
Abstract
Background
Flexible bronchoscopy (FB) has become an essential diagnostic and therapeutic tool in pediatric intensive care units (PICUs). Despite increasing adoption, comprehensive data on FB's current use, clinical impact and safety in critically ill children, particularly those supported by extracorporeal membrane oxygenation (ECMO), remain limited. We aimed to describe the utilization, findings, microbiological yield and complications of FB in critically ill pediatric patients, including its diagnostic and therapeutic applications and associated physiologic effects.
Methods
This retrospective cohort study included all children aged 0–18 years who underwent FB in a quaternary PICU between January 2019 and December 2024. Data were abstracted from the electronic medical record and analyzed descriptively. Physiologic variables before and after bronchoscopy were compared using paired differences (Δ = post − pre).
Results
A total of 179 patients underwent 246 bronchoscopies. The median age was 61 months (IQR 17-172), and the median time from PICU admission to bronchoscopy was 4 days (IQR 1-11). All patients were mechanically ventilated, and 26% were supported with ECMO. The most frequent indications were evaluation of infection (30.3%), focal imaging abnormalities (25.0%), and surveillance bronchoscopy (15.4%). Increased airway secretions were observed in 50% of procedures. Airway plug removal (22.8%), bronchoalveolar lavage (20.7%), and Dornase alfa instillation (7.7%) were the most common interventions. Multiple findings and interventions often occurred during a single procedure. Concordance between bronchoscopic and non-bronchoscopic lavage cultures was moderate, with highest agreement for Pseudomonas aeruginosa (67%) and Candida (100%). Complications were infrequent: minor bleeding (4.9%) and transient desaturation (4.5%) were most common; no pneumothorax or mortality occurred. Physiologic parameters showed minimal change post-procedure.
Conclusions
Flexible bronchoscopy is a safe and versatile diagnostic and therapeutic procedure in the PICU, including among ECMO-supported patients. The stable physiologic profile and low complication rate support its continued integration into multidisciplinary critical care practice.
Introduction
Flexible bronchoscopy (FB) has become an indispensable diagnostic and therapeutic tool in pediatric respiratory medicine. Since its introduction into critical care practice several decades ago, FB has been increasingly used in the pediatric intensive care unit (PICU
Multiple studies have demonstrated that FB can be safely performed in critically ill children, including those receiving mechanical ventilation.8–11 Reported complication rates are generally low, with transient desaturation and minor bleeding being the most frequent events.2,12 However, most available evidence are derived from single-center or indication-specific cohorts, and data describing procedure-related physiologic changes, therapeutic yield, and safety in high-acuity subgroups such as patients supported with extracorporeal membrane oxygenation (ECMO) remain limited.13–15 Furthermore, although non-bronchoscopic BAL is occasionally used as an alternative sampling method, the concordance between bronchoscopic and non-bronchoscopic techniques in the PICU is not well established.16,17
Given the increasing complexity of critically ill pediatric populations and the expanding interventional scope of FB, contemporary data are needed to determine its current use, clinical yield, and safety profile in modern PICU practice. This study was aimed to characterize the use of FB in the PICU setting, focusing on patient characteristics, procedural indications, therapeutic applications, and associated adverse events.
Methods
Study Design, Setting and Population of Interest
We conducted a retrospective cohort study in the 41-bed quaternary PICU at The Hospital for Sick Children (SickKids), Toronto. The study included critically ill children between the ages of 0–18 years, admitted to PICU between January 1, 2019 and December 31, 2024, and underwent FB during their admission. This study was approved by the SickKids institutional research ethics board (SickKids 3513) and procedures to conduct this study were followed in accordance with the ethical standards of the Helsinki Declaration of 1975. All reporting was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 18
Procedure and Practice
FB in our unit is part of an intensivist-led program and all bronchoscopy was performed by trained pediatric intensivists. Sedation was provided according to clinical discretion and commonly included ketamine, fentanyl, and/or propofol administered alone or in combination. Rocuronium was the preferred neuromuscular blocking agent and was used in most cases; it was withheld when adequate sedation allowed the procedure without paralysis or when dynamic airway assessment during spontaneous breathing was required. Procedures were performed using reusable bronchoscopes (Olympus®, Tokyo, Japan) and single-use flexible bronchoscopes (Ambu® aScope™ and GlideScope® systems). Bronchoscope size was selected based on advanced airway tube diameter. Dornase alfa instillation was used in selected cases as a therapeutic adjunct for thick airway mucus plugging at the discretion of the treating clinician and often where previous BAL demonstrated neutrophils. Non-bronchoscopic BAL was performed using the syringe-and-catheter technique. 18
Data Acquisition and Management
Data were abstracted from the electronic medical record (EMR) and entered into a secure research database. Extracted clinical information included patient demographics, primary diagnosis, type of respiratory support and duration of support. Patient transfers between hospital units and discharge times were captured electronically. Laboratory data including blood gas analyses and electrolyte values were extracted directly from the EM.Records of blood transfusions as well as all microbiological results from bronchoscopic and non-bronchoscopic BAL samples were also retrieved. Radiological reports of chest x-rays were also directly abstracted. Vital signs (heart rate, respiratory rate, temperature, and oxygen saturation) were collected for the 24-h periods before and after each bronchoscopy and the maximum or minimum value within each window was extracted to account for variability in retrospective physiologic recordings.
