
Abstract
Background
Data regarding the risk of infection related to reusable bronchoscopes, the global drive toward disposable technology and the COVID-19 pandemic have led to an increase in the use and production of single use or disposable bronchoscopes. An in-depth comparison of all available devices has not been published.
Methods
A benchtop comparison of the Ambu®aScopeTM, Boston Scientific® EXALTTM Model B, the Surgical Company Broncoflex© Vortex, Pentax® Medical ONE Pulmo™, and Vathin® H-SteriscopeTM (all 2.8 mm inner dimension other than the Pentax single-use flexible bronchoscope (3 mm)) was undertaken including measurement of maximal flexion and extension angles, thumb force required and suction with and without biopsy forceps. Thereafter, preclinical assessment was performed with data collected including experience, gender, hand size, and scope preference.
Results
The Vathin single-use flexible bronchoscope had the biggest range of tip movement from flexion to extension with and without forceps. The Boston single-use flexible bronchoscope required the maximal thumb force but had the least reduction of tip movement with forceps. The Boston single-use flexible bronchoscope significantly outperformed all other scopes including the standard Pentax scope and was the only scope capable of suctioning pseudo-mucus around the forceps. Although there was no significant difference in preference in the overall group, females and those with smaller hand size preferred the Pentax and males the Broncoflex single-use flexible bronchoscope.
Conclusions
Currently available single-use flexible bronchoscopes differ in several factors other than scope sizes and monitor including suction, turning envelope, and handle size. Performance in the clinical setting will be key to their success.
Introduction
Prior to the COVID-19 pandemic, evidence was gathering regarding the risk of infection and contamination of reusable bronchoscopes.1–9 Principally due to portability, accessibility, and the lack of requirement for cleaning and storage, single use or disposable flexible bronchoscopes (SUFBs) were already popular in operating room (OR) and intensive care units (ICUs).3,10–15 Pulmonologists started using SUFBs prior to the COVID-19 pandemic15–17 and there was an increase thereafter for several reasons including portability and lack of a requirement of staff and personal protective equipment to clean and transport scopes.15,18,19 In parallel, international bodies recommended switching from reusable to single-use devices 20 with the Emergency Care Research Institute listing contamination of scopes as a top 10 health technology hazard. 21
Published data however outside the OR or ICU are limited and again predominated by Ambu® SUFBs due to their release 10 years prior to competitors. 17 No comparison of scope parameters is available. Our center, therefore, compared SUFBs available to the European market in mid-2021 to help bronchoscopists decide which SUFB would best suit their practice.
Methods
All SUFBs with CE approval in mid-2021 (Ambu®aScopeTM (“AMBU SUFB”) Boston Scientific® EXALTTM Model B (“ Boston SUFB”), The Surgical Company (TSC) Broncoflex© Vortex (“Broncoflex SUFB”), and Vathin® H-SteriscopeTM (“Vathin SUFB”) were included (Figure 1). A newly developed Pentax® Medical ONE Pulmo™ (“Pentax SUFB”) was also included (CE approval in 2022) (Figure 1). Internal diameter (ID) was 2.8 mm other than the Pentax SUFB (3 mm). Scope measurements such as weight, length, and handle size were recorded.

The single-use bronchoscopes tested from left to right: Pentax® Medical ONE Pulmo™, Ambu® a Scope 4 Large, The Surgical Company Broncoflex© Vortex, Vathin® H-SteriscopeTM Large, and Boston Scientific® EXALTTM Model B.
Assessment included 3 evaluations:
Preclinical evaluation in a low-fidelity airway simulation model Benchtop assessment An assessment of scope suction
Preclinical Evaluation
With institutional ethical approval (UCC-ECM 4 (e) 2021), physicians, surgeons, anesthetists/ICU physicians, and endoscopy nurses with a range of expertise were invited through in-hospital group texts and emails to participate. Participant parameters were recorded including height, gender, hand size, and experience (e-Figure 2).
SUFBs were set up at 5 stations with a low fidelity airway simulator (plastic tubing including a 90° angle (Figure 2) and foam pseudo-tumor (Figure 3). Each station included an experienced bronchoscopist to supervise and assist. Participants with no experience were given a brief demonstration. Participants were rotated and asked to evaluate each SUFB by maneuvering and passing a Boston Scientific® Radial Jaw 4™ 2 mm forceps to biopsy the pseudo-tumor (Supplemental Figure 1). Likert scales (1-5) were used for the evaluation of scope metrics including ergonomics (scope grip, lever, button, and overall comfort), active usage (scope agility, comfort during active use, introducing, passing, and removing forceps, performing biopsy), and over all impression, with a total maximum score of 55 (Supplemental Figure 2).

Simple simulation of airway using plastic tubing and a 90° angle to facilitate basic bronchoscope maneuvering.

Forceps biopsy of a foam “pseudo-tumor” using a single-use flexible bronchoscope down a simple simulated airway with plastic tubing.
Statistical analysis was carried out using SPSS V26.0 (IBM Corp). Bronchoscope metrics (ergonomics, usage, and total score) were analyzed by gender with the independent sample t test and Mann-Whitney U test. The independent sample t test and Kruskal-Wallis test were used to analyze bronchoscope metrics by glove size, experience, and number of scopes performed. The interaction between the bronchoscopist and the evaluator can influence the evaluation scoring and thus to control the interaction a preparation meeting occurred to prevent bias and influence of the trainers at each station.
Benchtop Assessment of Flexion and Extension and Force Required
We compared technical metrics using a custom-built apparatus (Figure 4). Thumb force was measured using a force meter attached to ascertain the force required to flex the SUFB empty and with a forceps extended 15-mm beyond the tip with the forceps always in the closed position.
