
Abstract
Introduction
The aim of this study was to evaluate genetic risk factors in term-born children with antenatal periventricular hemorrhagic infarction (PVHI), presumed antenatal periventricular venous infarction and periventricular hemorrhagic infarction in preterm neonates.
Methods
Genetic analysis and magnetic resonance imaging were performed in 85 children: term-born children (≥36 gestational weeks) with antenatal periventricular hemorrhagic infarction (n = 6) or presumed antenatal (n = 40) periventricular venous infarction and preterm children (<36 gestational weeks) with periventricular hemorrhagic infarction (n = 39). Genetic testing was performed using exome or large gene panel (n = 6700 genes) sequencing.
Results
Pathogenic variants associated with stroke were found in 11 of 85 (12.9%) children with periventricular hemorrhagic infarction/periventricular venous infarction. Among the pathogenic variants, COL4A1/A2 and COL5A1 variants were found in 7 of 11 (63%) children. Additionally, 2 children had pathogenic variants associated with coagulopathy, whereas 2 other children had other variants associated with stroke. Children with collagenopathies had significantly more often bilateral multifocal stroke with severe white matter loss and diffuse hyperintensities in the white matter, moderate to severe hydrocephalus, moderate to severe decrease in size of the ipsilesional basal ganglia and thalamus compared to children with periventricular hemorrhagic infarction/periventricular venous infarction without genetic changes in the studied genes (P ≤ .01). Severe motor deficit and epilepsy developed more often in children with collagenopathies compared to children without genetic variants (P = .0013, odds ratio [OR] = 233, 95% confidence interval [CI]: 2.8-531; and P = .025, OR = 7.3, 95% CI: 1.3-41, respectively).
Conclusions
Children with periventricular hemorrhagic infarction/periventricular venous infarction have high prevalence of pathogenic variants in collagene genes (COL4A1/A2 and COL5A1). Genetic testing should be considered for all children with periventricular hemorrhagic infarction/periventricular venous infarction; COL4A1/A2 and COL5A1/A2 genes should be investigated first.
Periventricular hemorrhagic infarction (PVHI) is a well-described pathology among extremely premature infants.1–3 The mechanism behind periventricular hemorrhagic infarction in prematurely born infants is germinal matrix and intraventricular hemorrhage leading to periventricular venous obstruction and congestion and ending in periventricular infarction.3–7 On cerebral ultrasonography, periventricular hemorrhagic infarction is usually visible as porencephalic cavitation of various severity within the periventricular white matter. 3 On magnetic resonance imaging (MRI), periventricular hemorrhagic infarction is evaluated as prevalently unilateral medullary venous territory infarction in the periventricular area during the acute stage and as a porencephalic enlargement of the lateral ventricle of various severity, and/or periventricular gliosis and/or cystic changes with a spared cortex during the chronic stage.8–12 Germinal matrix hemorrhage is especially common in premature infants born below 32 gestational weeks because of the suggested fragile state of the vessel wall in the germinal matrix.3,8,13,14
Antenatal periventricular hemorrhagic infarction may be detected by fetal ultrasonography incidentally15,16 and probably reflect the same pathologic mechanism as is seen in preterm-born children.10,17–19 If the child manages to be born at term, there may be no neurologic symptoms after birth, as the stroke is already in the chronic phase. 16
Some children with undetected antenatal stroke survive and stabilize. After an unremarkable term birth and neonatal period, chronic signs of stroke are found on MRI later during infancy if spastic hemiparesis, delayed milestone, or seizures develop.8–10,12,14,17,20–23 Stroke in these children is presumed to have occurred in the antenatal period and MRI suggests periventricular venous infarction (PVI) as the causative pathology in two-thirds of those cases, although the hemorrhage is not always found on MRI.9,24
The injury visualized on MRI during childhood both in term-born children with presumed antenatal periventricular venous infarction and in preterm-born children with periventricular hemorrhagic infarction is similar. 10 MRI findings suggest that presumed antenatal periventricular venous infarction occurs at a certain stage of vascular development of the brain at gestational weeks 24-34 with germinal matrix hemorrhage as the source.3,8,11,13 Vascular disruption and development of periventricular hemorrhagic infarction before gestational week 24 can lead to schizencephaly, and after gestational week 24 can lead to porencephaly19,25–29 the severity of which depends on the size of initial stroke. Clinically, periventricular hemorrhagic infarction/periventricular venous infarction leads to congenital hemi- or tetraparesis of various severity, epilepsy, and cognitive disability.22,29–34 The outcome depends on the initial size of the periventricular hemorrhagic infarction/periventricular venous infarction.3,34–37
Research of the risk factors for presumed antenatal periventricular venous infarction has been inadequate and evaluation of the causes of germinal matrix hemorrhage in fetuses is still insufficient.8,9,14,17,20 Recent research shows that prenatal infection and chorioamnionitis may play a critical role in some term-born children with presumed antenatal periventricular venous infarction.11,38 Previously suspected thrombophilia risk is not increased in children with neonatal or presumed arterial ischemic stroke, or with presumed antenatal periventricular venous infarction. 39 A recent meta-analysis of antenatal periventricular hemorrhagic infarction studies showed typical pregnancy without co-occurring conditions in 39% of cases. 40
In children with antenatal intracerebral hemorrhage, genetic profiling has suggested presence of impaired hemostatic, prothrombotic, collagen, and X-linked GATA1 genes. 41 High prevalence of COL4A1 and COL4A2 pathogenic sequences has been found in cases of fetal multifocal hemorrhagic and/or ischemic cerebral lesions,28,42 in fetuses with schizencephaly,27,28 and in children with heterotopias and polymicrogyria, 43 as well as in cases of idiopathic perinatal intracranial hemorrhage, 44 schizencephaly, and porencephaly.29,31–33,42,45–47 A single variant in COL4A1 has been suggested as the cause of both arterial perinatal stroke and periventricular venous infarction. 23 Although periventricular hemorrhagic infarction/periventricular venous infarction in preterm- and term-born children leads to porencephalic enlargement of the lateral ventricles of various severity and/or periventricular white matter damage on MRI, there are no studies of genetic profiling to evaluate collagenopathies among preterm- or term-born children with periventricular hemorrhagic infarction/periventricular venous infarction. Also it has been suggested that in preterm-born children with periventricular hemorrhagic infarction, genetic predisposition might be the leading factor for development of periventricular hemorrhagic infarction.48,49
The aim of this study was to evaluate the variants causing genetic collagenopathies and coagulopathies in term-born children with antenatal periventricular hemorrhagic infarction and presumed antenatal periventricular venous infarction, as well as in preterm-born children with periventricular hemorrhagic infarction.
We hypothesize that children with periventricular hemorrhagic infarction/periventricular venous infarction show high prevalence of collagenopathies, such as has been found earlier in fetuses and in children with porencephaly.
Methods
Patient Selection
The data of term or near term-born children (≥36 gestational weeks) with antenatal periventricular hemorrhagic infarction (n = 6) diagnosed during the fetal period, or with presumed antenatal periventricular venous infarction (n = 43) diagnosed during infancy were drawn from the Estonian Pediatric Stroke Database for 1994-2019. The Estonian Pediatric Stroke Database has been created retrospectively since 1994 and prospectively with continuously added cases since 2003.9,11,21,22 The vascular classification of patients in the Estonian Pediatric Stroke Database is based on MRI according to Kirton and coauthors.9,12,14 Chronic changes after periventricular hemorrhagic infarction/periventricular venous infarction are described on MRI, based on this classification, 12 as a medullary venous territory infarction in the periventricular area, with a porencephalic enlargement of the lateral ventricle, and/or periventricular gliosis and/or cystic changes, spared cortex, and presence of hemosiderin in the area of the germinal matrix and in the ventricles and/or in periventricular lesion.8–12 The radiologic images for the present study were reviewed by radiology resident and 2 neuroradiologists to confirm the vascular genesis of periventricular venous infarction. Evaluation of the MRI findings, including the size of the basal ganglia and thalamus (normal/mild or moderate/ severe decrease in the size) and enlargement of the lateral ventricles (normal/mild or moderate/severe enlargement) was performed.