A standardized bronchoscopy procedure note within the EMR served as the primary source for data on specific elements of the procedure and operator-documented complications. Additional information on bronchoscopy findings, therapeutic interventions, and post-procedure physiologic changes were obtained from physician notes documented in the EM.These included descriptive observations of airway appearance, secretion characteristics, complications, and therapeutic maneuvers such as lavage, suctioning, and instillation of medications. Data on procedure-related adverse events, including oxygen desaturation, bleeding, hypotension, and airway trauma, were abstracted directly from operator documentation. The severity of bleeding was categorized using the Nashville Bleeding Scale. 19 When multiple sources contained duplicate or conflicting data, physician notes were considered the reference standard. Finally, physician notes were reviewed alongside respiratory therapist (RT) documentation to assess consistency and concordance in reporting procedure-related adverse events and physiologic changes.
Outcomes
The primary outcome was to describe the use and clinical characteristics of FB performed in the PICU, including patient demographics, procedural indications, and patterns of respiratory support at the time of bronchoscopy.
Secondary outcomes included procedural characteristics (such as timing from ICU admission, bronchoscope size, and indication), therapeutic interventions performed during bronchoscopy (eg, BAL, airway plug removal, Dornase alfa instillation), and the microbiological yield of bronchoscopic versus non-bronchoscopic lavage samples. Additional secondary outcomes included procedure-related adverse events, radiographic changes within 24 h post-procedure, and physiologic parameters recorded before and after bronchoscopy. Concordance between physician and RT documentation of adverse events was also evaluated.
Statistical Analysis
Demographic, clinical, and procedural characteristics, as well as primary and secondary outcomes, were summarized using frequencies and percentages for categorical variables, means and standard deviations (SD) for normally distributed continuous variables, or medians and interquartile ranges (IQR) for skewed distributions. Bronchoscopy findings, interventions, and complications were presented as proportions of total procedures. Concordance between paired data sources (eg, physician vs RT documentation) was assessed descriptively. Physiologic variables before and after bronchoscopy were analyzed using paired differences (Δ = post − pre) and reported as medians with IQRs. As per unit protocol, desaturation is defined as an SpO2 < 88%. To further characterize these events, we examined changes in SpO2, FiO2, and mean airway pressure (MAP) immediately before and after bronchoscopy for cases in which intra-procedural desaturation was documented. All analyses were performed using R software, version 4.1.0 (The R Foundation for Statistical Computing, Vienna, Austria). No imputation was applied for missing data.
Results
