
Abstract
Medical device-related pressure injuries (MDRPIs) represent a growing and often overlooked complication in critical care environments. These injuries, result from prolonged contact with essential therapeutic equipment such as endotracheal tubes, catheters, and monitoring devices, posing a significant threat to patient safety and recovery.
This systematic review synthesizes current research on the incidence and prevalence of MDRPIs in intensive care units, highlighting key risk factors including immobility, impaired perfusion, and the complexity of care in critically ill populations. Attention is drawn to the variability in reporting standards and methodological inconsistencies across studies, which obscure the true burden of MDRPIs globally. In examining evidence from diverse healthcare systems, this review emphasizes the urgent need for standardized protocols, early detection strategies, and multidisciplinary approaches to prevent device-related tissue damage. Addressing this silent threat is vital not only to improve patient outcomes but also to reduce healthcare-associated costs and strengthen the culture of safety in critical care settings.
Introduction
Pressure injuries (PIs) remain a global burden. There are various factors that can result in the formation of PIs such as decreased mobility, medical devices, disease processes and malnutrition. Throughout the world, healthcare organizations are searching for various methods to eradicate this high maintenance burden. One of the most common overlooked PIs are medical device related pressure injuries (MDRPIs) in critical care units. Medical devices are an integral aspect for caring for patients in all healthcare settings. Medical device-related pressure injuries arise when diagnostic or therapeutic equipment exerts continuous pressure on the skin or mucosal surfaces, leading to localized tissue damage. 1 These injuries often mirror the shape or contour of the device and are classified based on the severity of tissue involvement. 1 Patients in hospitals, especially in critical care units, are highly susceptible to developing MDPRIs. Both the elderly and the young who are hospitalized for long periods, who are critically ill and are attached to multiple devices face MDRPIs. 2 Medical device related pressure injuries usually present as the shape or pattern of the device and are usually categorized by the stage of PI once detected. When (PIs) develop on mucosal membranes, staging is not applicable due to the absence of keratinized epithelium, unlike cutaneous tissue. 3
Recent international research has highlighted the widespread nature of (PIs). These include findings from a study conducted in Iran that estimated the global prevalence to be around 28.5%. 4 In contrast, a pediatric intensive care unit study from Turkey reported an alarmingly high MDRPI rate of approximately 80%, highlighting the vulnerability of critically ill children to device-related skin damage. 5
Methods
Study Selection
This systematic review was conducted to examine the incidence and prevalence of MDRPIs in critical care units. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 guidelines to ensure transparency and reproducibility.
Search Strategy
A comprehensive search was performed in PubMed/MEDLINE, Science Direct, CINAHL, and the Cochrane Library for studies published between January 2019 and June 2025. “Medical device-related pressure injury” OR “device-related pressure ulcer” OR “MDRPI” OR “MMPI” AND “critical care” OR “intensive care unit” OR “ICU” AND “incidence” OR “prevalence”.
Study Selection
Titles and abstracts were independently screened by two reviewers, and full texts of potentially eligible studies were assessed against the inclusion and exclusion criteria. A narrative synthesis was performed due to heterogeneity in study designs, ICU populations, and definitions of MDRPIs. Incidence and prevalence data were summarized descriptively, with ranges reported. As this review uses previously published literature, ethical approval was not required. The population under study includes adult and pediatric population in the critical care units.