Preterm-born patients (<36 gestational weeks) with periventricular hemorrhagic infarction (n = 74) in the Estonian Pediatric Stroke Database were identified from the clinical database of a third-level regional university hospital, accounting for about one-third of the neonatal cases in the country. The medical records of neonatal intensive care unit of the hospital were searched for children with the diagnosis of severe grade of intraventricular hemorrhage (grade III or IV) or periventricular hemorrhagic infarction/periventricular venous infarction1,3,50 treated at the hospital between 2002 and 2019. Also the hospital's electronic database between 2002-2019 was searched for International Classification of Diseases, Tenth Revision, diagnosis codes P 52.2., P 52.3, P 52.4, P 52.6, and P 52.9. 51 In the final study group (n = 39), consisting of preterm-born children with periventricular hemorrhagic infarction, the diagnosis of periventricular hemorrhagic infarction was confirmed by autopsy or MRI, except for 1 preterm-born child with periventricular hemorrhagic infarction (clearly visible on ultrasonography), whose parents declined MRI, but agreed with genetic testing.
Children were excluded from the study if there occurred at least 1 of the following: (1) acute arterial ischemic stroke, (2) sinovenous thrombosis, (3) hemorrhage in the brain parenchyma without association with germinal matrix hemorrhage or intraventricular hemorrhage, or (4) other documented diseases or congenital malformations involving the central nervous system.
The flowchart of the inclusion criteria for the final study group of periventricular hemorrhagic infarction/periventricular venous infarction children (n = 85) is shown in Figure 1. All participants were Caucasian.
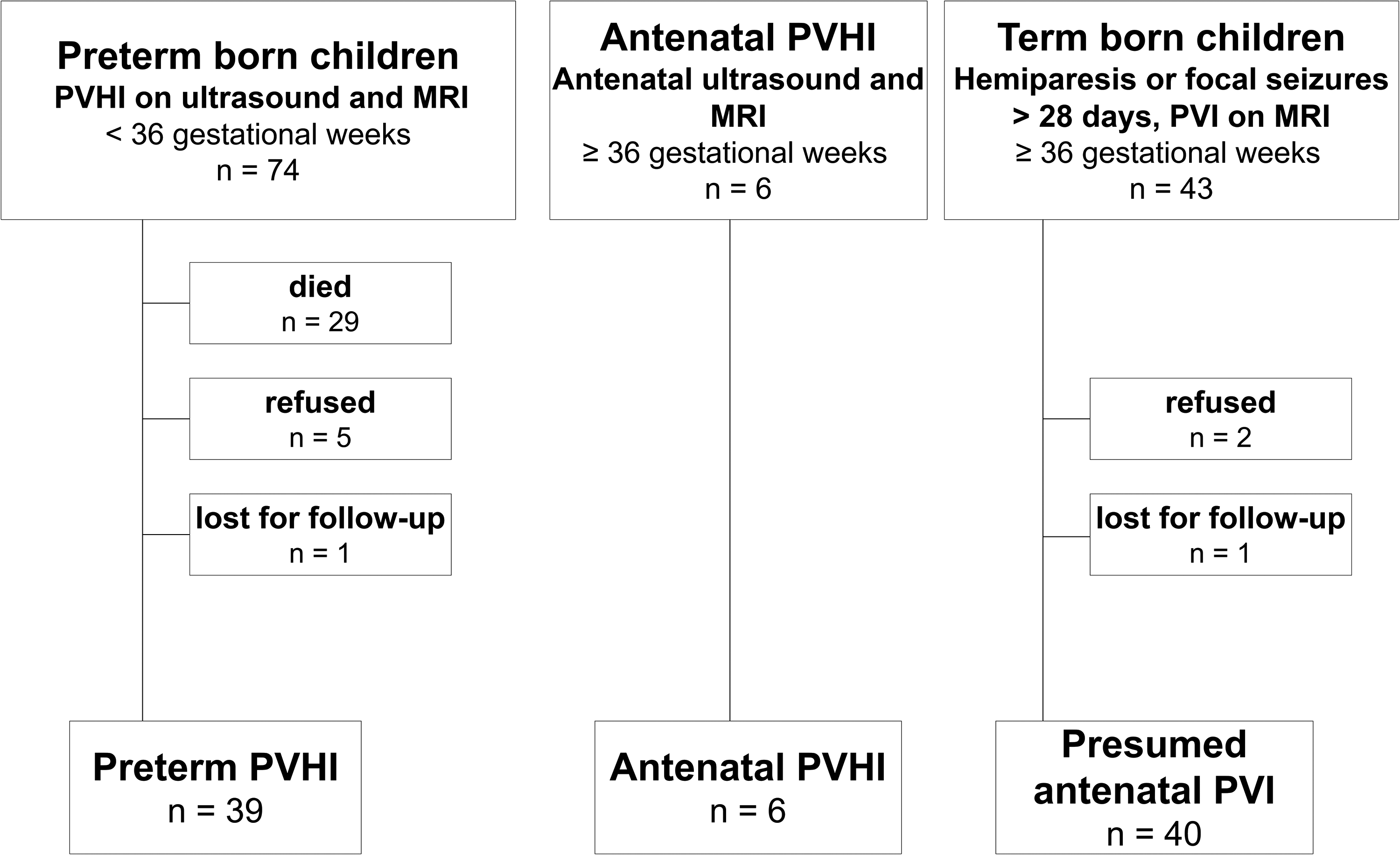
The flowchart of the inclusion criteria for periventricular venous infarction children for genetic testing.
Methods
The clinical data of pregnancy and delivery were extracted from medical records. For term-born children with antenatal periventricular hemorrhagic infarction or presumed antenatal periventricular venous infarction from 1994 to 2019 and for preterm children with PHVI since 2002, genetic testing was suggested as part of a larger follow-up study of perinatal stroke patients. The neurologic motor deficit was evaluated and defined according to the Surveillance of Cerebral Palsy in Europe criteria 52 : children with persisting increased tone and pathologic reflexes, resulting in an abnormal pattern of movement and posture, were considered to have unilateral or bilateral spastic cerebral palsy. Severity of the motor deficit was evaluated according to the Pediatric Stroke Outcome Measure (PSOM) 53 by the child neurologist (R.L.): mild, no impact on function; moderate, some functional limitations; severe, missing function.
Epilepsy was diagnosed by the treating pediatric neurologist according to the following definition: at least 2 unprovoked seizures occurring >24 hours apart or 1 unprovoked seizure with high recurrence risk, or diagnosis of the epilepsy syndrome. 36
Genetic Testing
Molecular screening was carried out on DNA extracted from the leukocytes of blood samples, with next-generation sequencing methods. In 60 individuals, whole exome sequencing was performed with Agilent SureSelectXT Human All Exon V7 library capture followed by sequencing on the NovaSeq 6000 platform (Illumina Inc.). The TruSight One Expanded panel covering the 6700 Mendelian disease-associated genes was sequenced on the Illumina NextSeq platform in a clinical setting in 23 individuals. In addition, 2 patients had received genetic diagnoses through single gene clinical testing before next-generation sequencing became available. Raw sequencing reads were aligned to the hg19 reference genome using the BWA MEM 54 algorithm. Variants were first called for individual samples using GATK HaplotypeCaller, 55 before multisample joint aggregation and reannotation using GATK GenotypeGVCFs. Read alignment and variant calling was carried out in the High Performance Computing Center of the University of Tartu “UT Rocket.” 56 The variant call set was annotated using hail 0.1 (Hail Team. Hail 0.1. https://github.com/hail-is/hail) and then uploaded to the Seqr platform (https://github.com/broadinstitute/seqr) for collaborative variant analysis. Variant filtration focused on rare variants in coding regions and on splice-sites predicted to affect protein function following the known inheritance pattern in 2 gene lists: (1) genes associated with stroke or associated with stroke through vascular stability, (2) genes associated with coagulopathies (Supplementary Tables 1 and 2). Familial segregation of the variants was assessed using Sanger sequencing. Also, if the variants did not meet the in-house criteria for quality control, the variants were Sanger sequenced for validation. Shortly, the variants were sent for Sanger validation if the sequencing depth was below 20, the variant allele was present in less than 30% of the reads, or the variant quality was flagged by the GATK VQSR algorithm.
The variants were classified according to the criteria published by the American College of Medical Genetics (ACMG). 57 The variants published in the known databases ClinVar and HGMDPro as disease-causing were considered pathogenic. The novel variants detected first by our study group were classified as pathogenic or likely pathogenic, if the variant fulfilled the following criteria: (1) a missense variant that replaces glycine by another amino acid in the triple helix domain, for COL4A1/2 and COL1A1 genes, (2) or a loss of function (changes at the canonical splice site, nonsense variants and frameshift variants) in genes for which other loss-of-function variants have been reported as pathogenic. For example, for COL4A1, COL4A2, and COL5A1, loss-of-function variants have been reported as pathogenic in the ClinVar and HGMD pro databases. If these characteristics were not met, sequence changes were classified as variants of unknown significance (VUS), as suggested by the ACMG criteria. No pathogenic variants were detected in the 7S or NC1 domain in COL4A1/2 or in the N-terminal or C-terminal region of COL5A1 gene. All variants detected in our study group and their allele frequencies were checked with the normal population's database: the Genome Aggregation Database (gnomAD v3.1 spans 76,156 genomes), which aggregates exome and genome data from large sequencing projects. 58 Also, the Estonian Biobank has sent the sequencing data of approximately 5000 exomes and genomes to gnomAD; these are presented in a separate category in gnomAD and can therefore be treated as a healthy control group.