A total of 179 patients admitted to the PICU between January 2019, and December 2024 underwent 246 bronchoscopies. The median age at the time of bronchoscopy was 61 months (interquartile range [IQR] 17-172), and the median weight was 23.2 kg (IQR 12.9-66.8). The median ICU length of stay was 15 days (IQR 7-29). The most common underlying medical conditions were oncological disorders (21.3%), pneumonia (14.9%), respiratory system disease (14.9%), and lung transplant (13.8%). All patients were receiving invasive mechanical ventilation, and just over a quarter (26%) were supported with ECMO. The median fraction of inspired oxygen (FiO2) before bronchoscopy was 0.60 (IQR 0.40-1.00) (Table 1). Most patients underwent a single bronchoscopy (n = 136, 76%), while 31 (17%) had two, 6 (3%) had three, and the remaining 6 patients (3%) underwent four or more procedures during the study period.
Patient and Bronchoscopy Characteristics.
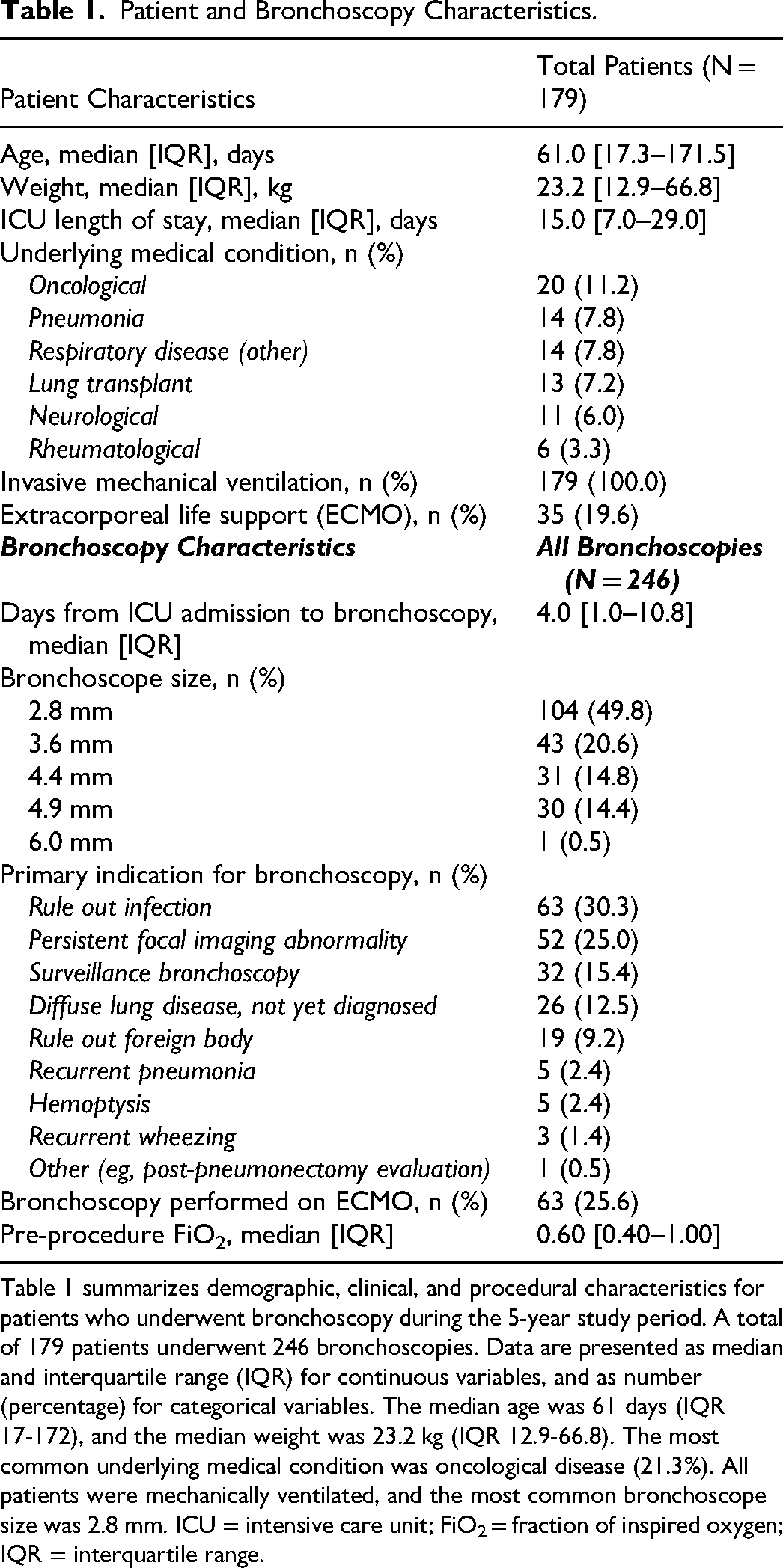
Table 1 summarizes demographic, clinical, and procedural characteristics for patients who underwent bronchoscopy during the 5-year study period. A total of 179 patients underwent 246 bronchoscopies. Data are presented as median and interquartile range (IQR) for continuous variables, and as number (percentage) for categorical variables. The median age was 61 days (IQR 17-172), and the median weight was 23.2 kg (IQR 12.9-66.8). The most common underlying medical condition was oncological disease (21.3%). All patients were mechanically ventilated, and the most common bronchoscope size was 2.8 mm. ICU = intensive care unit; FiO2 = fraction of inspired oxygen; IQR = interquartile range.
Bronchoscopy Characteristics, Interventions and Findings
The median time from PICU admission to bronchoscopy was 4 days (IQR 1-11) and half of all bronchoscopies were done using a size 2.8 mm bronchoscope. The most frequent indications were evaluation of infection (30.3%), assessment of persistent focal imaging abnormalities (25.0%), and surveillance bronchoscopy (15.4%). Less common indications included evaluation of diffuse lung disease (12.5%), suspected foreign body (9.2%), recurrent pneumonia (2.4%), and hemoptysis (2.4%). (Table 1) Increased airway secretions were the most frequent finding, observed in half of all procedures (50%). No abnormal findings or therapeutic interventions were documented in one-third of bronchoscopies (33.3%). Removal of airway plugs was performed in 22.8% of procedures, and BAL in 20.7%, and dornase alfa (Pulmozyme) instillation in 7.7%. Airway collapse was reported in 4.9% of bronchoscopies and bloody secretions in 1.2% (Figure 1). Multiple findings and interventions often occurred during a single procedure. Common combinations included bloody or increased airway secretions (51.2%) increased secretions with removal of airway plugs (8.5%) and BAL with increased secretions (8.5%). Additional multi-component combinations included increased secretions with Dornase alfa instillation and plug removal (3.3%) and BAL with increased secretions and plug removal (2.8%). More complex patterns, such as concurrent BAL, Dornase alfa instillation, bloody or increased secretions, and plug removal, were rare (<1%) (Figure 1).