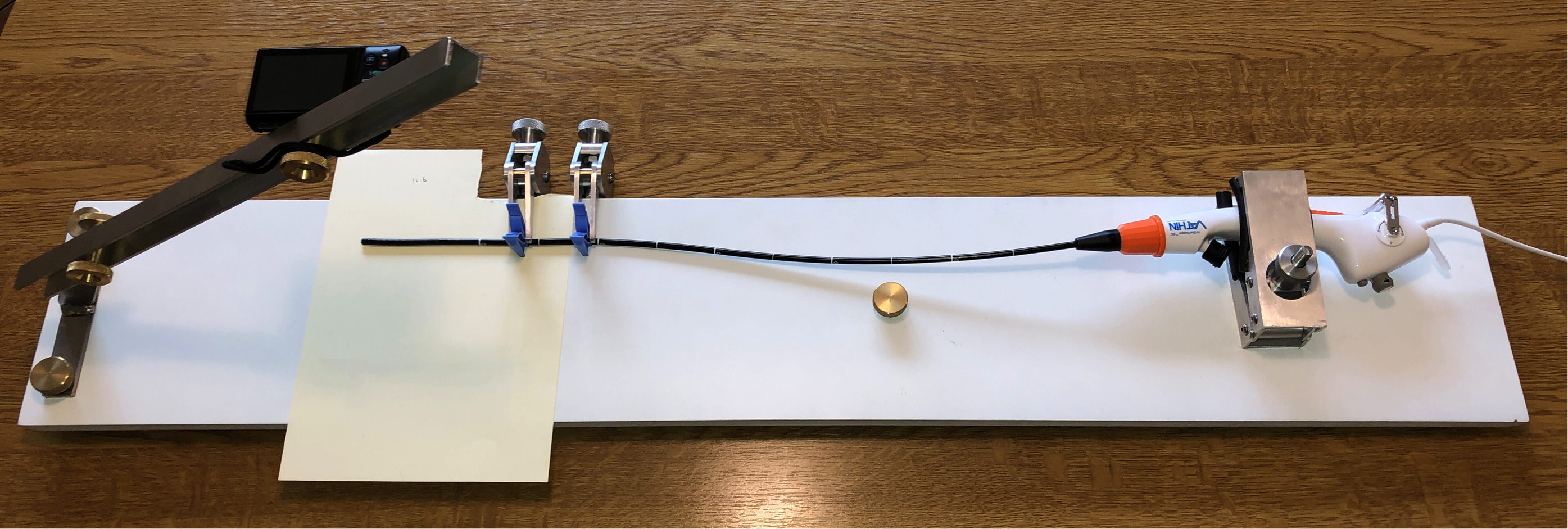
Custom-built measurement apparatus. Fixed distance digital camera. Distal and proximal clamps.
Each SUFB was clamped at its proximal grip with the distal end secured and isolated using 2 individual soft clamps to steady the articulating portion without affecting angulation or function of the SUFB. SUFB was flexed 3 times before testing to account for mechanical lag or stiffness and flexed up and down to maximum angulation (captured using a digital camera perpendicular to scope). These images were subsequently analyzed (Supplemental Figure 3) using computer-aided design software (AutoCad 2014, AutoDesk) (Figure 5A and B). The turning envelope was measured as the diameter of the turning arc relative to the distal end of the articulating portion of the bronchoscope (an imaginary circle the distal end of the bronchoscope creates as it angulates from fully flexed up to fully flexed down. Smaller measurement implies better agility.) Loss or gain of angulation with forceps was compared to vendor-reported specifications.
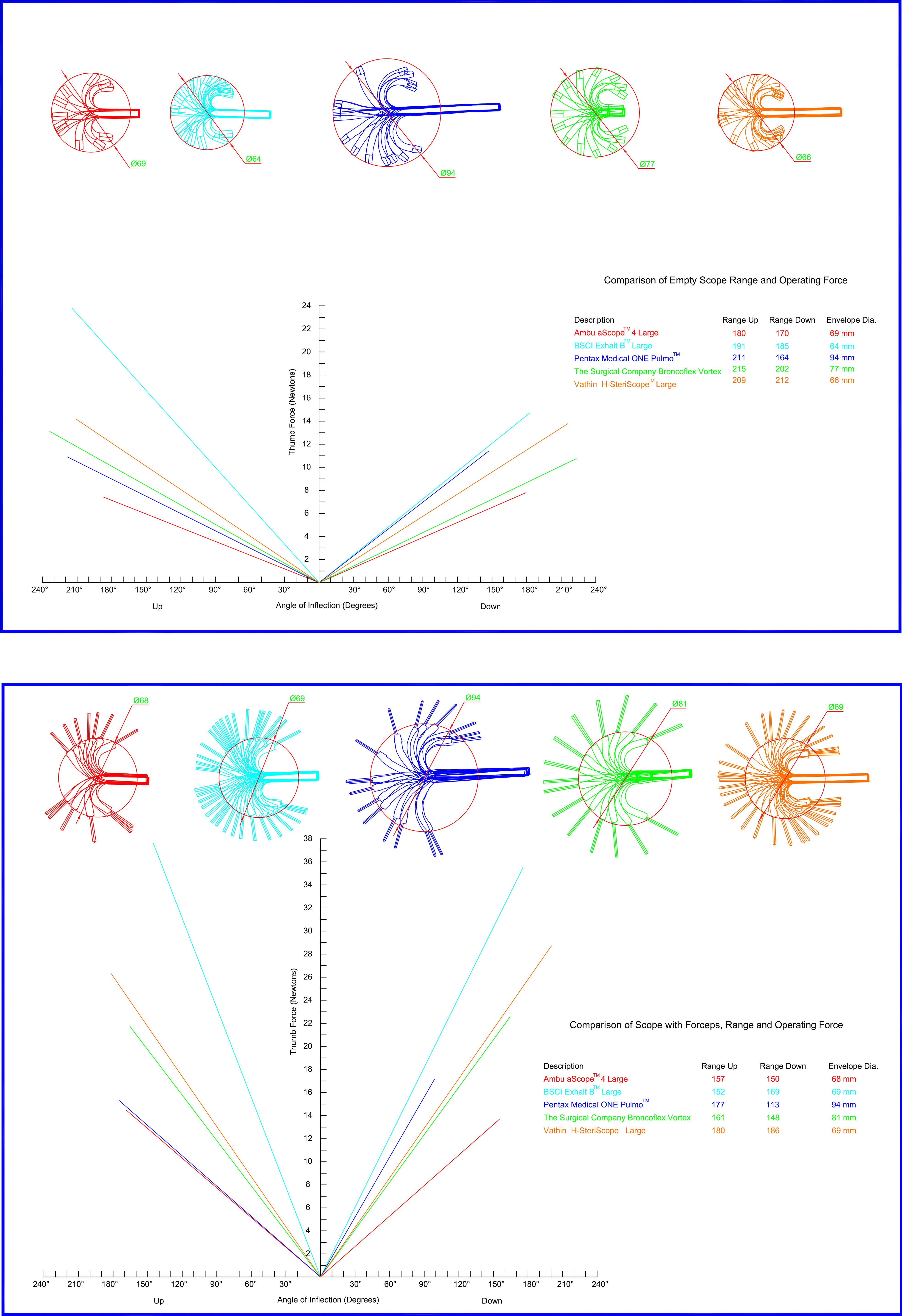
(A) AutoCAD Rendering of all SUFBs demonstrating turning envelope diameter, along with graphical representation of relative activation forces while empty. (B) AutoCAD Rendering of all SUFBs demonstrating turning envelope diameter, along with graphical representation of relative activation forces while accessed with forceps.
