
Abstract
During the hands-on teaching of Interventional Radiology (IR) to Residents and Fellows, certain learning tips or guiding statements are often repeated. Over the past two decades, these tips have evolved into the “Rules for Interventional Radiology.” Relying on humour and the technical and foundational principles of our subspeciality, it is hoped that these Rules for IR provide helpful guidance to learners and practising Interventionalists in their daily work.
Many physicians recall the painful process of memorizing innumerable facts in preparation for examinations in medical school. Mnemonics made this task easier, even if many were crude or lewd, for example, certain mnemonics for remembering the cranial nerves or the bones of the wrist. During residency, radiologists-in-training also utilized memory aids to help remind them of lists of differential diagnoses. Interventional Radiology (IR) is a subspeciality of Radiology 1 that involves the coordinated coupling of imaging interpretation with manual dexterity and expertise for the performance of minimally invasive, image-guided, percutaneous diagnostic and therapeutic procedures. Thus, memory aids in IR may be most useful in the form of rules or guidelines, rather than lists or mnemonics.
I have had the honour and pleasure of serving as Fellowship Supervisor for Vascular and Interventional Radiology (VIR) at University Health Network and Mount Sinai Hospital, University of Toronto, for more than 20 years. In helping to train more than 100 Fellows, whilst working alongside them, certain sayings or aphorisms would come up repeatedly. Over time, I would quote them and refer to them as rules, often ascribing a random number to it, such as “Rule number 17.” Past trainees have reminded me of some of these rules from time-to-time, indicating that perhaps these rules may have been helpful to them in optimizing their care of patients.
Many of the Rules for IR listed below are stated in jest or with a dose of humour; invoking levity can aid in recall. No offense is intended. All rules may not necessarily be helpful to an individual, and one may disagree with certain rules - diversity of opinion is most welcome.