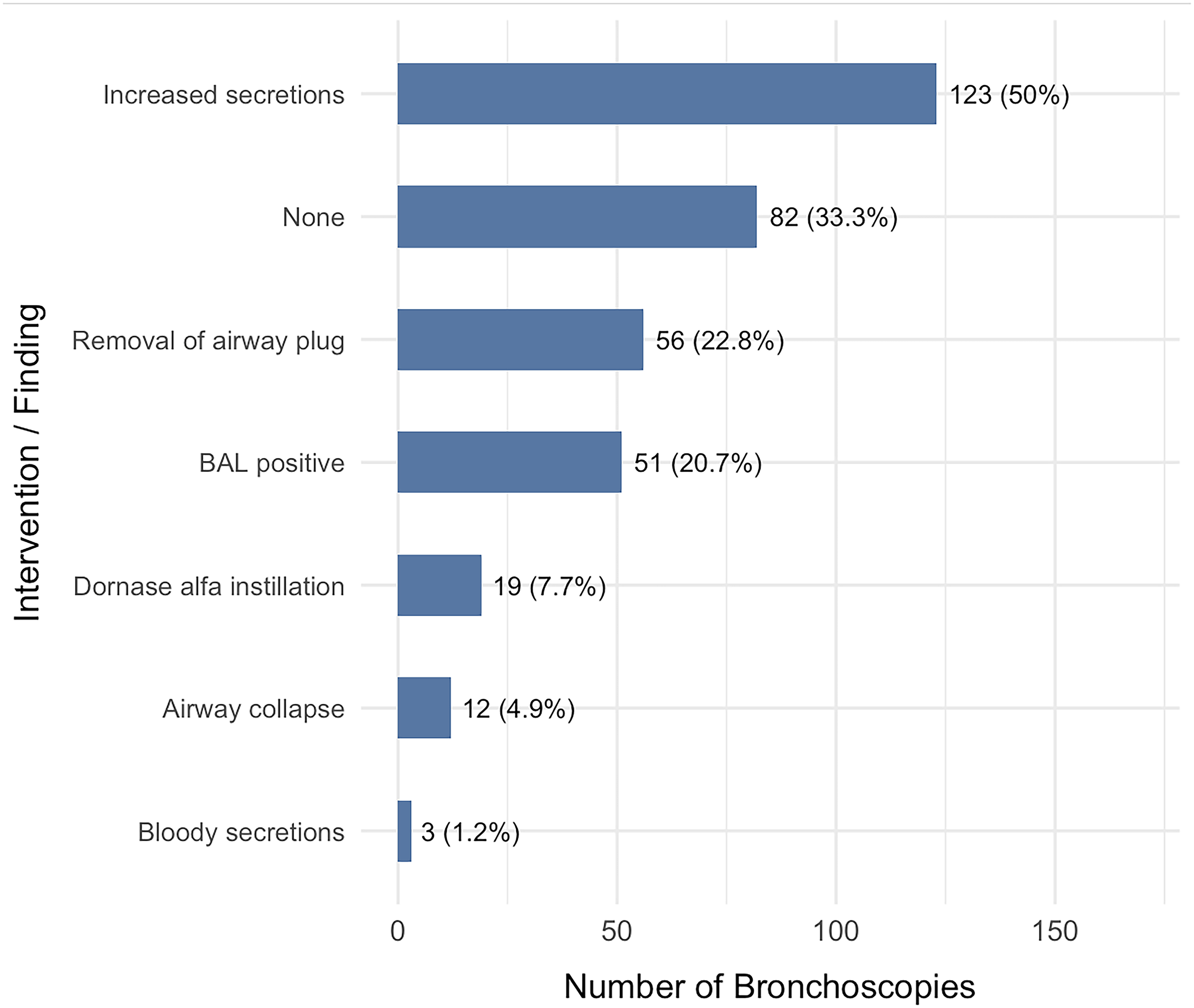
This Figure Summarizes the Therapeutic Interventions and Notable Findings Observed During Bronchoscopies Performed in the Study Cohort. Bloody or Increased Airway Secretions Were the Most Common Finding (51.2%), Followed by Procedures with no Therapeutic Intervention or Abnormal Findings (33.3%). Removal of Airway Plugs Occurred in 22.8% of Bronchoscopies, Bronchoalveolar Lavage (BAL) was Performed in 20.7%, Dornase Alfa was Instilled in 7.7%, and Airway Collapse was Identified in 4.9% of Procedures. Categories are not Mutually Exclusive; Individual Bronchoscopies Could Involve Multiple Interventions or Findings. BAL = Bronchoalveolar Lavage.
Microbiological Concordance
Among paired samples with results from both bronchoscopic and non-bronchoscopic BALs, overall concordance between sampling techniques was moderate. The highest within-category agreement was observed for Candida (100%, n = 5), Blastomyces (100%, n = 12), Klebsiella (69%, n = 18), and Pseudomonas aeruginosa (67%, n = 24). Concordance was lower for Enterobacter (46%, n = 6) and Staphylococcus aureus (60%, n = 3). Most discordant results occurred when non-bronchoscopic BAL samples grew other organisms (21%, n = 13) or mixed bacterial flora, whereas bronchoscopic BALs yielded a single bacterial isolate (Figure 2). Across all positive BAL results Pseudomonas aeruginosa was the most frequently identified organism. (Supp table 2).
