
Abstract
Survivors after pediatric critical care often have adverse sequelae in domains of cognition, executive function, attention, memory, visual-spatial skills, language, motor function, behavior, and emotional functioning, the post-intensive-care syndrome pediatric (PICS-p). The time from birth to approximately age 2 years is a period of rapid structural and functional brain development. The fundamental structural and functional architecture of the brain is in place by the second year of life. This narrative review focuses on how we, in the pediatric intensive care unit (PICU), can work towards maximizing each patient's full potential despite adverse experiences during hospitalization. In part I, concepts relevant to understanding the effects of hospitalization in PICU on brain development are clarified, including concepts of toxic stress and trauma, sensitive periods and cascades, experience-expectant neural plasticity in the early years, and resilience and buffering of adversity focused on relational care. In part II, evidence is presented that these concepts are important because they describe the effects of early childhood adversity that are pervasive on physical health, cognitive, and emotional outcomes throughout the lifespan. Evidence is presented to show that intervention to improve these outcomes can be effective. In part III, the concepts and evidence are synthesized by focusing on the opportunity before us, what we must and can do better while patients are in the PICU, in order to improve their long-term lifelong outcomes. We present evidence to argue that we in pediatric critical care must take a public-health approach to address the key environmental conditions necessary for optimal early childhood development and hence facilitate children's ability to thrive. Future research must aim to determine what works best and what does not work in the PICU. Early childhood investments to improve lifelong outcomes have great potential to help patients and reduce the growing burden of healthcare costs.
Keywords
Introduction
The time from birth to approximately age 2 years is a period of extremely rapid structural and functional brain development. 1 The basic fundamental structural and functional framework and architecture of the brain is in place by the second year of life. 1 This is a time of gray-matter growth, myelination and maturation of the microstructure of white-matter tracts, and the development of resting-state functional networks. 1 Brain development after this period mainly consists of reorganization, that is, fine-tuning of the major circuits and networks that had already been established. 1
As shown in Figure 1, brain tissue volume is 35% of adult volume at 2–3 weeks of age, and doubles in the first year, increasing another 15% in the second year (to approximately 80% of adult volume). 1 The cortical grey matter volume increases 108–149% and 14–19% in the first and second years respectively. 1 The cortical surface area increases approximately 76% and 22% in the first and second years respectively. 1 Cortical thickness peaks in the first 1–2 years of life. 1 In addition, the complexity of cortical neurons increases rapidly, peaking at age 2–4 years. 1 Functional brain networks have established their topologies by 2 years of age, including the default mode network (at approximately 6 months), the language network (with established asymmetry at approximately 1 year), the dorsal attention network (with an inverse correlation with the default mode network by 1 year), and the salience network, each with most major hubs and modules in place, and increased network integration (ie, interconnections, as opposed to segregated localized nodes and modules). 1
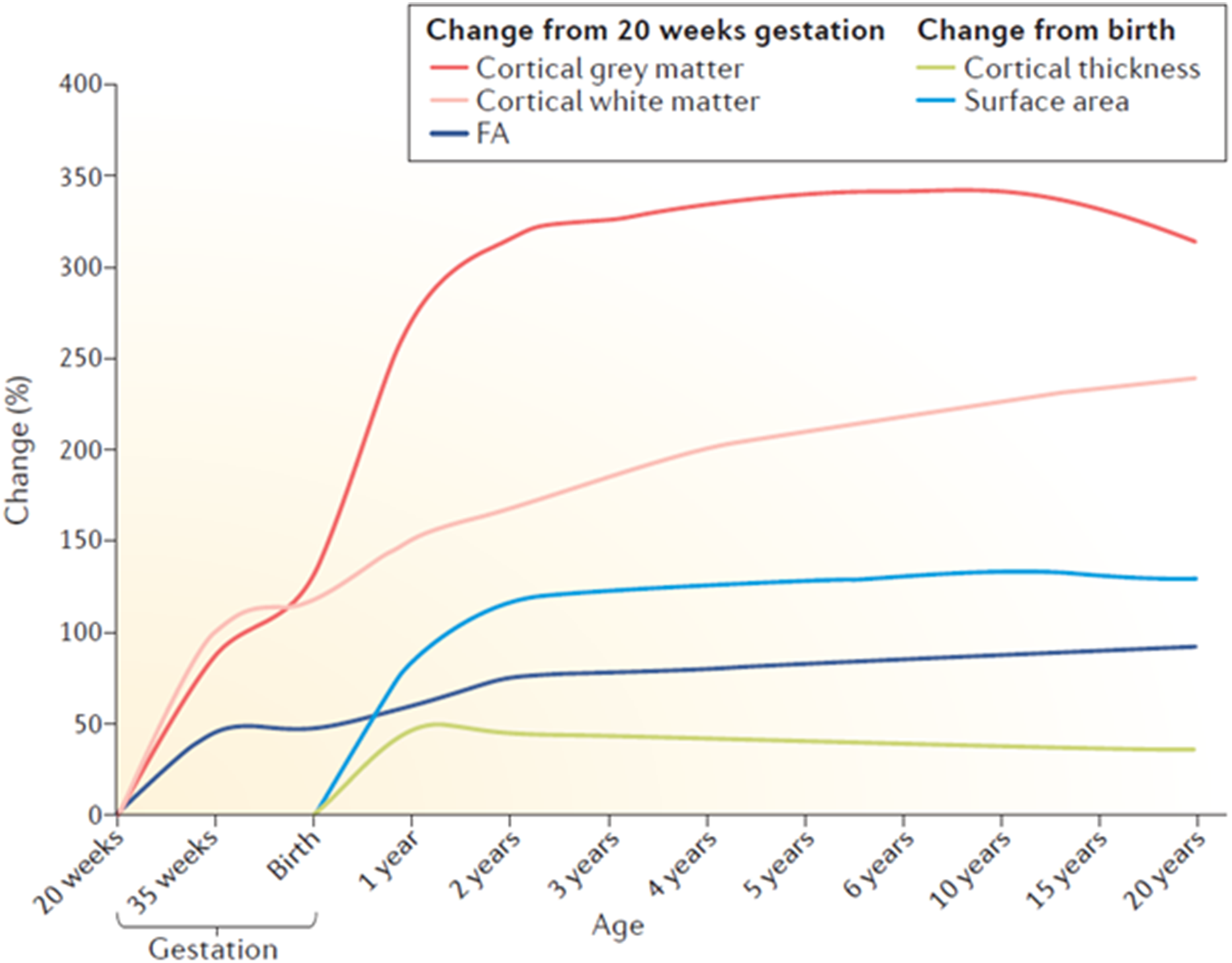
Estimated Trajectories of Brain Structural Parameters During Development.
