
Abstract
Severe community-acquired pneumonia (SCAP) is associated with significant morbidity and mortality, but there is a paucity of data regarding these infections in sub-Saharan Africa, especially among people living with HIV (PLWH). This study investigated the impact of HIV on clinical presentation, microbial aetiology, laboratory findings, and outcome of SCAP. This was additional analysis of data from a large, single-centre, retrospective, observational study conducted among consecutive adult patients (≥18 years) admitted to the multidisciplinary ICU at the Charlotte Maxeke Johannesburg Academic Hospital, between 1 July 2007 and 31 May 2019, with SCAP. The current study describes 718 PLWH and 131 HIV-negative cases extracted from the initial cohort. The median age was 37 [IQR 30-46] years with PLWH significantly younger than their HIV-negative counterparts (36 years [IQR 29-44] years vs 52 years [IQR 34-65] years; P < .001). PLWH were more commonly female (P = .053), while more of the HIV-negative patients were male. The median CD4 count of the PLWH was 42 [IQR 14-108] cells/mm3 and only 15.5% were on anti-retroviral therapy (ART) prior to hospitalisation. Differences were noted in clinical, laboratory and radiological features between the groups. Overall, Mycobacterium tuberculosis was the most common microbial aetiology in both groups, followed by Streptococcus pneumoniae, which was associated with a significantly lower mortality, whereas mortality with Pneumocystis jirovecii infection, which occurred only in PLWH, was high. Overall ICU mortality was high (48.9%), and while HIV was an independent risk factor for mortality (OR 0.58, 95% CI 0.37-0.92; p = .02) on univariate analysis, this finding was not true when HIV considered within the multivariable analysis. This study describes one of the largest cohorts of PLWH with SCAP and compares their findings with HIV-negative cases. HIV was not a significant predictor of mortality when considered in the context of other covariables on multivariable analysis.
Keywords
Introduction
The lung is one of the most frequently affected organ systems in people living with HIV (PLWH), commonly manifesting with infectious complications. 1 Community-acquired pneumonia caused by Streptococcus pneumoniae (SP) remains the most common cause in most areas of the world, exceeded only by tuberculosis in sub-Saharan Africa and other low- middle-income countries (LMIC).1,2 Several studies have described CAP in hospitalised PLWH2–16 and although there were some similarities compared to HIV-negative patients, there were also significant differences. One unresolved question is what impact HIV has on patient outcomes. Some studies have suggested that the outcomes are the same in PLWH and HIV-negative patients, particularly among those that are virally-suppressed and have a CD4+ T-cell count > 350/mm3.2,6,17–20 while others have documented a higher mortality associated with HIV.21,22
There is no universally accepted definition of severe community-acquired pneumonia (SCAP), and the term is used most commonly in the literature to describe patients with CAP who require ICU admission.23–29 Other terms sometimes used in the description of these cases include multisystem disease and/or multiple organ failure; requiring intensive monitoring and/or organ supportive care; higher morbidity and mortality; increased use of healthcare resources; and/or the diagnosis is based on one or more severity of illness scores.23–29 Nearly one in five patients hospitalised with CAP require ICU admission, with mortality reaching > 25% within 30 days, and as high as 50% within one year following infection. 28 Few studies or guidelines on SCAP have included PLWH and/or patients with various other forms of immunocompromise, who are at increased risk of infection with a broader spectrum of pathogens including Mycobacterium tuberculosis (MTB), Pneumocystis jirovecii (PJP), and other less common microorganisms.29–31 This is particularly so with regard to recent studies of SCAP in LMIC, such as sub-Saharan Africa and Asia, where few studies have compared PLWH with HIV-negative cases.11,32–36
The aim of this study was to describe a cohort of SCAP in PLWH, inclusive of all putative microbial aetiologies, and to compare all aspects of their infection, particularly mortality, with patients without HIV.
Patients and Methods
This study was a further analysis of data from a large, single-centre, retrospective, observational study conducted among consecutive adult patients (≥ 18 years) admitted to the multidisciplinary ICU at the Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), between 1 July 2007 and 31 May 2019, with a diagnosis of SCAP. The full details of the original study have been published elsewhere. 37
The current study compared the demographic, clinical and laboratory findings among PLWH with those that were HIV-negative. The criteria used to confirm the diagnosis of CAP were the same as those described previously. 38 The sources of data were ICU admission records, electronic discharge summaries and/or clinical case notes, and the Picture Archiving and Communication system (PACS; Phillips Intellispace PACS Radiology version 4.4.532.1), a pan-electronic platform used at CMJAH to access radiology.
Data collected included demographic and clinical details, severity of illness scores, laboratory data (including microbiology), radiological features, and details of the clinical course, ICU management, and patient outcomes. Data extraction was undertaken once approval had been obtained from the University of the Witwatersrand Human Research Ethics Committee (Medical) (Clearance certificate number M2008109) and the Chief Executive Officer of CMJAH.
Severity of illness was assessed using the CURB-65 score (Confusion, Urea >7 mmol/L, Respiratory rate ≥ 30 breaths/minute, Blood pressure < 90mm Hg (systolic) and/or ≤ 60mm Hg (diastolic), Age ≥ 65years 39 ) and the Apache II score.40,41 In addition, the ratio of the partial pressure of oxygen in arterial blood to the fraction of inspired oxygen (PF) ratio, one of the minor criteria of severity of CAP as per the Infectious Disease Society of America/American Thoracic Society guideline, was calculated for each patient. 38
Results of routine laboratory tests, performed for all patients on admission, were collected. For HIV testing, the Cobas HIV-1/HIV-2 qualitative assay (Roche) was used for screening, and HIV Ag/Ab combo assay (Abbott) for confirmation. HIV testing was performed with informed consent (in accordance with South African HIV testing policies at that time), 42 together with the corresponding CD4 cell count (flow cytometry on a Beckman-Coulter MPLFC500 cytometer) and HIV viral load (HIVVL) (Roche Cobas® 6800/8800 HIV-1 test). Routine microbiological testing was mostly in accordance with recommendations of the South African CAP guideline. 26 Results of any additional, more specialised, microbiological testing undertaken at the discretion of the attending physician, were also collected.