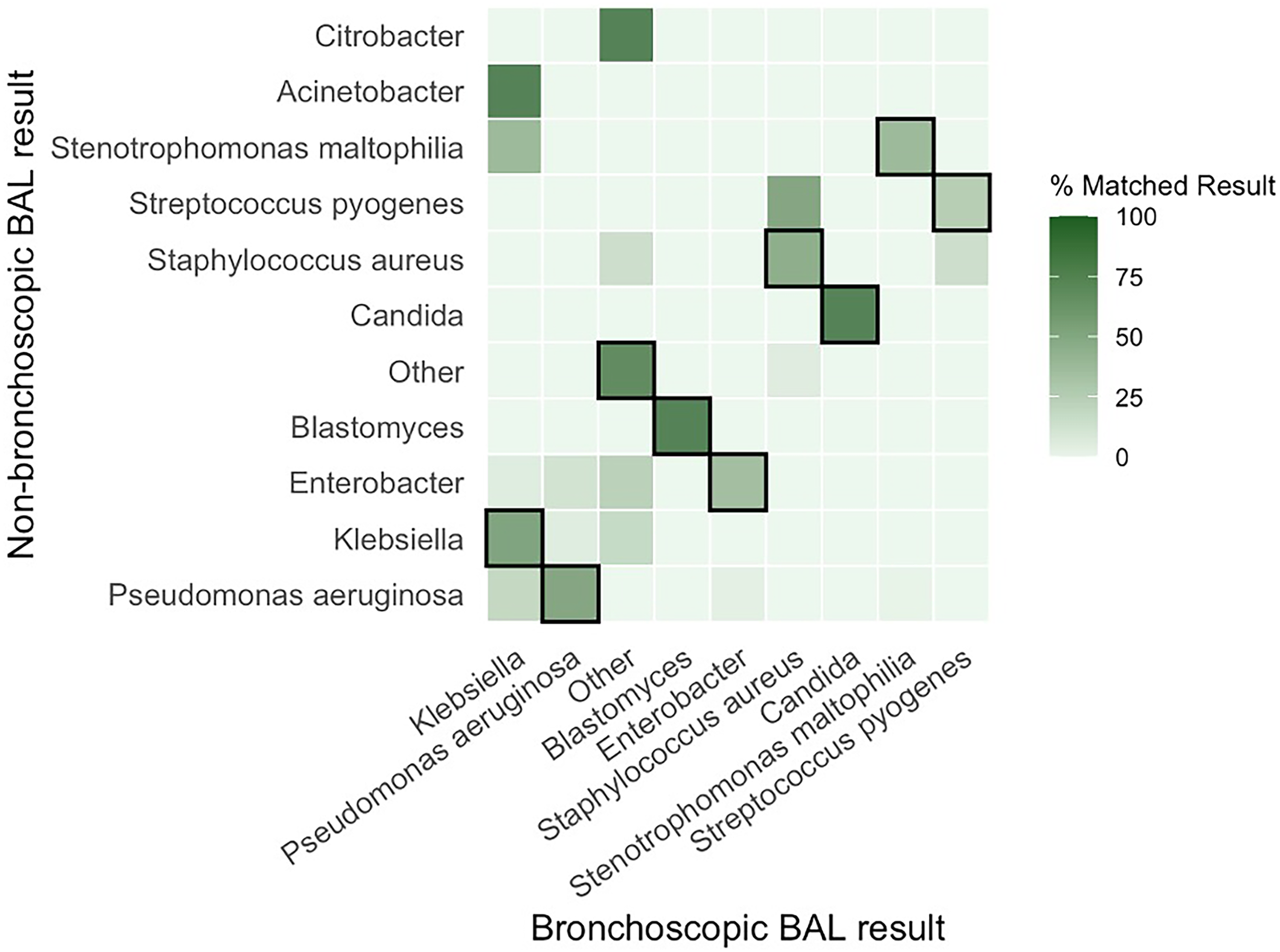
Concordance Between Bronchoscopic and Non-Bronchoscopic BAL Microbiology Results. Figure 2 is a Row-Normalized Heatmap Comparing Organisms Isolated from Paired Bronchoscopic and Non-bronchoscopic BAL Samples. Each Cell Represents the Percentage and Number of Cases for a Given Non-Bronchoscopic Result (row) and Bronchoscopic Result (column). Darker Indicates Higher Concordance. Diagonal-Outlined Cells Indicate Exact Matches Between Methods.
Complications of Bronchoscopy
Despite frequent therapeutic interventions, bronchoscopy was generally well tolerated. Procedure-related complications were uncommon, with bleeding (4.9%) and oxygen desaturation (4.5%) being the most frequent. Less common complications included mechanical airway obstruction attributed to the bronchoscope (1.6%), hypotension (1.2%), airway trauma (0.8%), and bradycardia (0.4%). No episodes of pneumothorax, cardiac arrest or procedure-related mortality were recorded (Figure 3). Bleeding complications following bronchoscopy were predominantly mild, with 67% classified as Nashville Criteria grade 1% and 33% as grade 2; no patients met grade 3 or 4 criteria for airway bleeding. Of the 246 bronchoscopies, 125 (51%) lacked any RT complication note, leaving 121 (49%) encounters with paired physician and RT documentation. Overall agreement was high but largely driven by negative (no-complication) documentation, yielding low κ for most outcomes (Supplementary Figure 1). Chest radiographs obtained within 24 h post-bronchoscopy demonstrated complications in a minority of patients (18%). The most frequent finding was atelectasis or consolidation (14.3%) followed by increased pulmonary infiltrates (4.6%). Other abnormalities, including pulmonary edema (1.3%), pleural effusion (2.9%), subcutaneous emphysema (0.4%), and pneumothorax (0%), were infrequent.
