
Abstract
Introduction
Interventional Radiology (IR) is an indispensable part of the medical armamentarium for the treatment of vascular and non-vascular conditions, many of which are of an urgent or emergent nature.1,2 These include procedures for acute venous thromboembolism, hemorrhage, acute aortic syndromes, ischemia, and complex drainage procedures for sepsis. IR has evolved into a Royal College of Physicians and Surgeons of Canada (RCPSC) recognized subspecialty. 3 This change was an acknowledgement of the distinct skills and role of IR building on diagnostic radiology. IR may support patients under the care of other healthcare providers but may also be the primary treating service.2,4 For many emergent conditions treated by IR, there is often a limited time period to treat and rescue from irreversible deterioration. 5 Prompt access to on-call IR procedures is regarded in many jurisdictions as a requirement for patient safety. 1 For large, well-resourced transplant, oncology, trauma, and cardiovascular centres, IR is a critical part of the healthcare team. 6
Emergencies are not limited to daytime office hours, so access must include after-hours services. On-call IR teams must be appropriately trained and resourced including trained interventional radiologists, technologists, nurses, and access to anaesthesia support.1,7 There are well-publicized guidelines for the availability of after-hours on-call IR services in the United Kingdom, which suggest a minimum of 6 interventional radiologists for a 1 in 6 rota at sites offering after-hours services.1,8 There are no comparable guidelines in Canada. Additionally, as the Canadian healthcare landscape evolves, medical services that were previously only available at tertiary care services are becoming standard at community sites. Much like how demand for diagnostic services has grown exponentially, the demand for IR services has and will continue to increase. 9
Ontario is Canada’s largest province with a population approaching 16 million. 10 There are many hospitals in Ontario with daytime access to IR services. However, it is unclear how many of institutions have access to IR and local after-hours IR on-call services. The purpose of this survey is to assess the availability of after-hours IR on-call services at Ontario hospitals that have a radiology department and to determine potential barriers to the provision of IR after-hours on call services within Ontario.
Methods
A survey was developed to understand the availability of after-hours IR services and the barriers to implement after-hours IR services in Ontario. The authors’ institution is a high-volume academic IR practice that receives patient transfers from other hospitals within Ontario and wider Canada. The availability of IR call services in Ontario directly impacts the institution’s IR procedural volume. Therefore, the study was conducted as a quality improvement (QI) project to guide local planning. Research ethics board approval was waived by the local QI department. IR services were defined as any image-guided procedural availability after-hours, with subcategories described below. The survey was not pilot tested. A hospital may provide after-hours IR services even if it does not have a formal IR department or division (eg, abscess drainage). The 17-question survey assessed several categories of information (Appendix—survey questions), with respondents falling into one of 4 categories:
NoIR/NoCall: Hospital/Centre with no formal IR department/division that also does not offer after-hours IR services.
NoIR/Call: Hospital/Centre with no formal IR department/division that does offer after-hours IR services.
IR/NoCall: Hospital/Centre with formal IR department/division that does not offer after-hours IR services.
IR/Call: Hospital/Centre with formal IR department/division that offers after-hours IR services.
For the groups that do not provide after-hours IR services, the survey evaluated these categories: (1) barriers to implementing after-hours services, (2) referral patterns for hospitals that do not offer after-hours IR, (3) interest in providing after-hours services. For the groups that provide after-hours IR services, the survey assessed the types of procedures available and the frequency of call.
Definitions used in the survey for after-hours services included “complete coverage” (provision of after-hours services 365 days a year, 24 hours a day), “weekend day coverage” (coverage during routine/minimally expanded daytime hours, eg, 08:00-17:00), and “weekday coverage” (weekday after-hours coverage, outside of normal working hours such as 17:00-08:00). Additionally, the survey asked about the provision of 5 broad categories of services: vascular (eg, gastrointestinal hemorrhage), neurovascular intervention (endovascular thrombectomy for stroke), drainage procedures (nephrostomy, abscess drainage, chest tubes, etc.), and venous access (eg, dialysis lines), or other.
The survey was administered through a regional radiology association: The Ontario Association of Radiologists (OAR). The survey was distributed to the list of the department heads (DH) of radiology maintained by the OAR. The OAR administered the survey using Survey Monkey (San Mateo, CA, USA), a commonly used service for email surveys. The survey was open for 6 weeks (March-April 2024). A reminder email was sent. All results were anonymous and self-reported.