Data analysis was performed using GraphPad Prism (v9) and Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA version 21.0. Continuous variables were presented as means and standard deviations or medians and interquartile ranges, as appropriate, and for comparison, unpaired t-tests or Mann-Whitney U tests were used. The categorical variables were presented as percentages, and associations among the categorical variables assessed using the Chi-squared or Fisher's exact tests. All tests were 2-tailed. Univariate and multivariable logistic regression analysis (MVA) with a generalized linear model were performed to identify which parameters were independent risk factors for mortality. Variables for the final multivariable model were backward selected, including variables with p > .20 on univariate analysis. However, HIV-specific variables were manually excluded, as data was not equally applicable to both the PLWH and HIV-negative groups. Additionally, variables with more than 10% missing data were manually excluded. Odds ratios for both univariate and multivariate modelling were reported. A P value of <.05 was regarded as statistically significant.
Results
From the original study of 931 patients with SCAP, 718 were PLWH and 131 HIV-negative and were included into the current study of 849 patients of known HIV status.
The median age was 37 [IQR 30-46] years with PLWH significantly younger than the HIV-negative group (36 years [IQR 29-44] vs 52 years [IQR 34-65] years; P < .001), and a smaller proportion of PLWH were aged ≥65 years (17 (2.4%) versus 33 (25.2%) respectively; P < .001). More PLWH were female (387 (53.9%); P = .053), while more of the HIV-negative patients were male. Fewer PLWH were smokers (19 (2.6%) versus 14 (10.7%) in HIV-negative cases; P < .001).
Table 1 documents the comorbid conditions present. In PLWH, 35.5% had additional comorbidities other than HIV, compared to 66.4% in the HIV-negative group (P < .001). In the latter group, diabetes mellitus (DM), chronic cardiovascular (CVD), respiratory (including chronic obstructive pulmonary disease), and renal diseases were significantly more common (P < .001). More PLWH had a history of previous MTB infection.
Co-Morbid Diseases and additional Conditions in PLWH and HIV-Negative Patients with SCAP (849 Patients).
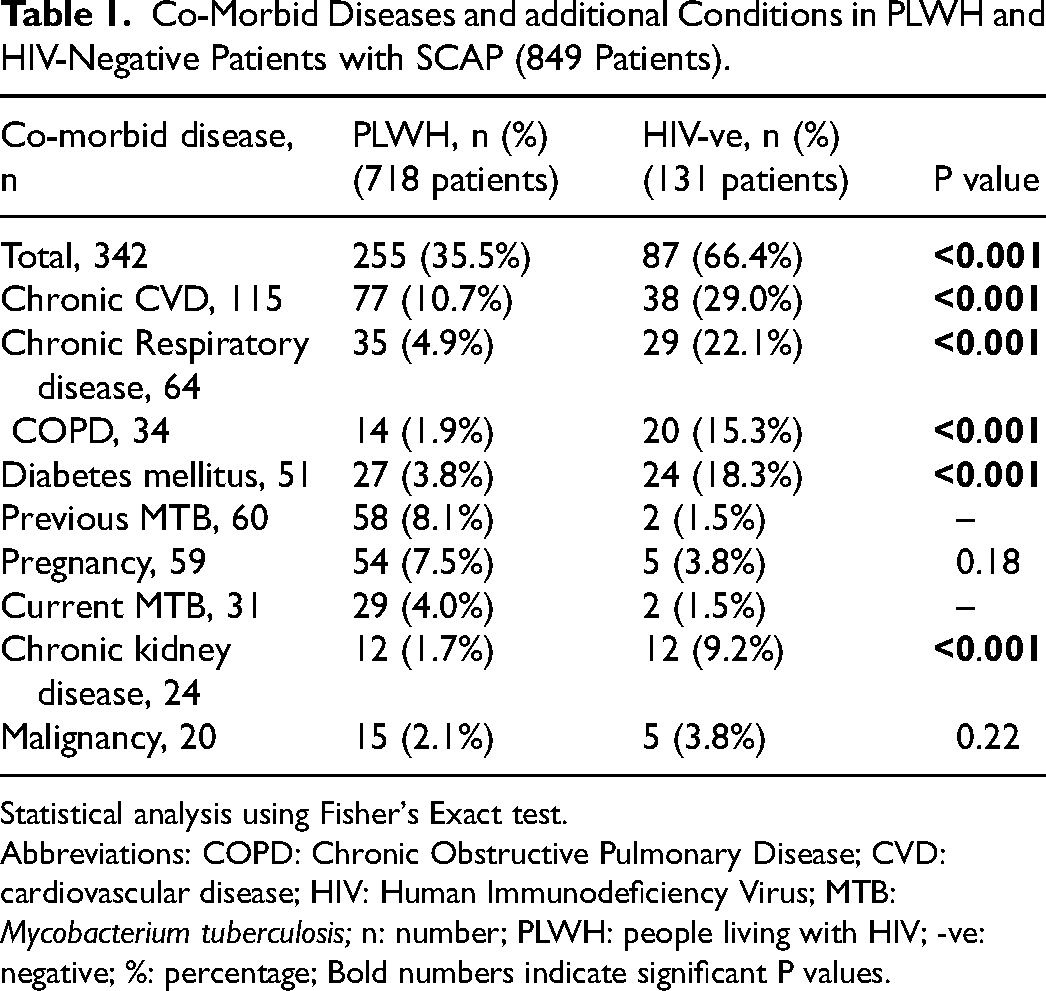
Statistical analysis using Fisher's Exact test.