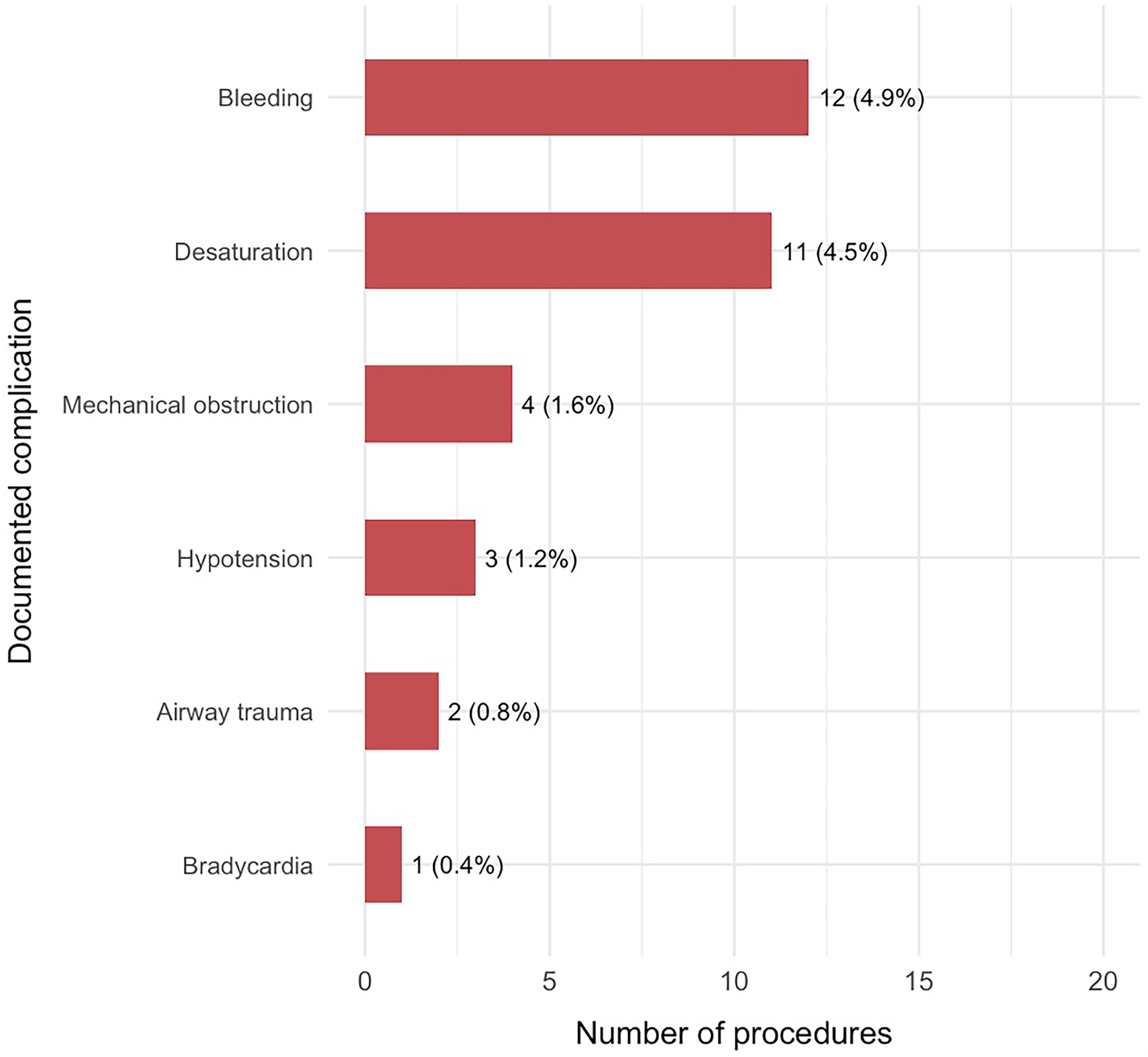
Operator Documented Bronchoscopy Complications Procedure-related Complications Were Uncommon as Demonstrated in Figure 2. The Most Frequently Reported Events Were Bleeding (4.9%) and Oxygen Desaturation (4.5%). Less Frequent Complications Included Mechanical Airway Obstruction (1.6%), Hypotension (1.2%), Airway Trauma (0.8%), and Bradycardia (0.4%). No Episodes of Cardiac Arrest or Procedure-Related Mortality Were Recorded.
Physiologic Changes
Physiologic parameters before and after bronchoscopy demonstrated minimal overall change (Figure 4). Median oxygen saturation (SpO2) remained stable [Δ 0.0 (0.0-0.0)], as did MAP [Δ 0 (–2 to 2) mm Hg], heart rate [Δ 0 (–5 to 1.3) bpm], and temperature [Δ 0 (–0.4 to 0.4) °C]. Fraction of inspired oxygen (FiO2) showed a small, clinically insignificant increase [Δ 0.0 (–0.05 to 0.15)], while respiratory rate demonstrated the greatest variability [Δ 1.0 (–7.0 to 7.5) breaths/min]. Collectively, these findings indicate that bronchoscopy was well tolerated with no appreciable physiologic deterioration following the procedure (Figure 4). Provider-documented desaturation occurred during 11 bronchoscopies. In these cases, SpO2 remained relatively stable pre- and post-procedure, while modest increases in FiO2 and MAP were observed (Supplementary Figure 2).
