
Abstract
The authors hypothesized that the risk of cerebral palsy at 2 years in children born extremely preterm to overweight and obese women is increased relative to the risk among children born to neither overweight nor obese women. In a multicenter prospective cohort study, the authors created multinomial logistic regression models of the risk of diparetic, quadriparetic, and hemiparetic cerebral palsy that included the prepregnancy body mass index of mothers of 1014 children born extremely preterm, cerebral palsy diagnoses of children at 2 years, as well as information about potential confounders. Overweight and obese women were not at increased risk of giving birth to a child who had cerebral palsy. The risk ratios associated with overweight varied between 1.1 for quadriparesis (95% CI = 0.5, 2.1) to 2.0 for hemiparesis (95% CI = 0.4, 9.8). The risk ratios associated with obesity varied between 0.7 for diparesis (95% CI = 0.2, 2.5) to 2.5 for hemiparesis (95% CI = 0.4, 13).
The risk of cerebral palsy, one of the most common causes of chronic disability in children, 1,2 increases with decreasing gestational age. 3 Despite the improvements in perinatal care in recent decades, the prevalence of cerebral palsy has not declined. 4 –6 This observation suggests that prenatal factors, including maternal conditions, contribute more to the onset/occurrence of cerebral palsy than do postnatal exposures.
The prevalence of obesity among gravidas increased during the past decades, with the latest figures showing that more than one-third of women entering pregnancy in the United States were identified as obese before pregnancy. 7 Overweight and obesity before pregnancy appear to be associated with such antenatal and intrapartum complications as gestational diabetes, preeclampsia, hypertension, and labor and delivery difficulties. 8,9 The mother’s obesity also appears to have adverse effects on her offspring 10 such as increased risk for cognitive deficits, 11,12 behavioral disabilities, 13,14 and cerebral palsy. 15 –19
Most studies linking maternal obesity to a child’s risk of cerebral palsy have been mainly of term-born children. To the authors’ knowledge, no report has assessed the relationship between high maternal prepregnancy body mass index and cerebral palsy among children born extremely preterm. The multicenter ELGAN (Extremely Low Gestational Age Newborn) Study, with its uniform and highly reliable assessments of cerebral palsy, provided an opportunity to correct this deficiency.
The different types of cerebral palsy will be investigated separately because the neuropathology underlying these types may differ from each other in children born extremely preterm. 20 –23 The risk factors and antecedents of the different types of cerebral palsy may therefore vary on the basis of differences in pathophysiology that are associated with these cerebral lesions.
Methods
Sample
The ELGAN study, a prospective cohort study designed to identify characteristics and exposures that increase the risk of structural and functional neurologic disorders, enrolled 1506 extremely low gestational age newborns (birth between 23 and 27 6/7 weeks of gestation) at 14 participating institutions between 2002 and 2004. 24 Institutional review boards of the participating institutions approved the enrollment and consent processes. Mothers were approached for consent either upon antenatal admission or shortly after delivery, depending on clinical circumstance and institutional preference. A total of 1249 mothers of 1506 infants consented. Approximately 260 women were either missed or did not consent to participate. Of the 1205 infants who survived to age 2, 1056 (88%) had a neurologic examination at approximately 24-months corrected age. Fully 1014 children had complete information on variables of interest and are the subjects of the analyses.
Demographic and Pregnancy Variables
In the entire ELGAN Study sample, both maternal obesity and cerebral palsy varied with gestational age at delivery. 25 –27 In early sets of analyses, the authors adjusted for gestational age in 2 ways, both by weeks of gestation (23, 24, 25, 26, 27) and by groups of weeks (23-24, 25-26, 27). Each provided almost identical results. Here the authors present data adjusted for gestational age in groups of weeks.
After delivery, a trained research nurse interviewed each mother in her native language using a structured data collection and following procedures contained in a manual. The mother’s report of her own characteristics and exposures, as well as the sequence of events leading to preterm delivery was taken as truth, even when her medical record provided discrepant information. Shortly after the mother’s discharge, the research nurse reviewed the maternal chart using a second structured data collection form. The medical record was relied on for events following admission.
Maternal Body Mass Index
Each mother was asked to provide her height and her prepregnancy weight shortly before, or shortly after delivery when she was interviewed, usually by a research nurse. These data were used to calculate her body mass index. The US government classifies body mass indexes as follows: <18.5 is underweight, 18.5–24.9 is normal, 25.0–29.9 is overweight, 30.0–34.9 is obese, 35.0–39.9 is very obese, and ≥40 is extreme obesity. 28 The authors collapsed these groups into <25, 25-29.9, and ≥30.
Pregnancy Disorders
The clinical circumstances that led to each maternal admission and ultimately to each preterm delivery were operationally defined using both data from the maternal interview and data abstracted from the medical record. 29 The authors were interested in the potential preconditioning/sensitization by antenatal inflammation. Therefore, the authors divided the sample into 2 groups defined by spontaneous indications for delivery (preterm labor, preterm premature rupture of membranes, abruption, or cervical insufficiency) versus maternal (preeclampsia) or fetal indications. The rationale for this was that spontaneous indications are often associated with inflammation, while fetal and maternal indications are mostly not. 30,31
Infant Characteristics
Gestational age estimates were based on a hierarchy of the quality of available information with estimates based on the dates of embryo retrieval or intrauterine insemination or fetal ultrasound before the 14th week of gestation (62%) as the most desirable. Next most desirable in sequential order were estimates based on a fetal ultrasound at 14 or more weeks of gestation (29%), last menstrual period without fetal ultrasound (7%), and recorded in the log of the neonatal intensive care unit.
