
Abstract
Objective:
To evaluate the safety and tolerability of adjunctive eslicarbazepine acetate (ESL) in pediatric patients (aged 4-17 years) with refractory focal seizures.
Methods:
Pooled safety data from patients aged 4-17 years in Study 208 (NCT01527513) and Study 305 (NCT00988156) were analyzed. Both were randomized, double-blind, placebo-controlled studies of ESL as adjunctive treatment in pediatric patients with refractory focal seizures receiving 1 or 2 antiepileptic drugs. Incidences of treatment-emergent adverse events (TEAEs), serious adverse events (SAEs), TEAEs leading to discontinuation, and TEAEs of special interest were evaluated.
Results:
The safety population comprised 362 patients (placebo, n = 160; ESL, n = 202). The overall incidence of TEAEs was similar between the ESL (67.8%) and placebo groups (65.6%), with no clear dose-response relationship. The most frequently reported TEAEs with ESL were headache, somnolence, vomiting, and diplopia. Overall incidences of SAEs and TEAEs leading to discontinuation were higher with ESL versus placebo (9.9% vs 5.0% and 5.9% vs 2.5%, respectively). The majority of SAEs with ESL occurred in Study 305. Two deaths were reported, 1 with ESL (0.5%) due to cluster seizures (resulting in herniation of the cerebellar tonsils) and 1 with placebo (0.6%) due to asphyxia. TEAEs related to allergic reaction, hyponatremia, hypothyroidism, cytopenia, seizure exacerbation, cognitive dysfunction, psychiatric disorders, or suicide occurred infrequently (<9%).
Conclusion:
Adjunctive ESL was generally well tolerated in children aged 4-17 years with focal seizures. The safety profile of ESL in children was comparable to that observed in adults.
The diagnosis of epilepsy is common in childhood. 1 Therefore, it is important to have sufficient options for the treatment of seizures in children. Eslicarbazepine acetate (ESL) is a once-daily, crushable, oral antiepileptic drug (AED) tablet for focal-onset (partial-onset) seizures. Five phase III clinical trials found that ESL was effective and well tolerated in adults (≥18 years) with focal seizures and supported the approval of ESL in the USA. 2,3
The Pediatric Research Equity Act requires that all drug applications to the US Food and Drug Administration (FDA) contain a pediatric assessment. 4 Based on analyses conducted by the FDA, the University of Maryland, and the Pediatric Epilepsy Academic Consortium for Extrapolation, exposure-response relationships are considered preserved between adult and pediatric subjects (aged ≥4 years) with focal seizures. 5 In order to obtain approval for use in children with focal seizures based on extrapolation of efficacy, the FDA provided guidance requiring that an AED meet 3 criteria: (1) an approved indication for treatment of focal seizures in adults, (2) a pharmacokinetic (PK) analysis to show that the proposed dosing regimens in children result in drug exposure similar to that demonstrated to be safe and effective in adults, and (3) long-term, open-label safety data in children aged ≥4 years. 5 -11
A subset of data pooled from 2 European double-blind clinical trials (with open-label extensions [OLEs]) of adjunctive ESL in children aged 2-18 years with focal seizures were used to support the FDA approval of ESL for the treatment of focal seizures in children aged ≥4 years. 12,13 Here, we report a post hoc analysis of the pooled data, which evaluates safety and tolerability outcomes (overall, and according to patient age or weight) with adjunctive ESL in the subpopulation of pediatric patients aged 4-17 years with focal seizures.
Methods
Study Design
Ethical approval
The 2 European studies were designed, conducted, and monitored in accordance with the principles of the Declaration of Helsinki, the International Conference on Harmonization guidelines, and relevant national and local laws. The study protocols were approved by the relevant independent ethics committees/institutional review boards, and all patients provided written informed consent.
Study 208
Study 208-part 1 (NCT01527513) was a randomized, double-blind, placebo-controlled, 12-week, phase II study with the primary objective of evaluating the cognitive effects of adjunctive ESL in children aged 6-16 years with ≥2 focal seizures in the month prior to screening. 12 Eligibility criteria, site locations, primary and secondary outcomes, and sample size determination have previously been reported. 12 An intelligence quotient (IQ) ≥70 was an inclusion criterion in this study, but not in study 305.
At the end of the baseline period, eligible patients were randomized 1:2 to receive double-blind placebo or ESL; patients continued to receive therapy with 1 or 2 background AEDs. Concomitant use of oxcarbazepine (OXC) was an exclusion criterion. ESL was titrated to the target dose (30 mg/kg/d) over 4 weeks (10 mg/kg/d for 2 weeks, 20 mg/kg/d for 2 weeks) (Figure 1A). If patients tolerated 20 mg/kg/d during the titration period, the dose was increased to 30 mg/kg/d (maximum dose: 1200 mg/d) for the 8-week maintenance period. Dose reduction was allowed once, during either the titration period (from 20 to 10 mg/kg/d) or the maintenance period (from 30 to 20 mg/kg/d). Use of rescue benzodiazepines was allowed.