Pressure Injuries
The National Pressure Injury Advisory Panel (NPIAP), European Pressure Ulcer Advisory Panel (EPUAP) and Pan Pacific Pressure Injury Alliance (PPPIA), define pressure injuries (PIs), as tissue damage that typically occurs over areas of the body where bones are close to the skin surface, or in regions affected by sustained contact with medical equipment. 4 These injuries may present as either intact skin or open wounds and are often accompanied by discomfort. 4 The underlying cause is prolonged mechanical stress, including pressure, shear, and friction forces. 4 Factors that enhance PIs include microclimate, nutrition, perfusion, co-morbidities and conditions of the soft tissue. 6 National Pressure Injury Advisory Panel officially changed the word ulcer to injury in 2016 as they stated that the word injury describes PIs in both intact and ulcerated skin. 4 A PI refers to damage that may occur on weight bearing skin underlying a bony prominence. 7 The extent of damage can range from skin redness to full tissue deterioration, where the underlying structures, such as bone, muscle, tendon and cartilage are visible. 7 Pressure injuries can be classified as superficial and severe PIs. 8 Abrasion, maceration and sloughing, and delamination of the skin layers are primarily associated with superficial PIs. 8 In comparison to superficial PIs, severe PIs occur in the muscle layers directly adjacent to bony prominences and develop due to sustained compression and deformation of deep tissue. 8 Pressure injuries are complex and rarely attributed to one single factor, instead, they are reported as systems failure due to the impact on the patient's health. 9 Pressure injuries can result from immobility, leading to continuous pressure of bony prominences on the skin. An Australian study has revealed that PIs are serious adverse events that can occur within a week of admission for the patient population of 60 years and above. 10 This injury to the skin occurs most commonly because of pressure, friction, shear force or any combination of these. 11 When these biomechanical factors co-exist with declining health conditions or chronic illness, the risk for developing PIs increases drastically. 8 Shear injury occurs when layers of skin and underlying tissue move in opposite directions, disrupting blood flow and depriving cells of essential nutrients and oxygen. 12 This mechanism is particularly harmful, as it can lead to deep tissue damage even in the absence of external pressure. 12 Friction on the other hand, results from the rubbing against surfaces, causing superficial abrasion that compromises the skin's protective barrier. 8 Patients with neurological conditions or who are partially immobile generally develop friction related PIs. 11 Patients living with PIs, especially severe cases, often experience pain, infection, amputation, emotional suffering, prolonged hospital stays, and significant costs. 13 In general, PIs place a significant burden on the healthcare system, while also impacting on the quality of life of individuals and their caregivers. 6 These effects can be associated with depression, helplessness, and anxiety, as PI prevention can be a life-long commitment for those with permanent mobility impairments. 6
Critical Care Units and Patient Profiles
Admissions to Critical Care Units
The word critical care unit is used interchangeably with intensive care unit (ICU). Patients are admitted to critical care units when their condition requires continuous monitoring or advanced life-support interventions that exceed the capabilities of a general ward. 14 There are various reasons for admission to ICU which include hemodynamic instability such as shock and arrythmias, respiratory failure requiring invasive or non-invasive ventilation, recent onset of altered level of consciousness, multi organ failure, burns and postoperative complications following major surgeries such as thoracic, cardiac, abdominal or trauma. 15 Patients admitted to general wards who are at high risk of health deterioration may be admitted to ICUs for further management. 14
Medical Admissions
Guidelines emphasize that admissions to critical care units care should be reserved for patients who are most likely to benefit from therapeutic and intensive interventions. 16 These units are equipped with advanced technologies and medications not routinely available in general wards, and care is delivered by staff trained in managing complex conditions. 16 Patients are typically admitted based on clinical indicators such as hemodynamic instability, multi organ failure, respiratory failure, altered level of consciousness or acute renal failure requiring hemodialysis. 16 The doctor's decision to admit the patient to ICU is influenced by the severity of illness and is often guided by scoring systems such as the Acute Physiology and chronic health evaluation II (APACHE II) or Sequential organ failure assessment (SOFA). 16 Patients with acute medical conditions or those at high risk of health deterioration or those requiring closer observations following major procedures, warrant ICU admission. 15 It is important to note that admission decisions must balance individual patient needs with resource availability and ethical considerations especially in times of limited capacity such as sufficient nurses, medication and equipment. 15
