
Abstract
Introduction
Extremity trauma is a common presentation to Emergency Departments (ED). It can occur as an isolated injury or in conjunction with injury to other organs, with severity ranging from minor to life- and limb-threatening.1,2 Although peripheral vascular injuries are relatively uncommon, they are more common than vascular injuries to the chest and abdomen in both civilian and military settings. The reported incidence of lower limb arterial injury varies by mechanism, occurring in 1% of long bone fractures, 16% of knee dislocations, and up to 30% of gunshot wounds. 3 Peripheral vascular injuries can have devastating consequences such as amputation, disability, and death, requiring rapid assessment and early management to prevent poor patient outcomes. 4
A retrospective cohort study evaluated the epidemiology and management of vascular trauma in Canada. The study included 1330 patients from 8 Canadian Level 1 trauma centres between 2011 and 2015. Lower extremity vascular injuries were identified in 10.1% (n = 134) of patients, with the superficial femoral and popliteal artery most commonly injured. Blunt trauma was responsible for 63% of all vascular injuries, with motor vehicle collisions the most common cause overall. Penetrating injuries accounted for 36% of all vascular injuries, the majority due to stabbing. One percent of patients had a combination of blunt and penetrating injuries. 5
Physical exam classifies suspected extremity vascular injury in trauma patients into 3 categories: normal, presence of hard signs, or presence of soft signs of vascular injury. Patients with hard signs of vascular injury typically require urgent surgical intervention without imaging, although hemodynamically stable patients with suspected multilevel injury may benefit from CTA prior to surgical intervention.3,6 Adding the Ankle-Brachial Index (ABI) to the physical exam increases diagnostic sensitivity and specificity to >95% in hemodynamically stable patients without hard signs of vascular injury. 7 However, ABI use is limited in patients with severe injuries, as it requires inflating a blood pressure cuff on the injured limb. 1 Current guidelines recommend no further workup for patients with normal physical exams and ABI >0.9, while CTA is advised for those with soft signs and ABI <0.9.1,4
With technological advances over the past decade, including improved temporal and spatial resolution of modern multidetector CT (MDCT) scanners, CTA has become the first-line imaging test for suspected extremity vascular injuries and has largely replaced CA. 8 CTA has a high sensitivity and specificity for detecting peripheral vascular injuries comparable to CA. Additional benefits include increased accessibility, relatively non-invasive investigation with the ability to assess non-vascular structures, combining extremity CTA with torso imaging in polytrauma patients, and lower cost and more time-efficient compared to CA.1,9,10 However, CTA is not without inherent risk to patients, and is a costly examination, with improper use proven to increase healthcare costs with no added benefit to patients, prolonging ED wait times and length of stay. 11
Recent studies have found that CTA utilization could be reduced if studies were ordered according to physical exam findings without negatively affecting patient outcomes. Callan et al showed a 48% reduction in CTA rates when imaging was limited to specific physical exam criteria. 3 Similarly, Warwick et al concluded that a normal physical exam can often eliminate the need for CTA, with hard signs being a better predictor of intervention than imaging. 4 Joseph et al performed a retrospective review of traumatic lower limb CTA studies at a level I trauma centre in Australia between 2016 and 2019. They concluded that CTA is unlikely to demonstrate a vascular injury requiring surgical intervention without clinical signs of vascular injury. 12 Despite the growing body of literature, there is a paucity of data on CTA utilization in lower extremity vascular trauma in Canadian Level 1 trauma centres.
This study aimed to evaluate CTA usage in patients with suspected lower extremity vascular injury in a Canadian level I trauma centre, determine the rate of positive CTA studies and those requiring intervention, and identify factors that could reduce unnecessary examinations.
Material and Methods
Study Design and Patients
This single-centre retrospective cohort study was conducted at a Canadian Level 1 trauma centre after approval from the Institutional Ethics Committee. A retrospective chart review was performed for patients referred for lower extremity CTA in the settings of trauma between January 2020 and September 2024. As per institutional policy for retrospective chart review, the requirement for patient informed consent was waived.
A Radiology Information System (RIS) search identified trauma patients referred for lower limb CTA and CTA abdomen and pelvis with lower limb runoff at the time of resuscitation in the ED. A detailed chart review was conducted using the Institution’s Electronic Patient Record (EPR). Patients were eligible if they presented with suspected lower extremity vascular injury, including those referred from outside facilities with CTA performed at our institution. Exclusion criteria included CTA ordered for non-traumatic indications, such as evaluation of peripheral vascular disease, surgical planning, assessment of postoperative complications, and non-acute trauma. Non-diagnostic studies and follow-up CTA examinations within the study period were also excluded.