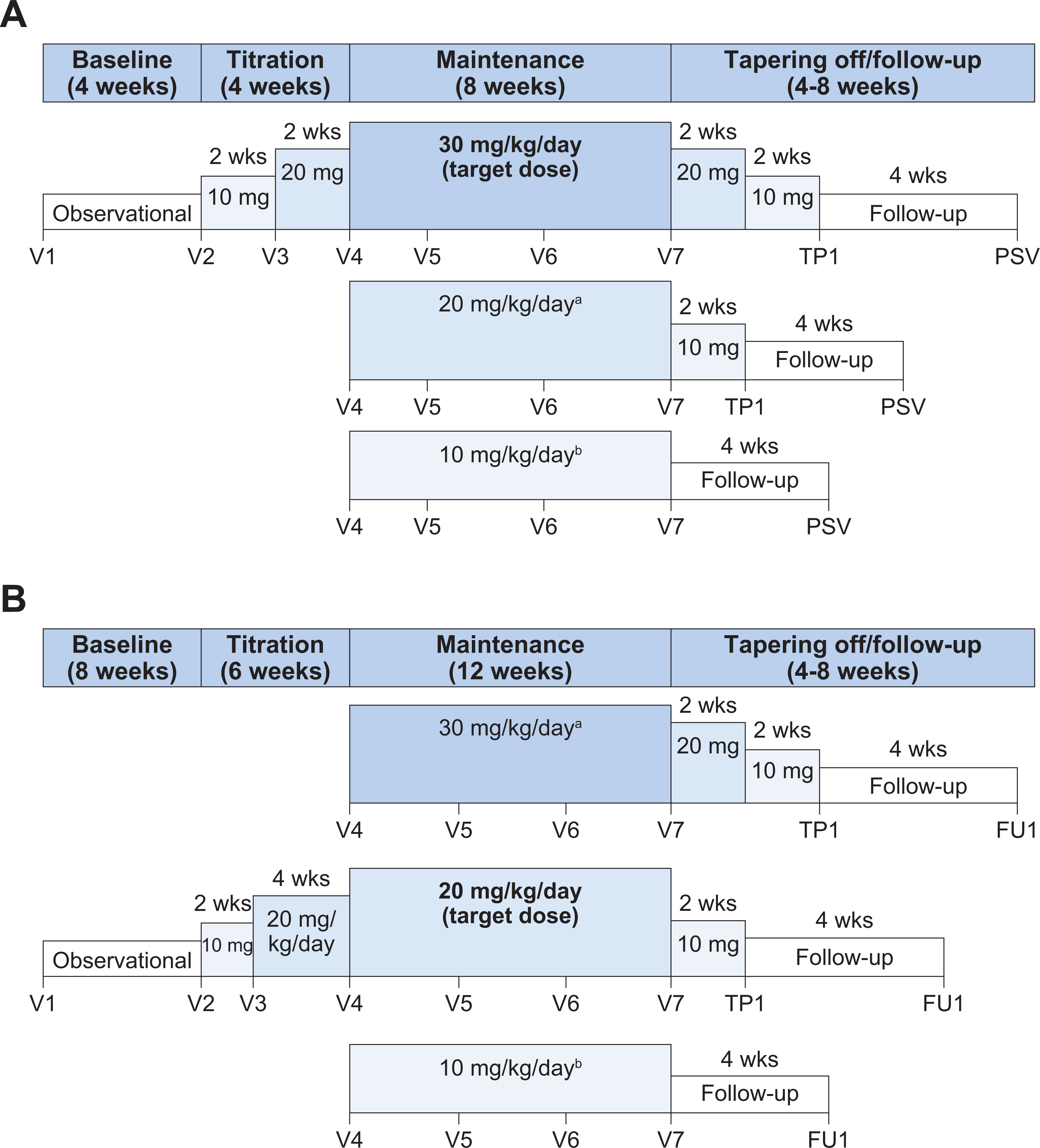
Study designs. (A) Study 208. aFor patients that down-titrated from 30 mg/kg/d because of intolerable AEs during the maintenance period. bFor patients who down-titrated from 20 mg/kg/d because of intolerable AEs during the titration period. (B) Study 305. aFor patients in which tolerability was considered acceptable but therapeutic response was insufficient. bFor patients who down-titrated from 20 mg/kg/d because of intolerable AEs. AE, adverse event; FU, follow-up; PSV, post-study visit; TP, tapering off; V, visit.
Patients could continue into a 1-year, uncontrolled, OLE (part 2) and subsequently into a 2-year OLE (part 3).
Study 305
Study 305-part 1 (NCT00988156) was a randomized, double-blind, placebo-controlled, 18-week, phase III study that evaluated the efficacy and safety of ESL in children aged 2 to 18 years with ≥4 focal seizures in the month prior to enrollment. 13
Patients previously treated with ≤3 AEDs at their maximum tolerated doses for at least 1 month without seizure control and currently treated with 1 or 2 AEDs were eligible to participate. Patients were required to take background AEDs at stable doses during the 8-week baseline period. At the end of the baseline period, eligible patients were randomized 1:1 to receive double-blind placebo or ESL; patients continued to receive therapy with 1 or 2 background AEDs. Children aged ≤6 years were treated with an oral suspension and those aged >7 years were treated with tablets (the protocol neither required nor prohibited the crushing of tablets). Concomitant use of OXC was an exclusion criterion. ESL was titrated to the target dose (20 mg/kg/d) over 6 weeks (10 mg/kg/d for 2 weeks, 20 mg/kg/d for 4 weeks) (Figure 1B). If tolerability and therapeutic response were considered acceptable after the titration period, patients continued to receive 20 mg/kg/d during the 12-week maintenance period. If tolerability was considered acceptable but therapeutic response was insufficient, the dose was increased to 30 mg/kg/d (maximum dose: 1200 mg/d) for the 12-week maintenance period. Dose reduction was allowed once, during either the titration period (from 20 to 10 mg/kg/d) or the maintenance period (from 30 to 20 mg/kg/d or 20 to 10 mg/kg/d). Use of rescue benzodiazepines was allowed ≤2 times per week.
Patients could continue into a 1-year, uncontrolled OLE (part 2) and subsequently into 2 additional 1-year OLEs (parts 3-4), followed by a 2-year OLE (part 5).
Assessments and Data Analysis
Double-blind safety data from patients aged 4 to 17 years in part 1 of studies 208 and 305 were analyzed.
Patient demographics, clinical characteristics, and adverse events (AEs) were evaluated during the baseline period. Incidences of treatment-emergent adverse events (TEAEs), serious adverse events (SAEs), and TEAEs leading to discontinuation were evaluated during the double-blind treatment period. TEAEs and SAEs were categorized using the Medical Dictionary for Regulatory Activities version 13.1. Incidences were evaluated overall and according to subgroups defined by weight (11-21, 22-31, 32-38, and >38 kg) and age (4-6, 7-11, and 12-17 years).
All statistical analyses were based on the pooled safety population, which comprised all patients who received ≥1 dose of study medication during part 1 of study 208 or 305, excluding 41 patients in the 2- to 6-year-old age group in study 305 who were withdrawn due to stability issues with the ESL oral suspension used.
Results
Patients
The pooled safety population comprised 362 patients (placebo, n = 160; ESL, n = 202), 123 from study 208 (placebo, n = 40; ESL, n = 83) and 239 from study 305 (placebo, n = 120; ESL, n = 119). A total of 24 patients were excluded from the analyses as they were aged <4 years (placebo, n = 9; ESL, n = 15); no patient in study 208 or 305 was aged >17 years. Patient demographics and clinical characteristics were generally comparable between the placebo and ESL groups (Table 1). The majority of patients taking ESL were white (97%), enrolled at sites in Europe (98%), aged ≥7 years (89%), >38 kg in weight (55%), and taking 2 or more AEDs at baseline (70%). The most commonly used concomitant AEDs were valproic acid, carbamazepine, lamotrigine, topiramate, and levetiracetam.