Abbreviations: COPD: Chronic Obstructive Pulmonary Disease; CVD: cardiovascular disease; HIV: Human Immunodeficiency Virus; MTB: Mycobacterium tuberculosis; n: number; PLWH: people living with HIV; -ve: negative; %: percentage; Bold numbers indicate significant P values.
Table 2 documents the clinical features, severity scores, laboratory data and radiological findings of PLWH compared to HIV-negative cases. PLWH had higher median temperatures (P < .001), although the difference was numerically small. The median Apache II score was higher in PLWH (18 [IQR 14-23] vs 17 [IQR 12-21] in those that were HIV-negative; P = .02); however, there were no significant differences in the CURB-65 score, the PF ratio, nor in the proportion of patients with an Apache II score > 25 or in cases with a PF ratio ≤ 250.
Comparison of Clinical Presentation, Laboratory Data and Chest Radiographic Finding in PLWH and HIV-Negative Patients with SCAP (849 Patients).
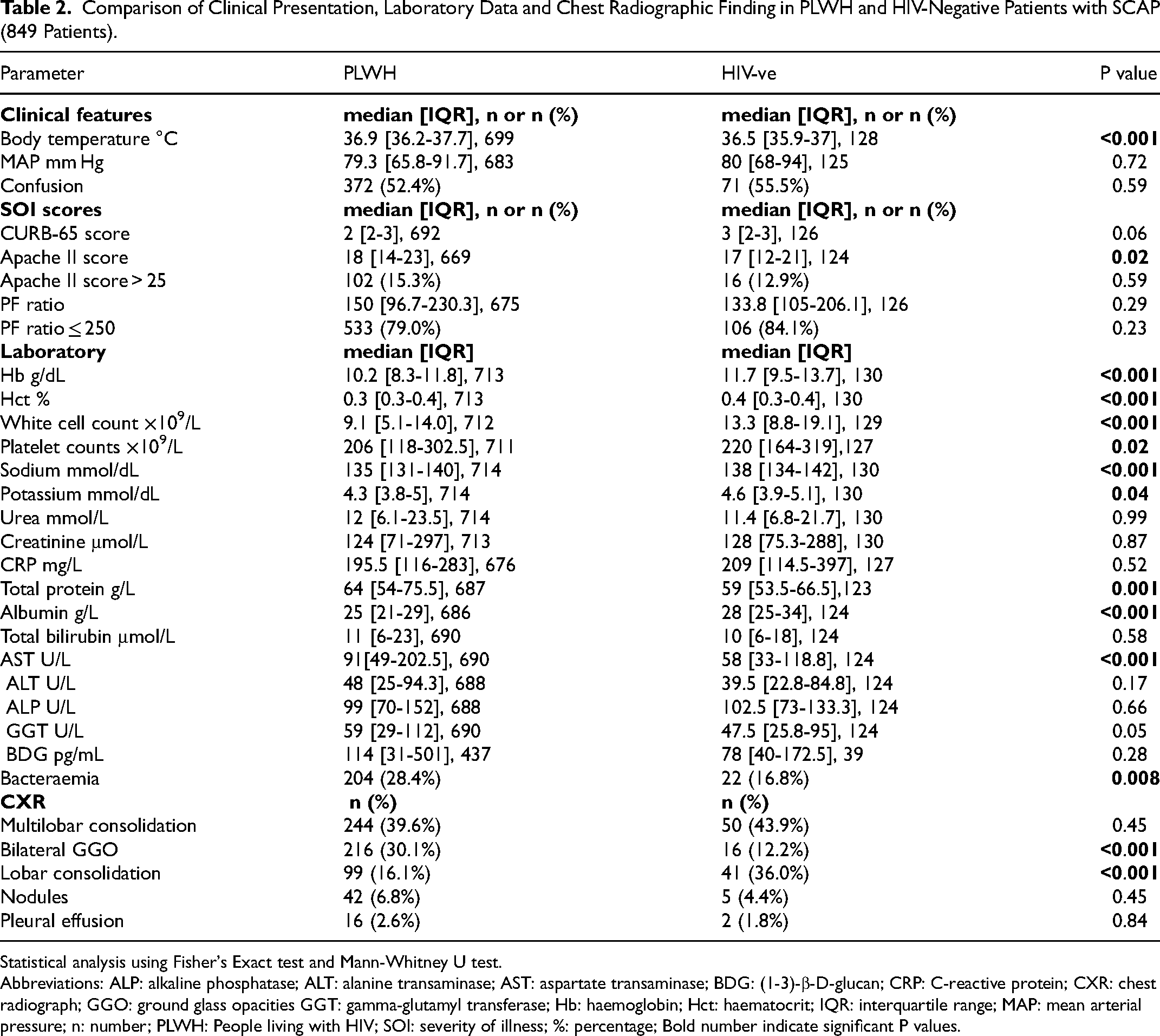
Statistical analysis using Fisher's Exact test and Mann-Whitney U test.