Data Analysis
Data were captured via the Survey Monkey (San Mateo, CA, USA) system and exported to a comma separated value file. Counts and percentages are reported for the categorical data. Limited open-ended responses and comments were also collected and reported in summarized form to preserve anonymity.
Results
The survey was sent to the email list of 73 DHs of radiology in Ontario and open for a period of 6 weeks from March to April 2024. The completion rate was 41% (30/73 DHs). The reported practice types were 23.3% (7/30) academic, 30.0% (9/30) large regional hospital/network, 43.3% (13/30) small regional hospital, and 3.3% (1/10) other—an academic ambulatory care centre. Additionally, 63.3% of respondents (19/30) reported an affiliation with an academic institution. Two thirds of the DHs stated that they had a formal IR division or department (20/30), while the other third did not have a formal IR division or department (10/30), of which all but one (a large regional hospital) were small regional hospitals. One of the small regional hospitals with no IR department reported full calendar call coverage for drainage procedures (eg, nephrostomies and abscesses). Another hospital reported that weekend daytime coverage was available for drainage procedures.
Hospitals were then split into groups based on the presence or absence of an IR department and whether they offered IR services after-hours (ie, 4 groups: NoIR/NoCall, NoIR/Call, IR/NoCall, IR/Call). Ten hospitals had no formal IR department/division, but 2 of these reported they offered after-hours IR services for urgent drainage procedures (eg, nephrostomies or abscess drains). Twenty hospitals had