The birth weight Z-score represents the number of standard deviations the infant’s birth weight was above or below the median weight of infants at the same gestational age in referent samples not delivered for preeclampsia or fetal indications. 32,33 The authors evaluated 2 groups of growth-restricted infants. The more severely growth-restricted infants had a birth weight Z-score <–2 (ie, more than 2 standard deviations below the median of the referent group). Infants in the less severely growth-restricted group had a birth weight Z-score ≥–2 and <–1 (ie, between 1 and 2 standard deviations below the median of the referent group).
The head circumference was measured as the largest possible occipital-frontal circumference. Measurements were rounded to the closest 0.1-centimeter when taken at birth, and when examined at 24-month corrected age. All head circumferences are presented as Z-scores because newborns were assessed at different gestational ages at birth (23-27 weeks) and at different approximations of 24 months corrected age (range: 16-44 months corrected age, with 68% assessed at 23-25 weeks corrected age). Z-scores were based on standards in the CDC data sets. 34
24-Month Developmental Assessment
Families were invited to bring their child for a developmental assessment close to the time when s/he would be 24-months corrected age for evaluation of a neurological examination. Fully 91% of children returned for the developmental assessment. Of these children, 75% had their exam within the range of 23.5-27.9 months, 14% were assessed before 23.5 months, and 12% were assessed after 27.9 months.
Cerebral Palsy Diagnosis
To standardize neurological examinations at all sites, a stand-alone, multimedia-training video/CD-ROM was developed, based on elements of a standard neurological exam. 35 The video/CD-ROM program had audiovisual teaching sequences, voice-over commentary, graphics and text to organize the training and amplify key teaching points. The training video provided instruction in the proper method of performing each item of the examination and illustrated all possible findings. In addition, the CD contained 6 sets of 20 video clips for interobserver testing purposes. Repeated testing resulted in 96% agreement with the gold-standard pediatric neurologist assessment.
Those who performed the neurological examinations studied a manual, a data collection form and an instructional CD designed to minimize examiner variability, and demonstrated acceptably low variability. 35 The topographic diagnosis of cerebral palsy (quadriparesis, diparesis, or hemiparesis) was based on an algorithm using these data. 23 Only 4% of examiners indicated at the time of the examination that they had knowledge of the child’s brain-imaging studies.
Statistical Analyses
The authors tested the null hypothesis that newborns of overweight (ie, body mass index > 25, < 30) and obese women (ie, body mass index ≥ 30) are not at risk of a specific topographic cerebral palsy diagnosis (ie, quadriparesis, diparesis, or hemiparesis).
The authors began the analyses by searching for potential confounders (ie, characteristics that varied with body mass index and the subtypes of cerebral palsy) (Tables 1 –5). Based on the findings in these tables the authors selected as potential confounders, mother-identified race, male sex, mother’s level of education, time since last pregnancy, any aerobe in the placenta, chorionic plate inflammation of the placenta, and preeclampsia. If a perceptible difference among adjacent categories was seen, then that variable became a candidate to see if it modifies the body mass index–cerebral palsy relationship.
The Percentage of Children Who Had the Characteristic at the Top of the Column Who Also Had the Characteristic Listed on the Left.
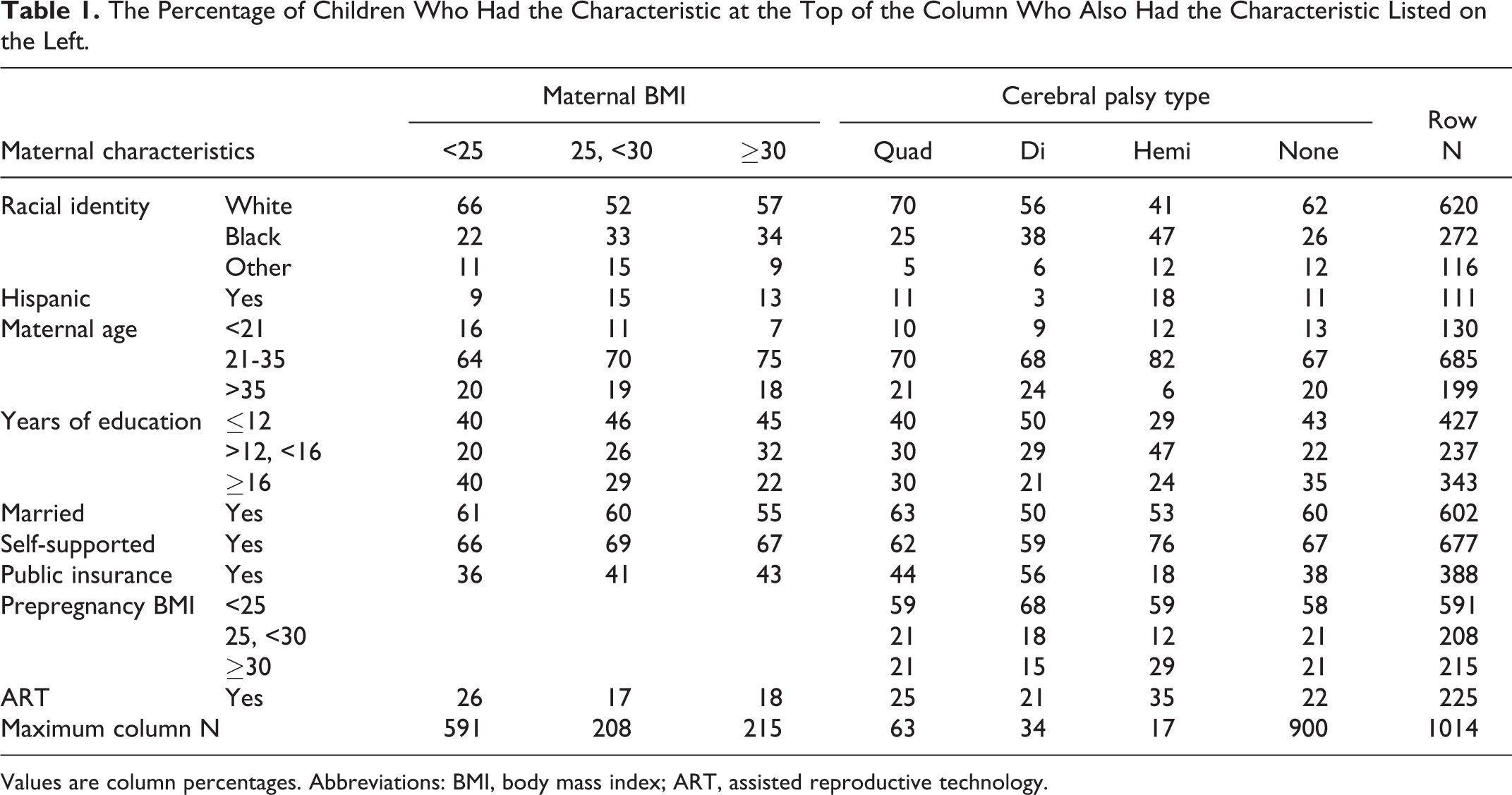
Values are column percentages. Abbreviations: BMI, body mass index; ART, assisted reproductive technology.