Abbreviations: ALP: alkaline phosphatase; ALT: alanine transaminase; AST: aspartate transaminase; BDG: (1-3)-β-D-glucan; CRP: C-reactive protein; CXR: chest radiograph; GGO: ground glass opacities GGT: gamma-glutamyl transferase; Hb: haemoglobin; Hct: haematocrit; IQR: interquartile range; MAP: mean arterial pressure; n: number; PLWH: People living with HIV; SOI: severity of illness; %: percentage; Bold number indicate significant P values.
The haemoglobin level, white cell and platelet counts, and serum sodium, potassium and albumin, were significantly lower in PLWH, whereas total protein and aspartate transferase (AST) were higher. The predominant radiological finding was multilobar consolidation in both groups, although more HIV-negative patients had lobar consolidation (41 (31.3%) versus 99 (13.8%); P < .001), and a higher proportion of PLWH had bilateral ground glass opacities (216 (30.1%) versus 16 (12.2%); P < .001).
PLWH were significantly less likely to have a microorganism identified but were more likely to have a polymicrobial infection (Table 3). MTB followed by SP were the most common pathogens in both groups, with no significant differences. Among the monomicrobial infections (Table 4), Staphylococcus aureus (SA) was more common in the HIV-negative cohort (8 (6.1%) infections versus 16 (2.2%); P = .03), while PJP occurred only in PLWH (35 (4.9%)) (Table 4). Furthermore, more PLWH had bacteraemia (204 (28.4%) versus 22 (16.8%); P = .008) (Table 2). More respiratory viruses were detected in HIV-negative patients; however further statistical analysis was not performed as numbers were small (Table 4).
Distribution of Monomicrobial and Polymicrobial Infections among HIV-Positive and HIV-Negative Patients with SCAP (849 Patients).
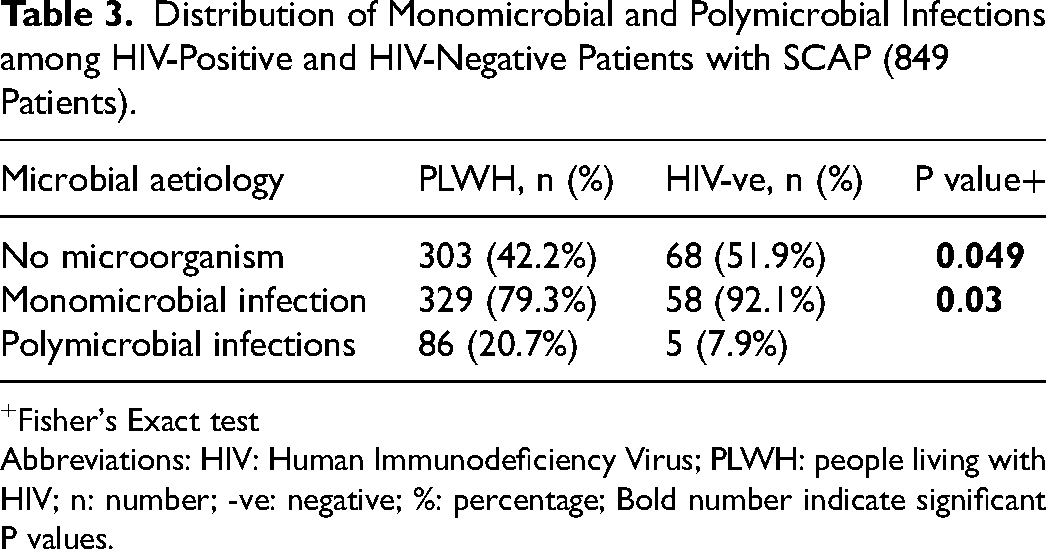
+Fisher's Exact test
Abbreviations: HIV: Human Immunodeficiency Virus; PLWH: people living with HIV; n: number; -ve: negative; %: percentage; Bold number indicate significant P values.
Aetiology of Monomicrobial Infections among HIV-Positive and HIV-Negative Patients with SCAP (42 l Patients).