With this background, it is obvious that the first two years are crucial to establishing cognitive abilities and behaviors that will last a lifetime. This review focuses on how we, in the pediatric intensive care unit (PICU), can work towards maximizing each patient's full potential despite adverse experiences during hospitalization. The review is organized as follows. In part I, concepts relevant to understanding the effects of hospitalization in PICU on brain development are clarified. This includes concepts such as toxic stress and trauma, sensitive periods and cascades, experience-expectant neural plasticity in the early years, and resilience and buffering of adversity focused on relational care. In part II, evidence is presented that these concepts are so important because they describe the effects of early childhood adversity that are pervasive on physical health, cognitive, and emotional outcomes throughout the lifespan. Evidence is also presented to show that intervention to improve these outcomes can be quite effective. In part III, the concepts and evidence are synthesized by focusing on the opportunity before us, what we must and can do better in the PICU, in order to improve the long-term lifelong outcomes of our patients.
Concepts and Terminology: Childhood Adversity and the PICU
Concepts: Problem Focused
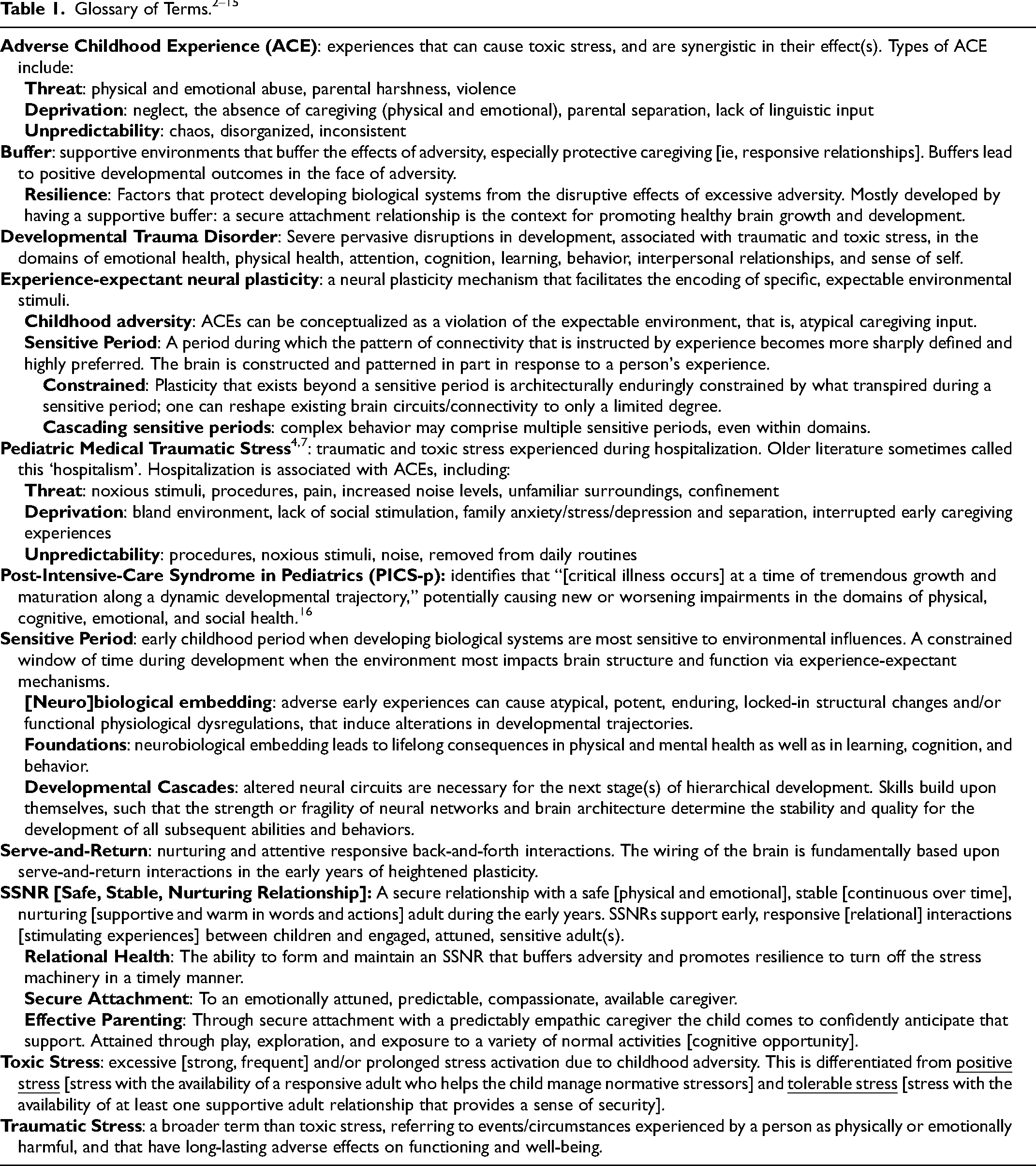
There are several terms and concepts that are important to understanding the problem facing us [Table 1: Glossary].2–15 Toxic and traumatic stress are typically seen when protective relationships are not available (ie, lack of a buffer contributing to resilience) or when the important relationship itself is the source of threat.2–4 Adverse childhood experiences (ACE) cause toxic stress and are synergistic in their effect(s).4–7 The GET framework suggests that genetic differences (ie, susceptibility), environmental exposures (ie, ACEs, including threat, deprivation, and unpredictability), and timing (ie, early during brain development) determine the effect of these experiences on the developing brain. 5 Pediatric Medical Traumatic Stress occurs during hospitalization, often a negative experience particularly in a PICU, leading to all three types of ACE.4–7
This toxic and traumatic stress is most important during sensitive periods of development. During these sensitive periods, disruptions of developing brain circuitry, architecture, and functioning become neurobiologically embedded.2,3,6,8–10 Essentially, neurobiological embedding means that what happened during sensitive periods lays the foundation for that person's entire future lifetime. A reason these embeddings are so foundational for a person's future potential is that there are developmental cascades, as skills build upon themselves; altered neural circuits are necessary for the next stage(s) of hierarchical development.2,3,6,8–10 For example, language development involves multiple sensitive periods, those for performing low-level more fundamental basic computations end before those that affect circuits processing more advanced higher-order aspects. 14 In other words, the first few years of life are windows of opportunity for positive, but also negative, effects - the origins of lifelong health are in early childhood. Early psychosocial adversity leads to biological change that in turn determines behavior change and adult outcomes, potentially causing lifelong impairments in physical, mental, and relational health. 9 These biological changes are embedded in altered physiology in body systems, with dose response effects, that are cumulative, and responsive to experience. 10 Changes include variation in brain structure and function (eg, activity and connectivity), neuroendocrine stress regulation (eg, hypothalamic-pituitary-adrenal axis and autonomic axis changes that predict stress-related chronic diseases), and immune functioning (eg, chronic inflammation with compromised control of infection, and disease risks).9,10 The mechanisms are complex, including effects on gene expression and telomere length (ie, epigenetic changes), brain development, and immunity at molecular and cellular levels.2,3,6,8–10
The explanation for how toxic and traumatic stress, that is, ACEs, can cause such neurobiological embedding has to do with experience-expectant neural plasticity.9,11–13 Violations of the expectable environment, in this case childhood adversity, are violations of species-expected caregiving conditions and alter the course of brain development. 14 These violations can occur when experiences that are universally expected do not occur (eg, lack of caregiving, poor complexity and stimulation, lack of essential input), and/or when experiences are atypical (eg, physical abuse). Violations of expected experience exert a profound influence on the brain, shaping brain development, and therefore determining behavior by consolidation (ie, embedding) of abnormal circuit connectivity.9,11–13 The brain may not receive typical or adequate instructions to guide its assembly. 12 This reliance on experience-expectant input explains why there are sensitive periods during development, constrained windows of time when the environment impacts brain structure and function most, where the pattern of connectivity is instructed by experience.9,11–13 Adverse experiences can disrupt cellular and molecular processes that regulate the structural and functional formation of neural networks and circuits that underlie cognition and behavior, laying the foundation for future learning. Mechanisms include that intense impulse activity from experience activates plasticity molecular cascades (ie, customizing developing neural circuits to the individual's needs), for example, axon elaboration and synapse formation based on activity, axon and synapse elimination (pruning) based on inactivity, and synapse consolidation.11–13,15
This experience-expectant mechanism can be leveraged for advantage. The wiring of the brain is fundamentally based upon serve-and-return interactions in the early years of heightened plasticity for the formation and functional maturation of the brain.6,11–13,15 The complex crucial neural circuits and connections are being formed and refined through an interplay of neural activity (excitatory and inhibitory neural input), synaptogenesis, pruning, myelination, and neurogenesis.9,15 This provides a unique advantage to early experience, that occurring before a circuit has ever been activated strongly (ie, when it is in a state that favors change). 13 Of great importance, there is a precipitous drop in brain plasticity after the first few years of life – in other words, it is easier to change a brain being constructed than a brain already built. 17 We can influence experience which in turn determines the extent to which a brain blueprint is carried out, 17 impacting neural mechanisms that mediate cognitive, language, and emotional outcomes.