Data were collected from the EPR, including entries from the Trauma team, Emergency Department, relevant specialties such as Orthopaedic Surgery, Vascular Surgery, Interventional Radiology, and operative reports. Patient demographics, mechanism of injury, initial vascular findings on physical exam, ABI, vascular and musculoskeletal findings on CTA, and subsequent vascular interventions (Vascular Surgery or Interventional Radiology) were collected.
Physical exam classifies suspected extremity vascular injury in trauma patients into normal physical exam, presence of hard signs, or presence of soft signs of vascular injury. A normal vascular exam is defined as a warm limb with palpable pulses and intact distal perfusion. Hard signs include absent or diminished pulses, pulsatile hematomas, active bleeding, bruits, neurological deficits, and distal ischemia. Soft signs include proximity-related injuries, non-pulsatile bleeding, and small, non-expanding hematomas.1,3,4
Patients were classified into one of 3 categories based on CTA results: normal CTA, major CTA findings, or minor CTA findings of vascular injury. The most severe injury was used to classify patients if multiple vascular injuries were present. Major and minor CTA findings of vascular injury were defined as an injury to the common femoral, profunda femoris, superficial femoral, popliteal, tibioperoneal trunk, anterior tibial, posterior tibial, or peroneal arteries. Minor injuries were considered luminal irregularity or vasospasm, whilst major injuries included stenosis, occlusion, rupture, arteriovenous fistula, or pseudoaneurysm.
Statistical Analysis
Descriptive statistics (ie, counts, proportions) of demographic characteristics were summarized for all respondents. Continuous variables were summarized using mean, standard deviation, minimum, and maximum values when normally distributed. When not normally distributed, continuous variables were summarized using median, 25th to 75th percentile interquartile range, minimum, and maximum values. Categorical variables were summarized using counts and percentages. For comparative statistics, Chi-squared tests were conducted to assess categorical associations, when appropriate. If any expected value in the contingency table was <5, Fisher’s exact test was used. Statistical analyses were performed with STATA software (Version 18.5).
Results
The initial RIS search identified 671 potential patients. Fifty-nine patients were excluded after the EPR review deemed them ineligible from further analysis. Reasons for exclusion included scans performed for non-trauma related conditions, such as the workup of peripheral vascular disease, preoperative planning, postoperative complication assessment, non-acute trauma, duplicate, and non-diagnostic studies (Figure 1).
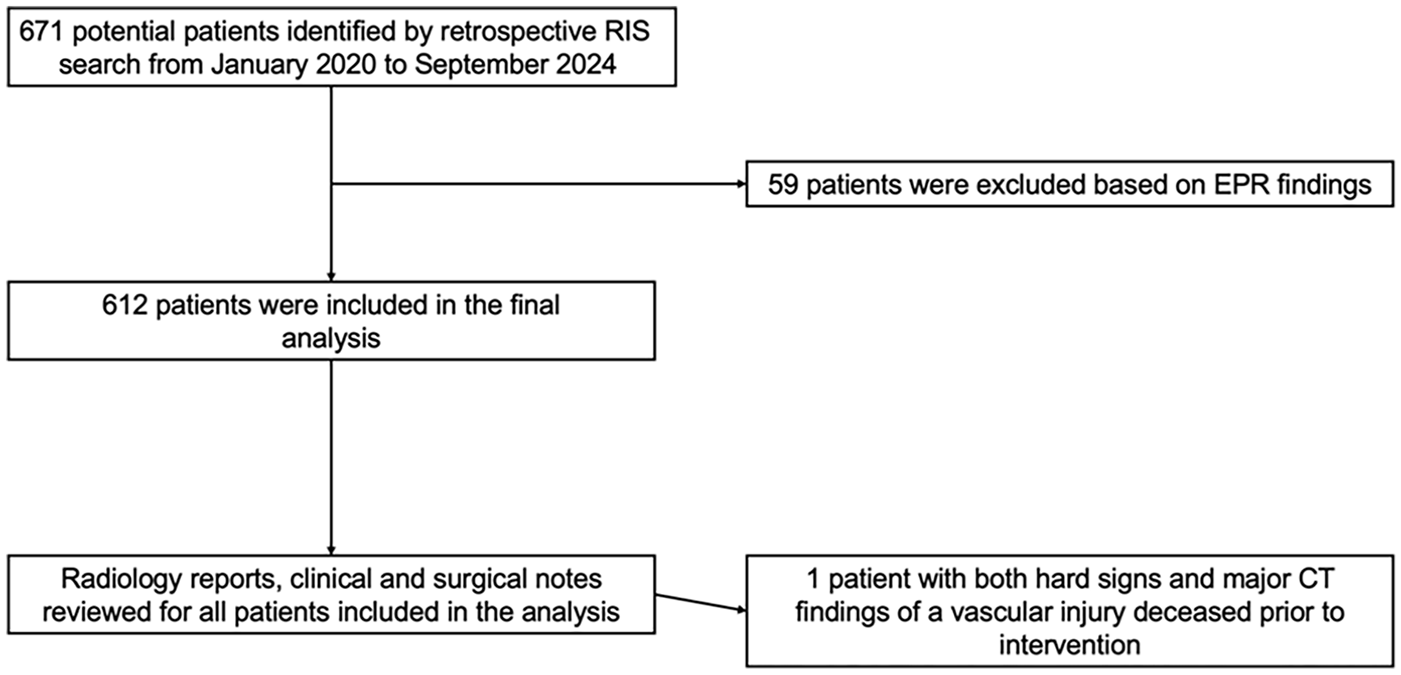
Flow chart for identifying eligible patients.