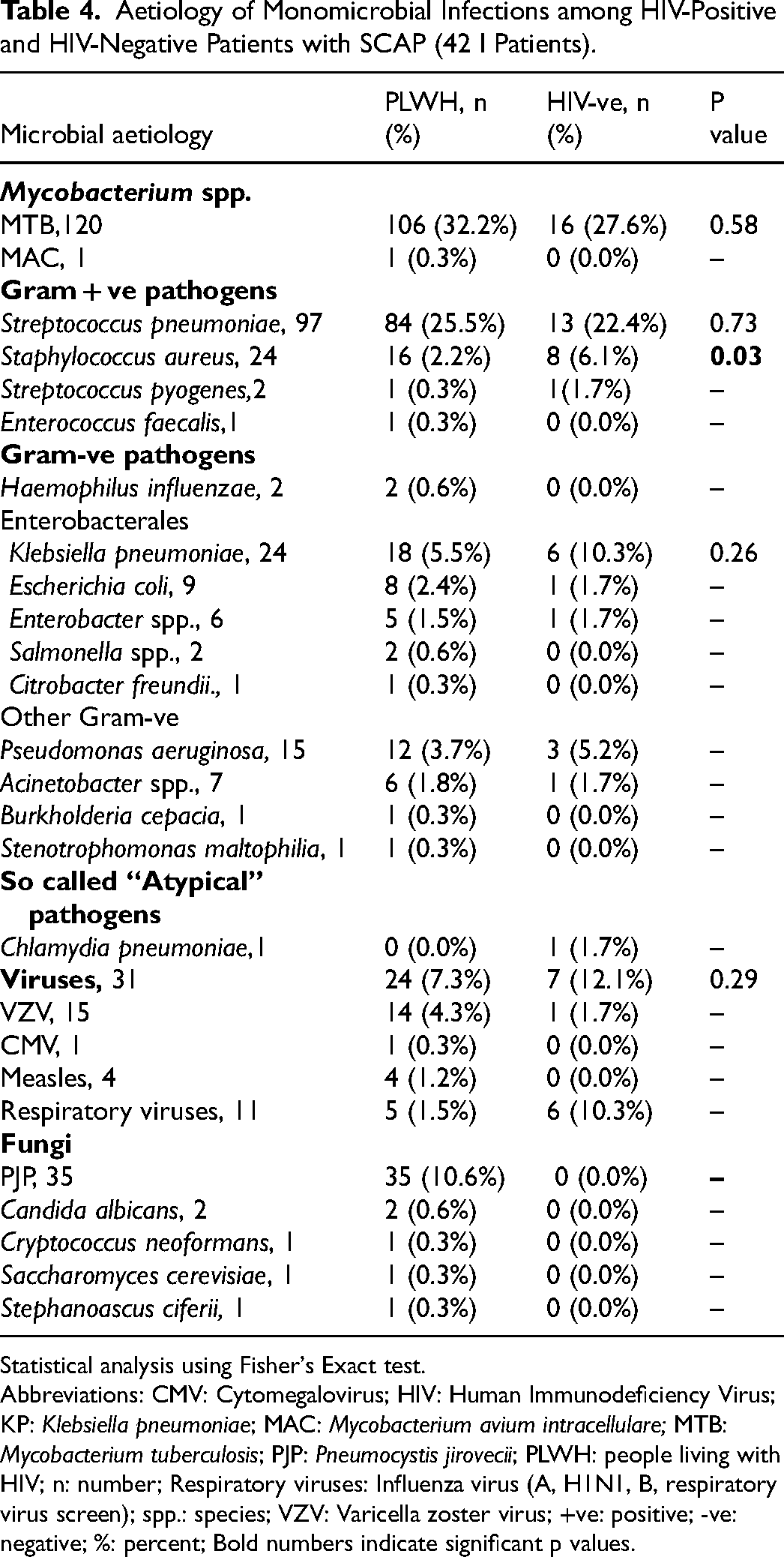
Statistical analysis using Fisher's Exact test.
Abbreviations: CMV: Cytomegalovirus; HIV: Human Immunodeficiency Virus; KP: Klebsiella pneumoniae; MAC: Mycobacterium avium intracellulare; MTB: Mycobacterium tuberculosis; PJP: Pneumocystis jirovecii; PLWH: people living with HIV; n: number; Respiratory viruses: Influenza virus (A, H1N1, B, respiratory virus screen); spp.: species; VZV: Varicella zoster virus; +ve: positive; -ve: negative; %: percent; Bold numbers indicate significant p values.
There were similar proportions of drug-resistant pathogens among PLWH and HIV-negative patients (22 (3.1%) versus 4 (3.1%), respectively) and although all drug-resistant MTB infections were in PLWH, numbers were too small to obtain statistically meaningful values.
There were no differences in the use of mechanical ventilation (MV) (invasive (IMV) or non-invasive (NIV)), dialysis, inotropic support, and corticosteroids in PLWH compared with the HIV-negative cases.
On univariate analysis (Supplementary Table 1), higher mean arterial pressure, PF ratio, and CRP levels were associated with a lower mortality, as were the presence of infection with S. pneumoniae, and lobar consolidation on chest radiograph. Higher Apache II and CURB-65 scores, as well as the presence of GGO on chest radiograph, and the need for ventilation and inotropic support (and trend for need for dialysis (P = .067)) were associated with a higher mortality. On univariate analysis, survival was lower in PLWH (354 (49.3%) compared to 80 (61.1%)) in HIV-negative cases (odds ratio (OR), 1.71; 95% CI, 1.08-2.70; P = .021).
A multivariate model was built as described in the methodology, which included all variables presented in Supplementary Table 2. While some of these variables predicted outcome, others did not, including APACHE II or CURB-65 scores. HIV-positivity per se was not noted to be a predictor of mortality (OR 1.111; 95% CI, .881-1.401; P = .373).
Among the PLWH, there were no differences in age, sex, or smoking habits in those who lived compared with those who died. A total of 225 (31.3%) PLWH were on antiretroviral therapy (ART), of which 111 (15.5%) were initiated prior to hospitalization, and 114 (15.9%) during ICU admission, and the proportion of patients who lived and died were similar regardless of whether they were initiated on ART, prior to or during, their ICU stay. The CD4 count was higher among patients on ART who lived, and the median level was 59 [IQR 23.5–122] cells/mm3 (P = .075) Cardiovascular disease was more common in patients that lived (47 (13.3%) versus 30 (8.2%); P = .03), while there was no difference in the overall presence of other co-morbidities among those who lived and those who died.
Table 5 documents the clinical presentation, laboratory results and chest radiography in PLWH that lived or died. CURB-65 and Apache II scores were significantly higher in non-survivors, whereas PF ratios were lower. Serum potassium and BDG were both significantly higher in PLWH that died than in survivors. BDG was also significantly higher in PLWH that died without documented fungal infections; however, in patients with PJP infection, BDG levels were similar between survivors and non-survivors. CRP, total serum protein, and albumin levels, as well CD4 cell counts in those not on ART were lower in the PLWH who died compared with survivors. There were no differences in HIVVL between the two groups. Bilateral GGO were the predominant finding among the patients who died, however, a higher proportion of survivors had lobar or multilobar consolidation on CXR.