Concepts: Solution Focused and Strength Based
There are concepts that explain how to buffer the effects of adversity and produce resilience to that adversity. We need to think of establishing safe, stable, nurturing relationships (SSNRs) as a public health approach to early childhood – “relational health, in the form of at least one SSNR, is a universal biological imperative [necessary in order] for children to fulfil their potential”, in order for children to be healthy, “successful academically, economically, and socially”, and in the future “to be the caregivers that value and build SSNRs for subsequent generations”. 18 At least one SSNR entails effective parenting and attachment, leads to relational health and associated resilience, hence buffering the effects of adversity on brain development.4,7,18,19 These early, responsive, stimulating interactions between children and engaged, attuned, sensitive, loving adults are the supportive caring relationships necessary to decrease stress responses, and provide optimal experience-expectant input to the developing brain.4,7,18,19
Without SSNRs, children experiencing adversity, including hospitalization in the PICU, may develop what has been called developmental trauma disorder. 4 This disorder is the result of effects on the limbic system [involved in interpreting the emotions of others, eg, being attuned to low-pitched sounds that warn of caregiver depression and anger, and focused on safety and a presumption of danger], hippocampus, prefrontal cortex [involved in cognition, emotional regulation, attention, impulse control, and other executive functions], and immune system [with persistent inflammatory response, impaired humoral immunity, and sick syndrome, the perception of feeling unwell with headaches, stomach aches, and lethargy]. 4 Signs of this disorder may sound familiar to those working in the PICU, organized around the pneumonic “FRAYED”: Frets and fears (anxiety and worry); Regulation difficulties (hyperactive, impulsive, easily becomes aggressive or emotional); Attachment challenges; Yawning (sleep problems) and yelling; Educational and developmental delays (cognitive, social-emotional, communication), and Defeated (hopelessness, depressed, dissociated). 4
Evidence: the Effects of Adversity on Health and Cognitive Development
Evidence: Effects on Health
The number of ACEs has been associated with premature mortality, cardiovascular disease (including coronary heart disease and stroke), diabetes mellitus, cancer, and respiratory infections, often refractory to later life change. 20 Early life adversity is one of the strongest known predisposing factors for the most common, and expensive, chronic non-communicable health conditions affecting adults.20–24 These early roots of human disease and lifelong health, the upstream, common, and preventable causes of morbidity and mortality, should be considered a critical public health priority.20–24 Childhood adversity is common, and it has been estimated to be, in the United States in 2019, the cause of over 15% of annual mortality, to lead to over 1/3 of suicide attempts, and contribute significantly to non-communicable diseases related to chronic inflammation (eg, heart disease, cancer, chronic lower respiratory disease, stroke, diabetes, metabolic syndrome).21,22 In addition, childhood adversity has cascading influences on social, emotional, and cognitive development that culminates in an increased risk for unhealthy behaviors and other disease markers, including substance use (illicit drug use, alcohol consumption), sexually transmitted diseases, physical inactivity, tobacco smoking, obesity, interpersonal and self-directed violence, and mental ill-health.21,22 Indeed, ACEs cause increased risk for many adult health outcomes in a dose-dependent manner, causing pervasive harm on health throughout the life-course. 22 The changes in development of the nervous, endocrine, and immune systems that result in impaired cognitive, social, and emotional functioning also cause broad harms to life prospects (eg, education, employment, poverty) and intergenerational effects (eg, can lock families into cycles of adversity and poor health). 22
Evidence: Effects on Cognitive Development
The only randomized controlled trial (RCT) to convincingly demonstrate that institutional rearing in early childhood, that is, being “deprived from the opportunity to develop attachment relationships with stable, primary caregivers… [and also] miss out on critical sensory, cognitive, linguistic, and emotional input,” 14 has severe causative effects on development was the Bucharest Early Intervention Project (BEIP).11,12,17,25 The BEIP also showed that “sensitive, consistent caregiving that is responsive to a child's needs is one of the most powerful interventions available” for childhood development. 11 The communist leader of Romania from 1965–1989, Nicolae Ceausescu, banned contraception and abortion, and imposed a tax on families with less than 5 children, aiming for rapid population growth. This led to many abandoned children, which he ‘solved’ by building state-run institutions to basically warehouse these children, with over 170 000 institutionalized children in 1990. The BEIP was an RCT of foster care (with timing/age determined by the fall of Ceausescu's regime) versus continued institutional care following early exposure to severe psychosocial deprivation. Those randomized to foster care had, even 16 years after randomization, higher full-scale intelligence quotient (FSIQ) by 9 points (0.6 of a standard deviation), and higher verbal comprehension (by 11 points) and processing speed (by 8 points). 25 A longer period of experienced institutional caregiving in the fostered children was associated with lower FSIQ at age 18 years. 25 Unfortunately, later optimized caregiving was not sufficient to completely reverse the lasting impact of psychosocial deprivation, with children having any history of institutionalization having a FSIQ 26.2 points below contemporary Romanian community participants.12,25 Those randomized to foster care, especially when placed before the age of 2 years, and when the foster placement was stable over time, also had improved electroencephalogram patterns, white matter volume, prefrontal cortex (PFC) thickness, indiscriminate behavior through age 8 years, stress responsivity (eg, sympathetic and cortisol reactivity at age 12 years), psychiatric symptoms/disorders, and peer social competence.11,12,17,25 The BEIP also found sensitive periods for rescuing brain development, and these periods closed at surprisingly young ages (eg, for language, reading, IQ, social skills, and stress responsivity) (Table 2). 12 Some effects of deprivation were mostly unaffected by foster care (eg, attention deficit hyperactivity disorder symptoms, and most executive functions) or had no obvious sensitive period (eg, psychiatric symptoms/disorders). 12
