacology. The safety of intravenous lidocaine infusions is briefly discussed as well. Our goal is not simply to endorse or discourage specific techniques, but to provide a practical pathway that leads to a safe analgesic plan.
If patients with hepatic failure are so high risk, why even consider regional anesthesia with local anesthetic? The answer lies in recognizing that nearly all components of multimodal analgesia carry some degree of risk including acetaminophen, ketamine, IV lidocaine, NSAIDs such as ibuprofen, and opioids. Expert recommendations emphasize that regional techniques can be used judiciously, and these recommendations reflect consensus from leaders in the field, including the Society for the Advancement of Transplant Anesthesia and International Liver Transplant Society. It is also important to appreciate that regional anesthesia is an evolving discipline: fascial plane blocks have gained prominence, and several newer techniques, such as the erector spinae plane (ESP) block, pericapsular nerve group (PENG) block, and external oblique intercostal (EOI) block, have emerged within the last decade.
This article provides a focused discussion of hepatic failure in the context of major hepatic surgery, including liver resection, living-donor hepatectomy, and liver transplantation. While overarching regional anesthesia modalities may be offered, such as epidural, spinal, paravertebral or peripheral nerve blocks, this review primarily emphasizes the profile of fascial plane blocks. Fascial plane blocks are increasingly viewed as the most progressive option as a part of multimodal analgesia in this high-risk population.
Pharmacologic Considerations
Metabolism
Commonly used amide local anesthetics, such as lidocaine, bupivacaine, ropivacaine, and mepivacaine, undergo cytochrome P450-mediated oxidation, dealkylation, and conjugation before renal excretion. Lidocaine behaves as a higher-extraction drug with clearance depending more on hepatic blood flow, whereas bupivacaine and ropivacaine are more capacity-limited, relying on enzymatic activity. Albumin and α1-acid glycoprotein bind to local anesthetics. A cirrhotic state lowers protein concentration in the serum, thereby increasing the active fraction of free local anesthetic and shrinking the safety margin for local anesthetic systemic toxicity (LAST).2,3