formal IR departments/divisions and of these 14 (14/20, 70%) offered IR after-hours coverage. Finally, of those respondents with IR departments with IR after-hours services (13/14, 92.9%), complete coverage was provided in 11/13 (84.6%). Two hospitals stated that after-hours coverage was only available on the weekdays. Six hospitals with IR services (6/20, 30%) offered no after-hours services. Therefore, there were 8 NoIR/NoCall groups, 2 NoIR/Call groups, 14 IR/Call groups, and 6 IR/NoCall groups.
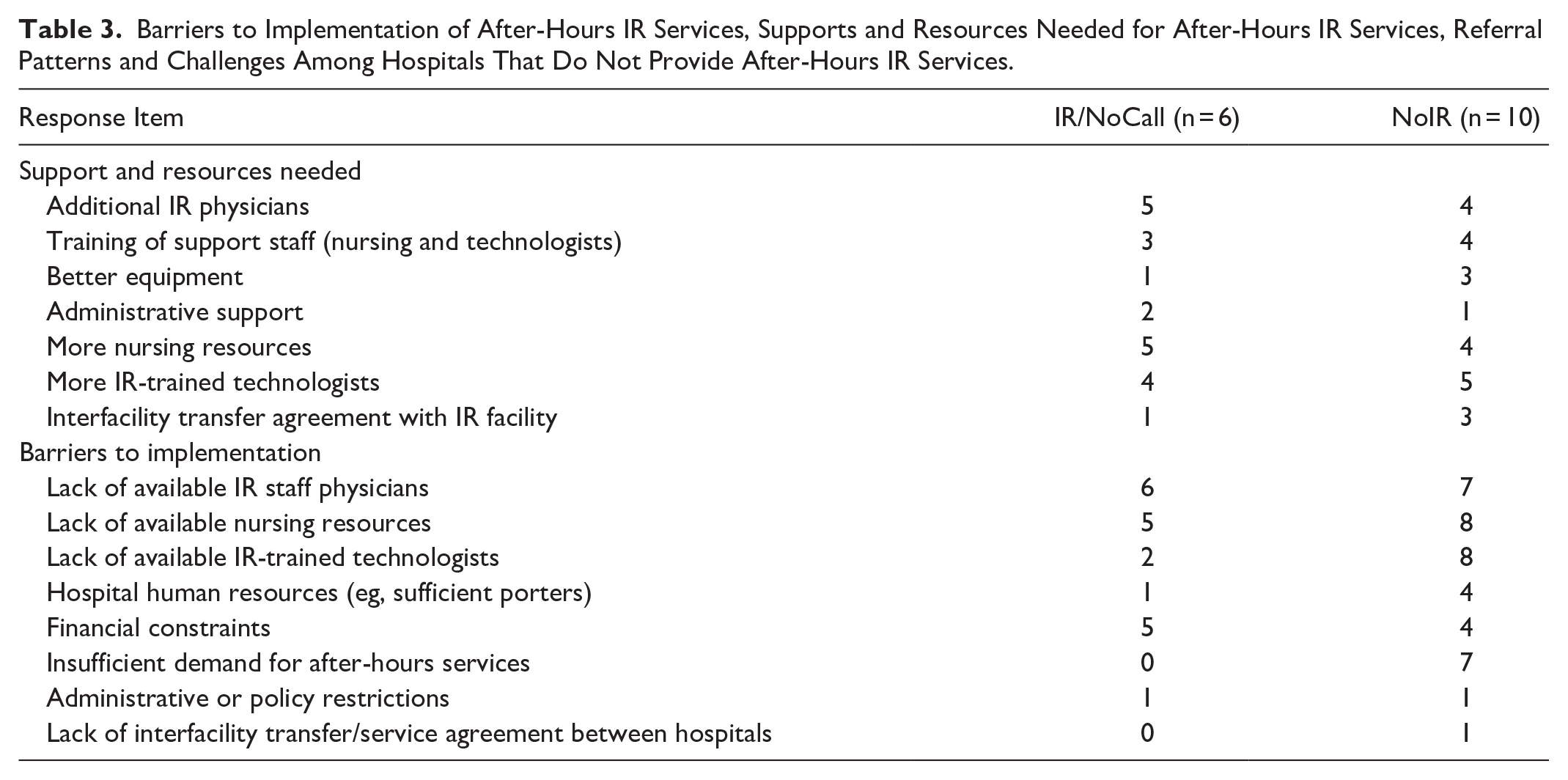
The services offered by the hospitals with formal IR departments/divisions are reported in Supplemental Table 1. All hospitals with formal IR departments/divisions had staff with formal IR training, conversely the hospitals without formal IR departments demonstrated a lack of staff with formal IR training (Table 1). The demand for IR services was highest in the hospitals that offered after-hours IR services whereas low demand was seen in both the NoIR groups and the IR/NoCall group (Table 2). 92.9% (13/14) of the IR/Call groups stated that after-hours demand was increasing year-over-year. Additionally, one of the 2 NoIR/Call department heads responded that their after-hours demand was increasing year-over-year. The barriers to implementation of after-hours IR services are reported in Table 3; the most common barriers were staffing resources including IR physicians, nursing, and technologists.
Number of IR Trained Physicians in the Hospitals/Centres.
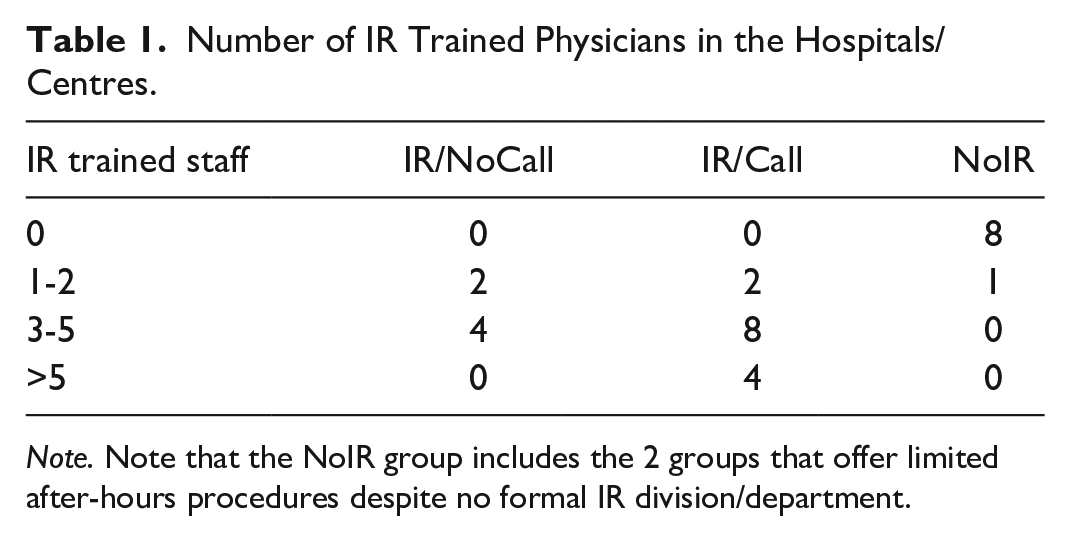
Note. Note that the NoIR group includes the 2 groups that offer limited after-hours procedures despite no formal IR division/department.