Patient Baseline Demographics and Clinical Characteristics.
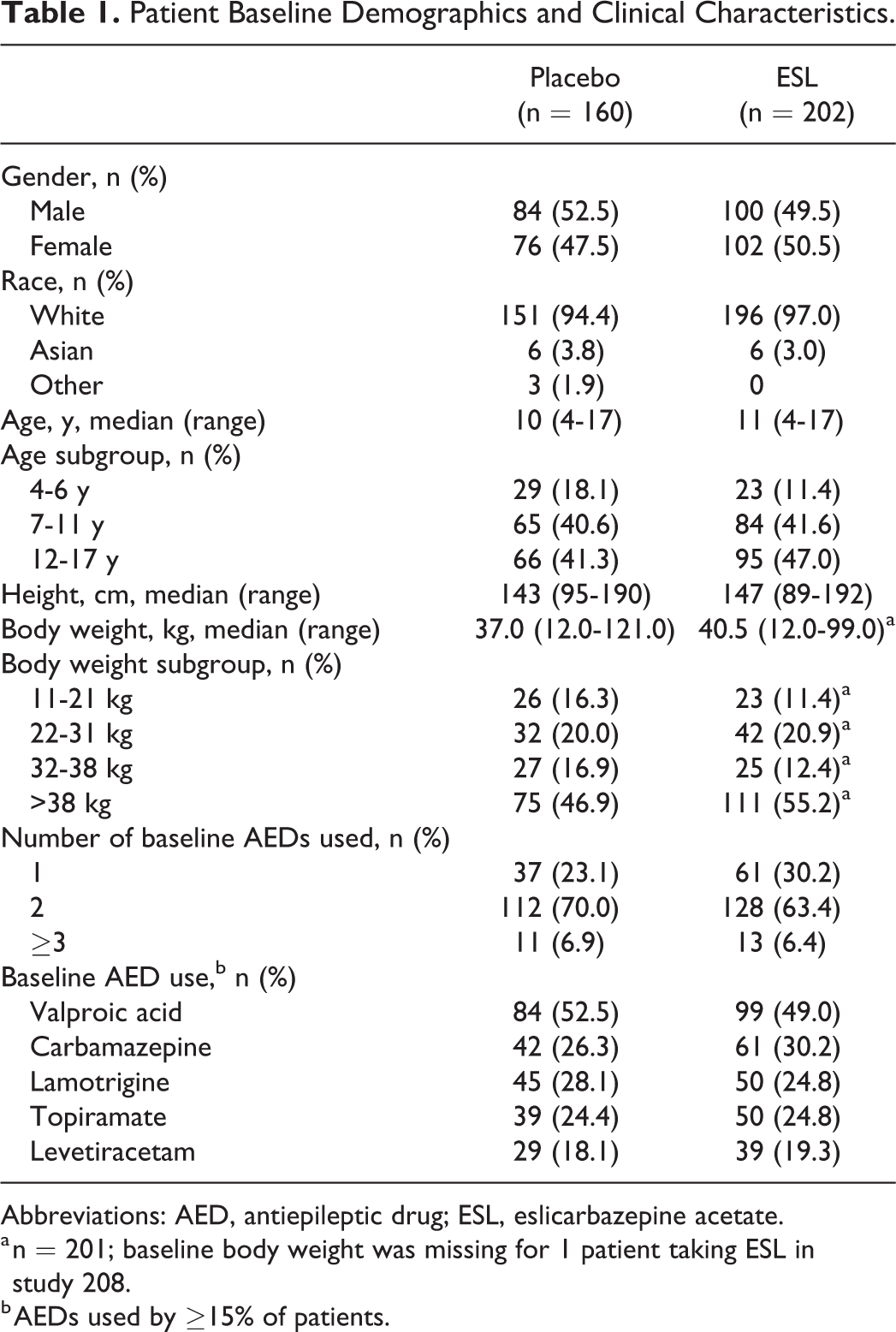
Abbreviations: AED, antiepileptic drug; ESL, eslicarbazepine acetate.
a n = 201; baseline body weight was missing for 1 patient taking ESL in study 208.
b AEDs used by ≥15% of patients.
Patients in the ESL group of study 305 were taking more baseline AEDs (study 305: 1 baseline AED 15.1%, 2 baseline AEDs 74.8%; study 208: 51.8% and 47.0%, respectively) and had a higher baseline monthly seizure frequency (study 305: mean [standard deviation (SD)], 54.4 [133.7]; study 208: 13.9 [24.1]) than those taking ESL in study 208. The mean (SD) daily dose of ESL was higher in study 208 (820.1 [246.0] mg/d) than study 305 (714.2 [264.1] mg/d), whereas median exposure to double-blind treatment with ESL was higher in study 305 (147 days [21 weeks]) than study 208 (112 days [16 weeks]).
Safety
Treatment-emergent adverse events
At baseline, the incidence of AEs in patients later randomized to ESL was greater than in patients later randomized to placebo (32.2% vs 20.6%, respectively). This was the case in both studies 208 (ESL, 18.1%; placebo, 12.5%) and 305 (ESL, 42.0%; placebo, 23.3%). The most frequently reported baseline AEs in patients later randomized to ESL (incidence ≥2% after rounding to the nearest whole percentage) were nasopharyngitis (ESL, 5.4%; placebo, 3.1%), headache (ESL, 3.0%; placebo, 2.5%), pyrexia (ESL, 2.0%; placebo, 2.5%), and pharyngitis (ESL, 2.0%; placebo, 1.3%).