Selected Sensitive Periods Suggested in the Bucharest Early Intervention Project. 12
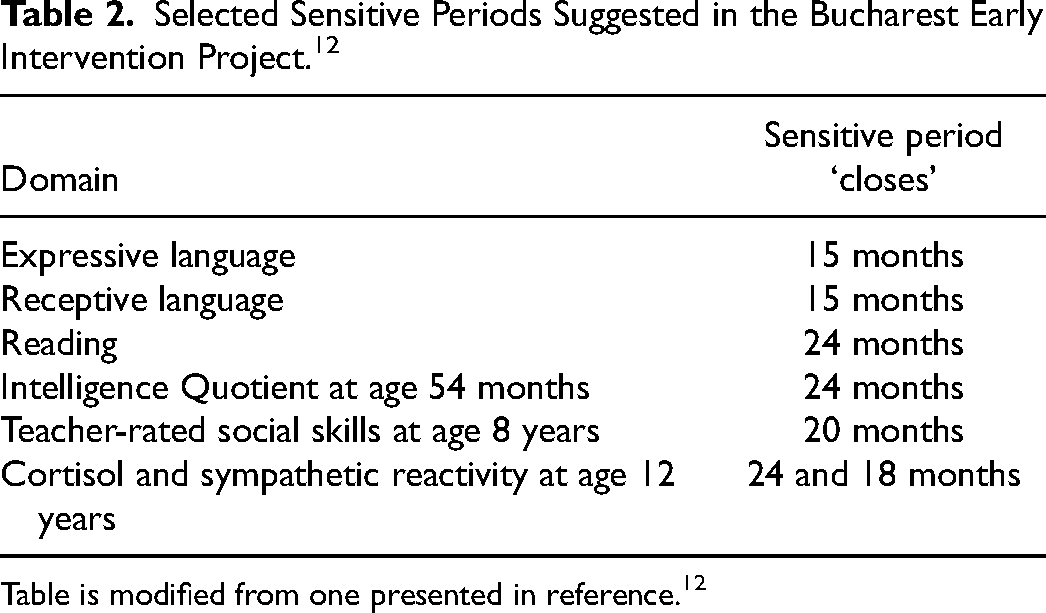
Table is modified from one presented in reference. 12
Another non-randomized natural experiment compared outcomes after adoption into UK homes after institutional care in Romania from early infancy (up to approximately 42 months) versus children adopted within the UK before age 6 months, the English and Romanian Adoptee (ERA) study.26,27 In this study adoption from Romania at the age of 6 months marked a division between children without appreciable sequelae from those with a high proportion of persisting deficits.26,27 After adoption there was substantial but incomplete recovery up to the age of 6 years, with prolonged neglect in Romanian institutions leading to “remarkably persistent deprivation specific psychological patterns”. 26 These patterns included i) quasi-autistic patterns of social behavior (eg, problems in social reciprocal interaction, communication, and repetitive and stereotyped behaviors), ii) disinhibited social engagement (eg, inappropriate intrusiveness, unaware of social boundaries, too friendly), iii) inattention/overactivity, and iv) cognitive impairment (eg, including theory of mind, executive planning, scholastic achievement, intelligence quotient, mathematical reasoning, basic reading, and reading comprehension, usually by at least 1 standard deviation).26,27 There was “profound and lasting psychological impact despite subsequent environmental enrichment in well-resourced and supportive families” that was of early onset, clinically significant and impairing, and highly persistent into adulthood (age 22-25 years). 28 Although cognitive impairment may have recovered to closer to FSIQ ∼90 at young adulthood, this is uncertain as in that study there was high attrition (of 27% between adolescence and young adulthood), especially in those with parent-rated emotional problems. 28 Outcomes at age 22–25 years included unemployment in 36% (OR vs UK adopted controls 6.26), low educational attainment (equivalent to grade 11) 40% (OR 5.45), mental health service use 43% (OR 13.34), autism spectrum disorder symptoms ∼18% (OR 3.1), disinhibited social engagement symptoms ∼14% (OR 2.5), attention deficit hyperactivity symptoms ∼32% (OR 3.6), emotional symptoms (depressed mood, worry, social anxiety) ∼45% (OR 1.9), and conduct problems 12% (OR 2.1); of note, approximately half (∼54%) had none of these problems in young adulthood. 28 It was recommended that clinical services should not consider this form of deprivation-associated autism as transitory or benign. 29
These effects of lack of challenging environments and stable attachments were also noted in a systematic review of 42 studies from 1940–2006 of children growing up in children's homes compared to foster families, with an IQ or developmental quotient difference of 20 points, 84.4 (SD 16.8) versus 104.2 (SD 12.9); the difference was even more marked in those assessed before age 2 years and in those placed before age 1 year. 30 Another systematic review of 91 articles, 82 cohorts, with 31 188 individuals, found that early-life threat, and even more so, deprivation/neglect, had adverse effects on executive functioning (eg, “top-down effortful cognitive processes that enable an individual to control cognition, plan actions, solve problems, and engage in goal-directed behavior”) in childhood and adolescence. 31 The effect size of threat on inhibitory control and working memory were g = −0.27 and −0.28, and for deprivation were g = −0.43 and −0.54 respectively. 31 These effects influence health, education (academic success), and economic stability (productivity) across the lifespan. 18 Similarly, a systematic review of 11 studies examining child maltreatment association with cognitive functioning found that “childhood maltreatment [most pervasively childhood neglect] is considered as one of the most consistent factors related to later life cognitive dysfunction.” 32
These effects of adversity are mediated by their effect on developing brain structure and function. Several evidence reviews noted global changes in brain structure, with reduced brain volumes including in amygdala [important for processing emotion cues], hippocampus [important for declarative memory], PFC regions [orbitofrontal cortex important for reinforcement-based decision making, superior frontal gyrus important for working memory, and dorsolateral PFC important for working memory, cognitive regulation of emotion, and planning], and in white matter organization [eg, in pathways and connectivity, especially between PFC and parietal cortex].11,14,33 These reviews also noted functional changes in brain activation patterns, including in dorsal anterior cingulate cortex [during conflict monitoring], inferior PFC and striatum [during inhibitory and response control], amygdala [during negative emotion cues], ventral striatum and caudate [during response to reward], and orbitofrontal cortex, infralimbic PFC, and medial and lateral temporal lobe [during emotion regulation, error monitoring, and conflict detection].11,14,33 These findings indicate that “the brain requires patterned contingent [experience-expectant] input;” otherwise, there can be under-specification, miswiring, reorganization, and errors in brain development, causing altered brain structure and functioning and ultimately behavior. 11 There are complex changes in resting state functional connectivity reported in those with histories of childhood maltreatment, including in the central and peripheral hubs of connectivity (wiring) of brain networks. 34 Systematic reviews also find that these structural and functional brain changes are different for different types of adversity.35–37 Threat has effects on accelerated pubertal development, accelerated cellular aging, thinning of ventromedial PFC, and altered structure and function of fronto-amygdala circuits and the salience network, leading to risk of psychiatric and socioemotional problems, particularly related to a lower threshold and attentional bias towards detection of anger and threatening stimuli.35–37 Unpredictability had effects on reduced amygdala volume, and inconsistent effects on functional connectivity between PFC and amygdala, leading to risk of psychiatric and socioemotional problems.35–37 Deprivation (absence of expected environmental input or complexity) had effects on thinning in fronto-parietal, default, and ventral visual networks, altered structure and function of fronto-parietal network and fronto-striatal function, leading to risk for psychiatric and socioemotional disorders, cognitive and academic difficulties.35–37