The Percentage of Children Who Had the Characteristic at the Top of the Column Who Also Had the Pregnancy Characteristic Listed on the Left.
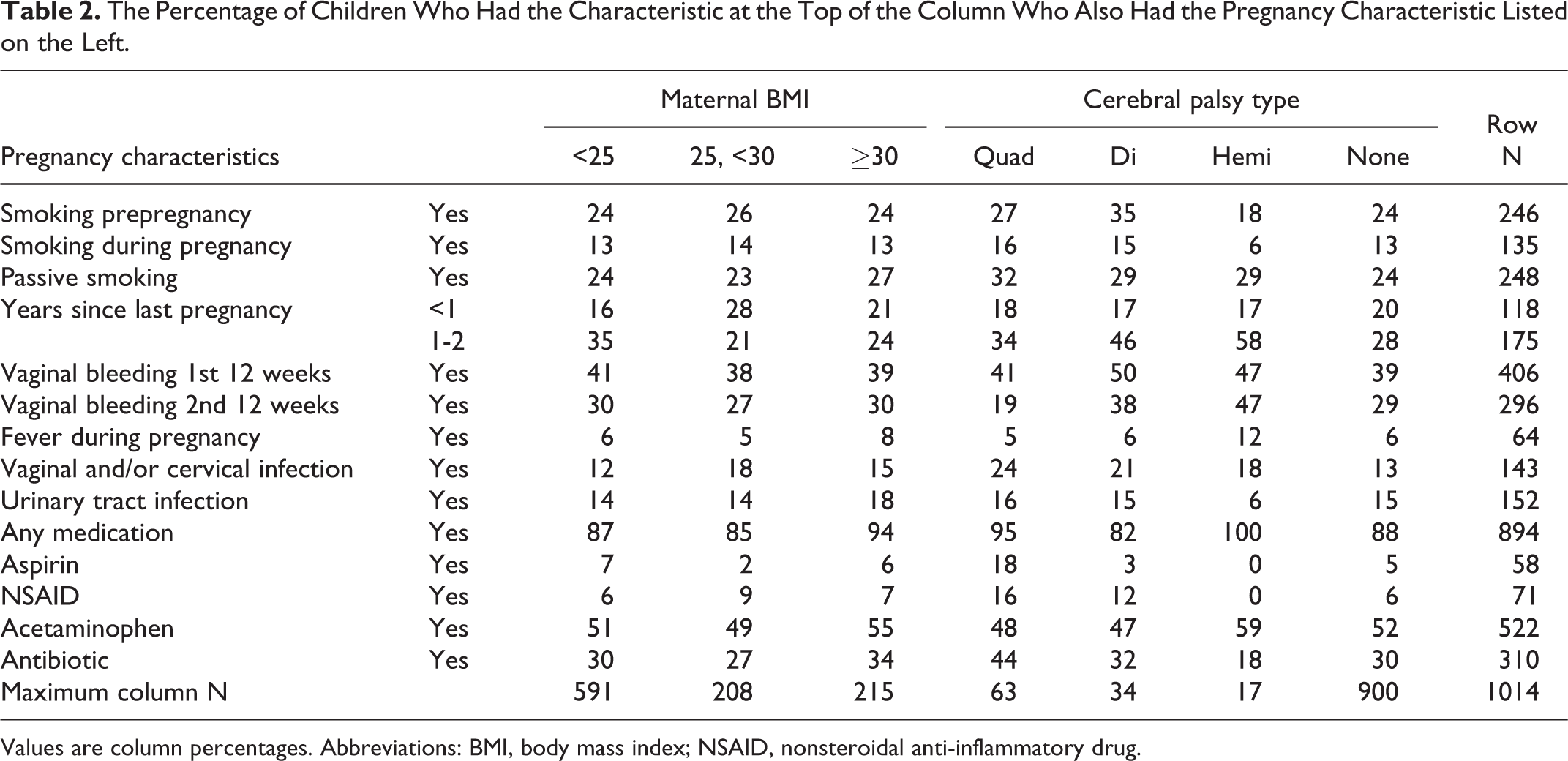
Values are column percentages. Abbreviations: BMI, body mass index; NSAID, nonsteroidal anti-inflammatory drug.