During the double-blind treatment period, the overall incidence of TEAEs was similar between ESL (67.8%) and placebo (65.6%) overall (Table 2), and in most subgroups defined by body weight (Figure 2A) or age (Figure 2B). The 11- to 21-kg subgroup was an exception, in which the incidence of TEAEs was >10% greater with ESL versus placebo (ESL, 82.6%; placebo, 69.2%). The number of patients in this weight subgroup was small (ESL, n = 23; placebo, n = 26) and there was a relatively marked difference in AE incidence between treatment groups at baseline (ESL, 34.8%; placebo, 19.2%). Another exception was the 7 to 11 years subgroup, in which the incidence of TEAEs was >10% greater with ESL versus placebo (ESL, 75.0%; placebo, 63.1%). The difference in AE incidence between treatment groups was less marked at baseline in this subgroup (ESL, 29.8%; placebo, 20.0%). Overall, there was some evidence to suggest that overall TEAE incidence was slightly higher in younger patient subgroups, compared with the oldest subgroup (12-17 years); this trend was also apparent to a lesser extent at baseline. However, it is important to note that the number of patients in the 4- to 6-year subgroup was small. Overall, differences in AE incidence between the placebo and ESL groups during the double-blind period were generally less pronounced than during the baseline period.
Incidence of TEAEs During the Double-Blind Treatment Period.
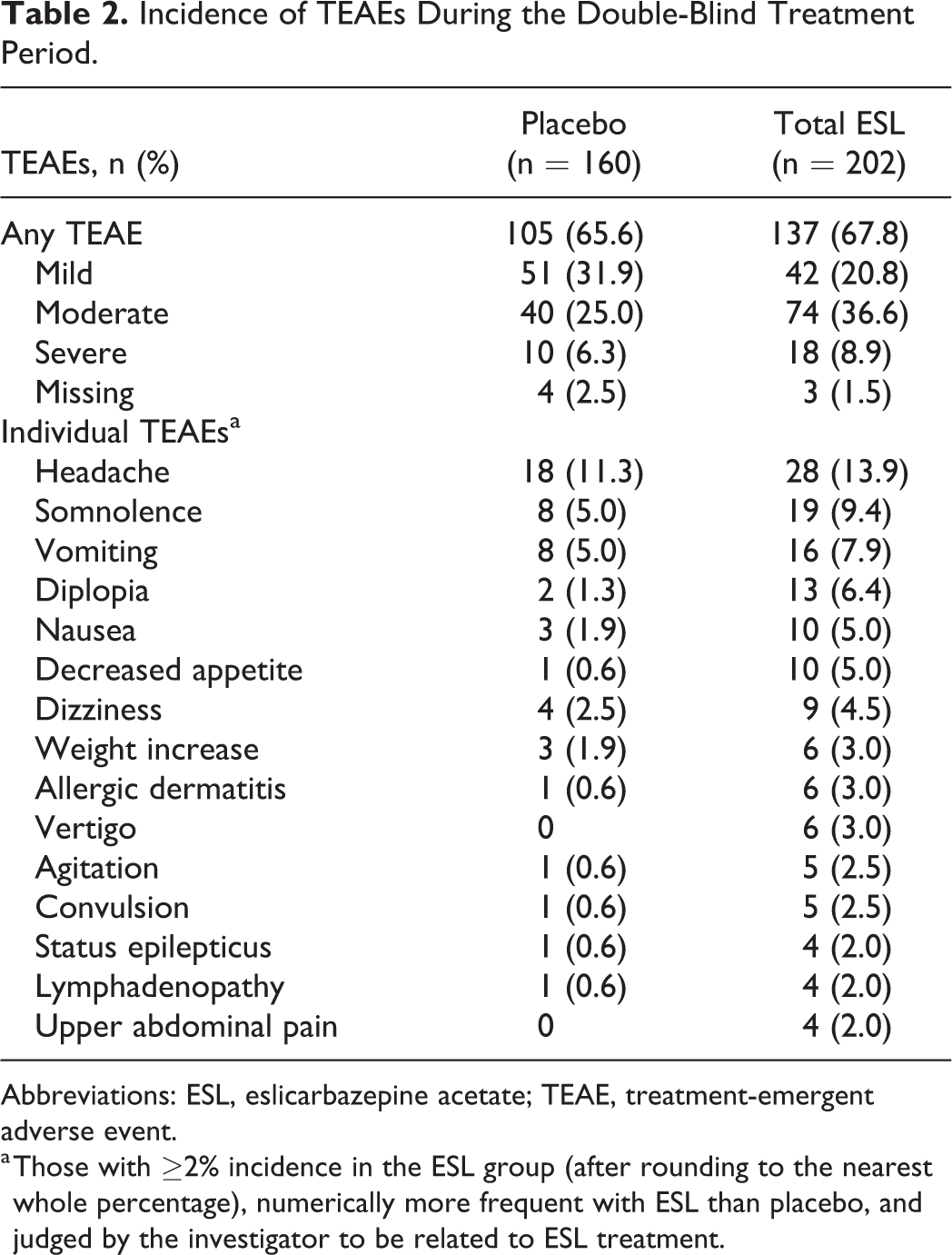
Abbreviations: ESL, eslicarbazepine acetate; TEAE, treatment-emergent adverse event.
a Those with ≥2% incidence in the ESL group (after rounding to the nearest whole percentage), numerically more frequent with ESL than placebo, and judged by the investigator to be related to ESL treatment.