In the ERA study, deprivation was associated with profound and enduring alterations in brain volume in young adulthood; the longer deprivation lasted, the more the adverse effect on brain volume, which mediated the association between deprivation with lower IQ and attention-deficit hyperactivity disorder. 38 This again demonstrated that extraordinary environments have the potential to override underlying genetic potential. 38 The enduring aspect of these findings are supported by the Norwegian Mother-Child cohort study that identified “an extensive cortical region [especially PFC and medial and posterolateral temporal cortex] wherein surface area related positively to general cognitive ability at age 4 years old.” 39 There was “remarkable stability in individual general cognitive ability relative to same-age peers”, and the cortical area change trajectories of higher and lower general cognitive ability groups “were parallel through life suggesting continued influences of early life factors”, that is, early life factors impact brain structure and cognitive function for the entire life course. 39
Evidence: Building Resilience with Trauma-Informed Care
There is evidence that we can improve outcomes by building resilience with trauma-informed care, which addresses the adversities of deprivation, threat, and unpredictability.2,4,6,7,18 How this can be done will be discussed in section III. The efficacy of intervention is discussed here.
A systematic review of 61 RCTs examined parenting interventions in early childhood, those that focused on improving sensitivity, responsiveness, and/or non-harsh discipline, ie, based on the hypothesis that brain development is “in part, constructed within cooperative social exchanges.” 40 This meta-analysis found that positive parenting interventions in infancy and early childhood caused an improvement of in mental abilities, measured by developmental quotient, IQ, and/or cognition scores, of g = 0.46 (33 studies); and in language abilities, measured by communication, receptive understanding, expressive production vocabulary, or speech production, of g = 0.25 (30 studies). 40 The effect on mental abilities was stronger in studies using standardized direct assessments of cognition, g = 0.53 (27 studies). 40 The effect on language outcomes was larger the earlier the age of intervention. 40 This is so important because early cognition is relatively stable across development, and predictive of several adult outcomes (eg, education, occupation, health, wellbeing). 40
Another systematic review examined 102 RCTs of parenting interventions in the first 3 years of life, those focused on improved interactions with their children, including stimulation (eg, shared book reading, early play and learning opportunities), attachment (eg, sensitivity and mental health), and behavior management (eg, positive nonviolent discipline). 41 The effect on cognitive development (56 studies) was a standardized mean difference (SMD) of 0.32, on language development (46 studies) a SMD 0.28, on motor development (35 studies) a SMD 0.24, on socioemotional development (29 studies) a SMD 0.19, and on behavior problems (29 studies) a SMD −0.13. 41 The effect on cognitive development was greatest for programs focused on responsive caregiving, those that promote and support “parental sensitivity and responsiveness in the context of play, communication, reading, and/or feeding.” 41 A systematic review of 21 RCTs examining childhood interventions focused on improving parenting skills in the first 3 years of life found positive effects on hypothalamic-pituitary axis (ie, morning and diurnal cortisol levels) and epigenetic regulation, especially with earlier timing of intervention, high quality and nurturant parenting traits (eg, responsiveness, sensitivity, and attachment), and greater intervention engagement. 42
The effect of early developmental intervention programs for premature babies in the neonatal intensive care unit (NICU) has been controversial, based on a Cochrane systematic review, updated in 2024, that found no effect on motor or cognitive outcomes at school age. 43 However, there was a statistically significant effect on cognitive outcome in the three studies where the early intervention started in the hospital (ie, in NICU, as opposed to after discharge), an IQ SMD 0.49 (p = .02). 43 In addition, in the 5 studies that focused on the parent-infant relationship there was suggestion of an effect, an IQ SMD 0.27 p = .06. 43
What We Must Do Better: Our Opportunity
Do These Findings Apply to PICU?
The short answer is, yes. The goal in critical care has shifted from preventing mortality alone, to the optimization of survivor outcomes, having the potential to affect the quality of the child's and family's life for their entire future. The concept of the Pediatric Post-Intensive-Care Syndrome (PICU-p) identifies that “[critical illness occurs] at a time of tremendous growth and maturation along a dynamic developmental trajectory,” potentially causing new or worsening impairments in the domains of physical, cognitive, emotional, and social health. 16 Survivors after pediatric critical care often have adverse sequelae in domains of cognition, executive function, attention, memory, visual-spatial skills, language, motor function, behavior, and emotional functioning (Table 3).44–53 These outcomes translate to lower educational achievement, diminished quality of life, and worse adaptive skills. 54
Recent Systematic Reviews of Long-Term Outcomes After Pediatric Intensive Care: a Significant Risk for Adverse Outcomes in all the Domains of PICS-p.