The final analysis included 612 patients with a median age of 32 years (range 15-99). Five hundred four were male (82%) and 108 female (18%). Blunt trauma (61%) was more common than penetrating trauma (39%), with motor vehicle accidents and gunshot injuries being the 2 most common mechanisms of injury in each category, respectively. Five patients (0.5%) sustained a combined blunt and penetrating injury (Table 1).
Demographic and Mechanism of Injury Data.
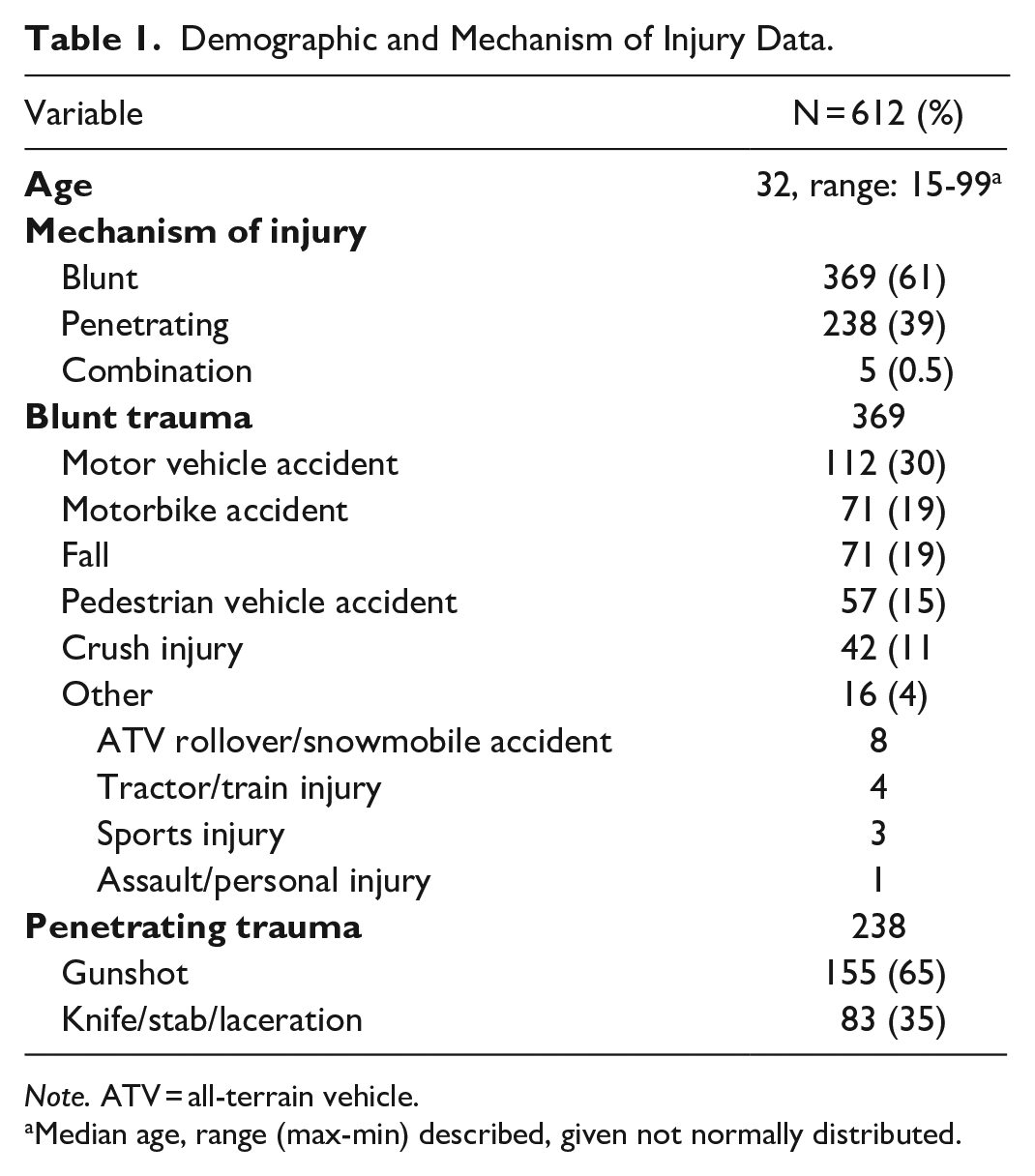
Note. ATV = all-terrain vehicle.