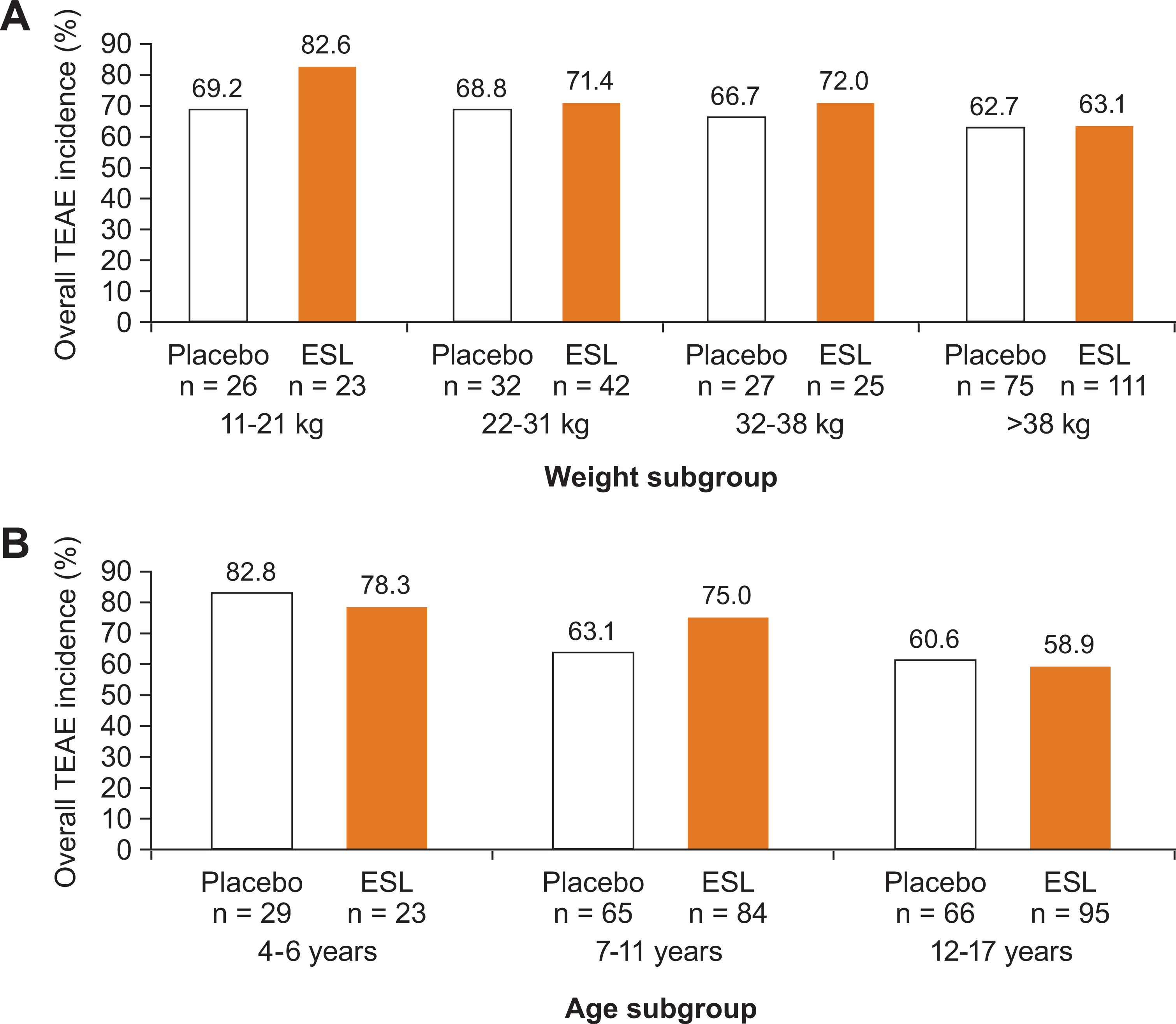
Overall TEAE incidence during the double-blind treatment period (A) by weight subgroup, and (B) by age subgroup. ESL, eslicarbazepine acetate; TEAE, treatment-emergent adverse event.
Headache, somnolence, vomiting, and diplopia were the most frequently reported TEAEs during the double-blind treatment period (Table 2). The majority of TEAEs were mild or moderate in severity. The incidence of severe TEAEs was numerically higher in the ESL group (8.9%) than in the placebo group (6.3%). Partial seizures (ESL, 3.0%; placebo, 1.3%) and status epilepticus (ESL, 1.5%; placebo, 0.6%) were the most frequently reported severe TEAEs in the ESL group.
When assessing TEAE incidence according to modal daily ESL dose category in subgroups defined by patient weight, neither overall TEAE incidence nor incidences of the most common individual TEAEs increased with increasing modal daily ESL dose in any weight subgroup (data not shown).
Serious adverse events and treatment-emergent adverse events leading to discontinuation
Overall, incidences of SAEs and TEAEs leading to discontinuation were numerically higher with ESL versus placebo (Table 3). In study 208, SAEs were infrequent with ESL (3 of 83, 3.6%); there were single cases of mitral valve incompetence, diabetes mellitus, and status epilepticus. All other SAEs with ESL were reported in study 305 (17 of 119, 14.3%). SAEs occurred in 5.0% of patients in the placebo group of study 208 and in the same proportion of patients in the placebo group of study 305.
Incidence of SAEs and TEAEs Leading to Discontinuation During the Double-Blind Treatment Period.a
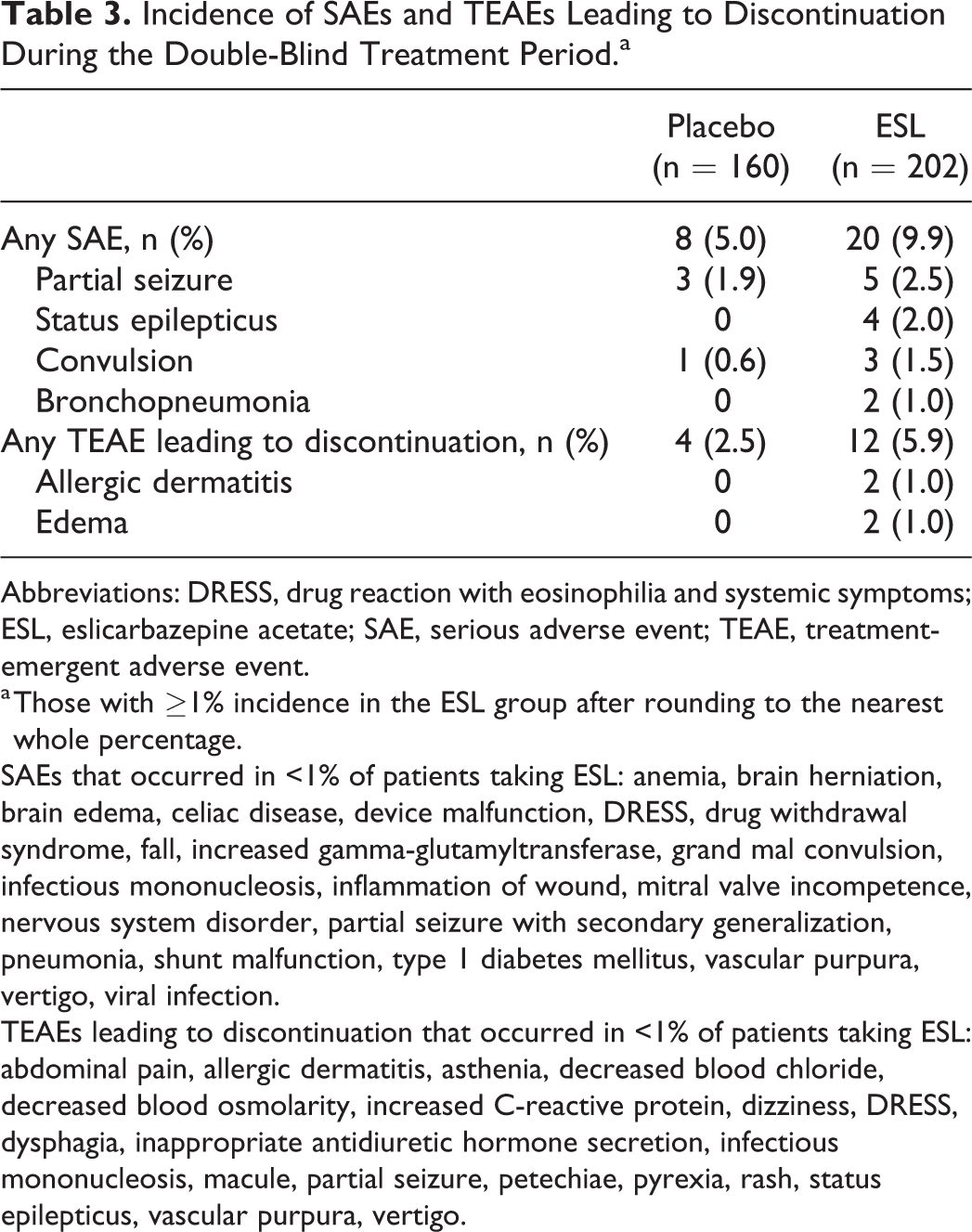
Abbreviations: DRESS, drug reaction with eosinophilia and systemic symptoms; ESL, eslicarbazepine acetate; SAE, serious adverse event; TEAE, treatment-emergent adverse event.
a Those with ≥1% incidence in the ESL group after rounding to the nearest whole percentage.
