
Abstract
Varicella vaccination is now virtually universal in North America, as well as in some European and Asian countries. Since varicella vaccine is a live attenuated virus, the virus replicates in the skin after administration and can travel via sensory nerves or viremia to become latent in the dorsal root ganglia. In some immunized children, virus reactivates within a few months to a few years to cause the dermatomal exanthem known as herpes zoster (shingles). Herpes zoster caused by vaccine virus often reactivates within the same dermatome as the site of the original varicella vaccine injection. We present evidence that occasional cases of herpes zoster following varicella vaccination in immunocompetent children can be as severe as herpes zoster following wild-type varicella. Analysis of the virus in one case disclosed that the vaccine virus causing herpes zoster was a wild-type variant with a mutation in ORF0. With regard to dermatomal localization of the viral eruption, we predict that herpes zoster of the lumbar dermatomes in children is likely to be caused by vaccine virus, because herpes zoster in those dermatomes is rare in children after wild-type varicella. One of the children with herpes zoster subsequently developed asthma, a known risk factor for herpes zoster, but none of the children had an autoimmune disease. Although postherpetic neuralgia is exceedingly rare, children who develop herpes zoster following varicella vaccination are at risk (albeit low) of developing meningoencephalitis and should be carefully observed for a few weeks.
Keywords
Live attenuated varicella vaccine virus is administered to most children in North America as well as to many children in Europe and Asia. 1 –3 The vaccine was attenuated by Takahashi and colleagues in Osaka in the 1970s by traditional serial passage in cultured cells. 4 The vaccine was first tested in large clinical trials and subsequently approved by the Food and Drug Administration in 1995. The vaccination program in the USA has been highly successful and varicella has been virtually eliminated as a common childhood disease. However, the fact is sometimes overlooked that the varicella vaccine is a live attenuated virus. Therefore, some immunized children will acquire a latent vaccine virus infection in their dorsal root ganglia. This latent virus can reactivate and cause herpes zoster during childhood or beyond.
Clinical observations over the past 25 years in the USA have led to the conclusion that the frequency and severity of herpes zoster after varicella vaccination are less than those induced by wild-type varicella infection. 5,6 Nevertheless, reports are accruing that herpes zoster does occur after varicella vaccination in immunocompetent children. 7 Furthermore, some of these children have developed meningoencephalitis. 8 Herein, we present 3 cases of severe herpes zoster following varicella vaccination in immunocompetent children and provide an overview of related neurologic complications. 9
Methods
VZV serology for measurement of IgM and IgG antibodies was performed by the fluorescent antibody to membrane antigen assay. 10 VZV sequencing was performed on DNA extracted from cells adherent to the swap, by methods known to this virology laboratory. 11 –13 A swab was collected by abrading skin vesicles; this sample was pelleted by centrifugation at high speed and then resuspended in buffered saline with Proteinase K (Qiagen, 1014023) for 30 minutes at ambient temperature. Total DNA was then extracted from the sample using the DNeasy kit (Qiagen, 69504) and yielded 3.6 ng/μL. Two sections (the first 1500 bases including ORFs 0 and 1; 2000 bases of ORF62) of the viral genome were then PCR amplified using previously described primers and the Expand Hi Fidelity DNA polymerase (Roche Diagnostics, 11732641001). The PCR amplicons were then sequenced by Sanger methodology. The generated sequences were then aligned to the VZV reference sequence (Dumas, GenBank X04370.1) to provide a consensus sequence using a locally written computer program. Differences between the consensus sequence and the VZV reference were then generated with the EMBOSS program diffseq to yield the differences summarized in Table 1 and Figure 1.