Surgical Admissions
An approach that prioritizes proactive planning and risk assessment for ICU admissions that can enhance patient outcomes and prevent the overuse of critical care resources. 15 Typically, patients are admitted to the surgical ICU when they require intensive postoperative monitoring, organ support, or urgent intervention due to complications, especially after high-risk surgeries such as major abdominal, cardiothoracic, neurosurgical, or vascular procedures. 16 This is particularly important for individuals with comorbidities or those experiencing hemodynamic instability during surgery. 16 Patients who experience major burns also necessitate ICU admission for close observation. 15 The decision to admit patients to critical care units is collaboratively made by surgeons, anesthesiologists and intensivists and is based on clinical indicators such as hemodynamic instability, respiratory compromise, altered mental status and the need for mechanical ventilation or renal replacement therapy. 15 Although there are no universal criteria for surgical ICU admission, guidelines emphasize that care should be reserved for those patients who are in dire need of this care and are most likely to benefit from these lifesaving interventions. 16
Medical Devices and Critically Ill Patients
Medical devices provide significant benefits for long-term patients in critical care units to improve health outcomes, enhance independence and ensure a better quality of life. However, common devices used in critical care unit settings such as CPAP masks; wound care drains, invasive lines and other therapeutic devices pose a risk of developing PIs. 2 Critically ill patients are admitted to hospital with complex disease processes coupled with a multitude of comorbidities which heighten their vulnerability to MDRPIs. 2 A Brazilian study highlighted that the more medical devices used in patients in the critical care units, the greater the risk of developing MDRPIs, especially with those patients who have suffered cerebrovascular accidents (CVA) and are bedridden, have restricted blood flow which can lead to tissue damage and ulceration, making them susceptible to edema due to the third spacing of interstitial fluid. 17 When devices such as blood pressure cuffs or pneumatic compression devices are used on this population of patients, the risk for MDRPI increases because of poor skin integrity. 7 This is the effect of skin and tissues being deprived of oxygen and nutrients. 7 Patients that suffer from chronic renal failure and are hospitalized in critical care units due to disease complications are generally attached to many medical devices. 18 The same authors noted that these patients may have poor skin integrity because of fluid and electrolyte abnormalities and are prone to long-term mechanical ventilation, they are susceptible to MDRPIs. 18 Additionally, patients that have systemic inflammatory response syndrome (SIRS) or multi organ dysfunction syndrome (MODS) often have multiple medical devices attached to them. 19 Persistent inflammation, immunosuppression, edema and catabolism that are characteristic of this condition, cause moisture to affect the skin in certain areas such as crevices and skin folds, making it fragile and susceptible and at risk of developing MDRPIs. 19
Medical Device Related Pressure Injuries
Patients hospitalized in critical care units are particularly susceptible to developing MDRPIs, due to factors like reduced sensory perception from sedation, edema, immobility, and prolonged hospitalization. 20 Medical device related pressure injuries occur because of localized damage to the skin and underlying tissues caused by sustained pressure, friction, and shear forces especially over bony prominences. 2 These mechanical forces can lead to tissue ischemia and edema, ultimately resulting in PIs. 19
A study conducted in Jordan reported that 5.01% of MDRPIs occurred in the ICU, highlighting the vulnerability of critically ill patients to device-related injuries. 21 This increased risk is primarily attributed to the compromised immunity of critically ill patients and their dependence on multiple medical devices which include invasive lines such as central and arterial catheters, mechanical ventilators and CPAP masks, blood pressure cuffs, oxygen saturation probes, tracheostomy ties, dialysis catheters, bedpans, tubes and drains, splints and braces, monitor cords, nasogastric tubes, and Foley catheters. 21
Additionally, underlying health conditions such as diabetes and chronic obstructive pulmonary disease (COPD) can further impair wound healing causing many of these patients to develop edema because of their disease processes, which exacerbates the risk of MDRPI development. 20 Although regional studies in the Middle East have emphasized the need for improved device management protocols and enhanced nursing education to mitigate the burden of MDRPIs in high-risk populations, data on MDRPIs remains limited. 22
Probable Causes and Risk Factors of MDRPIs in ICUs
There are probable causes and risk factors of MDRPIs in critical care units which include patient related risk factors, device related risk factors and ICU environment and treatment factors.