An Assessment of Scope Suction
Two new SUFBs from each vendor were compared to a reusable 3.2 mm channel Pentax® EB1970TK™ bronchoscope. An assessment of previously reported preparations to create a “pseudo-mucus” solution was informative in using a 1% guar gum solution.22,23 After completing our assessment, another study was published using a similar “pseudo-mucus” composition.
24
Four scenarios were tested:
0.9% sodium chloride 50 mL without forceps 0.9% sodium chloride 50 mL with forceps Pseudo-mucus 20 mL without forceps Pseudo-mucus 20 mL with forceps
Two trials for each of 2 company scopes were performed (16 suction trials per vendor).
Wall suction was set at 500 mm Hg (66.66 kPa) and therefore below upper limit recommended for each company. Suction was commenced prior to dipping the tip into the fluid and positioning the scope tip so as to not block the distal end by opposing the bottom of the sample bottle. Bending or kinking of suction tubing was avoided. The mean time of 2 trials for each scope was calculated. Results were compared using a 2-way t test with P < .05 considered significant. The forceps were always positioned in the closed position.
Results
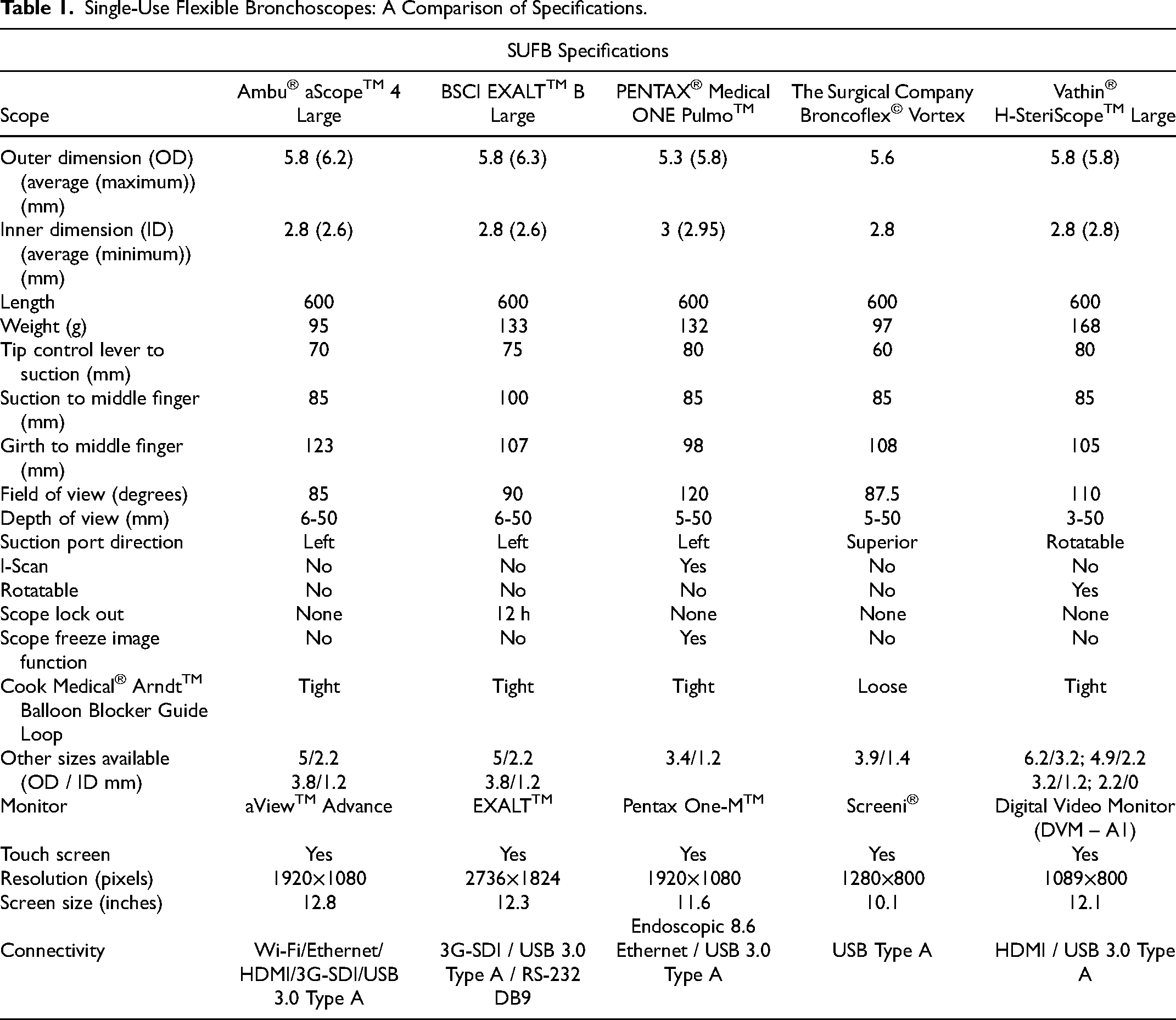
A comparison of a number of scope parameters, monitors, and features is presented (Table 1). The Vathin SUFB was the heaviest, however, had the biggest range of scope sizes and is rotatable. The Pentax SUFB has the smallest handle, has a picture freeze button on the scope handle and i-scan imaging. All scopes have left suction port direction other than the Vathin SUFB (180° angle rotatable) and the Broncoflex SUFB (superior direction- noted that can lead to reduced suction due to kinking of tubing between the suction port and the lavage trap). 25 The Boston SUFB locks out after 12 h. Differences in monitor size, resolution, and connectivity are also highlighted in Table 1.