Average Demand for After-Hours IR Services at the Institution.*
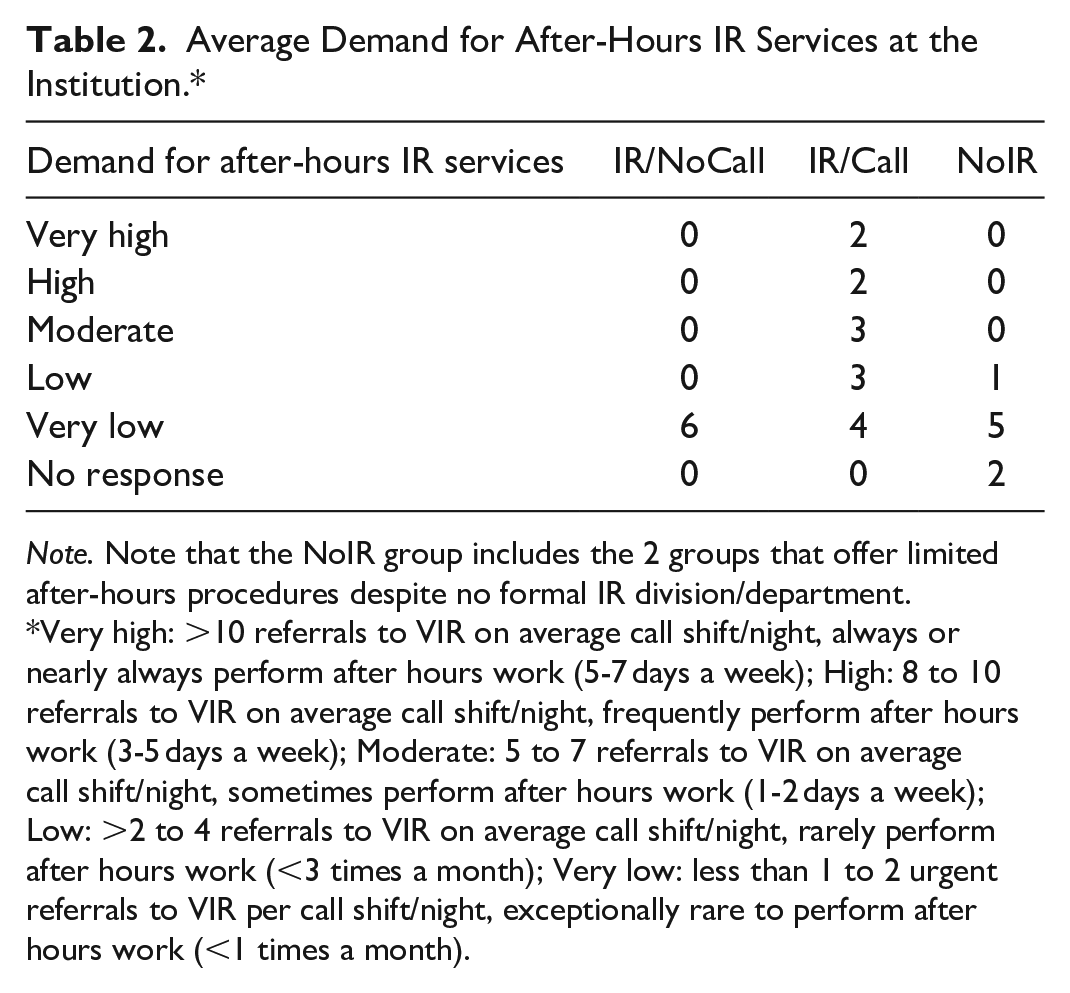
Note. Note that the NoIR group includes the 2 groups that offer limited after-hours procedures despite no formal IR division/department.
Very high: >10 referrals to VIR on average call shift/night, always or nearly always perform after hours work (5-7 days a week); High: 8 to 10 referrals to VIR on average call shift/night, frequently perform after hours work (3-5 days a week); Moderate: 5 to 7 referrals to VIR on average call shift/night, sometimes perform after hours work (1-2 days a week); Low: >2 to 4 referrals to VIR on average call shift/night, rarely perform after hours work (<3 times a month); Very low: less than 1 to 2 urgent referrals to VIR per call shift/night, exceptionally rare to perform after hours work (<1 times a month).