Confirmation That the Infecting Virus Was Vaccine Virus.a
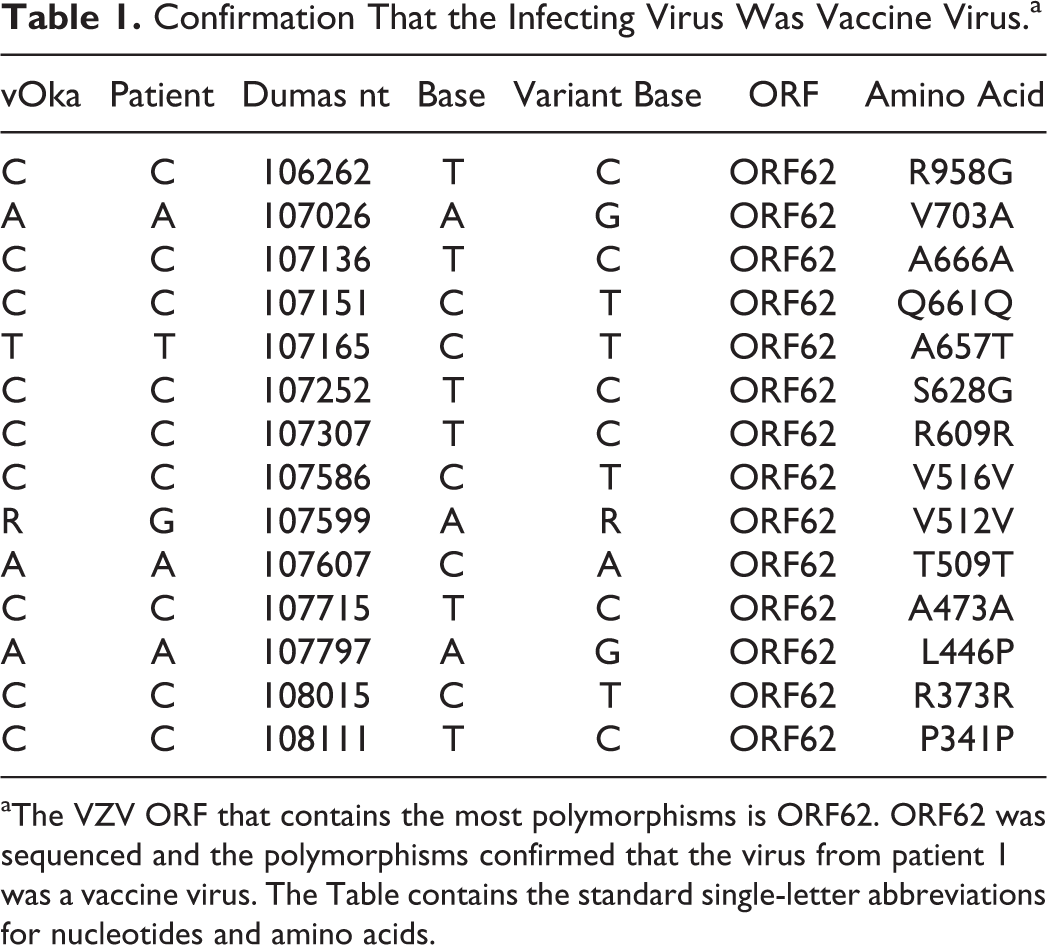
aThe VZV ORF that contains the most polymorphisms is ORF62. ORF62 was sequenced and the polymorphisms confirmed that the virus from patient 1 was a vaccine virus. The Table contains the standard single-letter abbreviations for nucleotides and amino acids.