Single-Use Flexible Bronchoscopes: A Comparison of Specifications.
Preclinical Evaluation: Airway Simulation Model
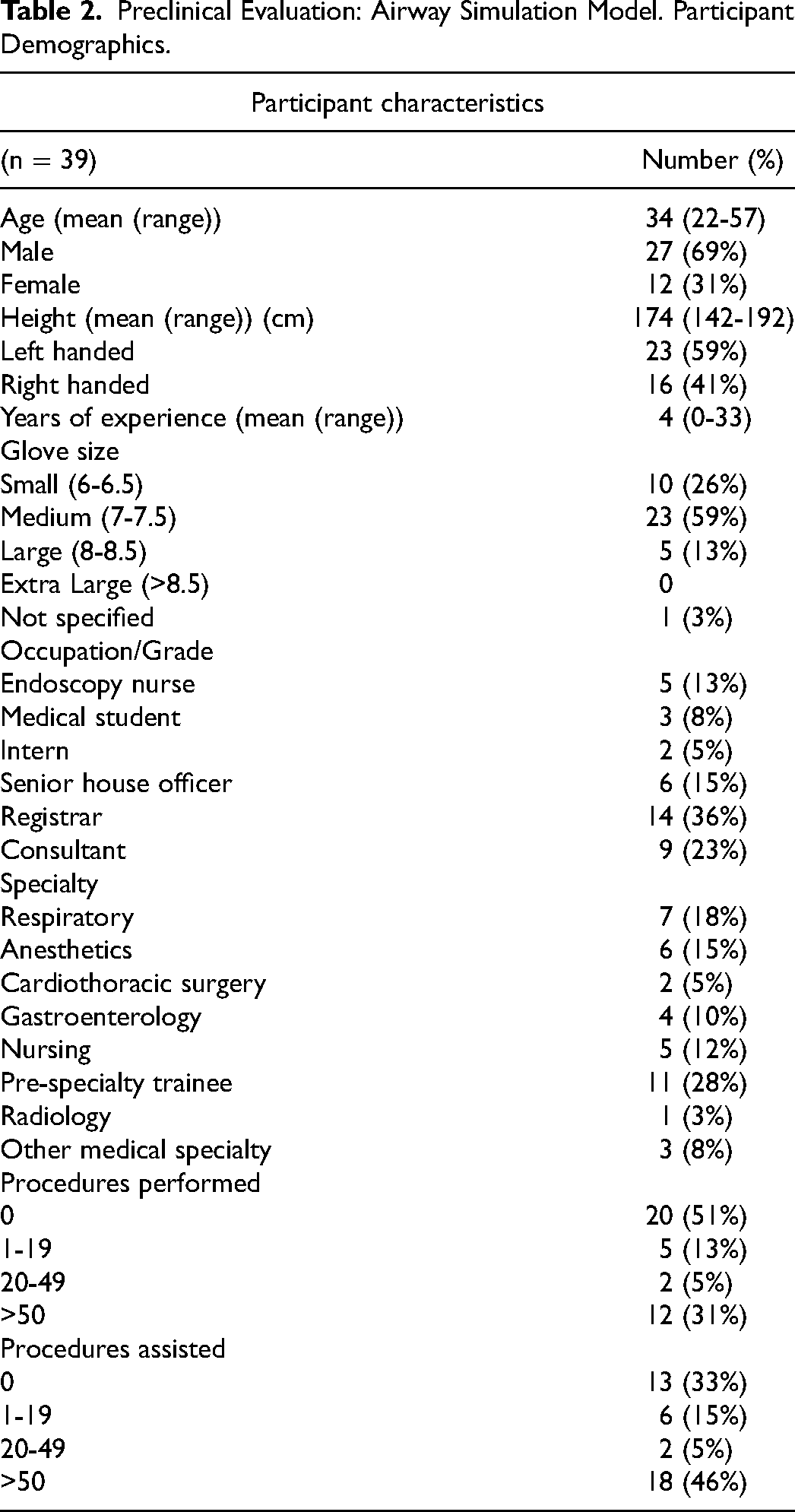
Thirty-nine participants took part including respiratory physicians (n = 7, 2 attendings, 5 fellows (all over 50 bronchoscopic procedures)), anesthetists/ICU physicians (n = 6, 3 attendings, 3 fellows (all over 50 bronchoscopic procedures)), gastroenterologists (n = 4, all endoscopists with 3 having prior bronchoscopy experience), cardiothoracic surgeons (n = 2 (attendings)), and endoscopy nurses (n = 5) (Table 2). Eleven participants were doctors in basic training (28%). Thus, 17/39 (43%) had no prior bronchoscopy experience.