The Percentage of Children Who Had the Characteristic at the Top of the Column Whose Placenta Had the Bacteriologic or Histologic Characteristic Listed on the Left.
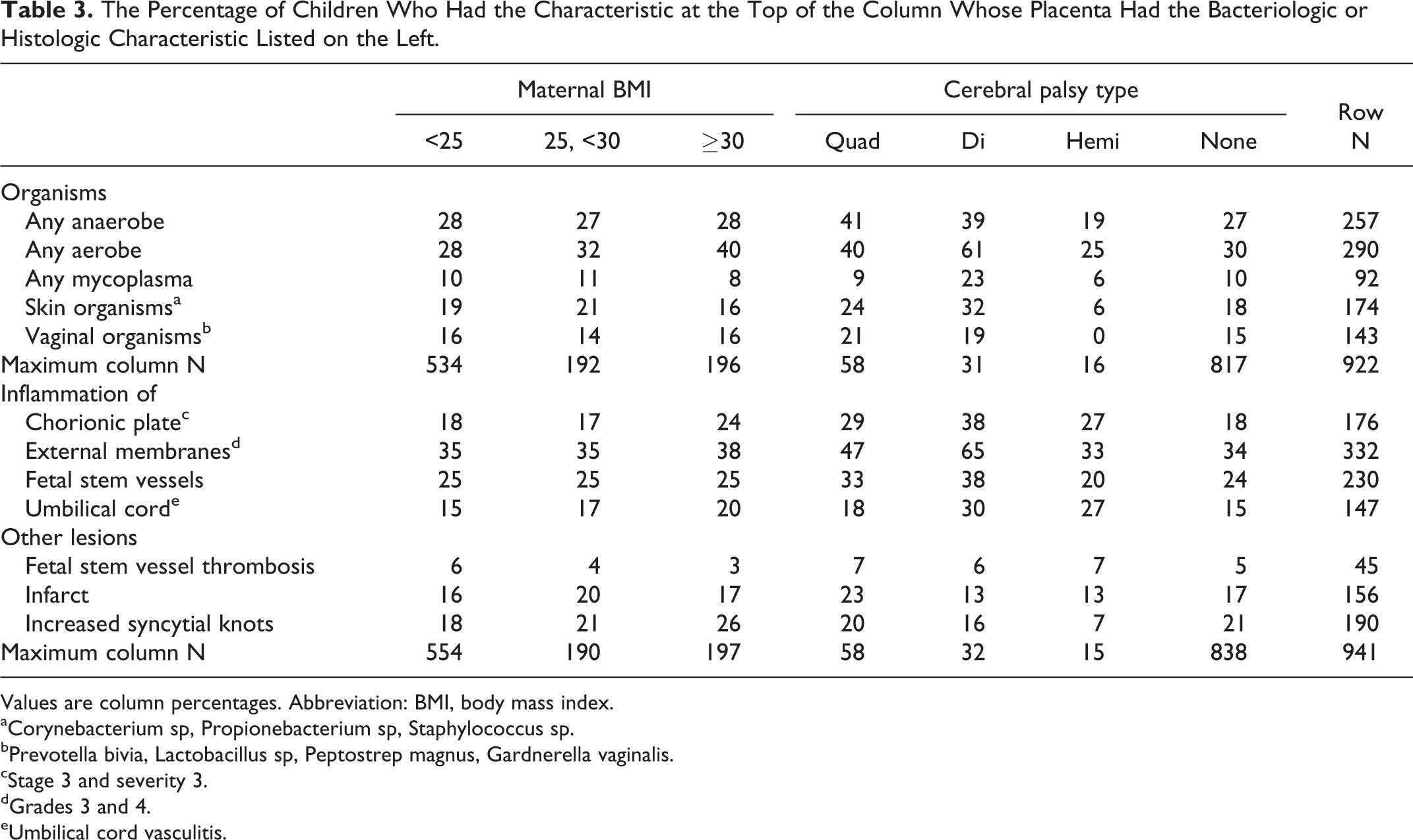
Values are column percentages. Abbreviation: BMI, body mass index.
aCorynebacterium sp, Propionebacterium sp, Staphylococcus sp.
bPrevotella bivia, Lactobacillus sp, Peptostrep magnus, Gardnerella vaginalis.
cStage 3 and severity 3.
dGrades 3 and 4.
eUmbilical cord vasculitis.
The Percentage of Children Who Had the Characteristic at the Top of the Column Who Also Had the Delivery Characteristic Listed on the Left.