The whole genetic testing was performed at the Medical Laboratory of Tartu University Hospital, which is accredited under ISO 15189:2012.
The studies were approved by the Ethics Review Committee on Human Research of the University of Tartu by protocol no 294/M-18. Written informed consent was provided by all individual participants older than 7 years and by their parents in all cases.
Statistical Analysis
Prior to further analysis, normality of the data was evaluated using the Shapiro-Wilk test. Continuous data were summarized as medians with the interquartile range (IQR) and range (minimum, maximum), and categorical data, as absolute counts and percentages. Differences between the 2 groups were analyzed by the nonparametric Mann-Whitney U test for continuous variables. Logistic regression, the χ2 test, or Fisher exact test was used to assess the relationship between the groups, as appropriate. Multinomial logistic regression was used to assess the relationship between the groups (preterm periventricular hemorrhagic infarction, antenatal periventricular hemorrhagic infarction, presumed antenatal periventricular venous infarction). The odds ratio (OR) with the 95% confidence interval (CI) was estimated as the measure of association. Multiple testing was corrected using the false discovery rate linear step-up procedure. 59 The Benjamini-Hochberg critical values were calculated as (i/m)Q, where i is the rank in an ascending list of P values, m is the total number of tests, and Q is a false discovery rate of 0.05. The threshold for significance of a single comparison for a set of pregnancy and delivery risk factors for study groups was 0.008, for children with pathogenic or likely pathogenic variants in the collagen genes compared to children with periventricular hemorrhagic infarction/periventricular venous infarction without genetic variants associated with stroke was 0.0028 and for a set of MRI findings was 0.035. All shown raw P values were 2-tailed. Statistical evaluation was performed using the statistical package SAS, version 9.4 (SAS Institute, Cary, NC), and the R Statistical Software (version 4.0.2, R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical Characteristics of the Study Group
The representative demographic data of the final study group of 85 periventricular hemorrhagic infarction/periventricular venous infarction patients are shown in Table 1. The study group included 39 preterm-born children with periventricular hemorrhagic infarction, 6 children with antenatal periventricular hemorrhagic infarction, and 40 children with presumed antenatal periventricular venous infarction. The study groups were well comparable in terms of maternal age, previous pregnancy loss, number of pregnancies, deliveries and mode of conception, gender of patients, number of patients small for gestational age, and number of patients with severe motor deficit or epilepsy (Table 1). Compared to the preterm periventricular hemorrhagic infarction group, the presumed antenatal periventricular venous infarction group showed significantly lower incidence of emergency caesarean section and 5-minute Apgar score <7 (Table 1).
Demographics and Distribution of Pathogenic/Likely Pathogenic Variants and Variants of Unknown Significance Associated With Stroke in Different PVHI/PVI Subgroups.
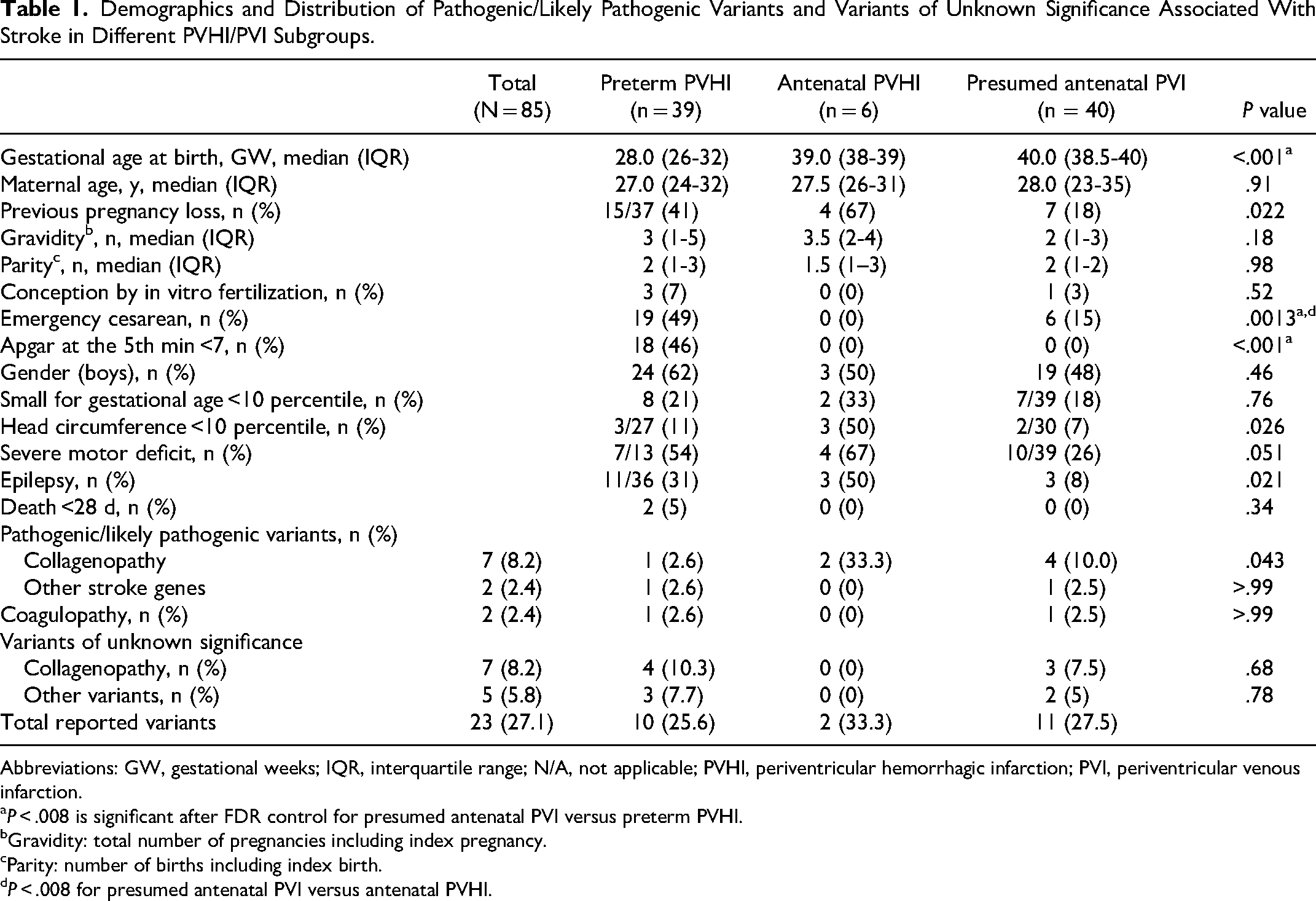
Abbreviations: GW, gestational weeks; IQR, interquartile range; N/A, not applicable; PVHI, periventricular hemorrhagic infarction; PVI, periventricular venous infarction.
P < .008 is significant after FDR control for presumed antenatal PVI versus preterm PVHI.
Gravidity: total number of pregnancies including index pregnancy.
Parity: number of births including index birth.
P < .008 for presumed antenatal PVI versus antenatal PVHI.
Altogether, we identified 11 of 85 patients (12.9%) with periventricular hemorrhagic infarction/periventricular venous infarction carrying pathogenic and likely pathogenic variants in genes associated with collagenopathy and coagulopathy, or in other genes associated with stroke. All pathogenic or likely pathogenic variants are listed in Table 2. Among the pathogenic variants, COL4A1/A2 and COL5A1 variants were found in 7 of 11 (63%) children. Pathogenic collagen variants were detected in COL4A1 gene (2 patients with antenatal periventricular hemorrhagic infarction and 3 with presumed antenatal periventricular venous infarction), in COL4A2 gene (1 patient with presumed antenatal periventricular venous infarction), and in COL5A1 gene (1 preterm-born patient with periventricular hemorrhagic infarction) (Table 1).
Description of the Stroke Patients With Pathogenic or Likely Pathogenic Gene Variants, Their MRI Findings, and Clinical Outcome.