Preclinical Evaluation: Airway Simulation Model. Participant Demographics.
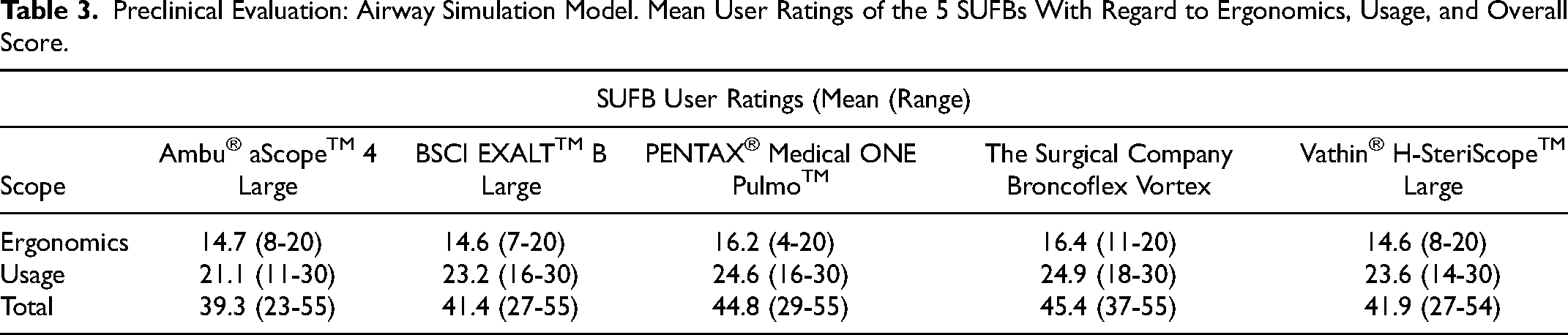
The Broncoflex SUFB was preferred overall with an average score of 45.4/55 including 82.1% for ergonomics and 83% for usage (Table 3). Female participants (n = 12) preferred the Pentax SUFB (P = .042); male participants (n = 27) the Broncoflex SUFB (P = .04) (Supplemental Table 1). Participants with small (n = 10) or medium (n = 23) glove size preferred the Pentax SUFB (P = .017) (Supplemental Table 2). Those with large glove size (n = 5) ranked the Vathin and Broncoflex SUFBs highest (44.4/55; 44/55). Participants with >10 years’ bronchoscopic experience (n = 15) preferred the Pentax SUFB (P = .037). There was no statistically significant difference in preference of SUFBs for the anesthetic group or respiratory physicians, with a trend toward a preference of the Broncoflex over the AMBU SUFB in an analysis of the groups combined (P = .06) (Supplemental Table 3).
Preclinical Evaluation: Airway Simulation Model. Mean User Ratings of the 5 SUFBs With Regard to Ergonomics, Usage, and Overall Score.
Benchtop Assessment
AMBU SUFB had the narrowest field of vision (FOV) and the worst outer diameter (OD) to ID ratio, 6.3 mm to 2.8 mm (Table 1). It was second only to the Vathin SUFB for its turning envelope (69 mm) (Figure 5A, Table 4). The AMBU SUFB required the least mean activating thumb force both while empty (4.15N/100°) and while instrumented (8.65N/100°) (Figure 5A and B, Supplemental Table 4). The Boston SUFB had mid-range specifications for OD, ID, FOV, and angulation. It had the tightest turning envelope encompassing a diameter of 64 mm while empty and 66 mm while accessed with forceps. However, this resulted in significantly poorer performance for thumb force activation, requiring more than twice the activation force of the AMBU SUFB at 9.5N/100° empty and 23.05N/100° when instrumented (Supplemental Table 4). The Pentax SUFB reported the best FOV (120°) and the best OD to ID ratio, 5.3 mm to 3 mm. This however resulted in the widest measured turning envelope, encompassing a diameter of 94 mm.
Comparison of Single-Use Flexible Bronchoscopes: Angulation.
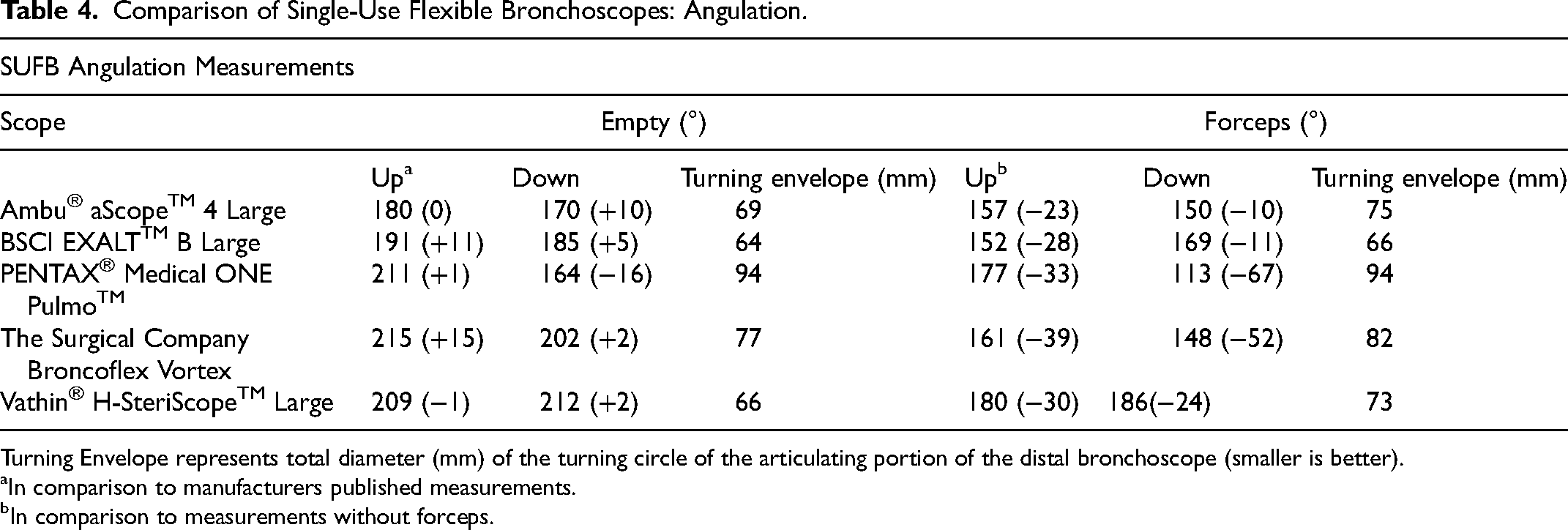
Turning Envelope represents total diameter (mm) of the turning circle of the articulating portion of the distal bronchoscope (smaller is better).