In contrast to local anesthetics, intravenous anesthetics such as propofol undergo hepatic glucuronidation and hydroxylation. Notably, clearance is not markedly affected in patients with chronic cirrhosis. 4 However, in severe hepatic impairment, target-controlled propofol infusion results in measured anesthetic concentrations that are higher than predicted values. 5
Pharmacokinetics
Hepatic failure increases free fraction and slows clearance, lengthening half-life, raising steady-state levels, and amplifying cumulative exposure during infusions (Figure 1).1–3 Acidosis promotes ion trapping in the central nervous system and myocardium. Low cardiac output and hypotension further delay clearance; sarcopenia/low body mass reduce volume of distribution, so the same dose yields higher peaks.6,7 When regional anesthesia techniques are employed, ropivacaine and bupivacaine accumulate toward steady state over hours. With impaired clearance, steady-state concentrations are higher for any given infusion rate. 8 Recent literature demonstrates that in patients undergoing liver donor hepatectomy, clearance of lidocaine from a continuous intravenous infusion is reduced by up to 60% when a segment of the liver is surgically removed. Despite this impaired clearance, a continuous lidocaine infusion was safely administered in 15 patients. In their protocol, a 1 mg/kg dose was given at anesthesia induction followed by a continuous infusion at 1 mg/kg/hr. 9 Notably, the lidocaine infusion was stopped upon completion of the hepatectomy portion of the procedure. Although the infusion was stopped in this study, lidocaine infusions have been shown to be safely delivered in this setting for up to 72 h. 10
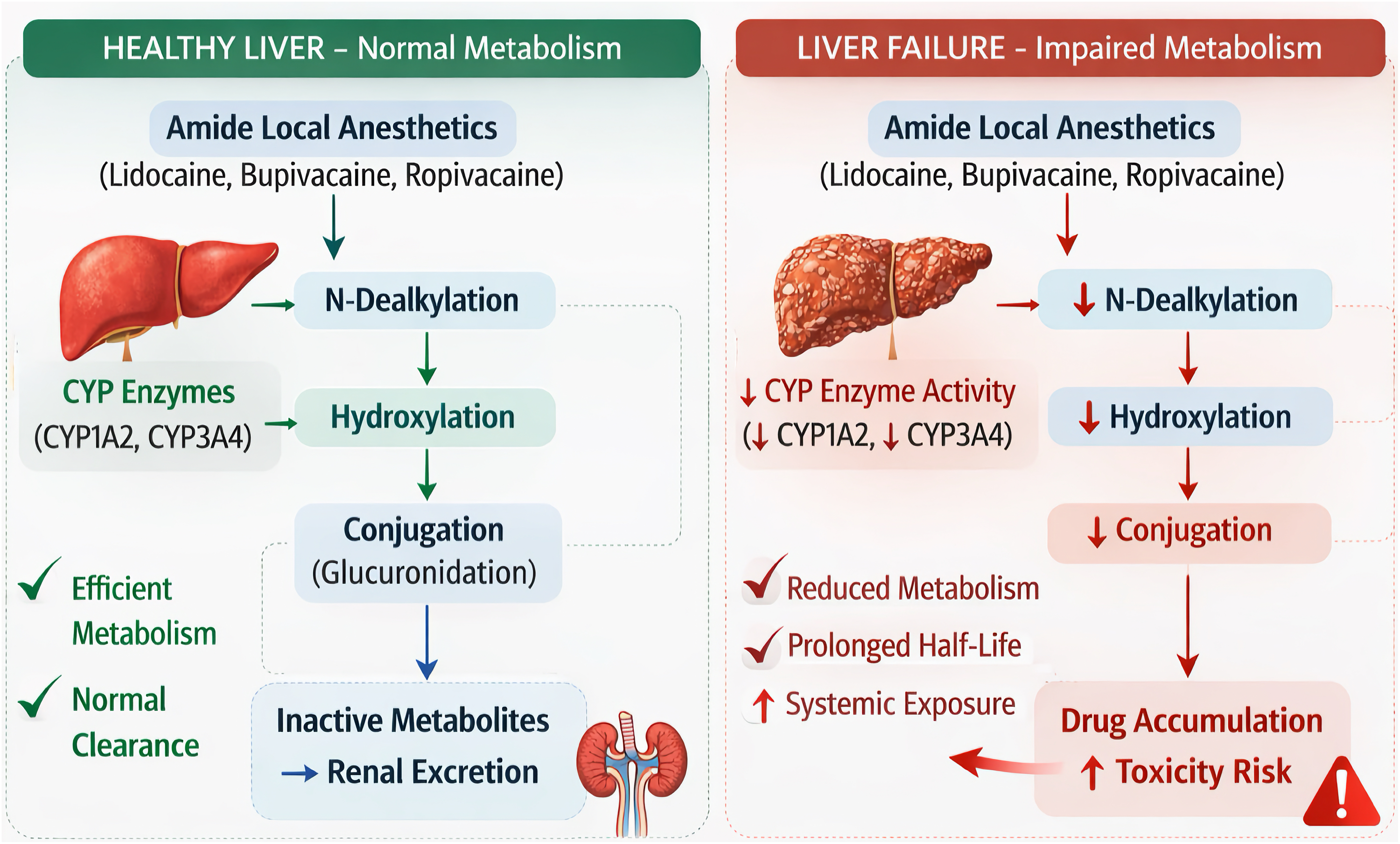
Biochemical pathway of local anesthetic metabolism - healthy liver versus liver failure.