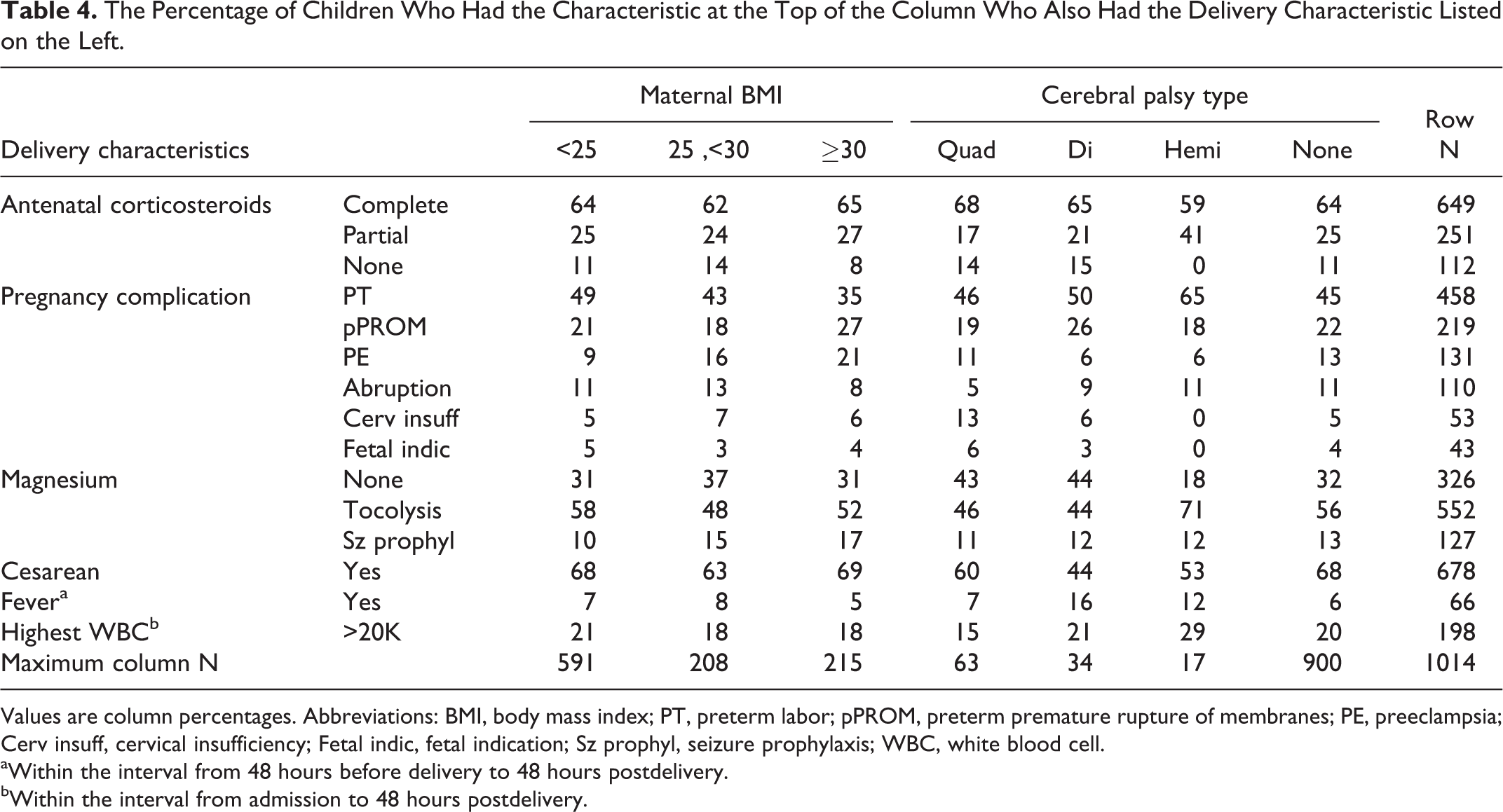
Values are column percentages. Abbreviations: BMI, body mass index; PT, preterm labor; pPROM, preterm premature rupture of membranes; PE, preeclampsia; Cerv insuff, cervical insufficiency; Fetal indic, fetal indication; Sz prophyl, seizure prophylaxis; WBC, white blood cell.
aWithin the interval from 48 hours before delivery to 48 hours postdelivery.
bWithin the interval from admission to 48 hours postdelivery.
The Percentage of Children Who Had the Characteristic at the Top of the Column Who Also Had the Characteristic Listed on the Left.
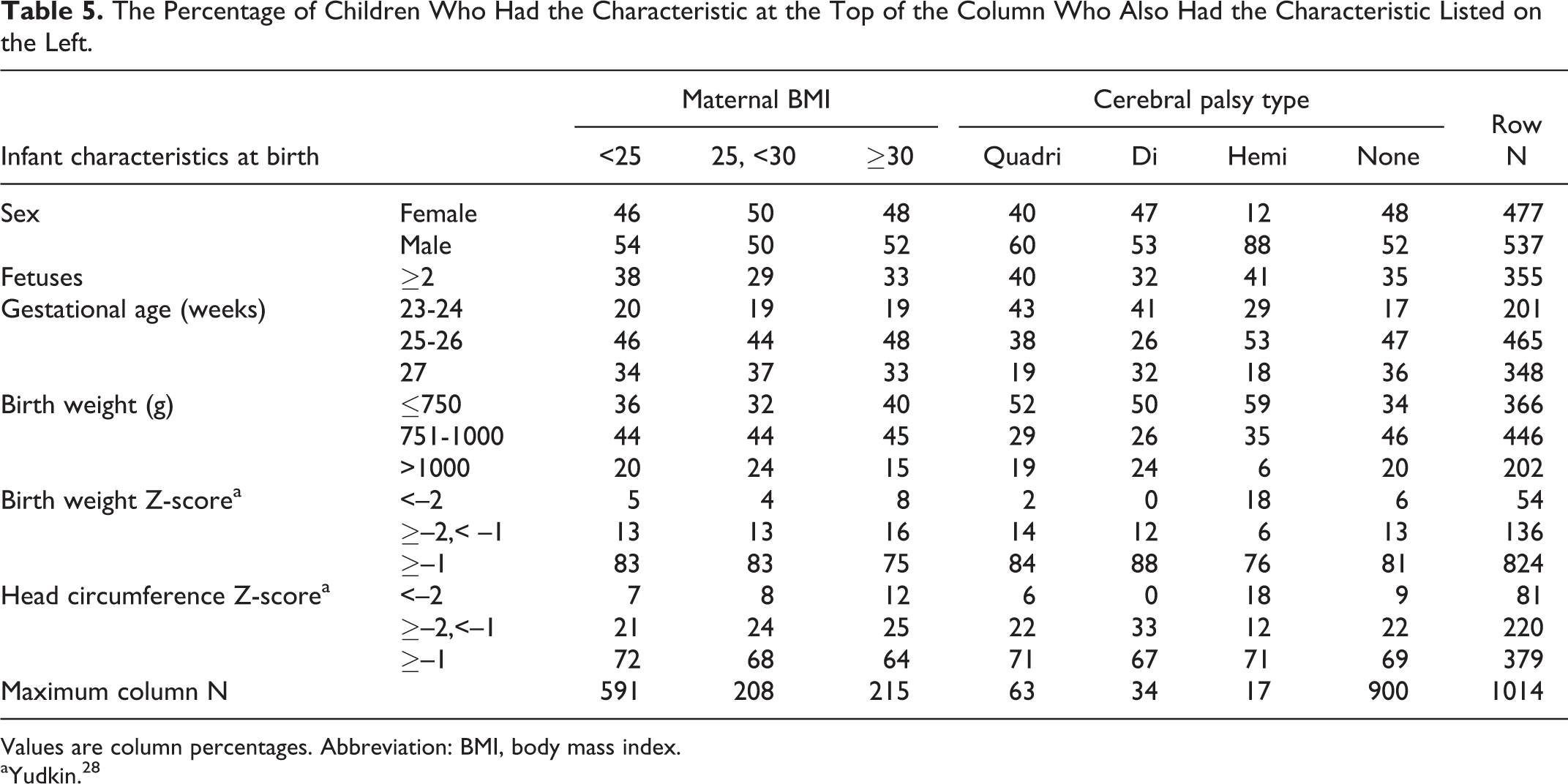
Values are column percentages. Abbreviation: BMI, body mass index.
aYudkin. 28
Then the authors created multivariable models to identify the contribution of maternal overweight and obesity to the risk of cerebral palsy in light of potential confounders (Table 6). The authors created logistic these regression models using a step down procedure seeking a