In comparison to manufacturers published measurements.
In comparison to measurements without forceps.
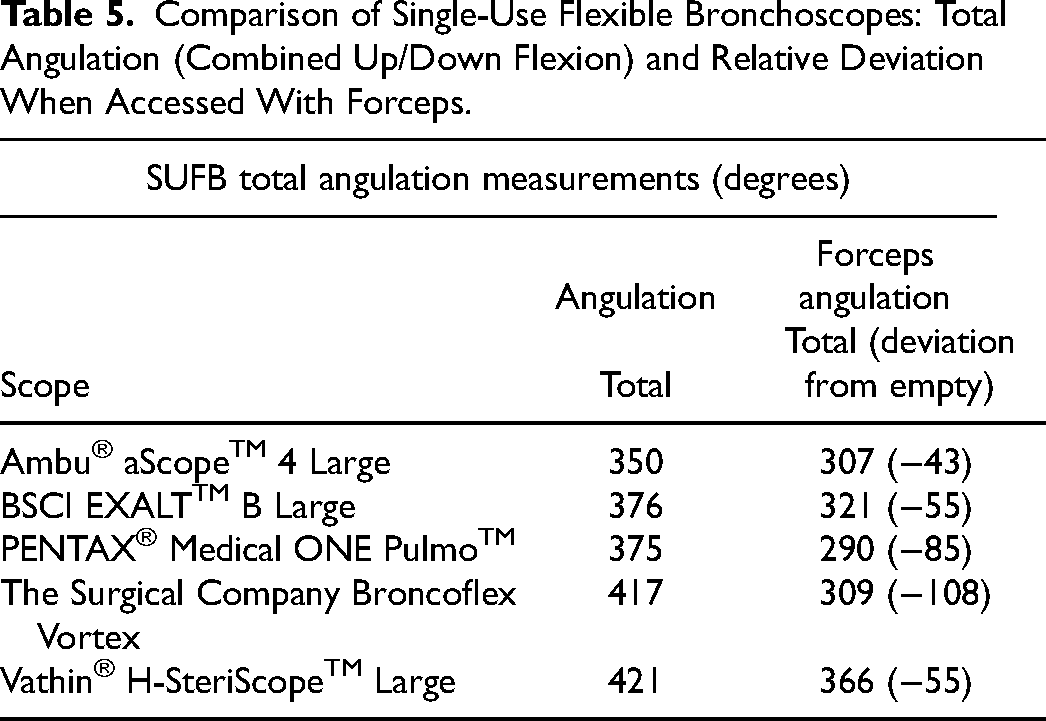
The Vathin SUFB had the widest amount of angulation based on product specifications with 210° of free movement in either direction. Measured angulation of all bronchoscopes relative to specifications was acceptable in most cases, ranging from −1° to +15°, except for the Pentax SUFB which measured −16° (164° vs 180°) relative to the reported downward flexion from product specifications. When instrumented, the Vathin SUFB provided the best angulation with 180° upward and 186° downward flexion, 366° in total (Table 5). The Pentax SUFB was most affected by instrumentation with a loss of 67° of downward flexion compared to baseline device specification; however, it was comparable to other devices in upward flexion, −33° relative to specifications bringing it to within 3° (177° vs 180°) of the Vathin SUFB in this plane. The Boston SUFB had the least amount of reduction in angulation related to instrumentation with the second largest level of free movement in either direction.
Comparison of Single-Use Flexible Bronchoscopes: Total Angulation (Combined Up/Down Flexion) and Relative Deviation When Accessed With Forceps.
An Assessment of Scope Suction
The Boston SUFB outperformed all other scopes in tests of suction with suction often twice as fast (Figure 6). Similar results were recorded for each sample of each scope. It was significantly quicker in comparison to the total group and to the reusable Pentax 3.2 mm scope in the suction of pseudo-mucus (P = .0001 for both total group and reusable scope), saline (P = .0010 for both), and saline with forceps (P = .0015, P = .0017). It was the only scope capable of suctioning pseudo-mucus around a forceps. It was also noted that despite not pushing the suction button, both Vathin SUFBs had a low amount of persistent suction.