Clinical Presentation, Laboratory Results and Chest Radiography among HIV-Positive Patients who Lived and Died.
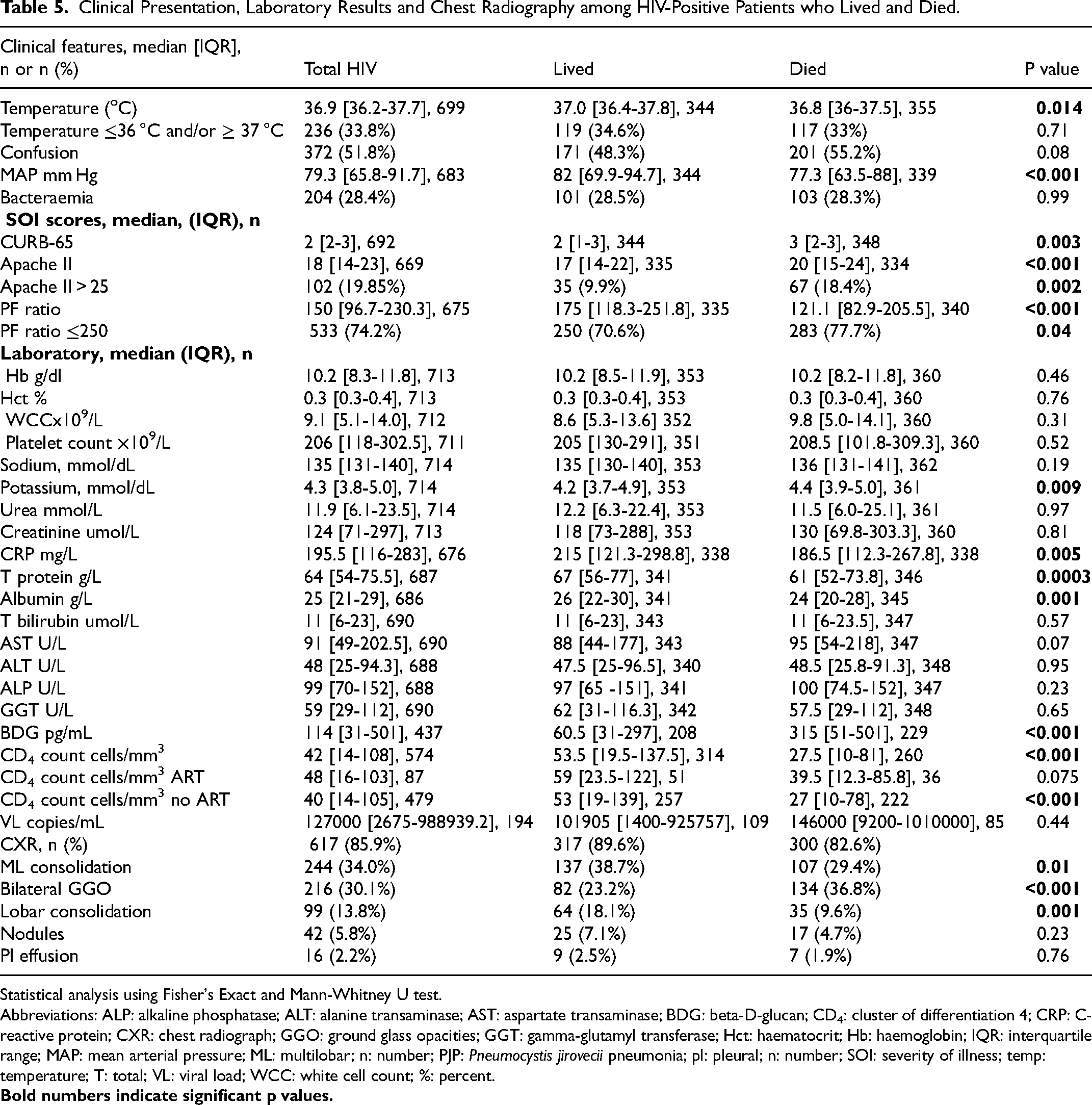
Statistical analysis using Fisher's Exact and Mann-Whitney U test.
Abbreviations: ALP: alkaline phosphatase; ALT: alanine transaminase; AST: aspartate transaminase; BDG: beta-D-glucan; CD4: cluster of differentiation 4; CRP: C- reactive protein; CXR: chest radiograph; GGO: ground glass opacities; GGT: gamma-glutamyl transferase; Hct: haematocrit; Hb: haemoglobin; IQR: interquartile range; MAP: mean arterial pressure; ML: multilobar; n: number; PJP: Pneumocystis jirovecii pneumonia; pl: pleural; n: number; SOI: severity of illness; temp: temperature; T: total; VL: viral load; WCC: white cell count; %: percent.
Supplementary Table 3 shows the comparison of outcomes and mortality among PLWH. Length of stay (LOS) in ICU was similar between PLWH that lived versus those that died. Slightly fewer PLWH survived ICU and survived to hospital discharge.
Supplementary Table 4 shows a comparison of outcomes and mortality comparing PLWH and those that were HIV-negative. There is a statistically significant relationship between HIV status and ICU survival.
Supplementary Table 5 describes the monomicrobial infections in PLWH and their effect on mortality. No difference in survival was noted among PLWH when no identifiable pathogen was documented. SP infection was more common in survivors; however, PJP infections and Acinetobacter spp., infections were higher in non-survivors. There were no differences in the frequency of MTB, Gram-negative or viral infections between the two groups.