In an era when millions are reading self-help books such as “12 Rules for Life”
2
herein are my suggested top 55 “Rules for Interventional Radiology.” Whilst this review is directed at ‘learners,’ perhaps even experienced Interventionalists may find some of these rules axiomatic, or at least entertaining. The rules are divided into 3 categories: the first 5 rules are foundational and apply to life as an Interventional Radiologist (Figure 1), then there are 10 general rules for IR (Figure 2) followed by 40 IR procedural rules (see Figure 3) (listed in no particular order in terms of importance). Following some of the rules are explanatory notes, as well as, on occasion, a “corollary” serving as an additional related or clarifying rule. Rules for Life as an Interventional Radiologist. Rules for Interventional Radiology in General. Interventional Radiology Procedural Rules.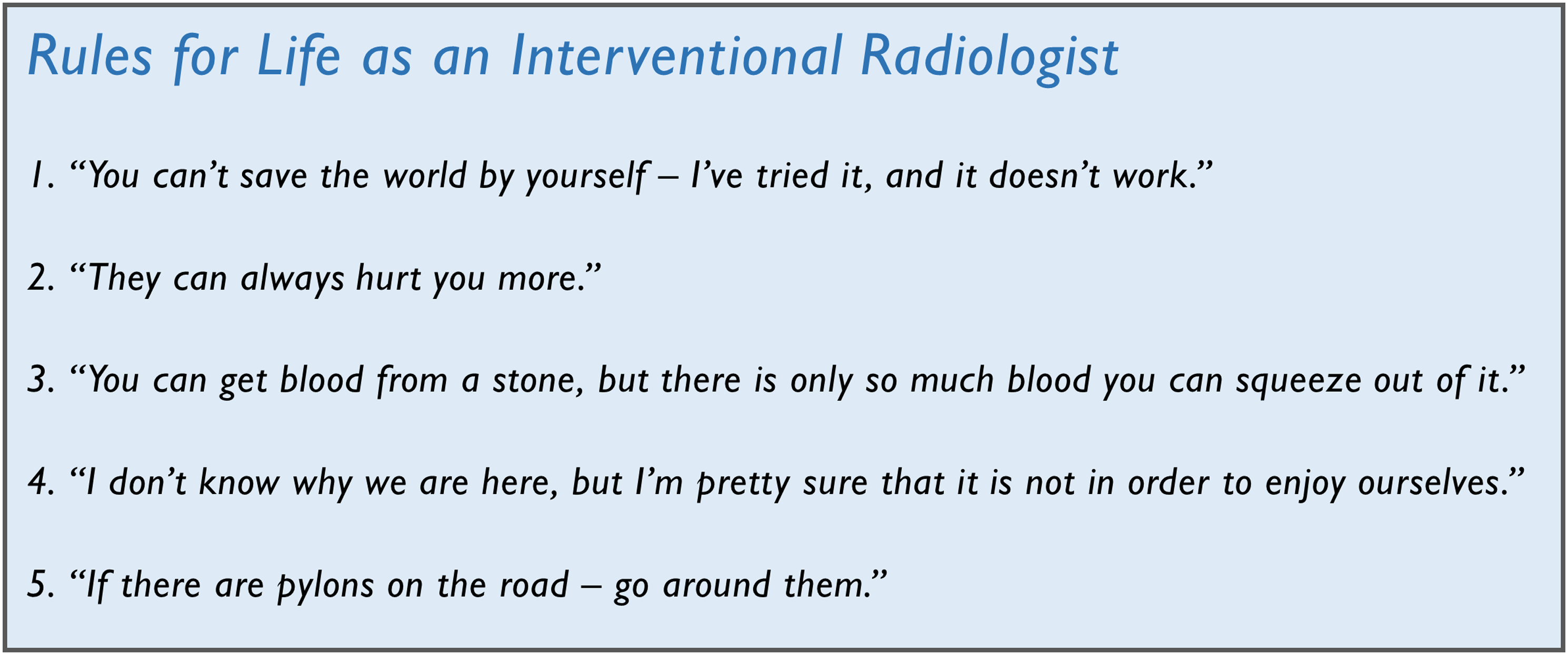
Rules for Life as an Interventional Radiologist
This rule reminds us that an individual can only do so much. But instead of despair, one should keep in mind the corollary to this rule: “If we all work together as a team, we can achieve so much more!”
This is a rule from Samuel Shem’s classic satirical novel, The House of God, about the coming-of-age of a physician-in-training. 3 A reminder that work and life can be challenging, and conflict may arise not only with adversaries but also with family, friends and colleagues. So things can always be worse than they are at present. But we should maintain eternal optimism and see the good in any situation, by remembering the corollary to this rule: “If things can get worse, then maybe things aren’t that bad right now.”
When one is asked to push oneself further, additional effort can be possible, as in giving 110%, but there is a limit.
A quote from my favourite philosopher, Ludwig Wittgenstein. 4 Aim a lot higher than happiness as the goal of your life’s work: helping others, for instance. Then welcome joy if it happens to land on you for brief moments of time.
There will be barriers to success. Learn how to navigate them.