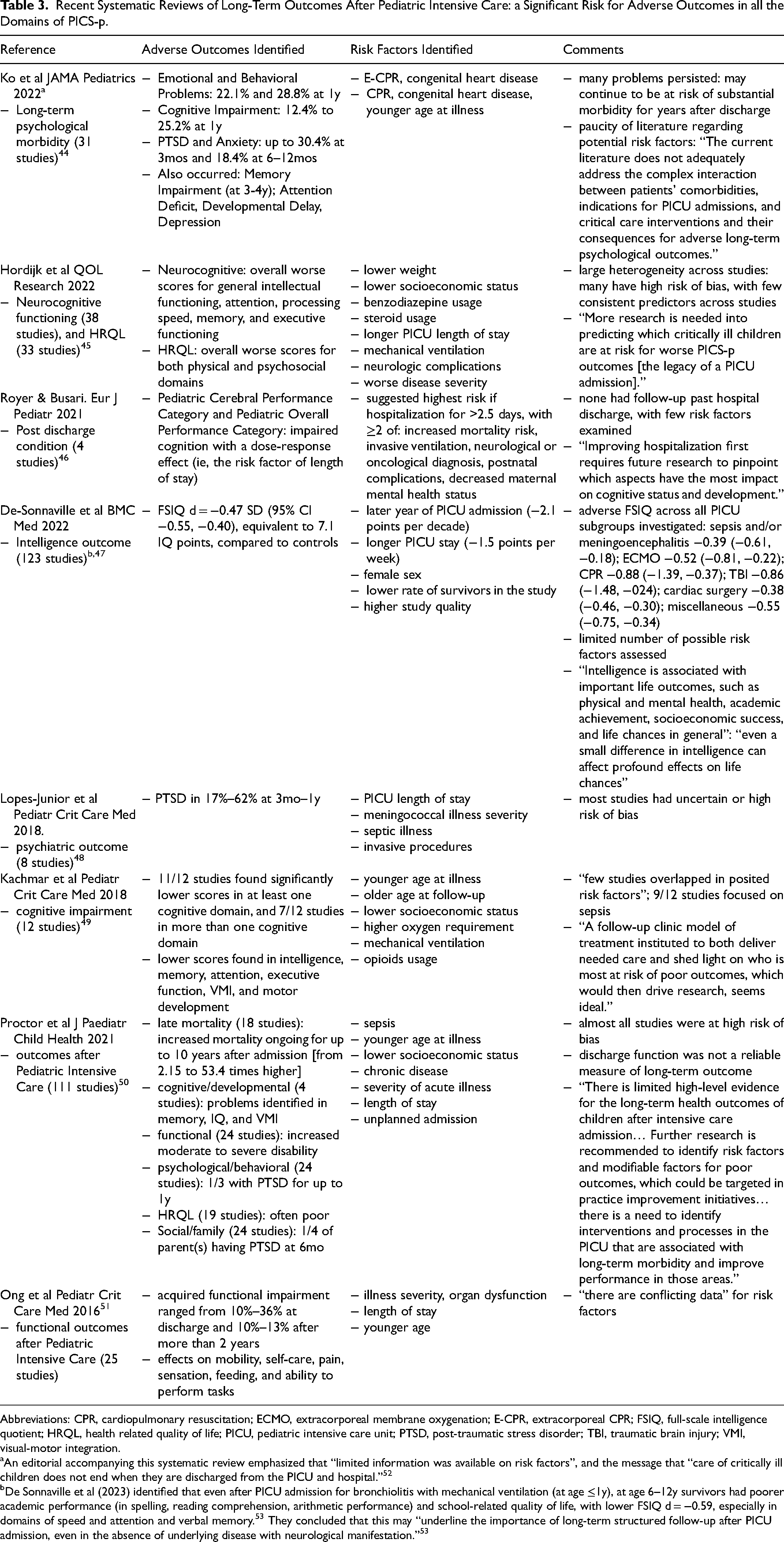
Abbreviations: CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation; E-CPR, extracorporeal CPR; FSIQ, full-scale intelligence quotient; HRQL, health related quality of life; PICU, pediatric intensive care unit; PTSD, post-traumatic stress disorder; TBI, traumatic brain injury; VMI, visual-motor integration.
An editorial accompanying this systematic review emphasized that “limited information was available on risk factors”, and the message that “care of critically ill children does not end when they are discharged from the PICU and hospital.” 52
De Sonnaville et al (2023) identified that even after PICU admission for bronchiolitis with mechanical ventilation (at age ≤1y), at age 6–12y survivors had poorer academic performance (in spelling, reading comprehension, arithmetic performance) and school-related quality of life, with lower FSIQ d = −0.59, especially in domains of speed and attention and verbal memory. 53 They concluded that this may “underline the importance of long-term structured follow-up after PICU admission, even in the absence of underlying disease with neurological manifestation.” 53
Research has explained, using biological and medical variables, many of which are non-modifiable, only up to one-third of the variance in developmental disorders and disabilities. This is the case after care for cardiac conditions in Pediatric Cardiac ICU (CICU) 54 and after care for non-cardiac conditions in PICU. 47 Moreover, the risk factors identified in different studies have been variable and often contradictory, again suggesting risk factors identified so far explain only a minority of the variance in outcomes.45,49,51 Despite improvements in survival, long-term survivor outcomes after care in CICU and PICU patients have little improved over decades.47,55,56 Two points are striking in the systematic reviews summarized in Table 3. First, PICS-p describes outcomes very similar to those that occur after childhood adversity, that is, emotional and behavior problems, cognitive impairment, executive functioning impairment, and neuropsychiatric problems.44–51 Second, PICS-p describes consistent risk factors very similar to those after childhood adversity, that is, younger age at illness, decreased maternal mental health status, and longer duration of adversity (PICU stay).44–51 A recent study of biomarkers for language outcomes in patients with single ventricle found the most common protein functions associated included those for neuronal proliferation and differentiation, axon guidance, and neurite growth. 57 In the Complex Pediatric Therapies Follow-up Program of children having had complex cardiac surgery in early infancy, 58 the number of, and/or longer hospitalizations in survivors were associate with adverse long-term outcomes, including behavioral concerns, 59 gross motor outcome, 60 and health related quality of life. 61 Moreover, maternal post-traumatic stress symptoms were an independent predictor of their toddler's cognitive and language outcomes, likely because parental mental health is a requirement for SSNRs. 62 Reviews of PICS-p recognized that sequelae can impact the child's lifetime trajectory,63–67 because injuries occurred during “periods of vulnerability during which injuries may alter development into adulthood” and the “new functional and cognitive impairments may affect a cascade of developmental milestones, school performance, and social interactions, placing a child at risk for a multitude of problems later in life.” 63 Moreover, even “small disruptions in any aspect of cognitive function during development can have a large impact.” 63
However, PICS-p reviews emphasized the need to focus on post-PICU care, and to identify potentially modifiable acute-care variables associated with outcomes, without explicitly considering the effects of threat, unpredictability, and deprivation (ie, toxic stress from adversity) during PICU hospitalization - and potential ways to address these (see below).63–66 The ‘bioecological theory of human development’ applied to PICS-p recognized that “the clinical condition of the child is not the only factor… it is essential to consider the broader context of their life like social surroundings, interactions with others, and available resources”; however, this review did not explicitly consider the causes of toxic stress during PICU. 68 A commentary about family centered care, which “aims to promote effective partnerships between children, their families, and practitioners” and is a concept that “governs all that we do in the PICU”, suggested we work toward “better family partnerships that enrich the experiences of critically ill children and their families during and after their PICU admission.” 69 While barriers to families “being present at their child's bedside” were mentioned, there was lack of focus on improving SSNRs, including serve-and-return interactions between parent/caregiver and young child while in the PICU. 69