Liposomal bupivacaine, otherwise known as EXPAREL (Pacira Pharmaceuticals, Inc., Brisbane, CA) is a sustained-release local anesthetic that has gained popularity as a non-opioid modality for pain management. The Food and Drug Administration has currently approved this product for local infiltration including fascial plane blocks, interscalene brachial plexus block, adductor canal block, and popliteal-sciatic nerve block. Pharmacokinetic data obtained in patients undergoing bunionectomy with liposomal bupivacaine infiltration shows that the mean plasma bupivacaine concentration shows a steady track over the course of multiple days, but that the peak concentration is less than half that of an equivalent dose of plain bupivacaine. 11
Pharmacodynamics
A patient is at risk for LAST when free plasma concentrations exceed neural and myocardial buffering. Modern reviews reveal that bupivacaine's tighter, slower-dissociating sodium-channel binding results in greater cardiotoxic potential relative to ropivacaine.12,13 Cirrhosis increases free drug and slows elimination and consequently, standard doses can yield substantially higher unbound concentrations than in healthy patients.1–3 In 2019, the first published report of 20% lipid emulsion (Intralipid) rescue following liposomal bupivacaine exposure described a patient undergoing liver resection for hepatocellular carcinoma who developed LAST after local infiltration with a bupivacaine–EXPAREL admixture. Despite receiving a dose within the manufacturer's recommended limits, the patient experienced profound hypotension and refractory arrhythmias unresponsive to aggressive vasopressor therapy. 14 Although this case study underscores the heightened risk of LAST in this patient population, it simultaneously demonstrates that Intralipid is an effective treatment even in this context.
Multimodal Pain Management
Multimodal pain management should be utilized even in patients with higher comorbid states such as hepatic failure. Non-opioid options for transplant recipients discussed in a landmark review in 2020 outline seven main categories of medications: acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, NMDA antagonists (ie ketamine), intravenous lidocaine, alpha-2 agonists (ie dexmedetomidine), and local anesthetics delivered via surgical infiltration or by regional anesthesia technique. 15 The degree of postoperative pain for major abdominal surgery is high, and therefore opioids can also be an integral part of the multimodal regimen. A recent survey revealed that intravenous hydromorphone is the most commonly used opioid for living donor hepatectomy. 16 In the same survey, the most common regional anesthesia technique employed was the transversus abdominis plane (TAP) block.
Outcomes
Caution is warranted when offering regional anesthesia in patients with hepatic failure. However, there are scenarios in which benefits outweigh risks, such as when optimizing a pain management regimen for patients undergoing liver hepatectomy or liver transplantation. In the regional anesthesia literature, a high-volume transplant center in Korea was able to demonstrate enhanced analgesia when a TAP block was performed on patients undergoing living donor hepatectomy. In 80 patients, this anesthesia group administered a total of 40 cc 0.2% ropivacaine in the TAP. 17 Within this same recent timeframe, a novel regional anesthesia technique, the external oblique intercostal (EOI) block, was first described in 2021. 18 Local anesthetic is delivered superficial to the sixth rib, targeting somatic nerves of the abdomen as they anteromedially from the axilla (Figure 2). A recent randomized controlled study demonstrated reduced opioid consumption when an EOI block was performed on 70 patients undergoing open hepatectomy at a large hospital system in China. These patients each received a total of 30 cc of 0.375% ropivacaine. 19 Both the TAP block and the EOI block appear to have comparable pain control outcomes in living liver donor patients when delivered at a volume of 40 cc of 0.25% bupivacaine in a prospective randomized trial. 20 Practically, for these cases, the location and length of the surgical incision below the costal margin may distort the abdominal anatomy, making the EOI block technically easier to perform when compared to a subcostal TAP block.

A. The external oblique intercostal (EOI) block. The ultrasound probe is placed in a parasagittal orientation along the anterior axillary line, as indicated by the green vertical line, and the expected area of analgesia is outlined in pink. 53 × 41 mm (300 × 300 DPI).