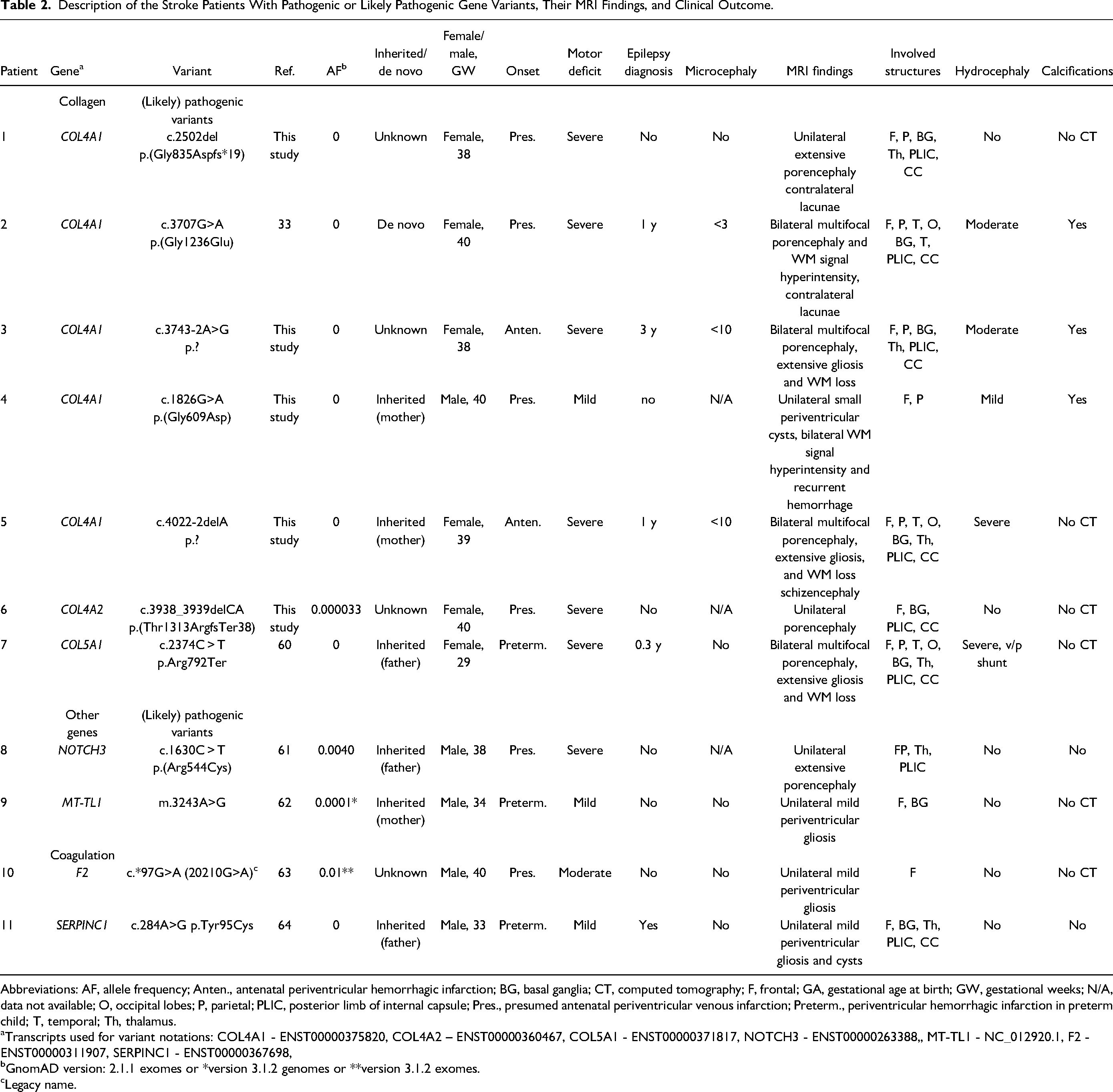
Abbreviations: AF, allele frequency; Anten., antenatal periventricular hemorrhagic infarction; BG, basal ganglia; CT, computed tomography; F, frontal; GA, gestational age at birth; GW, gestational weeks; N/A, data not available; O, occipital lobes; P, parietal; PLIC, posterior limb of internal capsule; Pres., presumed antenatal periventricular venous infarction; Preterm., periventricular hemorrhagic infarction in preterm child; T, temporal; Th, thalamus.
Transcripts used for variant notations: COL4A1 - ENST00000375820, COL4A2 – ENST00000360467, COL5A1 - ENST00000371817, NOTCH3 - ENST00000263388,, MT-TL1 - NC_012920.1, F2 - ENST00000311907, SERPINC1 - ENST00000367698,
GnomAD version: 2.1.1 exomes or *version 3.1.2 genomes or **version 3.1.2 exomes.
Legacy name.
Although the most severe cases were diagnosed already clinically, 5 of 11 cases with pathogenic or likely pathogenic variants had not been tested earlier, among them 3 cases with collagenopathy. These had been considered as too mild cases, and genetic disease had not been suspected earlier. All sequence changes detected in this group were unique; however, it was found that COL4A1 gene variants were most prevalent (5 patients). Of the 11 detected variants, 6 were described for the first time in this study.
Only 2 of 85 children (2.4%) had variants connected with coagulopathy: 1 child with presumed antenatal periventricular venous infarction had the common prothrombin 20210G>A (rs1799963) risk variant and 1 preterm-born patient with periventricular hemorrhagic infarction and antithrombin 3 deficiency had SERPINC1 variant inherited from the father who was also affected with thrombophilia (Table 2).
There were 2 of 85 (2.4%) pathogenic findings in other genes that have earlier been associated with stroke: NOTCH3 variant inherited from father to son with presumed antenatal periventricular hemorrhagic infarction and MT-TL1 variant in one preterm-born patient with periventricular hemorrhagic infarction (Table 2).
In addition, variants of unknown significance in collagen (COL4A2, COL5A1, COL1A1) and in other genes (ATP1A, PHACTR1, FV, ITGA2B) were detected in 12 of 85 patients (14.1%) with periventricular venous infarction. All variants of unknown significance are listed in Supplementary Table 3.
There were 7 patients with variants of unknown significance in collagen genes: 2 patients with periventricular hemorrhagic infarction among preterm-born children and 1 with presumed antenatal periventricular venous infarction had a change in COL5A1 gene; 1 patient with presumed antenatal PHVI had COL4A2 mutation, and 2 neonatal patients and 1 patient with presumed antenatal periventricular venous infarction had COL1A1 variant. There were only 2 patients with variants of unknown significance in coagulopathy-associated genes: and 3 of 85 patients (3.5%) had variants of unknown significance that may be associated with stroke (Supplementary Table 3).
Risk Factors in the Group of Collagenopathies and in the Group of Children Without Detected Gene Variants (Figure 2)
Children with collagenopathies (COL4A1/A2 and COL5A1) (n = 7) and children without any genetic changes (n = 62) were well comparable in terms of maternal age, number of pregnancies, deliveries, mode of conception, and other risk factors during pregnancy and delivery (Figure 2). The groups were also similar regarding the mode of delivery, Apgar scores, and need for resuscitation at birth. No children with collagenopathy needed intubation or long-term ventilation after birth. Only 1 of 7 children with collagenopathies had seizures during the neonatal period, which was not different from the group of children without listed gene variants. There were no differences in the number of children who were small for gestational age (<10 percentiles) 65 between the groups. Head circumference at birth was <10 percentiles in 3 of 5 (60%) children with collagenopathy compared to 5 of 46 (11%) children without detected gene variants (P = .023); however, this finding was not significant after false discovery rate correction (adjusted false discovery rate significance threshold level was 0.0028) (Figure 2).