SAEs that occurred in <1% of patients taking ESL: anemia, brain herniation, brain edema, celiac disease, device malfunction, DRESS, drug withdrawal syndrome, fall, increased gamma-glutamyltransferase, grand mal convulsion, infectious mononucleosis, inflammation of wound, mitral valve incompetence, nervous system disorder, partial seizure with secondary generalization, pneumonia, shunt malfunction, type 1 diabetes mellitus, vascular purpura, vertigo, viral infection.
TEAEs leading to discontinuation that occurred in <1% of patients taking ESL: abdominal pain, allergic dermatitis, asthenia, decreased blood chloride, decreased blood osmolarity, increased C-reactive protein, dizziness, DRESS, dysphagia, inappropriate antidiuretic hormone secretion, infectious mononucleosis, macule, partial seizure, petechiae, pyrexia, rash, status epilepticus, vascular purpura, vertigo.
In most weight subgroups, incidences of SAEs and TEAEs leading to discontinuation were higher with ESL versus placebo, with no clear or consistent relationship between weight and occurrence of these events.
SAE incidences were higher with ESL versus placebo in the 4- to 6-year and 7- to 11-year subgroups (Figure 3A), and similar between ESL and placebo in older children (12-17 years subgroup: ESL, 9.5%; placebo, 9.1%). The difference in SAE incidence between ESL and placebo was greatest in the 4- to 6-year subgroup; however, because of the small number of patients in this subgroup, definitive conclusions cannot be drawn. Incidences of TEAEs leading to discontinuation were numerically higher with ESL versus placebo across age subgroups and were generally more frequent in younger patient subgroups (Figure 3B).
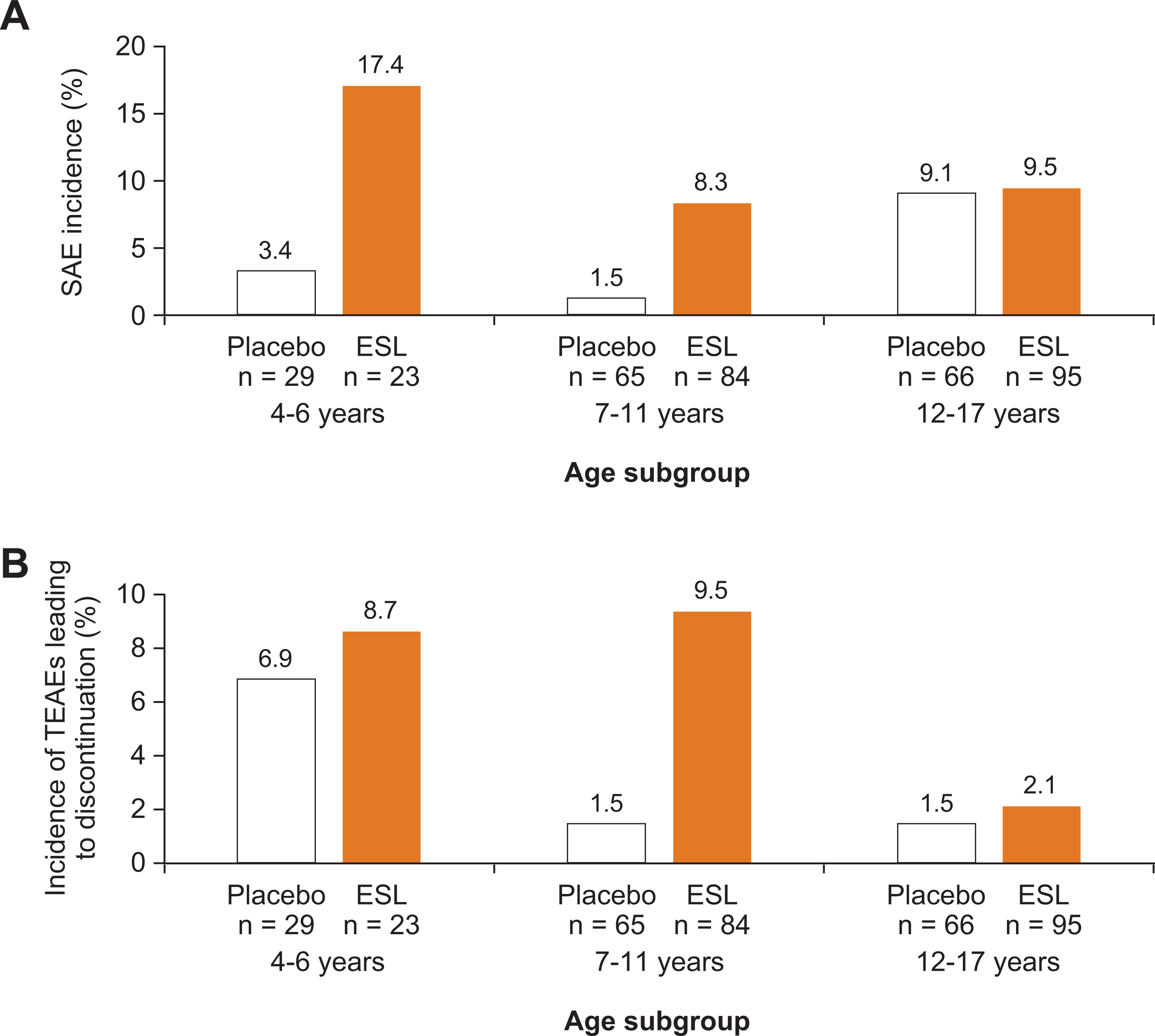
Overall incidence of (A) SAEs and (B) TEAEs leading to discontinuation during the double-blind treatment period, by age subgroup. ESL, eslicarbazepine acetate; SAE, serious adverse event; TEAE, treatment-emergent adverse event.