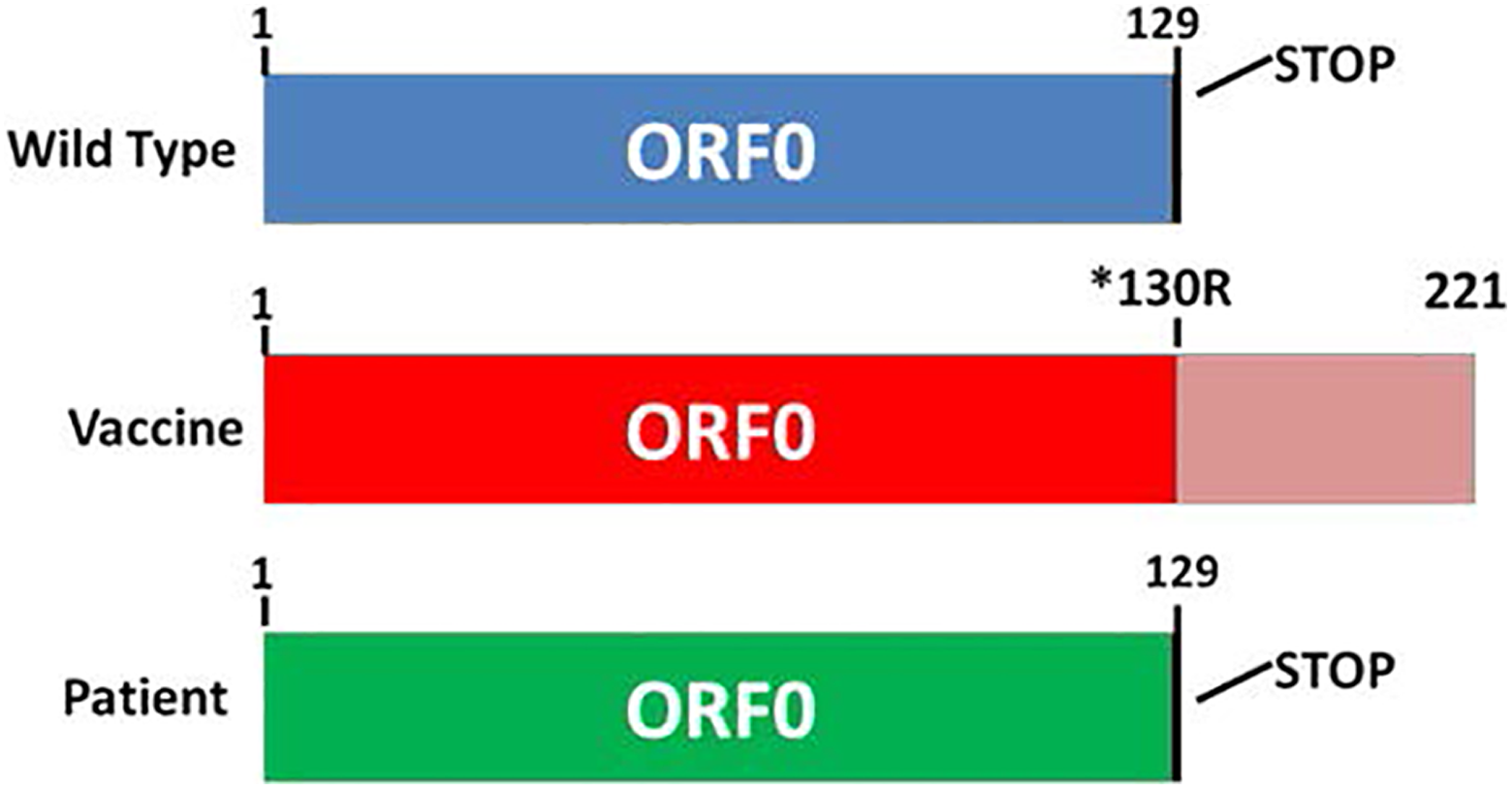
Identification of an ORF0 mutation in the vaccine virus of patient 1. The structure of ORF0 in wild-type virus is shown in blue; there is a stop codon after residue 129. The structure of ORF0 in the vaccine virus is shown in red; a nucleotide transition (TGA to CGA) after residue 129 replaces the stop codon with an arginine at residue 130. The ORF0 protein product is longer. When ORF0 was sequenced from the vaccine virus recovered from patient 1, there was a stop codon after residue 129, as shown in green.