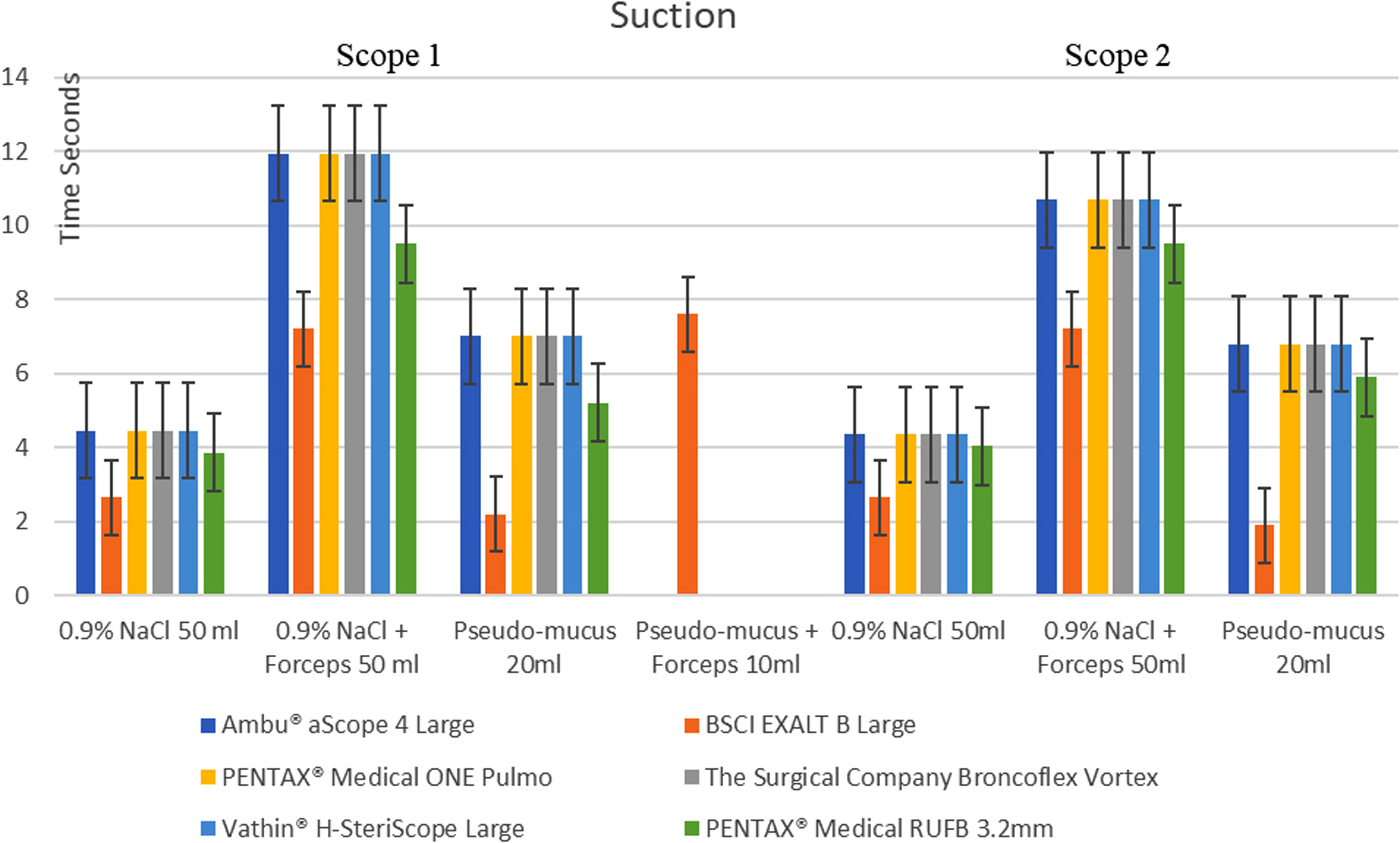
A comparison of suction. Graph depicting mean suction for 2 trials for each scope of 50 mL of 0.9% Sodium Chloride with and without instrumentation and 10 mL “pseudo-mucus” with (Boston SUFB was the only scope able to suction “pseudo-mucus” around instrument) and 20 mL without instrumentation. Two scopes were used for each company (Scopes 1 and 2) and compared to a reusable Pentax 3.2 mm scope (green bars).
Discussion
Although lacking in direct head-to-head comparisons, SUFBs have many advantages over reusable scopes including portability, lack of cleaning required before and after procedure, and immediate availability in an emergency. Other potential advantages include a reduction in infection and cost.1,3 Evidence associating reusable scope contamination despite adherence to cleaning protocols and infection is gathering.1,3 Superbug contamination has also been identified. 26 The true extent of this serious risk will only be identified with rigorous data including genetic analysis and specialized culture for bacteria, viruses, and fungal infections. Reduction in size and more complex devices such as endobronchial ultrasound scopes will make cleaning harder. 2 The cost-effectivity of SUFBs not only depends on this risk of infection but also the number of procedures a year (the more procedures, the more cost-effective reusable scopes are).3,15
We compared commercially available scopes in Europe in 2021 including a prototype scope of a leading bronchoscopy company that has subsequently being approved. A system from Verathon® Medical is available in other jurisdictions with data regarding their laryngoscope but not bronchoscope range is available. 27 An animal study using a new system not commercially available reported advantages over a similar reusable Ambu® aScope3™ scope. 28 All companies have a slim scope option with other some differences in other size available. We elected the larger 2.8 mm channel scope (3 mm Pentax SUFB) as this is more optimal for suction. Other differences in capabilities that need consideration include rotatable capabilities (Vathin SUFB) and technology to assist in the detailed view of mucosal and vascular patterns (Pentax SUFB). Monitor screen size and compatibility vary and it is important that the SUFB system you choose has connectivity to your endoscopy monitors. Although there have not been direct monitor comparisons, another preclinical study identified a preference for the Boston ExaltTM monitor over the aViewTM 2 Advanced monitor. 24 Due to in availability of all company monitors at the time of clinical testing, we did not report on monitor preference which is a critique of our analysis.