parsimonious solution without interaction terms. The contributions of relevant variables, including maternal overweight and obesity, are presented as risk ratios with 95% confidence intervals. The authors performed 2 additional analyses to look for possible effect modification by maternal or fetal indications. First they restricted the analyses to children who were born after maternal or fetal indications and then to those born after C-section, a proxy for maternal or fetal indications. No effect modification was found, as both analyses did not show an increased risk for cerebral palsy for infants born to mothers who were obese.
Risk Ratios (Point Estimates and 95% Confidence Intervals) for the Cerebral Palsy Form at the Top of the Column Associated With the Risk Factors Listed on the Left.
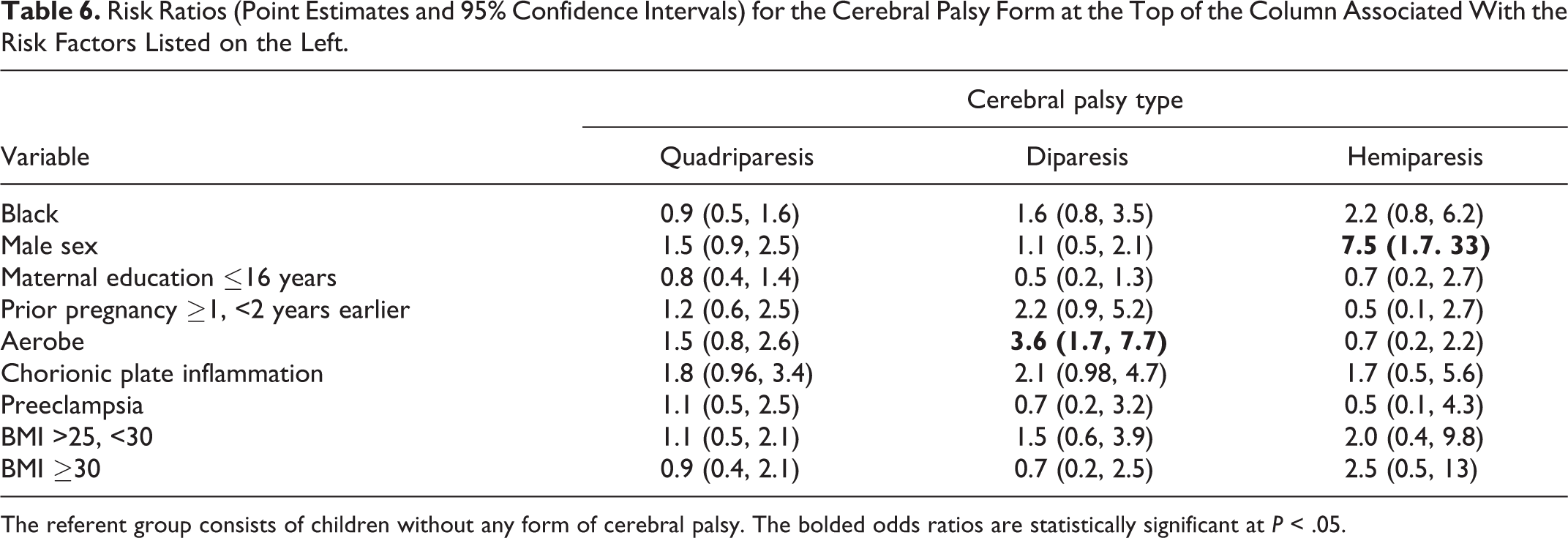
The referent group consists of children without any form of cerebral palsy. The bolded odds ratios are statistically significant at P < .05.