Practical Considerations
Local anesthetic absorption from the block site into the serum is dependent on the degree of vascularity in that anatomical region. More vasculature at the site results in faster uptake and a higher peak serum concentration. Anatomical sites with the highest to lowest uptake for common regional nerve block sites are as follows: intercostal > brachial plexus > epidural > femoral > sciatic > subcutaneous/fascial plane. 21 This pattern of uptake may explain the relatively safe profile of recent controlled trials in which fascial plane blocks are performed in the setting of living donor hepatectomy.
When a fascial plane block is performed, a large dose of local anesthetic is quickly administered. For single shot injections, peak serum concentrations typically occur within 20-45 min. With continuous infusions, such as intravenous lidocaine, local anesthetic concentrations reach a steady state over several hours, and with impaired hepatic metabolism, the plateau concentration rides higher. Fascial plane techniques often use larger volumes over broad surfaces – peaks may be lower, but total exposure, as indicated by area under the curve, can be greater and accumulated during continuous nerve catheter infusions. 8
Differences in the properties of each local anesthetic may guide selection based on clinical scenarios. Ropivacaine has lower cardiotoxic potential versus bupivacaine and therefore is favored for large-volume or continuous catheter techniques in high-risk patients. 12 Bupivacaine is potent and has long analgesic duration but should be avoided when high total doses are needed in patients with advanced organ dysfunction. When used, extra attention should be made regarding the timing of doses and the level of monitoring after administration. Lidocaine and mepivacaine are useful for small-volume single injection, but the high-extraction properties of these local anesthetics warrant an adjustment of total dosing with hepatic blood flow is reduced.2,3 Caution should be exercised with bilateral fascial plane blocks and total dose of local anesthetic per kilogram of ideal body weight should be considered.
Practical dosing and guidance of local anesthetic administration in patients with hepatic dysfunction is unavailable, although statements have been made by larger medical organizations (Table 1). The degree of hepatic dysfunction, as quantified by the Model for End Stage Liver Disease (MELD), may guide a dose-dependent reduction in the local anesthetic dose when a regional block technique is selected. For example, a patient with a low MELD (<11) would be considered to have well-compensated hepatic disease, a moderate MELD (11-18) suggests clinically significant decompensation, and a high MELD (>18) is associated with substantial short-term mortality and the need for expedited liver transplantation.
22
An example of a conservative dosing strategy is outlined here:
Low MELD (<11): no reduction in local anesthetic dose Moderate MELD (11-18): 25% reduction in local anesthetic dose High MELD (>18): 50% reduction in local anesthetic dose
Statements Provided by Organizations Regarding Local Anesthetic Dosing in Patients with Hepatic Impairment.

These recommendations, generated by the authors of the article, are intentionally conservative. While high doses of local anesthetic have consistently been reported as safe when fascial plane block techniques are used, reducing the total dose offers an additional margin of safety to minimize the risk of LAST.
The MELD score correlates with drug clearance, though no formal guidelines exist for local anesthetic dosing that is directly associated with it. Evidence supporting MELD as a pharmacokinetic predictor includes:
Our dosing recommendations should be preferably framed as precautionary recommendations rather than guideline-based, emphasizing the absence of formal pharmacokinetic validation for local anesthetics specifically.
Regional anesthesia techniques are not only guided by local anesthetic pharmacology but are also guided by coagulopathy which is often present in patients with hepatic dysfunction. Neuraxial techniques such as epidural or spinal can potentially provide good pain control for major abdominal surgeries. However, epidural hematoma is a feared complication which has led to lower extremity paralysis. 33 The American Society of Regional Anesthesia (ASRA) has established organizational coagulation guidelines, which direct timing of procedures, anticoagulation medication management, and laboratory study parameters. 34 Block procedures that require a target that is either deep or anatomically incompressible, such as a paravertebral block or lumbar plexus block, should be managed in the same manner as a neuraxial technique. Note that current practice in this decade leans towards fascial plane blocks over neuraxial technique due to anticipated coagulopathy. Common practice for local anesthetic administration during a regional block procedure includes a fractionated injection, aspirating every 3-5 mL to rule out inadvertent intravascular injection, and considering adding low dose epinephrine 1:200,000 as an intravascular marker if appropriate.