Barriers to Implementation of After-Hours IR Services, Supports and Resources Needed for After-Hours IR Services, Referral Patterns and Challenges Among Hospitals That Do Not Provide After-Hours IR Services.
The most common reason for ongoing provision of after-hours services in those hospitals that provide IR services on call were patient satisfaction and care (11/14), referring physician satisfaction (7/14), administrative policy (7/14), and collaboration with multidisciplinary cases in a hybrid operating room environment (7/14). Two groups reported financial incentives as contributing to the provision of services. Six groups reported the inability to complete elective or non-emergent cases during daytime hours as the reason for providing after-hours services.
Among the hospitals without after-hours IR services, 2 (2/10, 20%) of the hospitals without IR departments were interested in providing after-hours IR services in the future whereas the majority were not (8/10). In the IR/NoCall hospitals, 3 (3/6, 50%) hospitals were interested in implementing after-hours services in the future. Two (2/6, 33.3%) were unsure, with one commenting a mixed sentiment in the local radiology department/group. One group did not respond. The response to factors for providing after-hours services are listed in Table 4.
Factors That Would Be Impactful in Deciding to Implement After-Hours IR Services in Hospitals Not Providing After-Hours IR Services at Present.
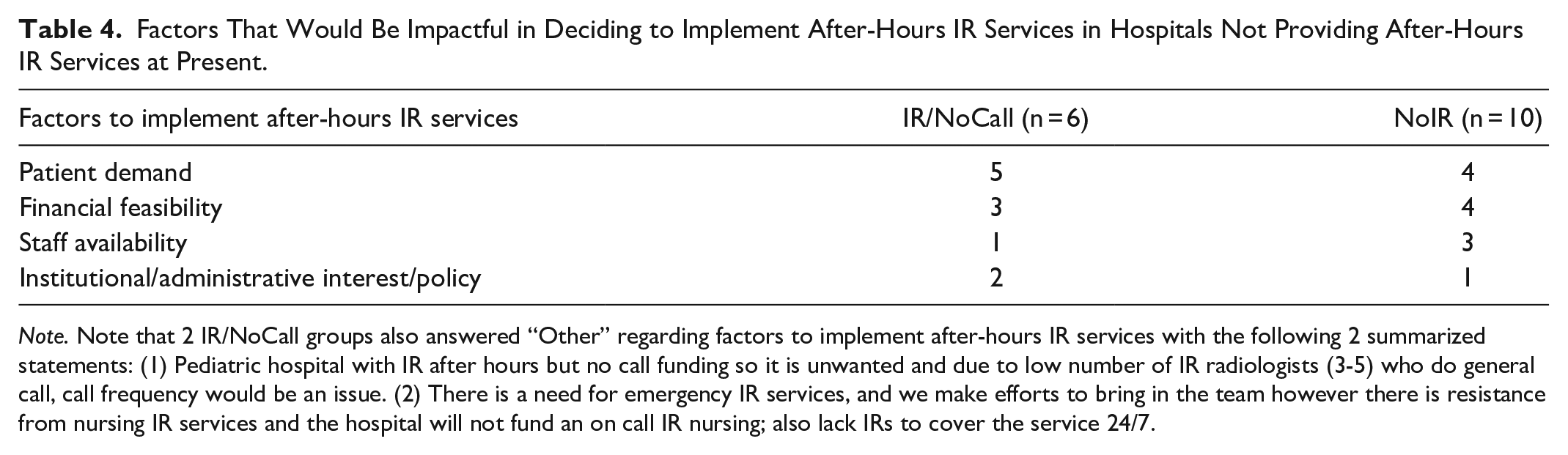
Note. Note that 2 IR/NoCall groups also answered “Other” regarding factors to implement after-hours IR services with the following 2 summarized statements: (1) Pediatric hospital with IR after hours but no call funding so it is unwanted and due to low number of IR radiologists (3-5) who do general call, call frequency would be an issue. (2) There is a need for emergency IR services, and we make efforts to bring in the team however there is resistance from nursing IR services and the hospital will not fund an on call IR nursing; also lack IRs to cover the service 24/7.