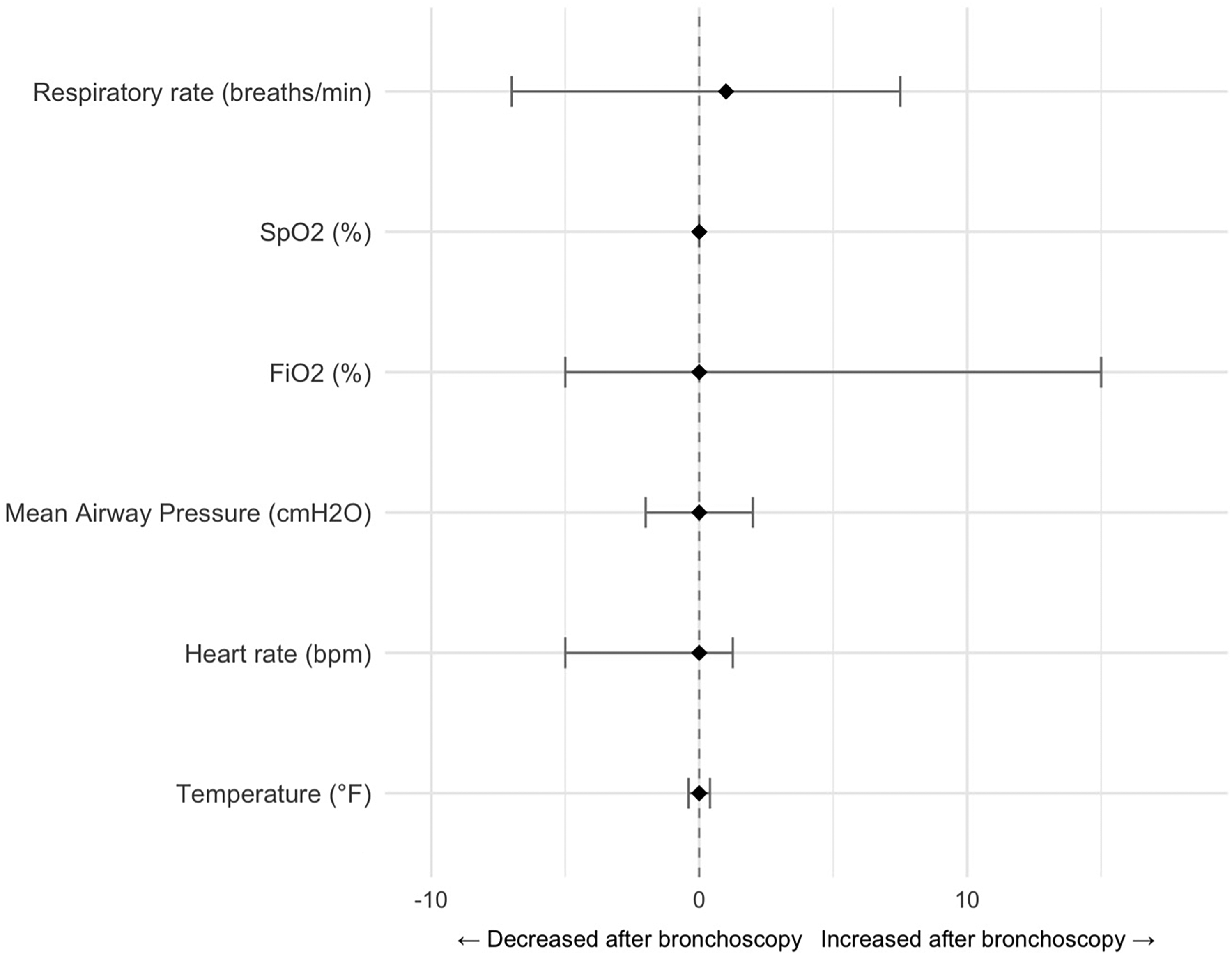
Median Change in Physiologic Parameters Before and After Bronchoscopy. Each Point of Figure 4 Represents the Median Change (Δ = Post − Pre) with Interquartile Range (IQR) for Paired Observations. The Dashed Vertical Line Indicates No Change (Δ = 0). Positive Values Reflect an Increase and Negative Values a Decrease Following Bronchoscopy. Across 199–225 Paired Measurements Per Parameter, Changes Were Small and Not Clinically Significant. FiO2 = fraction of Inspired Oxygen; SPO2 = Saturation of Oxygen.