Two deaths occurred during the studies. One patient taking ESL died because of cluster seizures on day 55 of study 305, approximately half way through maintenance treatment with ESL; this patient experienced additional SAEs of brain edema, bronchopneumonia, and herniation of the cerebellar tonsils. The investigator confirmed that the SAE of cluster seizures was the primary event leading to the fatal outcome; cluster seizures were considered “not related” to treatment with ESL by the investigator and “possibly related” by the sponsor. One patient in the placebo group died due to asphyxia; a plastic bag was found in the patient’s mouth.
Treatment-emergent adverse events of special interest
Allergic dermatitis (ESL, 3.0%; placebo, 0.6%) and rash (ESL, 1.0%; placebo, 1.3%) were the most frequently reported rash-related TEAEs. Drug reaction with eosinophilia and systemic symptoms (DRESS) was reported in 1 patient (0.5%) taking ESL. No cases of Stevens-Johnson syndrome or toxic epidermal necrolysis were reported.
Hyponatremia was not reported as a TEAE, but 1 patient in the ESL group (0.5%) had a post-dose plasma sodium concentration ≤125 mEq/L; this patient had a 3 mEq/L reduction in sodium concentration from baseline to the lowest on-treatment value during the double-blind treatment period (from 127 to 124 mEq/L). A decrease in plasma sodium from baseline >10 mEq/L was observed in 3 patients taking ESL (1.5%) and 1 taking placebo (0.6%). Hypothyroidism was infrequent in both treatment groups (ESL, 1.0%; placebo, 0.6%). Cytopenia occurred in 2.0% of patients taking ESL (neutropenia, 1.5%; anemia, 0.5%); no cases of cytopenia were reported in the placebo group.
The overall incidence of seizure exacerbation was similar between treatment groups (ESL, 8.9%; placebo, 6.3%). The majority of TEAEs related to exacerbation of seizures occurred in study 305 (ESL, 14.3%; placebo, 7.5%), with fewer in study 208 (ESL, 1.2%; placebo, 2.5%). Overall, the most frequently reported TEAEs related to seizure exacerbation were partial seizure (ESL, 4.5%; placebo, 4.4%), convulsion (2.5% and 0.6%), and status epilepticus (2.0% and 0.6%).
TEAEs related to cognitive dysfunction were infrequent; 4 occurred in patients taking ESL (amnesia: ESL 0.5%, placebo 0; aggression: ESL 0.5%, placebo 0; confusional state: ESL 0.5%, placebo 0; and bradyphrenia: ESL 0.5%, placebo 0) and 2 occurred in patients taking placebo (cognitive disorder: ESL 0, placebo 0.6%; and disturbance in attention: ESL 0, placebo 0.6%). All cognitive dysfunction-related TEAEs were reported in study 305.
Psychiatric or suicide-related TEAEs were infrequent; 5 occurred in ≥1% of patients taking ESL (agitation: ESL 2.5%, placebo 0.6%; abnormal behavior: ESL 1.5%, placebo 0; anxiety: ESL 1.0%, placebo 0.6%; insomnia: ESL 1.0%, placebo 2.5%; mood swings: ESL 1.0%, placebo 0). Aggression occurred in 1 patient taking ESL (0.5%; also reported above as a cognitive dysfunction-related treatment-emergent adverse event [TEAE]) and none taking placebo. No psychiatric SAEs or TEAEs leading to discontinuation were reported.
Discussion
Overall, this analysis of safety data demonstrates that ESL was generally well tolerated in children aged 4 to 17 years.
Although the overall incidence of AEs at baseline was more frequent in patients later randomized to ESL, the overall incidence of TEAEs was similar between ESL (68%) and placebo (66%) during the double-blind period, and comparable to TEAE rates observed during trials of ESL in adults aged ≥18 years (ESL, 73%; placebo, 57%). 2 There was no clear relationship between ESL dose and occurrence of TEAEs. Headache, somnolence, vomiting, and diplopia were the TEAEs reported most frequently during double-blind treatment with ESL, consistent with those most frequently reported during trials of ESL in adults. 2
The overall incidence of TEAEs was also similar between ESL and placebo in most subgroups defined by body weight or patient age. When analyzed according to age-related subgroups, the differences in overall incidence of AEs between ESL and placebo were generally less marked during double-blind treatment versus baseline, suggesting that ESL was well tolerated in these trials.