Results
Overview
The birth cohort in Iowa is just under 40,000 annually. More than 95% of children in Iowa receive the immunizations scheduled at 1 year of age, including varicella vaccine. There have not been community outbreaks of wild-type varicella in the past decade. The 2 children’s hospitals in Iowa have the only pediatric infectious disease and neurology specialists. Therefore, their specialists receive telephone consultations about most severe complications of vaccinations, and occasionally see the children as outpatients or inpatients. The 3 cases described below were seen over a period of 3 years by these specialists.
Illustrative Cases
Child 1 was 20 months old when he received varicella vaccine in his right upper arm. At age 3 years 3 months, he came to the emergency department because of lower back pain and a new rash of 3 days’ duration. The rash consisted of around 25 vesicles located to the left of the spine along dermatomes L4-S1, with a few vesicles on the left leg. He complained of pain and itchiness at the rash site, and was reluctant to walk in the emergency department. He had experienced no changes in bowel or bladder function. After admission, a neurologic examination revealed no deficits, but did reveal allodynia to light touch in the distribution of rash. He had full strength in all limbs, no apparent sensory deficits, and normal muscle stretch reflexes. Because a screening PCR test of the rash was positive for VZV, he was treated with acyclovir suspension for 10 days. His rash and other symptoms slowly resolved with no further complaints. The child had never had wild-type varicella nor had he been exposed to family members with herpes zoster. In follow-up, the child developed signs of asthma, but no evidence of autoimmune diseases or neuralgia.
Child 2 and child 3 were siblings. Child 2 was 13 months old when he was immunized in the right thigh with varicella vaccine. He was symptom free until he developed a rash 7 months later. The rash was beefy red, vesicular, and localized to his right thigh and lower back, mainly along dermatome L3. He was examined twice in the outpatient clinic. No neurologic deficits were apparent either time. The exanthem worsened for 1 week, then slowly cleared over the following 2 weeks. The inflamed skin appeared to be painful, since the child avoided sleeping on that side. He was not admitted to the hospital nor was he treated with acyclovir. Child 3 was an older sibling of child 2. When child 2 was seen in clinic, the physician and nurse recalled that both of them has seen an older sibling with a similar severe rash following varicella vaccination. They reviewed their medical records and confirmed that child 3 had varicella vaccination in the right thigh 2 days after his first birthday. He developed herpes zoster over the right thigh at age 3.5 years. The mother was interviewed again about child 3, and she confirmed that the rash was similar in size and location as with child 2. No laboratory studies were performed on case 3. Neither child 2 nor 3 had ever had wild-type varicella nor had they been exposed to family members with herpes zoster. In follow-up, neither child had evidence of asthma, neuralgia, or autoimmune disease.
Analysis of the Virus From Case 1
A swab of a vesicle was obtained for further VZV analyses, because of the initial severity of symptoms. We first demonstrated that the virus was the Oka vaccine strain by sequencing nearly 2000 bases of the VZV open reading frame (ORF)62 gene. 14 The patient’s VZV DNA was different from wild-type VZV at nine bases (Table 1), indicating that the patient’s VZV strain was the VZV vaccine strain. Because of our interest in ORF0 as a possible determinant of attenuation, we next sequenced the first 1500 bases of the VZV genome and detected an important difference from the vaccine virus within ORF0 at base 560, namely, a wild-type allele rather than a vaccine-type allele (Figure 1).
Severity of the Exanthem in Cases 2 and 3
The literature implies that rashes associated with herpes zoster following varicella vaccination are much less severe than rashes seen after reactivation of wildtype varicella. The rash in this child was an exception to that impression. The rash covered most of dermatome L3 and occurred at precisely the site of the earlier vaccination. The site of vaccination is indicated by a white circle in Figure 2. The rash on patient 2 was even more extensive than the rash on patient 1. Because of the severity of his rash, we performed serology studies to measure VZV antibody; he was positive for both IgM (>1:64) and IgG (>1:256) by the fluorescent antibody to antigen assay, which is considered to be the most sensitive VZV antibody assay. As noted by the mother of cases 2 and 3 and verified in the medical records, the rash of case 3 was very similar to the rash of case 2.