Discussion
This large single-center study describes the utilization, findings, and safety profile of FB in a heterogeneous cohort of critically ill pediatric patients over a six-year period. FB was widely used for both diagnostic and therapeutic purposes, with infection evaluation, focal imaging abnormalities, and surveillance bronchoscopy representing the most common indications. Despite frequent concomitant interventions including airway plug removal, BAL, and Dornase alfa instillation, bronchoscopy was well tolerated, with low complication rates and no procedure-related mortality. These results reaffirm FB's role as a safe, versatile, and clinically valuable tool in pediatric intensive care, even among the most critically ill patients. Our findings align with prior multicenter and single-center studies demonstrating the safety and utility of FB in the PICU.8,9,11,20,21 The complication rates in our cohort such as bleeding (4.9%), desaturation (4.5%), and mechanical airway obstruction (1.6%), are comparable to or lower than those reported in previous studies, where desaturation occurred in 2%–10% and bleeding in 2%–6% of procedures.2,10,12 Notably, 26% of procedures were performed on patients receiving ECMO, a population typically excluded from earlier series. Our findings extend the recent evidence that FB can be performed safely in ECMO supported children when conducted by experienced teams under close monitoring.13–15,22,23 The median time to bronchoscopy from ICU admission (4 days) and the predominance of diagnostic indications are consistent with prior observations that early FB can provide actionable information and guide therapy in children with unresolved atelectasis, pneumonia, or suspected airway obstruction.1,24,25 The frequency of airway plug removal (22.8%) and BAL (20.7%) in our cohort further supports FB's expanding therapeutic role beyond diagnostic sampling—consistent with the evolving interventional practices described in recent surveys of pediatric pulmonologists.5,6
This study contributes several new insights to the literature on FB in the PICU. First, it provides a comprehensive depiction of the procedural complexity associated with FB in critically ill children. More than half of all bronchoscopies involved multiple concurrent findings or interventions, underscoring that FB in the PICU is rarely a single-purpose procedure. Instead, it frequently combines diagnostic and therapeutic objectives such as simultaneous airway inspection, BAL, and airway clearance within the same session. This multifaceted use reflects the dynamic and integrative nature of FB in modern pediatric critical care
Collectively, these findings bridge a crucial gap between traditional bronchoscopy literature and contemporary practice, where FB serves as both a diagnostic and therapeutic extension of critical care management.2–4 Our results support the continued integration of FB into multidisciplinary ICU management. The low complication rate and stable physiologic profile observed post-procedure suggest that bronchoscopy can be performed safely even in patients receiving high FiO2 or ECMO support, provided that appropriate expertise and monitoring are in place. The data also emphasize the growing therapeutic scope of FB, such as airway clearance and mucolytic instillation, which may reduce ventilator dependence and improve alveolar recruitment. Moreover, the diagnostic precision of bronchoscopic BAL reinforces its role in guiding antimicrobial stewardship and targeted therapy in critically ill children. Along with its strengths, our study has limitations. The retrospective design and incomplete documentation of minor complications likely resulted in some underreporting. In this cohort because bronchoscopies were performed in intubated, mechanically ventilated patients, bronchoscopic findings of airway collapse may be influenced by sedation, the endotracheal tube, and airway inflammation and should not be interpreted as definitive airway malacia but nonetheless highlight the utility of bronchoscopy in identifying areas of airway collapse. Additionally, microbiologic concordance analyses were limited by the small number of paired samples for certain organisms. Our single-center experience may not reflect practices in institutions with different patient populations or procedural expertise. Nevertheless, the study's large sample size, detailed physiologic assessment, and inclusion of ECMO-supported patients enhance its external relevance.
Conclusions
FB in the pediatric ICU is safe, feasible, and diagnostically valuable, even among the most critically ill children. This study expands existing knowledge by providing a detailed characterization of procedural patterns, microbiologic yield, and physiologic tolerance while demonstrating safety in children supported by ECMO. As intensivist-led bronchoscopy becomes increasingly integrated into critical care practice, future multicenter prospective studies could focus on evaluating its impact on outcomes such as duration of ventilation and resolution of infection.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261438400 - Supplemental material for Characterizing Bronchoscopy in Pediatric Critical Care: A Cohort Analysis of Practice and Outcomes
Supplemental material, sj-docx-1-jic-10.1177_08850666261438400 for Characterizing Bronchoscopy in Pediatric Critical Care: A Cohort Analysis of Practice and Outcomes by Melany Gaetani, Thitima Sirimontakan, Karthi Nallasamy, Norbert Chin, Katherine Reise and Briseida Mema in Journal of Intensive Care Medicine
Footnotes
Ethical Considerations
This study was approved by the SickKids institutional research ethics board (SickKids 3513) and procedures to conduct this study were followed in accordance with the ethical standards of the Helsinki Declaration of 1975. All reporting was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Consent to Participate
As the data contains retrospectively collected de-identified patient information, the requirement for obtaining individual informed consent was waived by the SickKids institutional research ethics board.
Consent for Publication
Not applicable.
Author Contributions
Katherine Reise (KM), Thitima Sirimontakan (TM), Briseida Mema (BM) contributed to the study conception and design. Melany Gaetnai (MG) and BM conducted data analysis and drafted the manuscript. Norbert Chin, Thitima Sirimontakan (TM), Briseida Mema (BM) were responsible for data collection, cleaning, and literature review. Karthi Nallasamy revised and proofread the manuscript. Melany Gaetani, Thitima Sirimontakan, Karthi Nallasamy, Briseida Mema critically reviewed, edited, and approved the final version of the manuscript. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.