Median age, range (max-min) described, given not normally distributed.
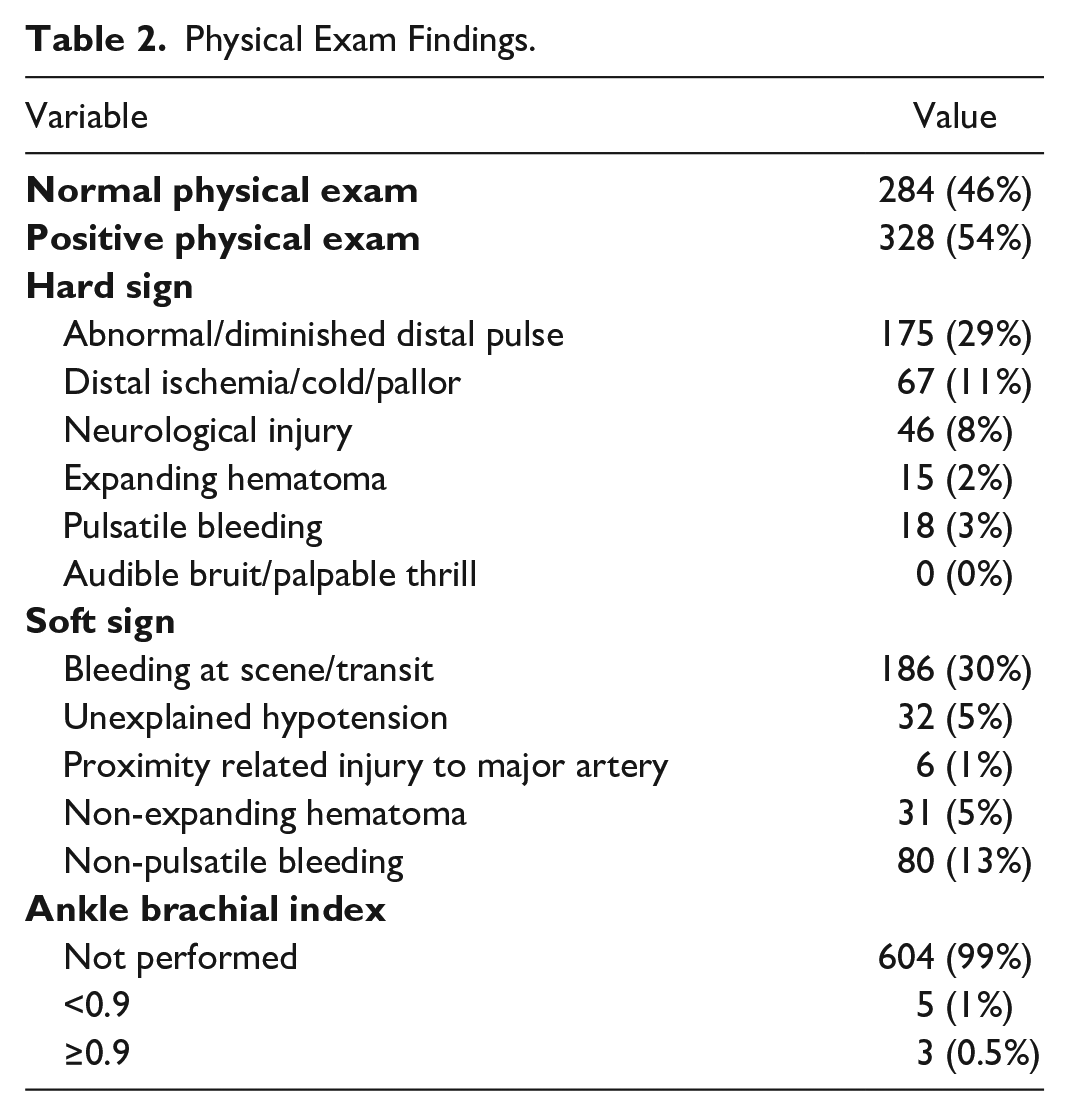
Nearly half (46%) of the 612 patients referred for CTA had a normal physical exam with no findings suggesting a vascular injury. Three hundred seventy-nine (54%) patients had soft signs, hard signs, or a combination of both on physical exam. Of those, 204 (62%) patients had at least one hard sign of a vascular injury, with abnormal and diminished pulses the most common hard sign (n = 175). Despite its high sensitivity and specificity, the ABI was performed in only 8 patients (1.5%) in our cohort (Table 2).
Physical Exam Findings.