Patient Related Risk Factors
Patients who are sedated or unconscious lack the sensory awareness and motor control necessary to perceive discomfort or reposition themselves. This immobility leads to sustained pressure on certain areas of the body, particularly where medical devices interface with skin. 20 Over time, this continued pressure can compromise tissue perfusion, resulting in ischemia, edema, and ultimately the development of MDRPIs. 20 Critically ill ventilated patients often receive sedation and neuromuscular blocking agents that impair their communicative ability which further impairs their cognitive abilities causing an increased risk for MDRPIs especially from medical devices such as endotracheal tubes, arterial lines, ECG leads or other cables that they are connected to. 20
During the acute phases of admission to critical care units, these patients are typically immobile which reduces tissue perfusion especially under devices. 23 Additionally, sedated patients often have decreased cardiac output which leads to decreased tissue perfusion, making them susceptible to PIs. 24
Patients with severe respiratory compromise are frequently managed in the prone position to enhance oxygenation. 25 However, this position increases the risk of MDRPIs, particularly to the face, due to prolonged contact with devices such as endotracheal tubes, oxygen masks, and monitoring equipment positioned near facial structures. 25
Device Related Risk Factors
Respiratory devices such as endotracheal tubes, tracheostomy tubes and ties, CPAP and BIPAP masks account for 68% of MDRPIs in critical care units. 20 The longer these devices remain in use, the greater the risk of tissue damage due to sustained pressure, friction and shear. 20 Another causative factor of MDRPIs includes poorly secured devices such as respiratory devices, nasogastric tubes and appropriate dressings for medical devices. 26
ICU Environment and Treatment Factors
Critical care units present with a unique set of environmental and therapeutic challenges that significantly increase the risk of MDRPIs. Factors such as limited patient mobility, continuous monitoring, and the use of life-sustaining equipment contribute to prolonged pressure and friction at device contact points. 18 Environmental stressors including noise, artificial lighting, and disrupted sleep cycles can impair tissue recovery and exacerbate vulnerability to PIs. 18 Vasopressors such as dopamine and norepinephrine constrict blood vessels thereby causing decreased tissue perfusion especially in peripheral areas like the skin making these areas more vulnerable to skin break down under medical devices. 26
Feeding via enteral tubes such as nasogastric and orogastric tubes are common in ICU patients who can’t take orally. 27 If these tubes are not properly secured or padded, they cause friction and shear by exerting localized pressure to the nose, lips and cheeks. 27 A combination of immobility and poor skin perfusion increases the risk of MDRPIs in the areas of contact. 27
Environmental stressors like noise, artificial lighting and disrupted sleep patterns impair tissue recovery, thereby causing vulnerability to MDRPIs. 26 Exposure to high decibel alarms, unfamiliar environment, staff activity and mechanical equipment interfere with the patient's sleep pattern. 28 Sleep deprivation has shown to impair immune function, reduce cellular degeneration and delay wound healing, all of which are essential for maintaining skin integrity. 29 Lack of sleep can exacerbate systemic inflammation which compromises microcirculation causing diminished ability of the skin to withstand pressure and shear forces. 30 These factors make patients vulnerable to MDRPIs especially in areas where devices exert prolonged contact. 30
An article by the authors Greenway et al 31 concluded that vasopressor associated vasoconstrictors can cause PIs in critically patients. The same authors further stated that patients in critical care units undergo stress due to various physiological factors and with added equipment such as invasive devices like ECMO machines, invasive catheters and tubes and medication compromises skin integrity, making it more susceptible to PIs. 31 A study in Beijing highlighted that prone positioning together with invasive devices such as endotracheal tubes and other invasive devices used for critical care patients are also a contributing factor to PIs. 32
Incidence and Prevalence Trends of MDRPIs in ICUs
Recent studies revealed a growing recognition of MDRPIs in ICUs, driven by increased awareness and improved detection methods. However, despite these advances, underreporting continues to obscure the true scope of issue. 18 According to existing literature, the reported incidence of MDRPIs in critical care units varies, with estimates ranging from 34%, influenced by factors such as the patient population, the types of medical devices used, and institutional practices. 18
Patients undergoing prolonged mechanical ventilation or experiencing reduced mobility are particularly vulnerable, with markedly higher prevalence rates. 20 A study found that medical devices such as endotracheal tubes, CPAP masks and tracheostomy ties accounted for 72.2% pressure injuries in ICUs, highlighting the substantial role of device-related factors in injury development. 20
The incidence of MDRPIs is significantly influenced by the type of device used, as it was noted in a study that respirators alone have been reported to account for approximately 30%-70% of MDRPIs, emphasizing their substantial role in PI development. 20 The (Table 1) highlights a global incidence of PIs
Incidence Rates of MDRPIs by Country.