Results
Sample Description
A total of 105 children from 1014 children were given a cerebral palsy diagnosis, with 52% quadriparetic, 30% diparetic, and 17% hemiparetic.
Demographic Characteristics (Table 1)
Overweight and obese women were more likely than others to have characteristics that are viewed as correlates of lower social class, including self-identifying as black, not graduating from college, being eligible for government-provided medical care insurance, and not having access to, or using assisted reproduction techniques. Children who had diparesis were also more likely than others to have a mother with these characteristics.
Maternal Characteristics (Table 2)
Overweight and obese mothers were less likely than mothers with a normal weight to have had a pregnancy 1-2 years before. Compared to the mothers of children who did not develop cerebral palsy, the mothers of all children who had cerebral palsy were more likely to have been exposed to the tobacco smoke of others, had a prior pregnancy 1-2 years earlier, and a vaginal/cervical infection during this pregnancy, while the mothers of children who developed diparetic or hemiparetic cerebral palsy were also more likely to have had vaginal bleeding during the first 2 trimesters. Mothers of quadriparetic children were more likely have consumed aspirin and nonsteroidal anti-inflammatory drugs during this pregnancy, while mothers of diparetic children were more likely to have smoked before this pregnancy and mothers of hemiparetic children were less likely to have smoked during this pregnancy. Only a prior pregnancy 1-2 years earlier was therefore a potential confounder.
Bacteriologic and Histologic Placenta Characteristics (Table 3)
Obese mothers were more likely than others to have aerobic bacteria recovered from their placenta and to have had chorionic plate inflammation and increased numbers of syncytial knots in their placentas.
Compared to the placentas of children who did not develop cerebral palsy, the placentas of all children who developed cerebral palsy were more likely to have chorionic plate inflammation, while those of diparetic and quadriparetic children were more likely to harbor aerobic and anaerobic organisms, as well as normal skin flora. The diparetic and quadriparetic children were also more likely to have had inflammation of the external membranes and fetal stem vessels. The umbilical cords of diparetic and hemiparetic children were more likely to have vasculitis than the umbilical cords of others.
In light of these findings, recovery of an aerobe and chorionic plate inflammation were the 2 placenta characteristics that were potential confounders.
Delivery Characteristics (Table 4)
With increasing body mass index, mothers were more likely to have preeclampsia, and the preeclampsia correlate of receipt of magnesium for seizure prophylaxis, than mothers with lower body mass indexes. Children with hemiparesis were more likely than others to have a mother who presented in labor, received magnesium tocolysis, a correlate of preterm labor, and to have had leukocytosis very near the time of delivery. Children with any type of cerebral palsy were less likely than others to be born via cesarean section. No delivery characteristic appeared to be a potential confounder.
Infant Characteristics at Birth (Table 5)
Compared to children who did not develop cerebral palsy, those who did were more likely to be born before the 25th week of gestation and to have a birth weight ≤750 grams. Quadriparetic and hemiparetic children were most likely to be male, while only hemiparetic children were most likely to be growth restricted.
Multivariable Analyses (Table 6)
In the multinomial, multivariable model that simultaneously evaluated the risks of quadriparetic, diparetic, and hemiparetic cerebral palsy and included black race, male sex, maternal education equal or less than 16 years, 1-2 years since last pregnancy, chorionic plate inflammation, preeclampsia, and overweight and obesity, only male sex was associated with an increased risk of hemiparesis (OR = 7.5; 95% CI: 1.7-33). In addition, recovery of aerobic bacteria from the placenta was associated with an increased risk of diparesis (OR = 3.6; 95% CI: 1.7, 7.7). Overweight and obese women were not at increased risk of giving birth to a child who had cerebral palsy. The risk ratios associated with maternal overweight varied between 1.1 for quadriparesis (95% CI = 0.5, 2.1) to 2.0 for hemiparesis (95% CI = 0.4, 9.8), while the risk ratios associated with obesity varied between 0.7 for diparesis (95% CI = 0.2, 2.5) to 2.5 for hemiparesis (95% CI = 0.5, 13).
Discussion
The main finding is that compared to extremely preterm children of women with a normal prepregnancy body mass index, those born to overweight and obese women are not at increased risk of any form of cerebral palsy.
Previous Studies of Maternal Obesity and Cerebral Palsy
One study that evaluated the relationship between maternal obesity and cerebral palsy found that children of overweight and obese mothers had a 3.5-fold increased risk of cerebral palsy, 15 while another study reported that maternal obesity was associated with a 30% increased risk of having a child with cerebral palsy. 16 This risk was even higher among infants born to a morbidly obese mother. 16,19 Two studies found no association between maternal weight and cerebral palsy. 36,37
Potential Confounders and Risk of Cerebral Palsy
The authors included in their model of cerebral palsy risks associated with maternal prepregnancy overweight and obesity only those additional variables that appeared to be potential confounders. Thus, the analyses were not intended to identify all the variables associated with the risk of cerebral palsy. With that caveat, the authors discuss male sex associated with increased risk of hemiparetic cerebral palsy and recovery of aerobic bacteria from the placenta associated with diparetic cerebral palsy.