One hundred sixty-three (27%) patients had positive CTA. One hundred twenty-one patients had major CTA findings, and 42 had minor findings of a vascular injury on CTA. The most common major CTA finding was arterial occlusion and rupture in 69 and 23 patients, respectively (Figure 2). Of the 612 patients in the study, 381 (62%) had a whole-body CT performed at the same time as the CTA of the lower extremities (Table 3). One patient included in the analysis had hard signs on physical exam and major CTA findings of a vascular injury but died before intervention.
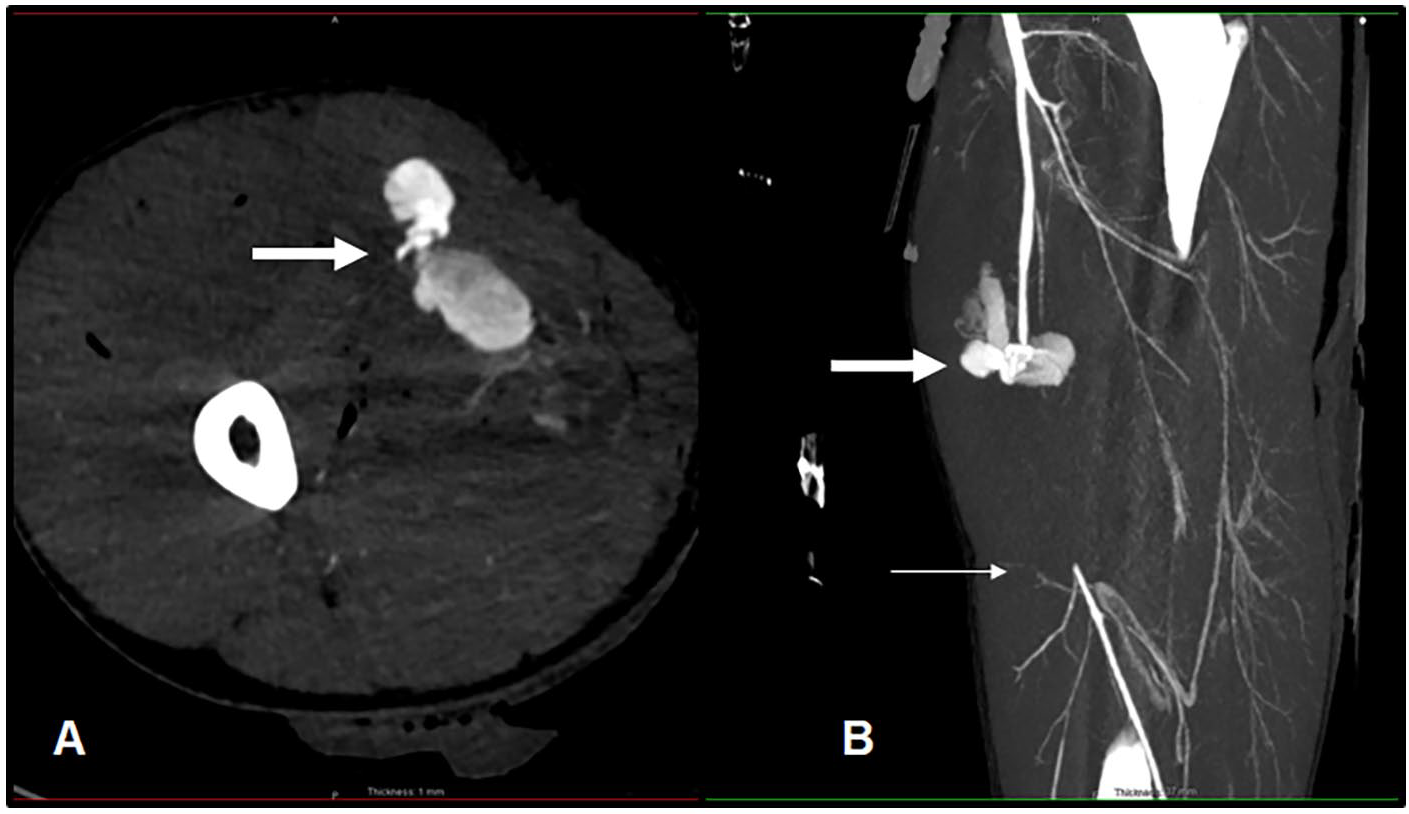
Fifty-one-year-old male with a right lower limb gunshot wound. Axial right thigh CTA (A) and sagittal right thigh maximal intensity projection (B) depicting a major CTA finding of a vascular injury with mid superior femoral artery rupture with active contrast extravasation (thick white arrows). The vessel reconstitutes distally from arterial collateral supply (thin white arrow).
Computed Tomography Angiography Findings and Intervention.