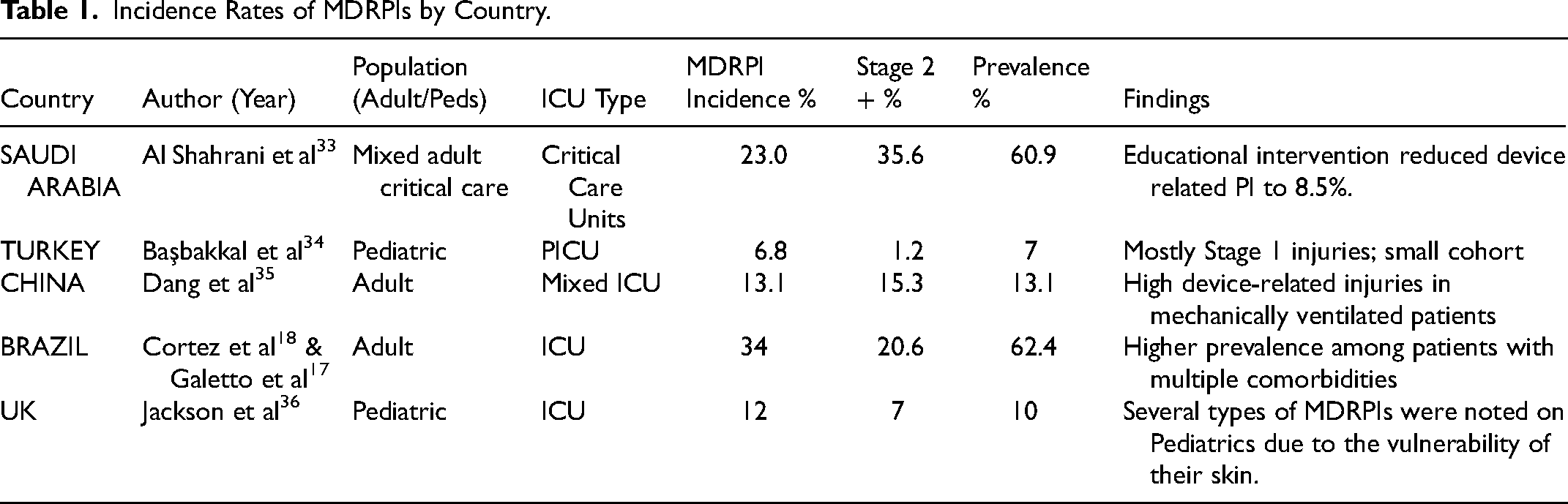
Across the five included studies, the incidence and prevalence of MDRPIs varied considerably across regions and patient populations. In Saudi Arabia, Al Shahrani et al 33 reported one of the highest MDRPIs incidence rates 23%, with a prevalence of 60.9%; however, an educational intervention significantly reduced device-related PI occurrence to 8.5%. Pediatric rates were lower overall, as demonstrated in Turkey and the United Kingdom. In a pediatric ICU in Turkey, Başbakkal et al 34 reported a relatively low incidence of 6.8%, with only 1.2% progressing to Stage 2 or higher. Similarly, Jackson et al 36 found a 12% incidence and 10% prevalence in a UK pediatric ICU, emphasizing pediatric vulnerability due to immature skin integrity.
Adult ICU studies in China and Brazil reported moderate to high MDRPI burdens. Dang et al 35 identified a 13.1% incidence in a mixed adult ICU, with the majority occurring among mechanically ventilated patients. In Brazil, combined findings from Cortez et al 18 and Galetto et al 17 demonstrated a notably high prevalence of 62.4% and a 34% incidence, largely attributed to patients with multiple comorbidities and prolonged device use. Overall, the evidence indicates that MDRPIs remain a significant global challenge, with highest rates seen in adult ICUs and lower, but still notable, rates in pediatric populations.
Adult Versus Pediatrics in ICU with MDRPIs
Comparative evidence demonstrates notable differences in the incidence and severity of MDRPIs between adult and pediatric intensive care populations. Adult ICU patients consistently exhibit a higher MDRPI burden, with incidence rates ranging from 13.1% to 34% and Stage 2 or greater PIs reported between 20.6% and 35.6% in the reviewed studies.17,18,33,35 These elevated rates reflect the combined influence of prolonged immobility, greater exposure to invasive devices, mechanical ventilation, and the presence of multiple comorbidities, all of which contribute to increased tissue susceptibility.
In contrast, pediatric ICU patients showed lower MDRPI incidence and severity. Reported incidence ranged from 6.8% to 12%, while Stage 2 or greater PIs were substantially less frequent at 1.2% to 7%.34,36 Despite these comparatively lower rates, children remain inherently vulnerable due to thinner, less keratinized skin, smaller body surface areas, and disproportionately higher pressure exerted by medical devices relative to their size.