This review has given the theory and evidence to show that early experiences on the vulnerable infant brain have lifelong implications, including a particular vulnerability to the interruption of normal developmental processes. 54 Given the similarities between PICS-p outcomes and risk factors to those after childhood adversity, the concept of pediatric medical traumatic stress during hospitalization in a PICU with similar categories of experienced adversities (ie, threat, unpredictability, and deprivation),4,7 and the missing explanatory variables for PICS-p outcomes, it becomes possible to suggest what we must and can do better in our care of patients. Recently, the term developmental care was used to describe “modifying the environment and caregiving to meet the developmentally appropriate expectations of the infant's brain.” 54 Although many of us knew this intuitively, we may not have known how extremely important this is for setting up the infant's entire future. We must have more focus on prioritizing this brain-directed care in the PICU.6,54,70
Parallels in the Neonatal Intensive Care Unit
A focus on family centered care, recognizing and emphasizing the critical role that parents play in actively caring for and hence promoting optimal development of their infant, is not new to the NICU.71–73 Engaging with and empowering parents includes interventions to support parents “to be emotionally, cognitively, and physically able to parent” 71 and spend extended periods with their baby 72 - eg, psychoeducational support and support of maternal mental health, participation in daily rounds, open visitation, overnight accommodations near their infant, peer-to-peer support, in-hospital parent spaces; and to enable parent-delivered interventions - eg, bathing, diapering, and clothing, modulating light, sound, and touch, provision of positive stimuli including skin-to-skin contact (especially Kangaroo care), holding, rocking, reading, talking, singing.71–73 This extends to family integrated care where parents “become their infant's caregiver… instead of passive observers of their infant's care,” 71 actively participating as integral members of the healthcare team. 72 Education of clinicians, and support of senior leadership, are recognized as critical to operationalizing these goals. 71
Almost all of the research suggesting improved outcomes is for relatively stable preterm and low birthweight neonates, although the model is being extended to and studied for term infants.71,72 The model is also being extended to and studied for neonates cared for in the cardiac ICU (CICU),54,70,74,75 recognizing that “sensory experience is the foundation for brain development in infancy” and the importance of “minimizing infant stress response to optimize brain development.” 74 Considerations of the safety of Kangaroo care and risk of accidental extubation are important, but the point remains of “supporting and encouraging parents to interact with their infants in safe ways.” 74 Overall, the goal is care “that minimizes the mismatch between infant neurobiological needs and the CICU environment” where “the infant is recognized as an individual who is communicating and interacting with the environment.” 75 Recognition that “to the developing brain, all experience matters, both positive and negative” 75 led to the concept of ‘infant medical trauma’ from the NICU experience that involves “intertwined and cumulative early experiences of stress, parental separation, and pain.” 73
Building Resilience with Trauma-Informed Care
There are important implications of the information reviewed above for what we can focus on and do better in the PICU. As discussed above, these may be conceptualized as providing developmental care, that is, “modifying the environment and caregiving to meet the developmentally appropriate expectations of the infant's brain”. 54 Putting together overlapping information from multiple sources on trauma-informed care (and family-centered care addressing infant medical trauma in the NICU) led to the suggestions in Table 4.2,4,6,70–78 These are general suggestions, and must be adapted to be age and developmentally appropriate for the individual patient. Serve-and-return interactions are particularly important for constructing the developing brain and achieving its genetic potential.76–79 We need to achieve a paradigm shift – a focus on SSNRs that buffer adversity and build resilience, to address the childhood origins of adult disease and wellness. 18 This focus must begin during the PICU hospitalization. Parental mental health should be a priority in order to empower them to develop and maintain SSNRs with their young child. 62 More specific advice on age and developmentally appropriate serve-and-return interactions, managing emotions, teaching rather than commanding, and building foundational capabilities (eg, social skills, emotional regulation, language, executive functions) is beyond the scope of this review.2,4,6,76–78
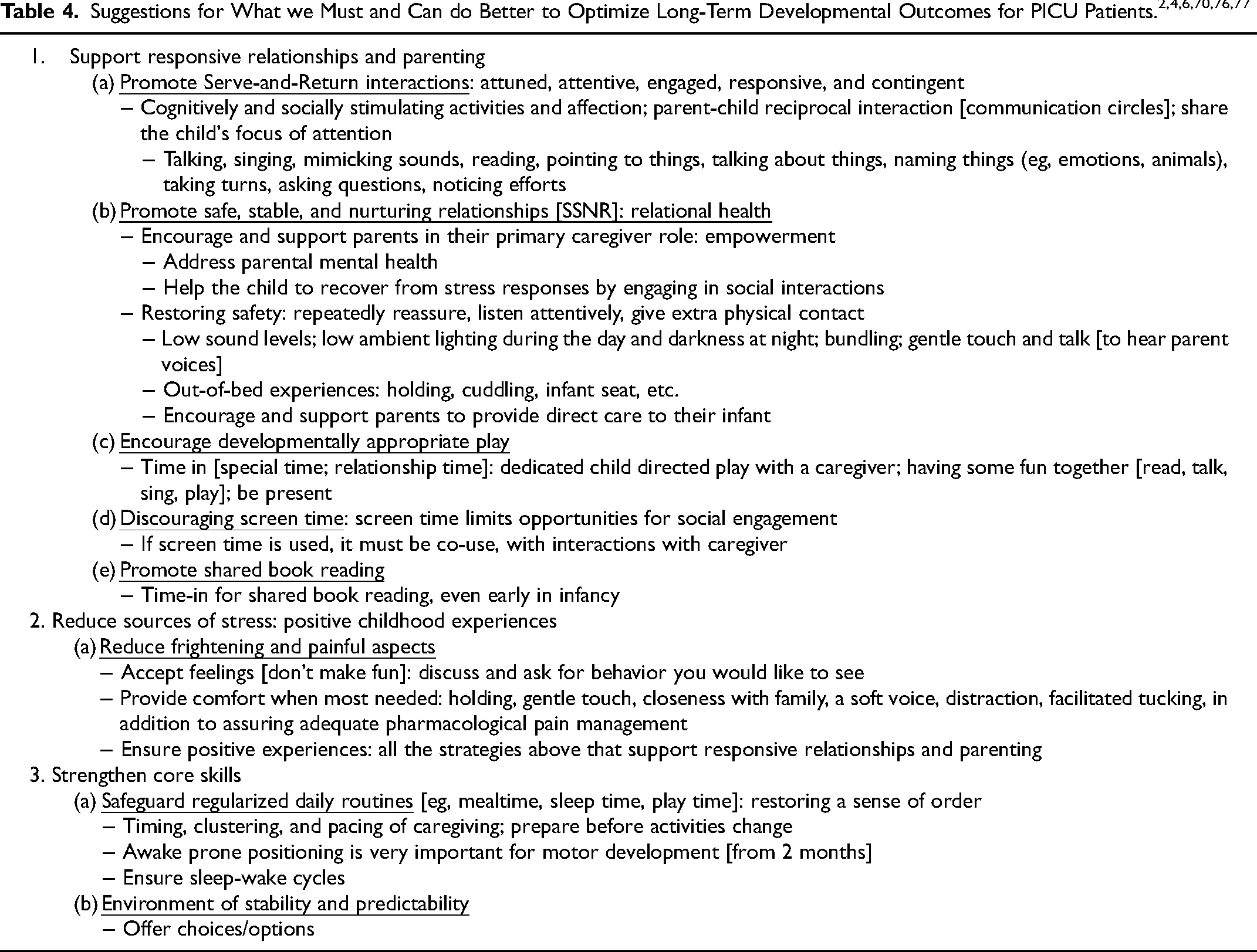
Anecdotal observation suggests that screen time is often used to entertain young children during busy clinical work in the hospital; however, this should be discouraged, and a renewed focus on the suggestions in Table 4 should be implemented. A systematic review including 64 observational studies of screen use in children under 6 years of age found adverse effects on cognitive (ie, language, executive function, and academic skills) and psychosocial (ie, prosocial behaviors, social-emotional competence, internalizing and externalizing behaviors) outcomes. 80 Specifically, adverse effects were associated with program viewing (eg, watching television, videos, movies, DVDs), background television (during child routines and interactions), age-inappropriate content (e.g, violence and action intended for a mature audience), and caregiver screen use during routines. 80 Positive cognitive outcomes were associated with screen co-use with others, that which promoted interactions, vocabulary development, and learning opportunities, with discussion of viewed content. 80