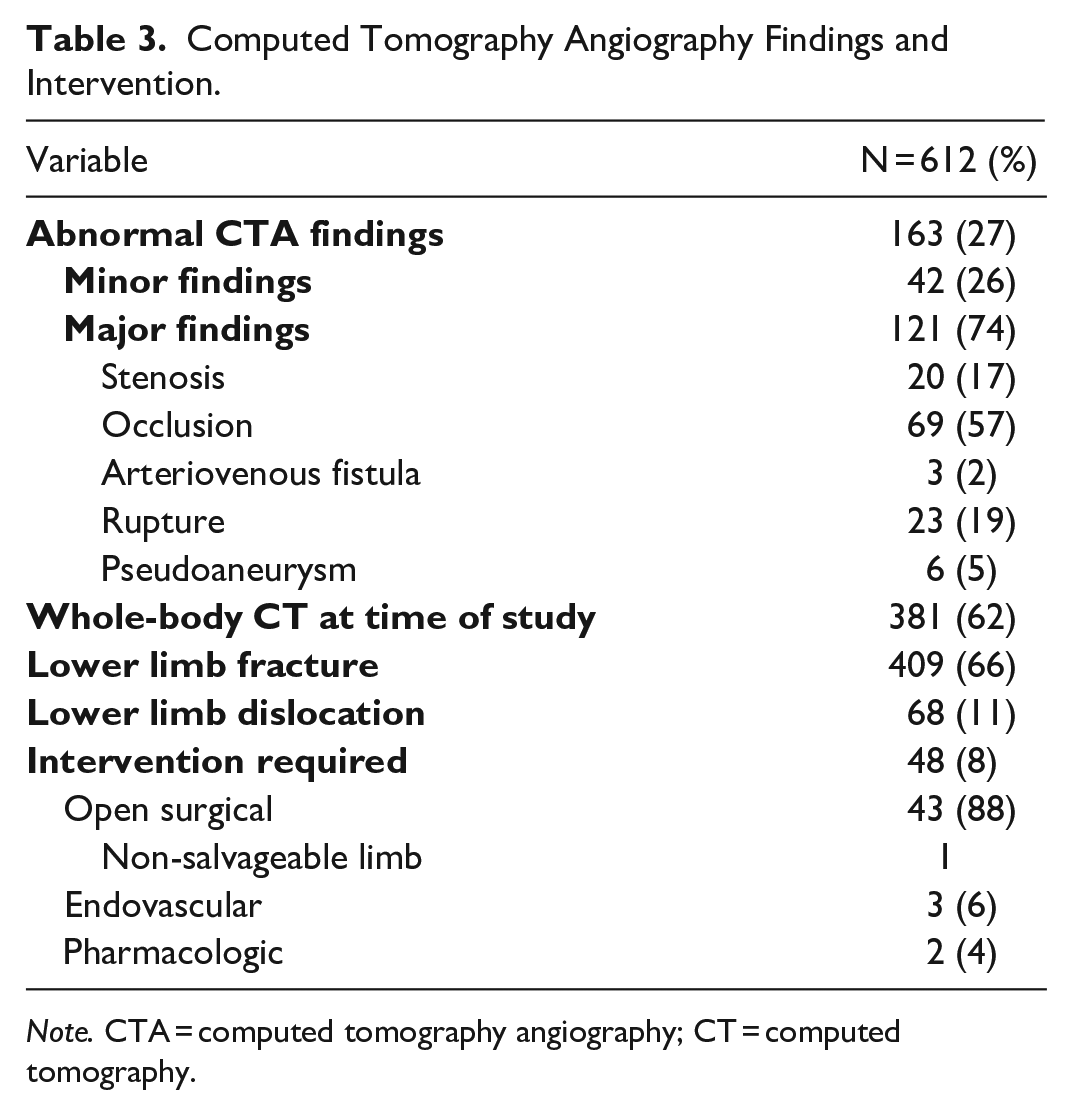
Note. CTA = computed tomography angiography; CT = computed tomography.
In the 328 patients with a positive physical exam, there were 100 (30%) major and 28 (9%) minor CTA findings of a vascular injury (Table 4). A positive physical exam was associated with a statistically significantly higher likelihood of a positive CTA (39% positive vs 61% normal CTA, P-value <.001) and major CTA abnormalities (30% major vs 9% minor CTA findings, P-value <.01). Patients with hard signs (n = 204) on physical exam had a higher prevalence of major (n = 84) versus minor (n = 20) CTA findings. There was no statistically significant difference in positive CTA versus normal CTA or major versus minor CTA findings based on the mechanism of injury. Forty-eight (8%) patients required an intervention, all of whom had at least one hard sign on physical examination. Forty-three patients underwent an open surgical procedure performed by Vascular Surgery, with one patient (2%) requiring an amputation. Three patients had an endovascular procedure performed by Interventional Radiology, and Vascular Surgery prescribed pharmacological treatments in 2 patients. CTA findings were confirmed in the operative reports for all patients who underwent open surgical and endovascular procedures.