Taken together, these findings highlight clearly differentiated risk profiles because adults exhibit a higher overall MDRPI burden driven by clinical complexity and device exposure, whereas pediatric patients, although sustaining fewer severe PIs, require age-appropriate prevention strategies tailored to their unique anatomical and developmental considerations. This comparison reinforces the importance of population-specific MDRPI prevention protocols, including device selection, correct fit, positioning, and surveillance, to ensure optimal outcomes across all critical care age groups.
Implications of High Rates of MDRPIs Hospitalised Patients
Medical device related PIs can lead to infections such as cellulitis, sepsis, or osteomyelitis and are associated with higher mortality rates, especially in critically ill patients. 26 Patients with MDRPIs often require extended hospital stays due to complications and wound care management resulting in delayed recovery and discharge. 26
Patients suffering from MDRPIs are at a greater risk of hospital re-admission, often due to wound-related complications. 26 These injuries often progress into complex wounds that require ongoing clinical management, including specialized dressings, debridement, and infection control. 26 If not properly treated during the initial hospital stay, patients may return with complications such as delayed wound healing due to poor tissue perfusion or underlying comorbidities. 20 Secondary infections such as cellulitis, abscess formation, or systemic sepsis may develop as complications, further compromising patient outcomes. 37 In severe cases, necrosis or deep tissue damage can occur, requiring surgical intervention or advanced wound management strategies. 37 Additionally, pain and impaired mobility may arise, potentially exacerbating existing comorbidities and impeding the patient's overall recovery process. 37
Moreover, MDRPIs can lead to significant physical discomfort and impaired mobility, potentially worsening existing comorbidities and hindering recovery. 38 Readmissions not only put a strain on healthcare systems but also negatively impact patient outcomes, causing emotional distress, financial burden, and a decrease in quality of life. 38 Furthermore, frequent readmissions are often seen as indicators of suboptimal care, prompting scrutiny from regulatory bodies and possibly leading to negative publicity for healthcare facilities. 38
The economic burden of MDRPIs is substantial as the treatment involving specialized wound care, antibiotics, and sometimes surgical intervention. 26 In cases where MDRPIs become infected, especially with multi-drug-resistant organisms (MDROs), patients may need broad-spectrum intravenous antibiotics, which are more expensive and carry a higher risk of complications. 36 Severe MDRPIs may escalate to the point of requiring surgical intervention, such as debridement or reconstructive procedures, further increasing costs through theatre use and extended recovery times. 22 These treatments often result in longer hospital stays, sometimes increasing from an average of 3 days to over 80 days, which increases the financial burden on healthcare facilities. 22 If the MDRPI is hospital-acquired, reimbursement may be denied, forcing institutions to absorb the full cost of care. 39 These factors contribute to an estimated annual cost of $11 billion in the U.S. alone, emphasizing the urgent need for prevention and early intervention strategies. 39
Medical device related pressure injuries significantly impair patients’ quality of life due to the physical and psychological toll they impose. 40 Persistent pain, discomfort, and emotional distress can severely affect sleep, mobility, and overall daily functioning. 40 These symptoms worsen in cases of MDRPIs, where the visibility and chronic nature of the wounds may lead to social withdrawal, feelings of humiliation, and diminished self-esteem. 40 The stigma associated with visible wounds, foul odor, and leakage can cause isolation, especially among patients with limited mobility or neurological conditions. 40 Studies have shown that the severity and duration of PIs correlate with increased levels of depression, anxiety, and reduced quality of life, requiring the need for holistic care approaches that address both physical and mental health. 40
Pressure injuries including MDRPIs are widely recognized as preventable adverse events, raising serious legal and ethical concerns within healthcare systems. Regulatory bodies such as the World Health Organization (WHO) and The Joint Commission International (JCI) classify PIs as indicators of substandard care, particularly when they occur in hospital settings despite established prevention protocols.41,42 When MDRPIs results from negligence-such as failure to conduct risk assessments, improper device placement, or inadequate documentation, hospitals may face litigation, financial penalties, and reputational damage. 43 A study on medico-legal practices emphasized that the development of PIs often triggers malpractice claims, particularly when preventive measures are poorly implemented or undocumented. 43 Moreover, public scrutiny and media coverage of such cases can erode trust in healthcare institutions, leading to loss of accreditation, reduced patient intake, and long-term brand harm. 43 These risks amplify the ethical imperative for healthcare providers to uphold patient safety standards and maintain transparent, accountable care practices. 43
Implications of Medical Devices Related to Education
The findings of this systematic review highlight important implications for clinical education, policy development, and medical device innovation. Firstly, targeted education and competency-based training for ICU staff are essential to strengthen early detection of MDRPI risk, improve device application techniques, and enhance routine skin assessment practices. Incorporating MDRPI prevention into orientation programs and ongoing professional development may contribute to sustained reductions in PI rates.