The finding that male sex was associated with increased risk of hemiparetic cerebral palsy is in keeping with other findings in this cohort, since boys appear to be at increased risk of multiple difficulties/dysfunctions. 38 The finding that the presence of aerobic bacteria recovered from the placenta was associated with increased risk of diparetic cerebral palsy is in keeping with the report that preterm infants (≤29 weeks GA) whose placenta harbored the aerobic bacterium E.coli were at increased risk of having cerebral palsy at age 5 years. 39 Histological chorioamnionitis is also associated with cerebral palsy in preterm neonates (<1500 gram). 40 In addition, E.coli-induced amnionitis leads to white matter damage in the fetal rabbit brain. 41
Immaturity/Vulnerability
The risk of cerebral palsy increases with decreasing gestational age 42 –44 and obese women are more likely than others to deliver very preterm. 45 For these reasons (and others below), the authors expected to find that infants of obese mothers are at increased risk of cerebral palsy. The authors’ failure to find this might reflect nothing more than the narrow range of the gestational ages they evaluated (23-27 weeks). Another possibility is that the immaturity/vulnerability information carried by the low gestational age variables is also conveyed by other variables in the model, such as histologic and bacteriologic indicators of intrauterine infection/inflammation.
Systemic Inflammation
In this cohort, extremely preterm children whose mother was obese were more likely than others to have systemic inflammation in the days following delivery. 46 Because early systemic inflammation has been associated with increased risk of cerebral palsy in this very cohort, 47 as well as others, 48,49 the authors again would have expected to find that the children of obese mothers were at increased risk. Here, too, correlates/indicators of inflammation (eg, recovery of aerobe from the placenta and inflammation of the placenta’s chorionic plate) might have diminished the opportunity to identify a maternal obesity-offspring cerebral palsy connection.
Strengths and Weaknesses
This study has several strengths. First, the authors collected the data prospectively in a manner that minimized examiner and cerebral palsy classification variability. Second, they selected infants based on gestational age, not birth weight, thereby minimizing the confounding that might be due to factors related to fetal growth restriction. 50 Third, the analytic strategy incorporated potential confounders that might account for why others have found that children of obese mothers are at increased risk of cerebral palsy and the current authors did not. Fourth, the authors standardized the assessment of cerebral palsy and subtypes of cerebral palsy 23 and minimized interobserver variability. 35
One limitation of the study is that the observational nature of the study does not allow us to draw causal inferences for what the authors have found. Indeed, with their attempts to reduce confounding, the authors might have diminished their opportunity to attribute to maternal prepregnancy overweight and obesity what could have been consequences of a high body mass index, including socioeconomic correlates of overweight and obesity (such as limited maternal education), and increased risk of preeclampsia. An additional limitation is the reliance on the mother’s report of her prepregnancy weight as women have a tendency to underreport their weight. 51
Footnotes
Acknowledgments
The authors wish to acknowledge their ELGAN study colleagues: Children’s Hospital, Boston, Massachusetts (Haim Bassan, Samantha Butler, Adré Duplessis, Cecil Hahn, Catherine Limperopoulos, Omar Khwaja, Janet S. Soul); Baystate Medical Center, Springfield, Massachusetts (Bhavesh Shah, Herbert Gilmore, Susan McQuiston); Beth Israel Deaconess Medical Center, Boston, Massachusetts (Camilia R. Martin); Brigham and Women’s Hospital, Boston, Massachusetts (Linda J. Van Marter); Massachusetts General Hospital, Boston, Massachusetts (Robert M. Insoft, Kalpathy Krishnamoorthy); Floating Hospital for Children at Tufts Medical Center, Boston, Massachusetts (Cynthia Cole, John M. Fiascone, Paige T. Church, Cecelia Keller, Karen J. Miller); U Mass Memorial Health Care, Worcester, Massachusetts (Francis Bednarek [deceased], Robin Adair, Richard Bream, Alice Miller, Albert Scheiner, Christy Stine); Yale University School of Medicine, New Haven, Connecticut (Richard Ehrenkranz, Nancy Close, Elaine Romano, Joanne Williams);Wake Forest University Baptist Medical Center and Forsyth Medical Center, Winston-Salem, North Carolina (Deborah Allred, Robert Dillard, Don Goldstein, Deborah Hiatt, Gail Hounshell, Ellen Waldrep, Lisa Washburn, Cherrie D. Welch); University Health Systems of Eastern Carolina, Greenville, North Carolina (Stephen C. Engelke, Sharon Buckwald, Rebecca Helms, Kathyrn Kerkering, Scott S. MacGilvray, Peter Resnik); North Carolina Children’s Hospital, Chapel Hill, North Carolina (Carl Bose, Lisa Bostic, Diane Marshall, Kristi Milowic, Janice Wereszczak); Helen DeVos Children’s Hospital, Grand Rapids, Michigan (Mariel Poortenga, Wendy Burdo-Hartman, Lynn Fagerman, Kim Lohr, Steve Pastyrnak, Dinah Sutton); Sparrow Hospital, Lansing, Michigan (Victoria J. Caine, Nicholas Olomu, Joan Price); Michigan State University, East Lansing, Michigan (Padmani Karna); University of Chicago Medical Center, Chicago, Illinois (Michael D. Schreiber, Leslie Caldarelli, Sunila E. O’Connor, Michael Msall, Susan Plesha-Troyke); William Beaumont Hospital, Royal Oak, Michigan (Daniel Batton, Karen Brooklier, Beth Kring, Melisa J. Oca, Katherine M. Solomon).
Author Contributions
OD and AL contributed equally to this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Neurological Disorders and Stroke (5U01NS040069-05; 2R01NS040069-06A2), the National Eye Institute (1-R01-EY021820-01A1), the NIH Office of the Director (1G3OD023348-01), and the National Institute of Child Health and Human Development (5P30HD018655-34).
Ethical Approval
The enrollment and consent processes were approved by the individual institutional review boards.