One site reached out to the authors to describe their local model, where they have a rotating IR physician that comes to the site to provide daytime services on a limited basis every week. This affords a hospital/group access to IR services during daytime hours and prevents hospital transfers of patients for such procedures. Other single free-form responses collected during the survey period were summarized below to ensure anonymity:
- Lack of provincial Ontario Hospital On-Call Coverage (“HOCC”) funding limits availability of services.
- Non-IR radiologists may block or disincentivize IR staff.
- Time/phone calls surrounding an IR procedure may greatly exceed the actual case time (eg, phone call for request, additional consultations, calling in team, booking transportation, patient transfer delays).
Discussion
As the scope of IR continues to grow, the need for 24/7 access to procedures performed by IR may become more ubiquitous. For example, access to IR is required for level I and II trauma centres, as defined by the American College of Surgeons. 6 Additionally, patients are increasingly older and medically complex, shifting the risk benefit ratio toward minimally invasive approaches offered by IR, especially for urgent or emergent conditions. 11 The Royal College of Radiologists in the UK recognizes access to IR services off-hours as essential to patient safety in acute care settings. 1 In the current study, two thirds of respondents stated their hospital had a formal IR division or department (20/30). The other third (without formal IR services) were all small regional hospitals but for one large hospital. Although the response rate was low (41%), it is likely that the overall provision of IR services is like other regions. For example, one study in Scotland found that 14 out of 38 acute care hospitals had IR services, that is, less than half of hospitals have formal IR services. 12 Of the groups with IR services in the current study, 70% (14/20) offered after-hours services and 30% did not (6/20). Similarly, 8 out of 14 hospitals with IR in Scotland offered IR after-hours with a formal rota. 12 Given the heterogeneity of IR services and inconsistency with on-call availability, province-wide clarity is needed regarding which institutions provide IR services, outlining when and to what extent. For example, the Ontario Regional Stroke Network clearly delineates patient transfer and access to stroke care based on region. 13 A list of critical procedures should be identified (eg, embolization for hemorrhage) at the provincial level with a clear guidelines on timeliness (eg, time to needle of <4 hours) and patient transfer methods.
For those hospitals that offer after-hours IR services, clear guidance on what procedures are offered after-hours is required. 14 In emergencies, there is limited time to rescue patients. For example, in trauma related active hemorrhage, the American College of Surgeons recommends an IR response of <1 hour. 6 Conversely, ad-hoc or informal on-call arrangements may delay the time from decision to treat to access to care when it is unclear if an on-call IR team is available. Referring clinicians also need clear policies on what types of treatment are offered after-hours and which are not. These guidelines would serve 2 purposes: (1) to ensure clear pathways to life-saving treatments for referring clinicians, and (2) to mitigate case priority drift, where non-urgent/emergent procedures occur out of hours. The current study found that for nearly half of the groups that provide after-hours IR services, the inability to complete daytime work was a source of after-hours work. Minimizing “non-essential” after-hours procedural activities may reduce healthcare worker burnout. 9
The survey respondents noted a demand for after-hours IR services in Ontario. Nearly all radiology groups (92.9%) that provide after-hours services stated volumes were increasing year-over-year. This is similar to data in other countries demonstrating that overall volumes have increased, notwithstanding the COVID-19 pandemic, with one study reporting volume increases as high as a 240% in 5 years in other jurisdictions.15,16 The current study was not designed to quantify volumes; nevertheless, it reflects the increased number of IR procedures being performed and highlights the demand in Ontario. To better characterize the ongoing IR needs of Ontario and Canada, more granular provincial health data on IR utilization is required.
The results from this survey found that most radiology groups that offer IR services on-call do it for patient care and to support hospital services. Financial incentives (such as on-call stipends or hourly rates) were not reported as an important reason, with only 2 groups reporting it. Some DHs reported a lack of on-call stipends and resistance from other radiologists in the group for the provision of IR services. This implies that financial support of IR on-call activity could improve access for some departments. Logistical challenges in preparing patients for on-call IR procedures were cited by some survey respondents as barriers. Process improvements to facilitate communication and transportation of patients to and from IR could reduce critical time to treatment and administrative burden.