Lastly, appropriate monitoring and preparation is warranted for regional block procedures. Patients routinely have monitors mandated by the American Society of Anesthesiologists (ASA), which include noninvasive blood pressure, pulse oximetry, and electrocardiography. 35 A notable number of cases of LAST occur within the first 15 min after a block procedure, and therefore patients should have standard ASA monitors with a qualified anesthesia provider during this time. 36 LAST can manifest as tinnitus, metallic taste or perioral numbness, but in more dire circumstances, have led to seizures and cardiac arrest. 37 Treatment of LAST, as recommended by ASRA, includes intravenous lipid emulsion, benzodiazepines for seizures, and lower dose epinephrine (100 micrograms instead of 1 milligram) during advanced cardiac life support. 38
A Fascial Plane Block Procedure: Technical Steps and Safety Considerations
A representative clinical scenario in which regional anesthesia may be offered to a liver transplant recipient is as follows: a theoretical patient with primary sclerosing cholangitis presents for a deceased-donor liver transplant. The donor graft has been preserved with normothermic machine perfusion, the surgery proceeds uneventfully, vasopressor support is discontinued, and only minimal blood product transfusion is required. The patient qualifies for fast track extubation in the operating room, and the surgeon requests a regional analgesic block to optimize emergence from anesthesia. Practical considerations when planning the block include confirming the patient's weight to guide maximum local anesthetic dosing, discussing the plan with the surgeon, and determining which clinician will perform the block. In liver transplant cases, timing is a unique variable, as the request for regional anesthesia may occur in the middle of the night.
An EOI block may be selected and performed at the conclusion of the procedure with the goal of maximizing the duration of postoperative analgesia. This clinical pathway is typically reserved for patients who have tolerated the operation well and extubation expected within a short timeframe. A visual representation of patient positioning, ultrasound probe placement, and needle insertion can be seen in Figure 3. A commonly used dosing strategy for an EOI block includes 0.25% bupivacaine up to 40 mL, combined with 266 mg (20 ml) of liposomal bupivacaine. For patients with significantly impaired hepatic function, such as those classified with a high MELD score, the total dose may be conservatively reduced by up to 50% to provide an additional margin of safety and minimize the risk of LAST.

A. Patient and provider positioning, ultrasound machine placement, and needle entry for a fascial plane block procedure. Ultrasound probe placement along the anterolateral chest in preparation for an EOI block. The patient is supine position. 48 × 64 mm (600 × 600 DPI). B. Patient and provider positioning, ultrasound machine placement, and needle entry for a fascial plane block procedure. With the ultrasound probe anchored along the paramedian axis, the needle entry is directed from cephalad to caudad. 53 × 71 mm (600 × 600 DPI).
Key safety strategies include meticulous needle visualization under ultrasound guidance, frequent aspiration, and the use of fractionated dosing to minimize the risk of intravascular injection. Maintaining low injection pressure adds an additional layer of protection. 39 Paresthesia-based techniques are not employed in this setting, as the patient is typically anesthetized and the block needle is not directed toward specific peripheral nerves. Finally, lipid emulsion therapy, with Intralipid most commonly used, should be immediately available in the event of LAST.
For documentation and billing purposes, the indication for this block is postoperative pain management performed at the request of the surgeon. Fascial plane blocks are relatively new within the Common Procedural Terminology (CPT) framework; prior to January 2025, the transversus abdominis plane (TAP) block was the only fascial plane block with dedicated CPT codes (64486-64489). As of January 2025, new codes (64466-64469) have been introduced for thoracic fascial plane blocks. 40 Because the EOI block is performed along the anterolateral chest wall, its billing would most appropriately align with this newer 64466-64469 range. However, final code selection may vary by institution and is often determined in consultation with the health system's coding and billing specialists. A summary of practical considerations is provided in a corresponding Table 2.