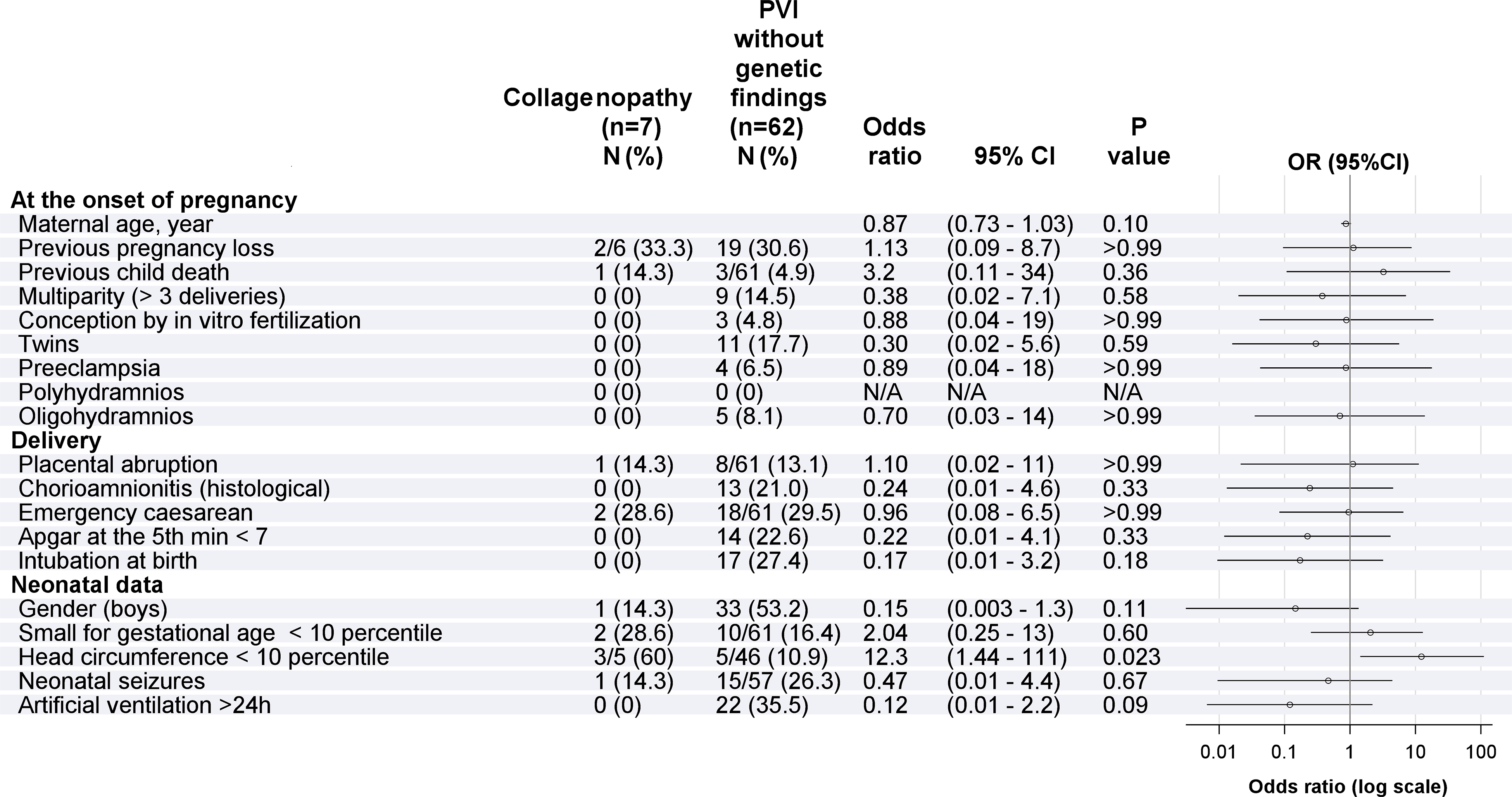
Maternal-, pregnancy-, and delivery-related risk factors in children with pathogenic/likely pathogenic variants in the collagen genes compared to children with periventricular hemorrhagic infarction/periventricular venous infarction without genetic variants associated with stroke. The adjusted false discovery rate significance threshold level was 0.0028, but no risk factors was revealed as significant (raw P values < .0028).
MRI Characteristics of Children With Genetic Changes in Collagen Genes (Figure 3)
Children with collagenopathies had significantly more often bilateral multifocal stroke (P = .0029), bilateral severe white matter loss (P = .01), bilateral hyperintensities in the white matter (P = .008), moderate to severe enlargement of the lateral ventricles (P = .01), extensive bilateral periventricular gliosis (P = .016), lacunae in the contralesional hemisphere (in the putamen) (P = .0098), moderate to severe decrease in the size of the ipsilesional caudate nucleus (P = .018), putamen (P = .0015), and thalamus (P = .017) compared to children with periventricular venous infarction without genetic changes in the studied genes (Figure 3). Presence of hemosiderin in the ventricles or in the periventricular areas, schizencephaly, and thin corpus callosum were not different between the groups (Figure 3). Computed tomography images were available for 3 of the 7 children with collagenopathies and all of them had small bilateral parenchymal calcifications (Table 2). Individual MRI findings for children with collagenopathies are presented in Figure 4.
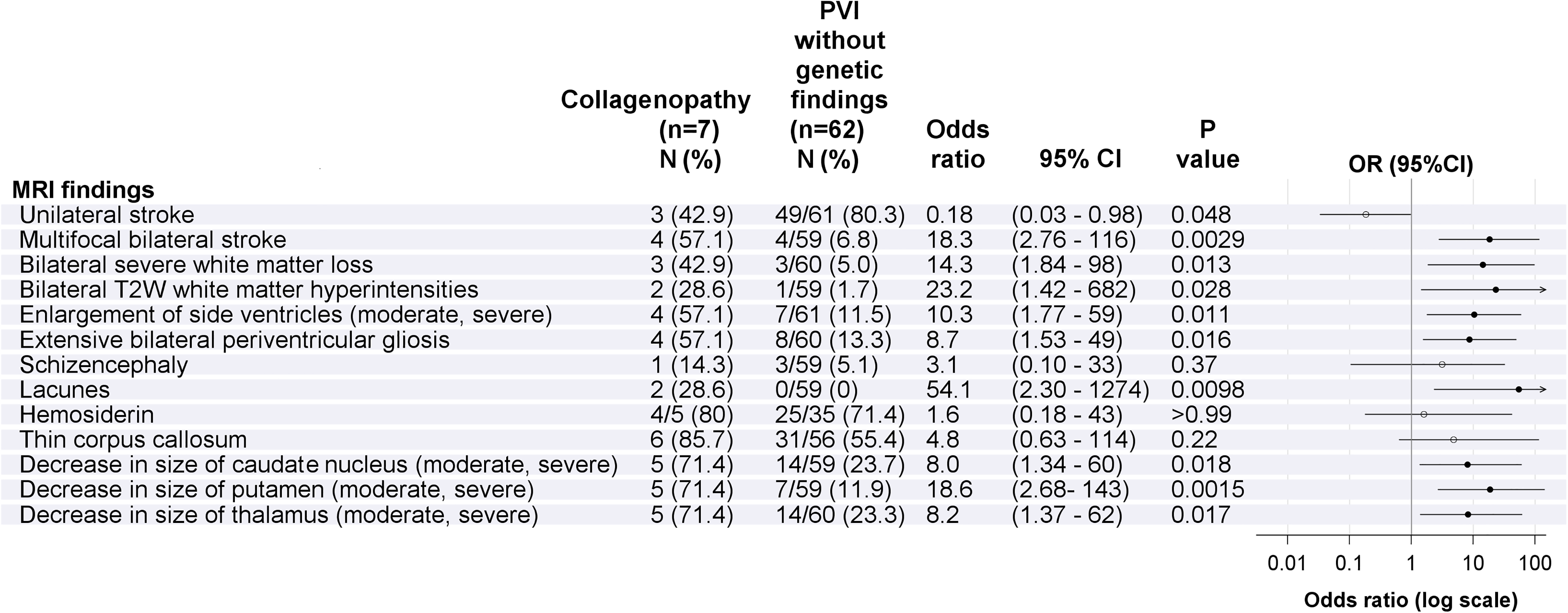
MRI findings for children with collagenopathies compared to children with periventricular hemorrhagic infarction/periventricular venous infarction without genetic changes. Only raw P values that were below the adjusted false discovery rate significance threshold .035 are marked as significant (black dot in the figure).