A higher proportion of PLWH that required MV died; however, more patients who received NIV survived compared to those on IMV. Moreover, there was no difference in survival in patients on NIV compared to no form of MV. Inotrope use was higher in patients that died, but there was no difference in corticosteroid use or dialysis between the two groups (Supplementary Figure 1).
Discussion
This study described a large cohort of patients with SCAP, of whom a significant proportion were PLWH, in a geographical region with a high HIV burden. The cohort was young, determined mainly by the significantly younger age of PLWH. There were more females among PLWH, with more males in the HIV-negative group. MTB was the most common pathogen in both groups, followed by SP. The mortality of PLWH was higher on univariate analysis (OR 1.71; 95% CI 1.08-2.70; P = .02), but HIV per se did not remain a predictor of mortality when corrected for covariates on multivariable analysis.
The younger age, largely due to PLWH, is similar to the findings of other studies from South Africa,12,32,43–45 as well as some international studies with significant numbers of PLWH,3,35 but differs from other international studies of SCAP, in which patient age was considerably higher.46–50 The younger age of the current cohort is representative of the South African population, which has a median age of 27.6 years (62.2% between 15-60 years), with PLWH comprising 18.7% of those aged 15–49 years. 51
The frequency of the different comorbidities varies in studies of SCAP, most likely reflecting local disease patterns, the average age of the population, and their habits. 48 For example, the proportion of PLWH in this cohort was much higher than in other studies. 46 The reason for the high number reflects the demographics of the South African population, which has the largest number of PLWH in the world, with 13.7% of the general population infected, and up to 20% of those aged between 15 and 49 years. 52 Only 15.5% of PLWH in this study were using ART prior to admission; unfortunately, this study was not able to determine why this was the case, it is important to recognise that the ART program in South Africa was only initiated in 2004, and initially only among patients with very low CD4 cell counts. Since this study began in early 2007, this may have accounted for some of these findings in the earlier years. A study performed more recently at CMJAH did elucidate additional reasons. 53
There were an almost equal number of male and female patients in the current study, which differs from several other international SCAP studies which had a higher proportion of males.7,34,46,47,49,50,54,55 This was due to PLWH being more commonly female and more females are living with HIV in South Africa, 51 especially in the 15–24-year-old age group. 52
The original validation of CURB-65 39 excluded PLWH, those with suspected pulmonary Tb (PTB), and studied an older population. The median CURB-65 score in the current cohort was higher in patients who died (P = .002). However, PLWH tended to have lower CURB-65 scores compared to those without HIV (P = .06), although all were cases admitted to ICU. This finding is consistent with other CAP data, in which PLWH hospitalised with CAP also had lower CRB-65 (CURB-65 excluding urea) and pneumonia severity index (PSI) scores. 18 Possible reasons include the younger age of PLWH, and the infrequent finding of confusion and hypotension in patients with PJP. 56 As such, the CURB-65 score is an imprecise tool for assessing severity in this population.
The median Apache II score was 18 [IQR 14-23] in PLWH, with a predicted mortality of 24% [IQR 15%-40%], lower than the mortality in this study. It has previously been shown that the Apache II score underestimates mortality in patients with SCAP requiring IMV, 57 and/or in those with a low total lymphocyte count, pneumonia or sepsis. 58 In this study, however, the Apache II score was higher in patients that died and in PLWH, and it was also an independent predictor of mortality on MVA in the original study, 37 similar to other studies of SCAP.47,57 Furthermore, the PF ratio was shown to be an independent predictor of mortality (both univariate and multivariable analysis) as was noted in the original study. 37 While those who died had a lower mean arterial pressure (MAP) and more inotrope use, there were no differences in these parameters between PLWH and HIV-negative cases.
Albumin levels were significantly lower in PLWH than HIV-negative patients. This may reflect pneumonia severity, 59 or the large proportion of PLWH, the majority of whom were not on ART, as albumin levels in PLWH are lower pre-ART and correspond with weight and CD4 cell count. 60
Similar to other SCAP studies in both PLWH and HIV-negative patients,3,47,54,55,57,61 multilobar consolidation was the predominant radiological finding (34.7%) with a similar incidence in both groups. Ground-glass opacities were more common in PLWH and were significantly associated with PJP infection and associated with a higher mortality. Patients with lobar consolidation, more common in HIV-negative patients and in those with SP and MTB infection were, regardless of HIV status, more likely to live, similar to other data from Pune. 34
An identifiable microbial cause was found in 478 (56.3%) of cases, more commonly in the HIV-negative group. This is lower than other studies,35,47,62 probably related to their use of more comprehensive diagnostic techniques.
The current study found that MTB was the most common organism, regardless of HIV status, both among mono- and polymicrobial infections. This reflects the high burden of tuberculosis in the community which is strongly related to HIV infection.2,63 MTB had no impact on mortality, even in PLWH, although a high mortality has previously been noted in pneumonia patients admitted to ICU. 64
SP was the second most common bacterium isolated in both groups. This differs from studies, in which the pneumococcus is the predominant pathogen, 65 although, most SCAP studies have excluded patients with Tb and/or PLWH.7,34,43,46,49,50 On univariable analysis, patients with pneumococcal infection had a lower risk of mortality even in PLWH. SA infections, although well described in PLWH,1,66 were more common in the HIV-negative group.