CTA Findings and Management Based on Physical Exam Findings and Mechanism of Injury.
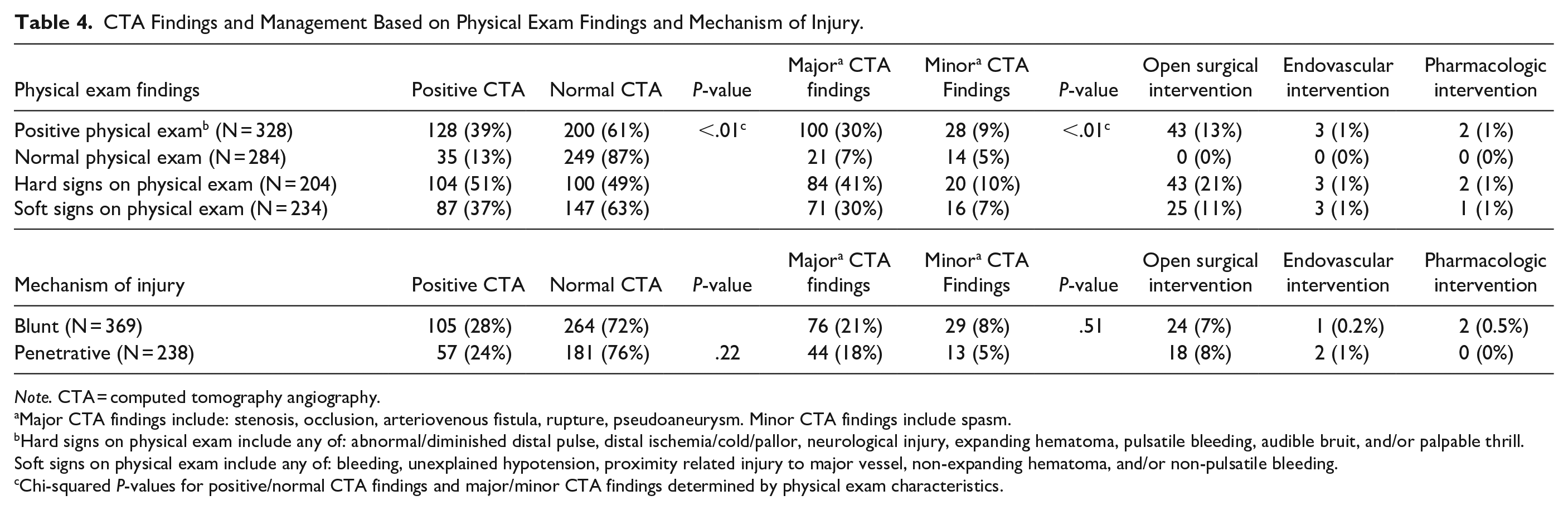
Note. CTA = computed tomography angiography.
Major CTA findings include: stenosis, occlusion, arteriovenous fistula, rupture, pseudoaneurysm. Minor CTA findings include spasm.
Hard signs on physical exam include any of: abnormal/diminished distal pulse, distal ischemia/cold/pallor, neurological injury, expanding hematoma, pulsatile bleeding, audible bruit, and/or palpable thrill. Soft signs on physical exam include any of: bleeding, unexplained hypotension, proximity related injury to major vessel, non-expanding hematoma, and/or non-pulsatile bleeding.
Chi-squared P-values for positive/normal CTA findings and major/minor CTA findings determined by physical exam characteristics.
Two hundred eighty-four patients with a normal physical exam were referred for CTA. Of these, 87% had a normal CTA study. Thirty-five patients (13%) had a positive CTA, with 21 major and 14 minor CTA findings of a vascular injury. Vascular Surgery assessed all patients with a positive CTA in the ED. No patients with a normal physical exam and a positive CTA required an intervention.
Discussion
Trauma is a leading cause of death among patients under 45 years and accounts for approximately 9% of deaths across all age groups worldwide.13,14 Despite lower extremity vascular injuries being relatively uncommon, these injuries can have devastating consequences, such as amputation, disability, and death, and require rapid assessment and multidisciplinary management to prevent poor outcomes.4,15-18 Due to technological advances in MDCT, CTA has largely replaced CA in the workup of patients with suspected lower extremity vascular injury, with increased CTA utilization and potential overuse reported in some centres. Le Roux et al reported a 13% annual increase in CTAs performed for penetrating lower extremity trauma without a corresponding rise in positive findings. 6 Monazzam et al also found no evidence to support routine CTA in patients with fractures and no signs of vascular injury on physical exam. 15
Patients with a positive physical exam were more likely to have a positive CTA. No patients with a normal physical exam and a positive CTA required an intervention, indicating an inverse relationship between a normal physical exam and a vascular injury requiring an intervention. Of the 163 patients in our cohort with a positive CTA, 48 (8%) required an intervention, all of whom had at least one hard sign of a vascular injury.