Key Considerations for Fascial Plane Block Planning.

Conclusion
Administration of local anesthetic in patients with hepatic failure can be risky, but in most cases, beneficial for pain management when delivered as a regional block procedure. Although cases of local anesthetic system toxicity have been reported and discussed, this article also describes recent literature in which effectively large doses of local anesthetic were thoughtfully and safely delivered via fascial plane block with ultrasound guidance.
Regional anesthesia represents an attractive strategy for perioperative analgesia in patients with hepatic failure because it may reduce opioid exposure, preserve respiratory function, and improve postoperative recovery. These benefits are particularly relevant in patients undergoing major hepatic surgery, including liver resection and transplantation, where poorly controlled pain contributes to delirium, respiratory compromise, and prolonged hospitalization.
However, the pharmacokinetic alterations associated with liver dysfunction require careful consideration when selecting local anesthetics and determining dosing strategies. Reduced hepatic clearance, decreased synthesis of albumin and α1-acid glycoprotein, and impaired cytochrome P450 metabolism increase the unbound fraction of amide local anesthetics and prolong their elimination half-life, thereby elevating the risk of local anesthetic systemic toxicity (LAST). These effects are compounded by acidosis, low cardiac output, and sarcopenia, which further narrow the therapeutic window.
Fascial plane blocks, including the transversus abdominis plane (TAP) block and external oblique intercostal (EOI) block, are particularly appealing in this population. Compared to neuraxial techniques, they avoid the risks of epidural hematoma in coagulopathic patients while providing effective somatic analgesia. The relatively low vascularity of fascial plane injection sites results in slower systemic absorption and lower peak plasma concentrations compared to intercostal or brachial plexus blocks. The randomized controlled trials discussed in this review demonstrate that these techniques can be performed safely with standard local anesthetic doses, supporting their role in multimodal analgesia for hepatic surgery.
Dosing should be individualized according to the severity of liver disease, with consideration of MELD-based dose reductions as a precautionary strategy. Safety measures—including ultrasound guidance, fractionated injection with frequent aspiration, and immediate availability of lipid emulsion therapy—remain essential components of safe practice.
Future studies are needed to better define the pharmacokinetic profiles of local anesthetics in advanced liver disease and to validate dosing strategies that balance analgesic efficacy with patient safety. Prospective pharmacokinetic trials correlating MELD scores with local anesthetic clearance would provide the evidence base necessary to develop formal dosing guidelines for this vulnerable population.
Abbreviations
ESP - erector spinae plane
PENG - pericapsular nerve group
EOI - external oblique intercostal
TAP - transversus abdominis plane
MELD - Model for End Stage Liver Disease
ASRA - the American Society of Regional Anesthesia
ASA - the American Society of Anesthesiologists
CPT - Common Procedural Terminology
Footnotes
Acknowledgements
There were no non-author contributors to this article. Writing assistance was provided by Chat GPT 5.0, specifically with grammar and syntax edits, as well as to ensure proper format of references in the AMA Manual of Style. Image development in Figure 1 was created by Chat GPT 5.0 to enhance visual effect.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
A stock photo from Canva was used for the underlying chest image in Figure A, and therefore copyright was not required. In Figure B, the image was obtained by performing an ultrasound scan on one of the authors (MT), and therefore copyright permission was not required.
Author Contributions
Montather O. Taheer (MOT) provided the initial literature search, and helped write and edit the entire manuscript.
Amanada M. Kleiman (AMK) helped write and edit the entire manuscript.
Hari K. Kalagara (HKK) helped write and edit the entire manuscript.
Bryant W. Tran (BWT) helped write and edit the entire manuscript, and provided the edits necessary for final submission of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors do not have any financial disclosures or conflicts of interest related to this manuscript.