Dermatomal rash of herpes zoster in patient 2. The rash was broadly distributed over the L3 dermatome on the anterior aspect of the right thigh (A); the location of the original varicella vaccine injection 9 months earlier is indicated by a white circle. The rash lessened as it extended around the flank and toward the spinal column (B).
Discussion
The 3 cases in this report document that immunocompetent children can develop herpes zoster following varicella vaccination. The cases further demonstrate that the zoster rash can be as severe as that following wild-type varicella (chicken pox), and that the zoster rash can emerge in the same dermatome in which the vaccine was injected or at a remote location.
Herpes zoster has been linked to dermatome mapping since the classic 170-page article by Head and Campbell in 1900, called the pathology of herpes zoster and its bearing on sensory localization. 15 The natural history of herpes zoster in patient 2 is a similar example of the technique used by Head and Campbell to map dermatomes more than a century ago; specifically, since the site of the vaccine virus injection is known and the rash can be traced to the region of L3 along the spine, one can map the region of the thigh (dermatome) innervated by L3 (Figure 2). In this case, the vaccine virus replicated in the subcutaneous tissue of the thigh after immunization, then entered the sensory nerves and traveled to the L3 dorsal root ganglion, from which the virus subsequently reactivated and caused the rash mapping to the L3 dermatome. By reviewing prior reports of herpes zoster in children, we also conclude that herpes zoster in the lumbar dermatomes is so rare following wild-type varicella that, when it occurs in children, it is likely an indicator of herpes zoster secondary to vaccine virus. 16,17
On the other hand, the medical history with patient 1 is equally important and implies a different mechanism of viral spread, because the zoster localization (left thigh) was very distant from the vaccine injection site (left arm). The most likely explanation for this situation is that a viremia occurred following administration of the varicella vaccine, which carried the virus to distant neuronal locations. 18 Indeed, a small but thorough prospective analysis of children immunized with their first varicella vaccine demonstrated a viremia in 50% of the recipients. 19 Case 1 is also important because a review of his medical history after herpes zoster included visits for treatment of asthma. Several epidemiology studies of both children and adults have documented an increased risk of herpes zoster in subjects with a medical history of asthma. 20 –23 Although asthma was not evident when case 1 was admitted for severe herpes zoster, we propose that his subsequent development of asthma indicated that he was a child at higher risk of developing herpes zoster.
Further, the virology studies from patient 1 were revealing because they showed that a wild-type variant of the vaccine virus may be more virulent. The commercia
As our 3 cases emphasize, herpes zoster induced by varicella vaccination usually occurs within months to a few years after the vaccination in immunocompetent children. Another neurologic complication of zoster, meningoencephalitis, occurs within 1-2 weeks of onset of herpes zoster. We point out 2 reported cases of meningoencephalitis caused by wild-type VZV reactivation in immunocompetent children and young adults, in which the patients had varicella in childhood but never has a zosteriform rash prior to their central nervous system disease. 13,28 Their correct diagnosis required testing with every available individual bacterial, viral, and fungal diagnostic kit. Undoubtedly, there are similar cases of herpes zoster without rash following varicella vaccination that are leading to undiagnosed meningoencephalitis caused by vaccine virus in children. 29 Therefore, we recommend increased use of the newly available multivalent Biofire Filmarray multiplex PCR system to screen cerebrospinal fluids from immunocompetent children with new-onset encephalitis for multiple pathogens. 30
Footnotes
Author Contributions
All authors reviewed the medical records and contributed inputs to the manuscript. CG and DJB wrote the final manuscript and prepared the figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research by Dr Grose and Dr Bonthius is funded by the NIH Grants AI89716 and HL126667.
Ethical Approval
This study was approved by the University of Iowa Institutional Review Board, Iowa City, IA, USA.