Secondly, healthcare institutions and regulatory bodies should strengthen policies that support standardized risk assessment, consistent documentation, and age-specific prevention protocols. Mandating regular reporting of MDRPI incidence at unit or national levels could further improve quality and accountability.
Finally, the persistent burden of MDRPIs highlights the need for advances in medical device design. Manufacturers should prioritize pressure-reducing materials, improved ergonomics, and innovations tailored to both adult and pediatric populations. Partnerships between clinicians and industry can facilitate the development of safer devices and promote the integration of technologies that reduce pressure exposure.
Considerations Related to Prevention of MDRPIs
Integrated Risk Assessment
Critical care unit protocols should incorporate tools that assess risk not only for classic PIs but also for MDRPIs, incontinence associated dermatitis (IADs), including medical device–related mucosal membrane pressure injuries (MMPIs). Recognizing shared risk factors such as immobility, compromised perfusion, moisture exposure, and device contact can support more comprehensive and proactive prevention strategies.
Multifactorial Prevention Strategies
Prevention interventions should address MDRPIs comprehensively through interventions such as repositioning schedules, pressure-relieving surfaces, and protective barrier products as well as rigorous moisture management to be applied to areas at risk for both device-related and traditional PIs. Coordinated care plans can mitigate the additive effect of multiple risk factors.
Interdisciplinary Education and Awareness
Clinicians should be trained to differentiate between MDRPIs, traditional PIs, and IAD/MMPIs, understanding their distinct etiologies while recognizing areas of overlap. Education should emphasize accurate skin assessment, documentation, and early intervention to prevent progression.
Data Integration and Monitoring
Healthcare institutions should establish integrated monitoring systems to track incidence, severity and recurrence of MDRPIs alongside traditional PIs. Such surveillance, supports evaluation of preventive interventions and enables benchmarking for quality improvement initiatives.
Policy and Protocol Development
Policies and protocols should explicitly address the relationships among MDRPIs and classic PIs, ensuring prevention strategies are holistic and aligned with safe device usage practices. Collaboration with clinical teams, administrators and medical device manufactures strengthens prevention efforts and improves patient outcomes.
Recommendations
To reduce the incidence of MDRPIs in critical care units, standardized prevention bundles including regular skin assessments, patient repositioning schedules, and protective dressings should be consistently implemented. 44 Emphasis must be placed on incorporating a specialized multidisciplinary team (MDT) approach, as this fosters collaboration in managing patients with complex medical devices and has demonstrated efficacy in reducing medical device-associated injuries. 44 Staff education remains vital, as training enhances clinical vigilance and facilitates timely interventions, particularly for high-risk devices such as endotracheal tubes, tracheostomy tubes, oxygen masks, urinary catheters, and other invasive lines. 45 Employing evidence-based practices supported by validated tools like the Braden and Norton scales strengthens clinical outcomes and promotes safer care environments. 46 Furthermore, engaging all members of the MDT is crucial, especially in critical care settings where patients are highly vulnerable to MDRPIs and require a coordinated approach to prevention and management. 46
Conclusion
It is essential to prevent MDRPIs from the onset of admission to critical care units. A multifaceted approach in prevention including skin assessment, device management and education is essential. Regular skin inspections underlying and around medical devices are important to eradicate PIs. Repositioning of devices can significantly reduce the risk of MDRPIs.
MDRPIs represent a significant and preventable complication in critical care units. The incidence and prevalence of these PIs indicate the vulnerability of critically ill patients from sustained pressure from medical devices. If the hospital initiates prevention strategies from the onset which include skin assessment, repositioning of medical devices and ongoing staff education, this will decrease the incidence and prevalence of PIs and improve patient outcomes.
Footnotes
Author Contributions
D Anwar – contributed to the writing of the manuscript and topic conceptualization.
V Naidoo – topic conceptualization, reviewed and supervised the research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.