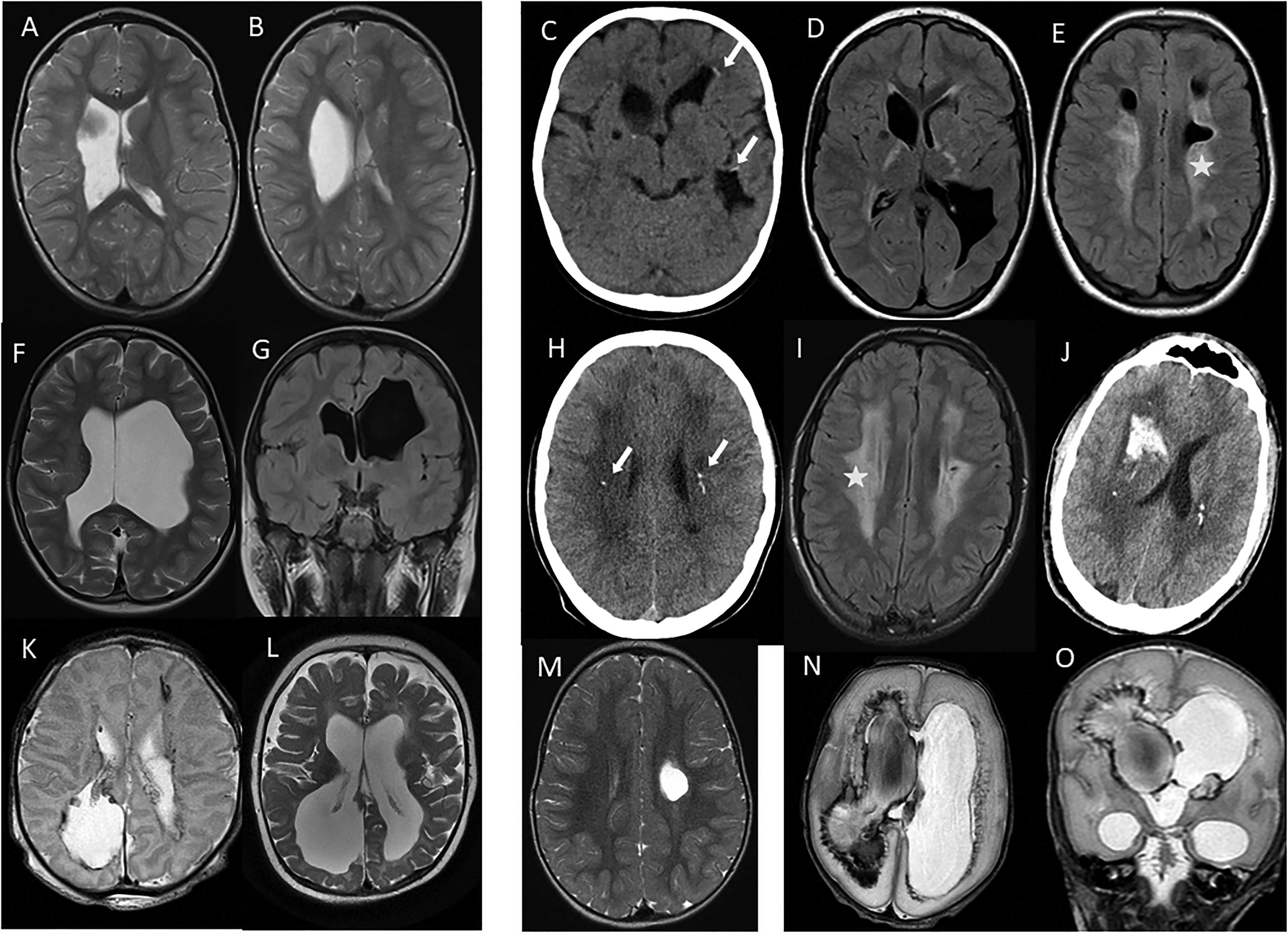
Individual MRI findings for children with collagenopathies. Patient 1: (A, B) axial T2-weighted MRI images of a girl with presumed antenatal periventricular venous infarction with unilateral focal porencephalic enlargement of the left ventricle at age 3 years. Patient 2: (C) axial computed tomography image with calcifications (arrows) of a girl with presumed antenatal periventricular venous infarction at age 13 months; and (D-E) axial MRI fluid-attenuated inversion recovery images with multiple bilateral porencephalic enlargement of the lateral ventricles and bilateral signal increase of the white matter (star) at age 12 years. Patient 3: (F) axial T2-weighted image of a girl with antenatal periventricular hemorrhagic infarction with severe porencephalic enlargement of the lateral ventricles and loss of white matter at age 7 years; and (G) coronal fluid-attenuated inversion recovery image with thin corpus callosum at age 19 years. Patient 4: (H) axial computed tomography image of a boy with presumed antenatal periventricular venous infarction with calcifications (arrows) at age 12 years; (I) axial fluid-attenuated inversion recovery image with bilateral signal increase of the white matter and small periventricular cysts on the left at age 14 years; and (J) at age 22 years, computed tomography image shows large intraparenchymal hemorrhages. Patient 5: (K) axial T2-weighted MRI image of a girl with antenatal periventricular hemorrhagic infarction with bilateral porencephalic enlargements of the ventricles and hemosiderin in side ventricles and parenchyma on the first day of life; and (L) axial T2-weighted MRI image at age 10 months with enlarged lateral ventricles and loss of white matter. Patient 6: (M) axial T2-weighted image of a girl with presumed antenatal periventricular venous infarction with unilateral focal porencephalic enlargement of the left lateral ventricle at age 2 years. Patient 7: (N) axial and (O) coronal T2-weighted images of a preterm-born girl at gestational week 29 with extensive bilateral intraventricular hemorrhage and right-side periventricular hemorrhagic infarction with ventriculomegaly at age 14 days.
Outcome Characteristics of Children With Possibly Stroke-Causing Genetic Variants
No deaths occurred among children with collagenopathies or other pathogenic variants during the study period (Table 3). Moderate-severe motor deficit developed more often in children with pathogenic variants in collagen genes (85.7%) compared to children without genetic variants (20.7%), respectively (P = .0013, OR = 233, 95% CI: 2.8-531). Epilepsy developed more often in children with pathogenic variants in collagen genes compared to children without genetic variants (57.1% vs 15.5%, respectively, P = .025; OR = 7.3, 95% CI: 1.3-41). One child (patient 4) had only mild motor deficit and normal cognitive function initially; although he had extensive bilateral white matter signal intensity and small periventricular cystic lesions on the left hemisphere, but he developed macrohemorrhage at age 22 years with poor outcome (Table 2). No other patient had recurrent hemorrhage so far.
Outcome in Children With Periventricular Hemorrhagic Infarction / periventricular Venous Infarction With Pathogenic Variants and In Children Without Pathogenic Variants or Variants of Unknown Significance.
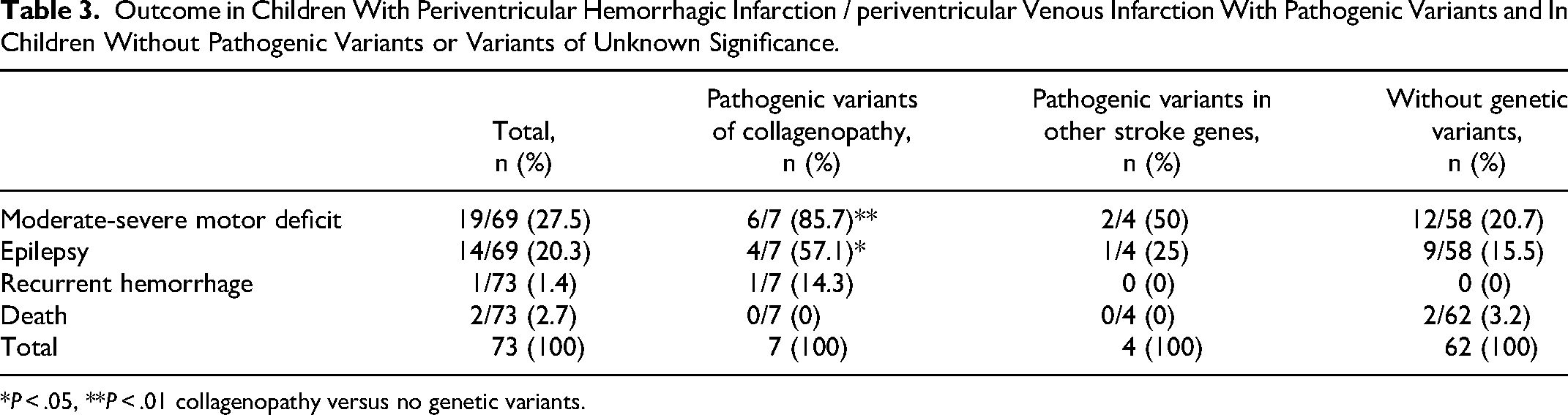
*P < .05, **P < .01 collagenopathy versus no genetic variants.
Discussion
Main Finding of the Study
We found high prevalence of collagenopathies, specifically pathogenic/likely pathogenic variants in COL4A1/2 and COL5A1 genes, leading to microangiopathy in both term-born children with antenatal and presumed antenatal periventricular hemorrhagic infarction/periventricular venous infarction and in preterm-born children with periventricular hemorrhagic infarction. Five of the 7 pathogenic/likely pathogenic variants of collagen genes found in this study were previously not associated with a genetic condition. To our knowledge, this is the first study evaluating the genetic profile, including collagen genes, of children with presumed antenatal periventricular venous infarction, where earlier clinical research has not found clear etiologic causes other than maternal bacterial infection or preeclampsia in some patients.9,11,14,20,38
Emergence of Collagenopathies
Defects of COL4A1/A2 gene have emerged as the cause of antenatal and neonatal hemorrhage, schizencephaly, and porencephaly.23,27,28,31,33,41,42,44–47,66 According to recent study, even some children with heterotopias and polymicrogyria may have collagenopathy. 43 High prevalence (16%) of COL4A1 variants has been found earlier in patients with porencephaly. 29 We found similar high occurrence (13%) of COL4A1/A2 variants among term-born children with antenatal or presumed antenatal periventricular venous infarction of various severity of periventricular venous infarction.