Regarding the preference of SUFBs in a preclinical scenario without monitor or suction, interesting differences arise. The Broncoflex SUFB was the SUFB preferred by the majority assessed. Females prefer the Pentax SUFB which is consistent with a gender hand size difference. Males preferred the Broncholex SUFB which with a larger male group influenced overall preference. More experienced physicians preferred scopes with handle structure similar to reusable bronchoscopes. A trend toward this differentiation was also identified in a comparison of respiratory physicians and anesthetists. In another preclinical simulator survey including 38 participants conducted at an interventional pulmonology conference, reusable scopes were preferred to SUFBs with Vathin preferred to Ambu SUFB. 16 It could be argued that it was futile to include junior doctors and endoscopy nurses without bronchoscopy experience; however, data from this group may potentially provide a more “genuine” opinion on aspects such as ergonomics and more robust data from this larger group regarding gender and hand size preferences. The opinion of endoscopy nurses is clearly important, particularly with the prevalence of advanced nurse practitioner roles increasing.
Our benchtop analysis also identified mechanical differences. The larger turning envelope of the Vathin and Ambu SUFB may make it more difficult to engage smaller or distorted segmental anatomy. In parallel in our preclinical assessment, both ranked in the bottom 3 as regard user ratings for biopsy. The Boston SUFB required the most thumb force; however, the clinical significance of this is unclear. It ranked second last in the usage user ratings. Loss of movement related to instrumentation and maximal flexion to extension is however clearly significant. When accessing difficult-to-instrument airways such as upper lobe, subsegmental bronchi millimeters matter. This can lead to the inability to access bronchi making biopsy difficult. 29 The Vathin SUFB and Boston SUFB had optimal mobility with forceps in situ.
The most striking difference and probably the most clinically significant, however, was the suction superiority of the Boston SUFB. In addition to significantly outperforming (often twice as fast) all other SUFBs and a standard bronchoscope, it was the only scope able to suction “pseudo-mucus” around an instrument, which suggests ability to suction mucus or blood around a biopsy instrument. The reason for this is probably the clamshell shape of the suction channel that replicates another recent comparison of Boston with Ambu SUFB. 24 Our center has subsequently published a pilot clinical study of 24 patients using the Boston SUFB highlighting the ability to control hemoptysis both in the endoscopy suite and OR. 30
Clinical trials clearly are warranted. In addition to our pilot study of the Boston SUFB, our center has published an evaluation of the Broncolfex SUFB in a quaternary referral center including an interventional pulmonology service. 25 A total of 139 procedures were included with no complications. Procedures included transbronchial, endobronchial and cryobiopsy, transbronchial needle aspiration, argon plasma coagulation, and stent placement; 85% of procedures were scored at the highest level of satisfaction by proceduralists. Four procedures required conversion to a reusable scope.
Other limitations include the inability to blind participants and a lack of suction and monitor comparisons in a preclinical trial. The suction of “pseudo-mucus” out of a container in no way is the same as clearing secretions out of an airway involving scope angulation, cough, collapsing airways, and patient movement. Our study also assessed only one scope size; however, better suction was identified in another study across the range of scope sizes comparing Boston and AMBU SUFB. 24 In addition, our low-fidelity simple simulation tubing is clearly not validated in any study as a training tool.
To summarize findings related to each scope, although the Ambu SUFB has the most published data (ICU, bronchoscopy suite, and theater trials), it ranked lowest in preference for respiratory physicians and intensivists combined and maximal flexion to extension angle and was second worst in losing this range with forceps in-situ. A new fifth-generation AMBU SUFB generation scope is in the process of approval with revisions in design which appear to approximate the scope handle of a reusable scope. Of course, vendors are constantly improving both monitors and scopes and thus after our evaluation, newer devices will be released.
The Boston SUFB outperformed all in suction, mid-ranking in preference, the fourth least flexion to extension angle (albeit maximal thumb force) but reserved with instrument (second best). The Broncoflex SUFB was the preferred scope overall, particularly in males. It reduced from second to fourth ranking with instrumentation. The Pentax SUFB was the preferred scope for females and smaller hands. However, its range of flexion to extension is the least with instrumentation. The Vathin SUFB was heaviest, has the best scope size range, and best maximal flexion to extension angle.
These differences should be considered when selecting which SUFB to use in your institution. Other factors such as cost, institutions’ relationship with individual vendors including available company representatives and local or national group tender evaluation will influence scope selection. A clinical trial comparing all SUFBs available in matched patients and scenarios is not feasible. The robustness of such a trial would be poor given the inability to blind proceduralists and the lack of a sham control. Ultimately, the performance of SUFBS in clinical trials25,30 will provide the most important information for switching from reusable scopes to SUFBs.
Supplemental Material
sj-docx-1-jic-10.1177_08850666221148645 - Supplemental material for Single Use or Disposable Flexible Bronchoscopes: Bench Top and Preclinical Comparison of Currently Available Devices
Supplemental material, sj-docx-1-jic-10.1177_08850666221148645 for Single Use or Disposable Flexible Bronchoscopes: Bench Top and Preclinical Comparison of Currently Available Devices by Kevin Frederick Deasy, BSc, MB, MRCPI, Anne-Marie Sweeney, MB, MRCPI, Hammad Danish, MB, MRCPI, Emily O'Reilly, MB, MRCPI, Hisham Ibrahim, MB, MRCPI, and Marcus Peter Kennedy, MD, FRCPI, FCCP in Journal of Intensive Care Medicine
Footnotes
Authors’ Note
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was approved by institutional/regional/national ethics/committee/ethics board of University College Cork (UCC-ECM 4 (e) 2021) with a waiver of informed consent for individual participants.
Author Contributions
(I) Conception and design: Drs Kennedy was the author who conceived and designed the project, (II) Administrative support: All authors, (III) Provision of study materials or patients: All authors, (IV) Collection and assembly of data: All authors, (V) Data analysis and interpretation: Drs Kennedy, Sweeney, Deasy were the team who analyzed and interpreted the data. (VI) Manuscript writing: All authors, (VII) Final approval of manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form. Prof MPK has received speaker fees from The Surgical Company, Boston Scientific Ireland, Pentax Medical, and Cook Medical. He also received equipment as part of a training grant for pulmonary trainees valued at 2000 Euro.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.