The United Kingdom Provision of Interventional Radiology Services document, a joint document from the Royal College of Radiologists and the British Society of Interventional Radiology, states that for provision of on-call services a minimum rota of 1 in 6 is required—that is, at least 6 IR physicians. 1 A survey of both private practice and academic interventional radiologists in the United States found that call was usually 1 in every 5 to 6 days, similar to UK guidelines. 17 Therefore, unless volumes are very low, the groups with less than 3 to 5 IR physicians should not be required or expected to provide out-of-hours IR services (or special scheduling arrangements such as a shared IR call pool). One study examining a newly created hospital and the provision of IR services found that the variety, volume, and complexity of on-call IR cases increased year over year. 16 When IR is available, it is used, much like diagnostic radiology services. Therefore, in the absence of a fully staffed team 24/7, it is conceivable that introduction of a service might result in a snowball effect of unintentionally increasing volumes. Regarding interest in providing after-hours IR services, most groups with IR services have responded to local demand, with the IR/NoCall group all citing very low demand. Similarly, the groups without a formal IR division also cited low or very low demand.
Demand is expected to grow, even if only from population growth. In 2023 and 2024, Ontario, Canada’s most populous province, saw the total population grow by more than 3%. 18 However, the number of PGY-1 radiology training spots across Canada has remained grossly stable (range of quota 77-84) since 2014. 19 The current study found a lack of IR-trained physicians and nursing staff were the 2 most commonly reported barriers to implementation of after-hours IR services. Other studies have found high levels of burnout among IR team members (nursing and technologists) with up to 50% saying they have considered leaving their position. 7 Therefore, as demand increases, health human resources might become the main limiting factor, if not already. One potential solution to alleviate IR physician demand is to increase practice mobility and inter-provincial practices through a pan-Canadian medical licence, further building on the Atlantic provinces’ model of the “Atlantic Registry.” 20 Similarily, a regional call pool of IR physicians might be able to serve a larger number of hospitals. This practice model might help IRs who rarely see emergent cases increase volumes maintain a broader procedural competency and also limit patient transfers. Indeed, data from cardiology highlights increased mortality in patients requiring interhospital transfer and there is similar concern for pulmonary embolism.21,22
Compared to other countries, Ontario is fortunately well resourced for physical supplies (such as stents or coils) for the treatment of patients. To leverage these resources (both human and physical supplies/equipment) and ensure equal access to patient care, regional transfer agreements or an IR call pool may be useful to ensure all patients have access to life or limb saving IR procedures, even when not available at the local institution.
Limitations of the current study include a low response rate, which is commonly observed in surveys. 23 This may reflect a non-response bias whereby hospitals with IR services might have responded whereas those without may not. The proportion of provision of IR services may be lower than captured. Given the limited response and small sample sizes in each category, statistical analysis is limited and therefore only response rates and proportions were reported. To maintain anonymity, the institution of the DHs was not captured, limiting geographical analysis. Finally, to reduce survey length but maintain a wide scope, it was limited in granularity. We did not obtain any information on whether other local providers from non-radiology specialties offer image-guided procedures, such as vascular surgery for ischemic legs.
In conclusion, IR continues to grow in scope and demand. Access to IR in Ontario is heterogeneous and not all hospitals with formal IR divisions provide after-hours IR services. As a variety of IR procedures are emergent/urgent, clear provincial guidance is required on what IR services should always be available and how patients get access to these services. At present, a main barrier to the provision of after-hours services in IR is the lack of health human resources, in particular IR physicians. Regional IR call pools, inter-hospital or regional transfer agreements may be a solution. Future studies to evaluate the number of IR procedures performed in Ontario and across the country and the number of IR physicians in the training pipeline will be instrumental in guiding/advocating for provincial and federal funding for IR training programs.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251340368 – Supplemental material for A Survey of After-Hours Interventional Radiology Availability in Ontario
Supplemental material, sj-docx-1-caj-10.1177_08465371251340368 for A Survey of After-Hours Interventional Radiology Availability in Ontario by Blair E. Warren, Alanna Supersad, Sebastian Mafeld, Arash Jaberi and George Oreopoulos in Canadian Association of Radiologists Journal
Supplemental Material
sj-docx-2-caj-10.1177_08465371251340368 – Supplemental material for A Survey of After-Hours Interventional Radiology Availability in Ontario
Supplemental material, sj-docx-2-caj-10.1177_08465371251340368 for A Survey of After-Hours Interventional Radiology Availability in Ontario by Blair E. Warren, Alanna Supersad, Sebastian Mafeld, Arash Jaberi and George Oreopoulos in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.