Our findings align with prior studies. Patient demographics and mechanism of injury in our cohort were similar to those reported by Brian et al, supporting the generalizability of our findings despite its single-centre design. 1 Our findings further corroborate Brian et al, who demonstrated that many patients referred for CTA had a normal physical exam, with the majority having no vascular injury and requiring no intervention and Callan et al, who found that CTA was often ordered without an indication based on physical exam findings in their institution, most of which did not alter the patient’s treatment or outcome.1,3 Unlike previous research, our study provides new insights into CTA usage in a Canadian Level 1 trauma centre.
Only 1.5% of patients had a documented ABI, emphasizing the underutilization of the ABI as part of the physical exam. This corroborates work by Warwick et al and Callan et al, who reported 2% and 12.5% ABI rates, respectively.3,4 The ABI is a non-invasive test that forms part of the diagnosing and management guidelines published by The American Association for the Surgery of Trauma in 2020. It has been proven to assist physicians in their decision-making process when assessing patients with a suspected lower extremity vascular injury and who are hemodynamically stable without hard signs of vascular injury. 19 Despite the advantages of ABI, factors such as time, experience, and technical difficulty create potential barriers to routine use in clinical practice.
CTA has many advantages, including increased availability, rapid diagnosis, and the ability to combine with whole-body CT. Still, it is not without risk, and the workup for patients with suspected extremity vascular injury needs to be individualized. CTA exposes patients to ionizing radiation, which increases their lifetime risk of developing cancer. This risk is higher in young patients and correlates with exposure. 20 The median age of patients in our cohort was 32. A study published in the Journal of the American Medical Association by Berrington de González et al determined that approximately 15 000 people would die from CT-induced cancer from scans performed in the United States of America in 2007, with one-third of cancers occurring in patients who underwent a CT scan between the ages of 35 and 54 years. 21 Sixty-two percent of our patient cohort had a CTA study with whole-body CT. Trauma patients are at an increased risk of higher cumulative effective radiation doses (CED) compared to surgical and medical patients, and this is primarily related to the use of whole-body CT and follow-up examinations. Physicians should consider patients’ CED and should keep it as low as possible to decrease the attributable future cancer risk. 22 CTA examinations require intravenous contrast material, and when CTA of the lower extremities is combined with whole-body CT, it requires an additional contrast bolus. Despite the risk of CA-AKI in trauma patients being low, it should be taken into account when deciding if a CTA examination is warranted. 23 In addition to the aforementioned patient factors, CTA is an expensive and time-consuming study that can negatively impact radiology services and healthcare resources. Improper CT use has been proven to increase healthcare costs with no added benefit to patients, prolonging ED wait times and length of stay. 11
Our study is not without limitations, including its retrospective design with the potential for introducing bias and incomplete data. This single-centre study may not be generalizable to other Level 1 trauma or non-trauma centres. The physical exam and CTA findings were gathered from the EPR, with reported findings dependent on physician experience and documentation practices. We only assessed patients referred for CTA as identified through a search in RIS. We did not assess all patients presenting to the ED with suspected extremity vascular injury during the study period. We did not follow up with patients beyond their initial CTA and intervention, which could account for the low incidence of amputation in our cohort. The decision whether a limb is salvageable or not is multifactorial and not solely based on the presence of a vascular injury. We did not reassess the images to ensure the accuracy of the reported injuries. However, using the provided report does mean that routine practice was not altered.
Our findings suggest that CTA studies should be conducted according to institutionally appropriate criteria, such as those of the American Association for the Surgery of Trauma, to prevent potential overuse. Future prospective studies are needed to determine if implementing an institution-specific protocol would reduce CTA utilization without negatively affecting patient outcomes.
Conclusion
A positive physical exam was associated with a statistically significantly higher likelihood of a positive CTA and major CTA findings of a vascular injury. Patients with hard signs on the physical exam had a higher prevalence of major than minor CTA findings, irrespective of the mechanism of injury. A normal physical exam had an inverse association with a vascular injury requiring an intervention, with no patients with a normal physical exam in our cohort requiring an intervention. In contrast, hard signs of a vascular injury were predictive of interventions, with all patients requiring an intervention having at least one hard sign of a vascular injury. Our findings suggest that implementing institution-specific appropriate criteria may reduce unnecessary CTA studies, minimize radiation exposure, and optimize resource use.
Footnotes
Acknowledgements
We would like to express our gratitude to all those who contributed to the completion of this research and to our families for their continued support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.