Type IV Collagens
Type IV collagen is abundantly detected in different tissues, causing a wide spectrum of phenotypes involving different organ systems, with brain abnormalities and neurologic sequelae being more prevalent.29,32,33 Type IV collagens are expressed in the basal membrane of a wide range of tissues, including vessel walls. Most of the pathogenic variants in COL4A1 are missense mutations inducing Gly substitution that disrupts the normal triple helix configuration of the collagen. In the HGMDPro database, 24 splicing mutations, 4 pathogenic small deletions, and 5 small insertions have been described earlier as pathogenic. The variable expressivity of these genetic variants leads to the underdiagnosing of this condition. In the general population's database gnomAD v2.1.1, the total allele frequency of loss-of-function variants and the variants listed as (likely) pathogenic in the ClinVar database for COL4A1 is 0.00302, which translates to a carrier prevalence of 1 per 1650. The COL4A1 variants have been found more often compared to COL4A2.
Defective COL4A1 gene compromises the structural integrity of the vascular basal membrane with interruptions of the basement membrane of capillaries with both normal and markedly increased thickness of the basement membrane. 31 Collagenopathies cause microangiopathy, leading to development of porencephaly and/or schizencephaly with variable clinical severity from asymptomatic to fatal cases.29–33,42,43,66 High prevalence of microbleeds, cerebral white matter abnormalities and lacunar infarcts were found among children with collagenopathies, indicating the shared pathogenesis of microangiopathy.31,42 Severe and/or multifocal ischemic/hemorrhagic cerebral lesions can be of different ages and associated with schizencephaly and porencephaly. 42
MRI changes in children with COL4A1/A2 variants show a wide spectrum of severity,29,31–33,42,47 as was also seen in our study of children with periventricular venous infarction. Children with periventricular venous infarction usually have single, asymmetric periventricular white matter damage, persistent over time, the prognosis is highly dependent on the location and severity of the stroke.1,3,35 Among collagenopathies, porencephalic enlargement of the lateral ventricles and/or periventricular white matter damage can be unilateral or bilateral.29,31,42 Only 2 of 7 children in our group had unilateral periventricular stroke, 1 child had mild unilateral brain damage and white matter hyperintensities, whereas all others had bilateral changes. Most of the children with collagenopathies have severe porencephaly involving several lobes, or multifocal porencephalic brain damage with irregular borders, which can be of different ages. 42 According to our study, children with collagenopathy had significantly more often multifocal bilateral stroke, extensive bilateral periventricular gliosis, moderate to severe irregular enlargement of lateral ventricles and also moderate to severe decrease in the size of the caudate nucleus, putamen, and thalami, compared to children with periventricular venous infarction without genetic changes. Extensive bilateral diffuse white matter T2-weighted signal hyperintensities and extensive bilateral white matter loss and lacunae on MRI were noted more often in children with collagenopathies, indicating microangiopathy, as has been found earlier. 33 Presence of hemosiderin as well as schizencephaly and thin corpus callosum, were not different between groups. We found bilateral calcifications in all 3 children with collagenopathies, with an available computed tomography examination, as reported earlier.29,42,47 Therefore, besides congenital infections, also collagenopathies should be considered as a differential diagnosis in cerebral calcifications.
Individuals affected with collagenopathies have a wide spectrum of phenotypes causing congenital hemiparesis, epilepsy, intellectual disability, leukoencephalopathy, microbleeds, and lacunar stroke.32,33,43,47 Severe motor deficit and epilepsy developed more often in children with pathogenic variants in collagen genes (85.7%) compared to children without genetic variants (20.7%), respectively. Epilepsy has been found earlier in 55 of 123 patients with COL4A1/2 pathogenic variants. 33 Of 7 patients with COL4A1/A2 and COL5A1 pathogenic variants 4 had epilepsy also in our study. Outcome in patients with collagenopathies can worsen due to spontaneous intracranial macrohemorrhages later in life, 31 as was also seen in one of our patients.
Collagens V and I
Besides COL4A1/A2 variants, we found COL5A1 pathogenic variant in a premature child with severe intraventricular hemorrhage and periventricular hemorrhagic infarction. In 3 children, a variant of unknown significance was identified in COL5A1 and in 3 children, in COL1A1. To our knowledge, it is the first study to present a case with pathogenic COL5A1 variants with intraventricular hemorrhage and periventricular hemorrhagic infarction. Type V collagenopathies are known to cause the classical type of Ehlers-Danlos syndrome and type I collagenopathies cause the classical, vascular, or arthrochalasia type Ehlers-Danlos syndrome. Type V collagen is coexpressed with type I collagen in many connective tissues and plays an important role in the fibrillogenesis of this collagen type. In Ehlers-Danlos syndrome, bleeding diathesis is explained by an abnormal capillary structure with a deficiency of normal perivascular collagen, resulting in poor support for cutaneous blood vessels that can rupture when subjected to shearing forces. Specific gene variants of COL1A1 can lead to arterial rupture or dissection <40 years of age. 67 COL5A1 was identified as one of the genes associated with predisposition for preterm birth. 68
The fact that COL4A1/A2 and COL5A1 pathogenic variants are so prevalent in children with antenatal and presumed antenatal periventricular hemorrhagic infarction/periventricular venous infarction and also in preterm-born children with periventricular hemorrhagic infarction, can be explained by the period of developmental between gestational weeks 24 and 34 when periventricular hemorrhagic infarction/periventricular venous infarction occurs,3,8,13 as described also in previous studies focusing on antenatal intraventricular hemorrhage and periventricular hemorrhagic infarction cases.15,16 The median age of the diagnosis of fetal hemorrhage was gestational week 24 (22-26) in fetuses with COL4A1/A2 variants and gestational week 32 (29.5-34.5) in fetuses without genetic changes. 42 It can be presumed that if the child has a pathogenic variant in COL4A1/A2 or COL5A1, the disruption of the immature fragile vessels and hemorrhage in the germinal matrix is more likely to occur. Not only environmental factors during pregnancy, distress at birth, or fluctuations in the cerebral blood flow but also genetic factors may be important in development of severe intraventricular hemorrhage and periventricular hemorrhagic infarction/periventricular venous infarction in fetuses and neonates.48,49 It has even been suggested that in some periventricular hemorrhagic infarction/periventricular venous infarction cases genetic predisposition like connective tissue disorders might be the leading factor for intraventricular hemorrhage development.29,33,42,46,49 According to our study, gene variants leading to collagenopathies, coagulopathies, and other genetic changes connected with microangiopathy are frequently found among children with periventricular hemorrhagic infarction/periventricular venous infarction.
Familial Segregation of the Variants
COL4A1/2 and COL5A1/2 variants can be familial and hence both parents and siblings must be investigated.29,31,43,45,66 In our study, we have so far identified 2 families with a presumed antenatal periventricular venous infarction child with COL4A1 pathogenic variants and 1 family with COL5A1 variant and a preterm-born child with periventricular hemorrhagic infarction. Collagenopathies are inherited in an autosomal-dominant pattern with incomplete penetrance, in which case MRI is unable to identify all cases. 30 There were 2 children with presumed antenatal periventricular venous infarction with collagenopathy and only unilateral periventricular stroke, like most of the periventricular hemorrhagic infarction/periventricular venous infarction children without an identified genetic cause of periventricular venous infarction before this study. We had a familial case of COL4A1 variants with only mild motor deficit, mild unilateral periventricular damage, and bilateral white matter hyperintensities indicating microangiopathy; the boy developed hemorrhagic stroke by the age of 22 years with poor neurodevelopmental outcome. As reported earlier, hemorrhages can occur later in life in patients with COL4A1 gene variant. 31 This accentuates again the need for the genetic testing of children with periventricular hemorrhagic infarction/periventricular venous infarction with only mild hemiparesis/motor deficit, mild signs of periventricular brain damage, unilateral stroke and/or signs of microangiopathy, because of the recurrence risk of intracerebral hemorrhages.