Developmental long-term follow-up in experienced multidisciplinary clinics (especially for the younger children) must be a priority.6,16,54,58,67,81,82 This outcomes determination performed by developmental teams familiar with the different subgroups of critically ill children should have several components. 58 First, to provide service, that is, early detection and intervention for children found to have adverse outcomes. Second, to provide quality improvement by iteratively providing feedback to the intensive care clinicians on outcomes and potentially modifiable predictors of those outcomes. Third, to conduct and publish research to facilitate knowledge translation for the critical care community. This entails prospective recording of pre-specified acute-care and demographic variables (especially those that may be potentially modifiable), and follow-up over time (eg, at 18-24 months, and 4-5 years of age) to determine neurodevelopmental, neurocognitive, motor, health related quality of life, and behavior outcomes.58,81 Only then will we learn how to serve our patients optimally, and what works best to prevent adverse long-term outcomes that affect the developing brain and biological systems for a lifetime.
Limitations
The main limitation of this review was its narrative content, without a systematic review having been done. However, many systematic reviews and meta-analyses were used in synthesis of the literature. Second, the focus was on young children. This was not to say that we cannot improve the care of older children. For example, a recent RCT in children age 7 (SD 2) years found that 25–30 min of story condition (listening to narratives from a storyteller) versus riddle condition (social interaction without narrative) increased salivary oxytocin, decreased salivary cortisol, resulted in less reports of pain, and resulted in children using more positive lexical markers (higher proportion of positive emotion words) when describing their time in hospital. 83 Third, studies on early active mobilization were not considered. This was because the efficacy of early active mobilization is unclear; a systematic review of adult RCTs found that at 6 months after intensive care, there was no statistically significant effect on days alive and out of hospital, in-person measured physical function, health related quality of life, mortality, or adverse events (although it was “possible it might increase mortality and adverse events” especially in mechanically ventilated patients). 84
Finally, whether and to what extent the developmental interventions may improve outcomes after hospitalization in the PICU has not been well studied. In the setting of severe bronchopulmonary dysplasia some studies suggested that there may be improved neurodevelopmental outcomes with a multidisciplinary team focused on developmental stimulation; however, outcomes were compared to historical controls, limiting conclusions made.85–88 The “first study to show associations between cardiac inpatient neurodevelopmental care practices and improvements in… cognitive outcomes in children with CHD at age 12 to 39 months” found “these low-cost, low-risk, generalizable program interventions using existing personnel and resources” had medium effect sizes (eg, developmental care rounds effect size 9.6 (95% CI 2.4, 16.8) for Bayley-4 cognitive score). 89 However, this study was limited by “only about 12% of the hospitalized cohort returning for neurodevelopmental follow-up”. 89 The suggestions here should be subjected to outcomes research to determine their efficacy.
Conclusion
This review has argued, with evidence, that we in pediatric critical care must take a public-health approach to address the key environmental conditions necessary for optimal early childhood development and hence facilitate children's ability to thrive. 90 Steps we can take to achieve this were suggested in Table 4. Future research must aim to determine what works best and what does not work. These early childhood investments to improve lifelong outcomes have great potential to help patients and reduce the massive growing burden of health care costs. 23
Footnotes
Author Contributions
Both authors made substantial contributions to conception or design of the work, and interpretation of data for the work; reviewed the work critically for important intellectual content; made final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. ARJ drafted the first version of the manuscript.
Ethics Approval
Approval was not required for the narrative review as we used only already publicly available published data for review.
Consent for Publication
Not applicable.
Data Availability
All data used are given in the publication, and the original reference(s) for that data provided.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.