There were a similar number of infections due to Gram-negative enteric bacteria (GNEB) in PLWH compared with the HIV-negative group. However, in another SCAP study, there were more in PLWH relative to the HIV-negative group (20% vs 0%; P < .001), 35 and in yet another study, a high incidence of Pseudomonas aeruginosa (PA) was noted in PLWH with SCAP (17.9%), which was associated with a mortality of 20.6%. 67
Varicella zoster virus (VZV) infections were the most common viral infection, with most in PLWH, of whom most survived (10 (71.4%) lived and 4 (28.6%) died). Respiratory viruses were more common in HIV-negative patients; however, there were no differences in mortality overall. All PJP infections occurred in PLWH and were responsible for 10.6% of all monomicrobial infections.
A total of 10.5% of patients had polymicrobial infections, the third most common aetiology, occurring more commonly in PLWH. This was similar to a cohort of PLWH with CAP, 3 in which 11.5% of infections were polymicrobial (after SP and PJP). In the current study, there was no increased mortality among patients with polymicrobial infections.
Although 26.6% of infections in the current study were bacteraemic, more common among PLWH (P = .008), it was not associated with mortality in PLWH. Park et al, reported a trend towards more bacteraemia in patients with SCAP compared to those without (14% vs 8%; P = .07). 35
In the ICU, 726 patients (85.5%) were ventilated, (predominantly IMV), with a similar proportion in PLWH and HIV-negative patients, and this was higher than in other SCAP studies.46,49,54,57,68 There was also an increased mortality where IMV was required, which is compatible with another cohort of PLWH with CAP, in which 15.4% required IMV and had an increased 30-day mortality. 3 Intravenous CS were used in most patients in the current study (650 (76.6%)) of which some may have been for adjunctive therapy of PJP; however, there was no mortality difference noted in those that did or did not receive CS overall. Other studies have noted benefit with the use of CS in SCAP.26,69–72
Fifty percent of all patients required inotropic support, associated with increased mortality, as noted in other studies of SCAP.49,50,73 There were no differences in the use of IMV or NIV, dialysis, or inotropic support, between PLWH and HIV-negative cases.
The ICU LOS in the current study was increased in patients on IMV and who required renal dialysis and was similar regardless of survival (P = .072). Furthermore, LOS was similar between PLWH and HIV-negative patients. Other studies of PLWH with CAP have noted a difference in hospital LOS depending on the pathogen isolated (10 days with PJP infection vs 7 with bacterial CAP, P = .03). 3
Overall ICU mortality was 48.9%, similar to SCAP studies from Johannesburg (47.4%) 43 and in Pretoria, South Africa, 12 but higher than in other SCAP studies.34,46,48–50 Although PLWH had a higher risk of mortality than their HIV-negative counterparts on univariate analysis, with a similar trend on MVA, HIV was not found to be a predictor of mortality when considered in the context of other covariables on multivariable analysis. Cilloniz et al, reported a 30-day mortality of 6.6% in PLWH with CAP, which was lower with a bacterial aetiology compared to PJP infection (5.5% vs 14.3%, P = .03), but higher than in HIV-negative patients. 3 Cordero et al, also reported an attributable mortality of 13.1% for PLWH with SCAP, and this was associated with radiological progression, septic shock and CD4 count <100 cells/mm3. 67 Within our cohort, the median CD4 count was 44 (95% CI, 14-110.5) cells/mm3, and the higher mortality noted may reflect the larger proportion of patients with HIV co-infection with MTB, PJP and other opportunistic infections.
This study appears to be the largest study of SCAP in PLWH. Nevertheless, it has potential limitations. First, it was a single-centre study from South Africa, and so the findings may not be generalizable. Second, it only included cases with SCAP admitted to ICU, and so the findings are only pertinent to this category of patients. Third, the study was a record review and since there was limited access to electronic medical records, much of the data had to be retrieved from stored files, some of which were incomplete and, because they did not allow confirmation of the diagnosis of CAP, these cases were excluded, with the consequence that there may have been a significant underestimation of the number of cases of SCAP. Fourthly, due to initial unavailability, and subsequent limited use of the more modern microbial diagnostic techniques because of resource constraints, it is likely that a proportion of pathogens, specifically viruses and atypical microorganisms, may have been undiagnosed, although putative pathogens were documented in 56.3% (n = 478) of cases. Lastly, it was concerning to note in this cohort of patients with SCAP, as mentioned previously, that the frequency of antiretroviral therapy (ART) use was extremely low, with associated low CD4 cell counts and high viral loads in most of the patients, clearly significantly contributing to their poor outcome. This may have been different in the presence of a highly successful ART programme as currently exists in South Africa. 74 However, the initial approach of the South African Government to HIV in the first decade of its occurrence has previously been described as being denialist, and it was only in the later years, certainly post 2008, that the ART programmes expanded aggressively. 74 Nevertheless, there still remain a number of individuals who are unaware of their HIV status, and therefore are not on ART, who only become identified once they present with a significant infectious illness, such as SCAP.
Conclusions
This was a study of 849 patients with SCAP admitted to ICU at a tertiary referral hospital and appears to be the largest ICU cohort of patients with SCAP. The study documented various similarities and differences between the two groups of patients. The ICU mortality of 48.9% was very high and while PLWH appeared to have a higher risk of mortality than their HIV-negative counterparts, HIV per se was not a predictor of mortality on multivariable analysis.
Supplemental Material
sj-docx-1-jic-10.1177_08850666251359546 - Supplemental material for Severe Community-Acquired Pneumonia: Impact of HIV on Clinical Presentation, Microbiological and Laboratory Findings, and Outcome
Supplemental material, sj-docx-1-jic-10.1177_08850666251359546 for Severe Community-Acquired Pneumonia: Impact of HIV on Clinical Presentation, Microbiological and Laboratory Findings, and Outcome by JP Venturas, A Titus, GA Richards and C Feldman in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.