Perinatal Risk Factors
We found no pregnancy, delivery, or neonatal symptoms that could distinguish periventricular hemorrhagic infarction/periventricular venous infarction children with collagenopathy from those without an identified genetic cause, as also suggested earlier. 33 If antenatal periventricular hemorrhagic infarction is not detected with prenatal ultrasonography, the birth is likely to be uneventful like in children with presumed antenatal stroke. However, the head circumference of 3 of 7 children in our group with collagenopathy was <10 percentiles, all with bilateral porencephaly and white matter loss, and poor outcome with severe motor deficit. This finding indicates that a small head circumference at birth can be a possible sign of congenital brain damage, including periventricular hemorrhagic infarction and collagenopathy. Collagenopathy and antenatal stroke should be one of the differential diagnoses in children with microcephaly at birth, as noted earlier.29,33
Coagulopathy
The role of inherited thrombophilia in the pathogenesis of perinatal stroke is still controversial. Some studies have suggested abnormalities in coagulation as a possible cause of perinatal stroke.23,41 Others have found that thrombophilia risk is not increased in perinatal stroke in term-born children, including presumed antenatal periventricular venous infarction and arterial ischemic stroke, compared to controls.39,63 Recent study highlight the importance of arterial endothelial dysfunction, rather than thrombocytopenia. 69 An earlier study of preterm infants with an atypical presentation of periventricular hemorrhagic infarction recommends testing of thrombophilia, especially for factor V Leiden and prothrombin gene mutation, which was found in 7 of 17 cases, although COL 4A1 gene variants were found in 2 of 17 cases. 70 The prothrombin (F2) 20210G>A [rs1799963 G>A] genetic variant and the factor V Leiden mutation predispose to inherited thrombophilia with the highest prevalence of the genetic variant in Caucasian population. 70 An earlier study in Estonia has established a prevalence of the carriers of prothrombin common variant in 3.3% and of the carriers of Factor V Leiden variant in 3% among the tested 400 controls. 63 In a review article on the genetic profiling of antenatal intracranial hemorrhage, Cavaliere and coworkers 41 found 2 case reports with factor V deficiency, but none with the prothrombin 20210G>A variant. 41 Although our study did not find increased prevalence of the factor V Leiden and prothrombin 20210G>A gene variants in the small cohort of children with periventricular hemorrhagic infarction/periventricular venous infarction, we cannot exclude predisposition to stroke in children with these genetic variants. One preterm-born child with periventricular hemorrhagic infarction had antithrombin 3 deficiency due to the SERPINC1 variant inherited from the father.
Other Genes
Interestingly, we found 2 variants in other genes that can be connected with microangiopathy and stroke or strokelike episodes, both being familial cases. In the the group of periventricular hemorrhagic infarction among preterm-born children one child had the most common mitochondrial variant m.3243A>G in MT-TL1 like her mother and other family members with the family history of hearing loss, diabetes, and migraine. However, the causality of mitochondrial DNA variation in the MELAS (Mitochondrial myopathy, Encephalopathy, Lactic Acidosis, and Strokelike episodes) syndrome in relation to our clinical findings is uncertain. Still, the MELAS syndrome is known to lead to microvascular blood perfusion damage and strokelike episodes at age <40 years with serious long-term consequences. 61
A child with presumed antenatal periventricular hemorrhagic infarction and a pathogenic change in NOTCH3 inherited from father that is known to lead to CADASIL (Cerebral Autosomal Dominant arteriopathy with Subcortical Infarcts and Leukoencephalopathy). He had focal porencephaly and severe motor deficit but no other signs of microangiopathy by the age of 9 years. Although the prenatal diagnosis of NOTCH variant has been reported earlier in the fetus of a couple where the father had a known gene variant, 71 the finding has not been reported for children with perinatal stroke.
Indications for Testing
Periventricular hemorrhagic infarction/periventricular venous infarction leads to lifelong impairments: motor deficit of various severity, cognitive impairment, behavioral problems, and epilepsy.13,17,22,36,72 Poor outcome has been found in survivors among preterm children with periventricular hemorrhagic infarction. 35 Systematic genetic testing has been suggested earlier in term-born children with intraparenchymal hemorrhages, 42 in children with antenatal intracranial hemorrhage, especially in severe cases, 41 and in children with porencephaly. 29 Systemic genetic evaluation in patients with periventricular hemorrhagic infarction/periventricular venous infarction is not a routine clinical practice. Although the most severe cases were diagnosed already clinically, 5 of 11 children with pathogenic/likely pathogenic variants had not been tested earlier as genetic disease was not suspected in mild cases. Awareness of the genetic causes of periventricular hemorrhagic infarction/periventricular venous infarction gives the children's parents an understanding that it is not only preterm birth, perinatal stress, postnatal environment, or possible treatment failure that can cause severe periventricular hemorrhagic infarction.48,49 Therefore, we suggest that in all children with periventricular hemorrhagic infarction/periventricular venous infarction, both term-born and preterm, genetic testing should be considered, especially in the case of bilateral and multifocal stroke with bilateral white matter alterations; however, even with unilateral periventricular hemorrhagic infarction/periventricular venous infarction. First of all, collagen genes (COL4A1/A2 and COL5A1/A2) leading to vascular instability need to be investigated, whereas other genes associated with perinatal stroke and coagulopathies may need to be evaluated. Thus, large gene panel or exome sequencing should be preferred. Identifying the genetic cause of periventricular hemorrhagic infarction/periventricular venous infarction can guide one to counseling for recurrence risks in the family and identify the threat of later macrohemorrhages in early adulthood.
Limitations
The most important limitation of the study is the small size of the groups of term-born children with antenatal and presumed antenatal periventricular hemorrhagic infarction/periventricular venous infarction and preterm-born children with periventricular hemorrhagic infarction. Yet it is the largest study of patients with presumed antenatal periventricular venous infarction who were evaluated genetically and radiologically as a cohort.
None of the preterm-born children with periventricular hemorrhagic infarction diagnosis who died had been genetically tested except for 2 cases among preterm children in whom the samples for genetic testing were taken prior to death. Therefore, there can be more children with genetic variants among the preterm population with severe intraventricular hemorrhage or periventricular hemorrhagic infarction, as children with the worst outcomes were not tested.
Conclusion
Our data suggest that children with periventricular hemorrhagic infarction/periventricular venous infarction have high prevalence of pathogenic variants in collagen genes (COL4A1/A2 and COL5A1). Genetic testing should be considered for all children with periventricular hemorrhagic infarction/periventricular venous infarction; COL4A1/A2 and COL5A1/A2 genes should be investigated first.
Supplemental Material
sj-csv-1-jcn-10.1177_08830738231186233 - Supplemental material for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction
Supplemental material, sj-csv-1-jcn-10.1177_08830738231186233 for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction by Norman Ilves, Sander Pajusalu, Tiina Kahre, Rael Laugesaar, Ustina Šamarina, Dagmar Loorits, Pille Kool and Pilvi Ilves in Journal of Child Neurology
Supplemental Material
sj-csv-2-jcn-10.1177_08830738231186233 - Supplemental material for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction
Supplemental material, sj-csv-2-jcn-10.1177_08830738231186233 for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction by Norman Ilves, Sander Pajusalu, Tiina Kahre, Rael Laugesaar, Ustina Šamarina, Dagmar Loorits, Pille Kool and Pilvi Ilves in Journal of Child Neurology
Supplemental Material
sj-docx-3-jcn-10.1177_08830738231186233 - Supplemental material for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction
Supplemental material, sj-docx-3-jcn-10.1177_08830738231186233 for High Prevalence of Collagenopathies in Preterm- and Term-Born Children With Periventricular Venous Hemorrhagic Infarction by Norman Ilves, Sander Pajusalu, Tiina Kahre, Rael Laugesaar, Ustina Šamarina, Dagmar Loorits, Pille Kool and Pilvi Ilves in Journal of Child Neurology
Footnotes
Acknowledgments
The authors thank all pregnant women, patients and their parents, as well as colleagues from the Department of Genetics of Tartu University Hospital for their contribution.
Author Contributions
Conceptualization: NI, RL PI; Data curation: NI, TK, RL PI; Formal Analysis: NI, SP, TK, US; Funding acquisition: RL, PI, SP; Supervision: PI, SP; Statistical analysis: PK, NI, PI; Writing – original draft: NI, PI, TK, RL, SP; Writing – review & editing: all authors. All authors contributed to manuscript revision, read, and approved the submitted version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Estonian Research Council grants (PUT148, PRG471, PSG774, PRG1912, MOBTP175) and basic financing from the University of Tartu.
Supplemental Material
Supplemental material for this article is available online.
Ethical Approval
The studies were approved by the Ethics Review Committee on Human Research of the University of Tartu by protocol no 294/M-18. Written informed consent was provided by all individual participants older than 7 years and by their parents in all cases.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.