In the 11- to 21-kg weight subgroup, the incidence of TEAEs was greater with ESL versus placebo. The incidence of AEs was also higher with ESL (vs placebo) at baseline, suggesting potential differences in patients between treatment groups in this weight subgroup; nevertheless, it is important to note that the number of patients in this subgroup was small (ESL, n = 23; placebo, n = 26). The overall incidence of TEAEs was also higher with ESL versus placebo in the 7- to 11-year subgroup. Indeed, there was some evidence to suggest that overall TEAE incidence was slightly higher in younger patient subgroups, compared with the oldest subgroup (12-17 years); this trend was also apparent at baseline, although less marked. Again, it is important to note that the number of patients in the 4- to 6-year subgroup was small. These trends are consistent with previous research findings that certain adverse effects associated with AEDs can occur more frequently in younger versus older age groups, potentially related to PK differences between children and adolescents. 14,15
Incidences of SAEs and TEAEs leading to discontinuation were numerically higher with ESL versus placebo in the younger age groups. In the 4- to 6-year subgroup, a higher proportion of patients were taking ≥2 baseline AEDs in the ESL group than in the placebo group, a factor that may have contributed to this effect in the youngest age group. TEAEs leading to discontinuation were generally more frequent in younger age groups, and the difference in incidence of SAEs between ESL and placebo was least notable in the oldest age group, again suggesting that adverse effects to AEDs, including ESL, may be more frequent in younger children.
The majority of SAEs occurred in study 305, with only 3 occurring with ESL in study 208. The incidence of SAEs with placebo was the same in both studies. There were some differences in inclusion and exclusion criteria, and patient demographic and clinical characteristics between studies 208 and 305, which may, at least in part, explain the higher incidence of SAEs in study 305 versus study 208. Patient age differed slightly between studies (study 208: 6-16 years; study 305: 2-17 years [only patients aged >4 years were included in this analysis]), and patients entering study 305 were required to have a higher baseline seizure frequency (≥4 focal seizures in the month prior to enrollment) than those entering study 208 (≥2 focal seizures in the month prior to screening). Furthermore, patients entering study 208 were required to have an IQ of ≥70, whereas there were no inclusion criteria relating to intelligence for study 305. Therefore, there were more patients with a medical history indicative of intellectual and developmental disability (IDD) in study 305 (placebo, 38%; ESL, 31%) than in study 208 (no patients in study 208 had IDD). Children with IDD may be more susceptible to medication intolerance than children without IDD, because of potential differences in metabolism and comorbidities resulting in different PKs and pharmacodynamics. 16 Indeed, approximately half (8/17) of patients who had a SAE in the ESL group of study 305 had a medical history indicative of IDD. In addition, patients taking ESL in study 305 were taking more baseline AEDs than those taking ESL in study 208 (2 baseline AEDs: 75% vs 47%, respectively), and had a longer duration of treatment with ESL (median: 147 vs 112 days, a 5-week difference), increasing the risk of drug-drug interactions. Furthermore, patients in study 305 had a higher baseline seizure frequency (mean [SD]: 54 [134] vs 14 [24]) than those in study 208, potentially suggesting greater disease severity.
We specifically evaluated the incidence of TEAEs of special interest when using AEDs in general, or ESL in particular. We found that TEAEs related to allergic reaction, hyponatremia, hypothyroidism, cytopenia, seizure exacerbation, cognitive dysfunction, psychiatric disorders, and suicide occurred infrequently in these trials. Indeed, TEAEs related to seizure exacerbation and cognitive dysfunction were primarily reported in study 305, potentially due to the differences between studies discussed above.
A potential limitation of the current analysis is that, due to FDA guidance with regards to extrapolation of efficacy from adults to children, 17 only patients aged 4 to 17 years were included. Study 305 included patients aged <4 years, and so 24 patients were removed from the full study data set prior to analysis.
It is also of note that the ESL dosing in these clinical trials is different from the body weight–based dosing recommended in the ESL Prescribing Information in the USA. 18 The weight-based dosing was calculated using PK modeling to extrapolate effective exposures in adults to children, with the assumption that the relationship between weight and exposure is nonlinear, because of the nonlinear ontogeny of metabolic pathways. 19
Conclusions
Overall, ESL was well tolerated in children aged 4 to 17 years with focal seizures. The safety profile in these patients was comparable to that in adults (≥18 years) with focal seizures, 2 with no new safety concerns.
Footnotes
Authors’ Note
Acknowledgments
Medical writing support was provided by Mallory Gough, PhD, ISMPP CMPP™ of FireKite, an Ashfield company, part of UDG Healthcare plc, and was funded by Sunovion Pharmaceuticals Inc.
Author Contributions
DC, DB, MM, PEM, and TG contributed to the conception and design of the manuscript. SMW contributed to the conception of the manuscript. DC, JM, PEM, and RC contributed to the acquisition, analysis, and interpretation of the data. SJ contributed to the acquisition and interpretation of the data. DB, MM, JEPG, SMW, RC, TG, and YL contributed to the analysis and interpretation of the data. DB, MM, JEPG, and SJ contributed to the drafting of the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content and final approval.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MM serves on the editorial boards of the Journal of Child Neurology and Vision Development and Rehabilitation; has functioned as Principal Investigator for clinical trials research contracted through the Clinical Research Center of New Jersey (CRCNJ) sponsored by the following companies: Aquestive Therapeutics, Curemark, Eisai Inc., Impax Laboratories, Neurim Pharmaceuticals, Nuvelution Pharma Inc, PhenoSolve, Sunovion Pharmaceuticals Inc, and Teva; is consultant to Philips-Electrical Geodesics contracted through The Center for Neurological and Neurodevelopmental Health (CNNH NeuroHealth); is on the scientific advisory board of NeuroNeeds; is Chief Medical Officer, owner and founder of CNNH and CRCNJ; is a board member of CNNH Management, Inc; is President and Founder of NeurAbilities, a 501(3)c public charity; and has functioned as an expert witness in various litigation and mitigation cases, contracted through CNNH NeuroHealth. JEPG reports being on an advisory council or committee for, and receiving honoraria and consulting fees from Sunovion Pharmaceuticals Inc, Eisai, Aquestive, Greenwich, UCB, and Supernus. SMW reports receiving consulting fees from Lundbeck, Sunovion Pharmaceuticals Inc, Eisai, BioMarin, and NeuroPace. PEM reports receiving honoraria from Sunovion Pharmaceuticals Inc, Greenwich, Eisai, and LivaNova. SJ has no conflicts of interest to report. TG, DC, YL, and DB report employment with Sunovion Pharmaceuticals Inc. RC and JM report employment with BIAL–Portela & C
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Studies 208 and 305 were funded by BIAL–Portela & C
Ethical Approval
The study protocols were approved by the relevant independent ethics committees/institutional review boards, and all patients provided written informed consent.