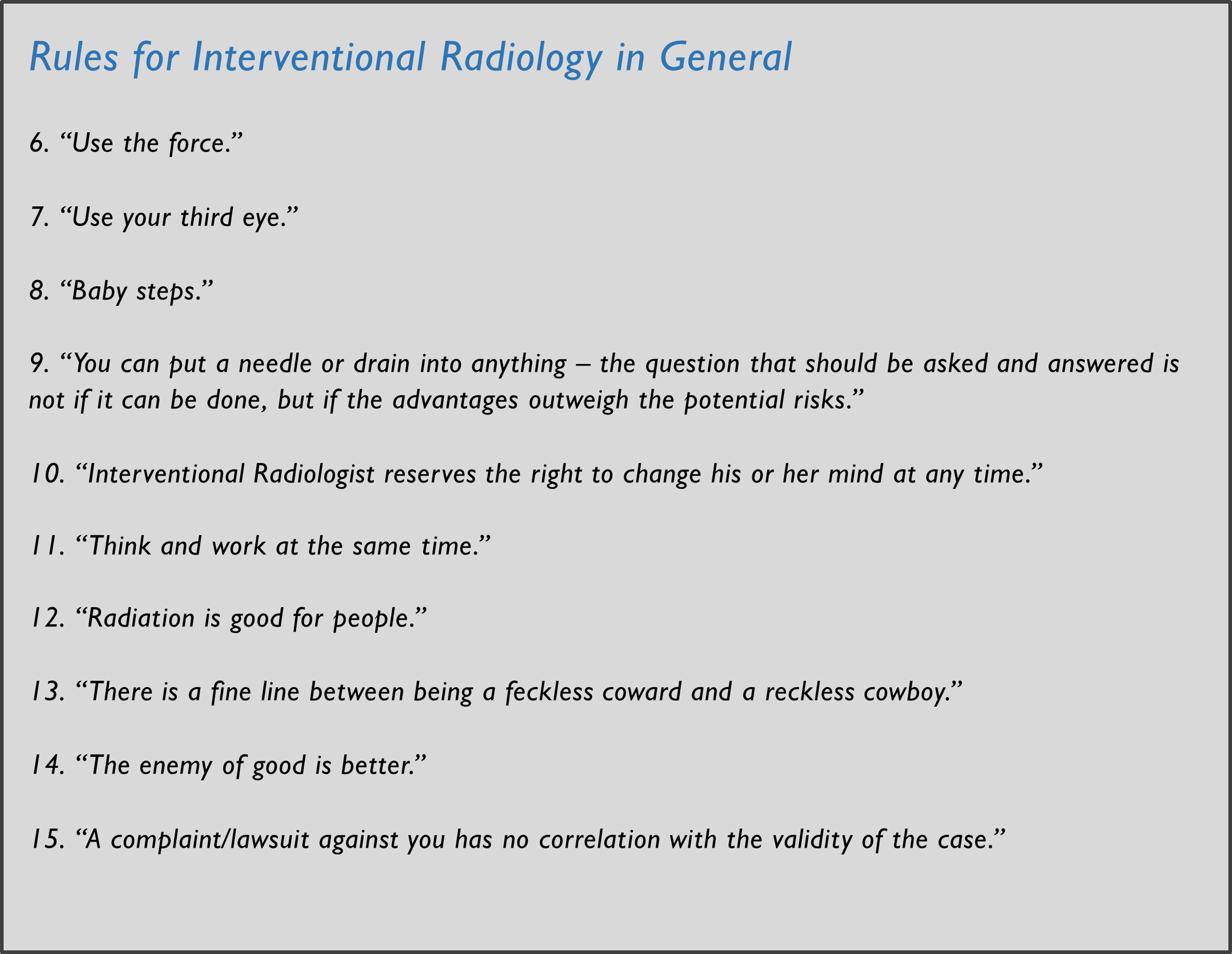
Rules for Interventional Radiology in General
In the original 1977 Star Wars movie Episode IV - A New Hope, 5 Luke is instructed to ‘Use the Force’ or trust his feelings during an important task by his mentor and Jedi Knight, Obi-Wan Kenobi. A similar instruction is often needed for IR trainees.
A reference to a mystical invisible inner eye or mind’s eye in various spiritual traditions, this is a call for Interventional Radiologists to mentally visualize the trajectory of their needle or catheter insertion.
A reminder that learning is often slow and occurs in a step-wise fashion (and also a reference to the 1991 comedy film, ‘What About Bob?’ 6 )
Decision-making in patient care is always in flux, dependent on new knowledge gleaned during the process. One need not apologize for asking for a different wire or catheter, for example, in the course of performing an IR procedure.
Of course as diagnostic imaging specialists, we adhere to the ALARA principle and minimize unnecessary exposure of patients (and healthcare workers) to ionizing radiation, but one should always keep in mind that our use of fluoroscopy and CT scanning is an integral component of the diagnostic and therapeutic procedures that provide a net health benefit to our patients.
Aim for balance, but err on the side of caution.
When a good result has already been achieved, think carefully before aiming for perfection as additional intervention could lead to complications and/or a worse result.
Continue to do the best that you can in caring for patients.
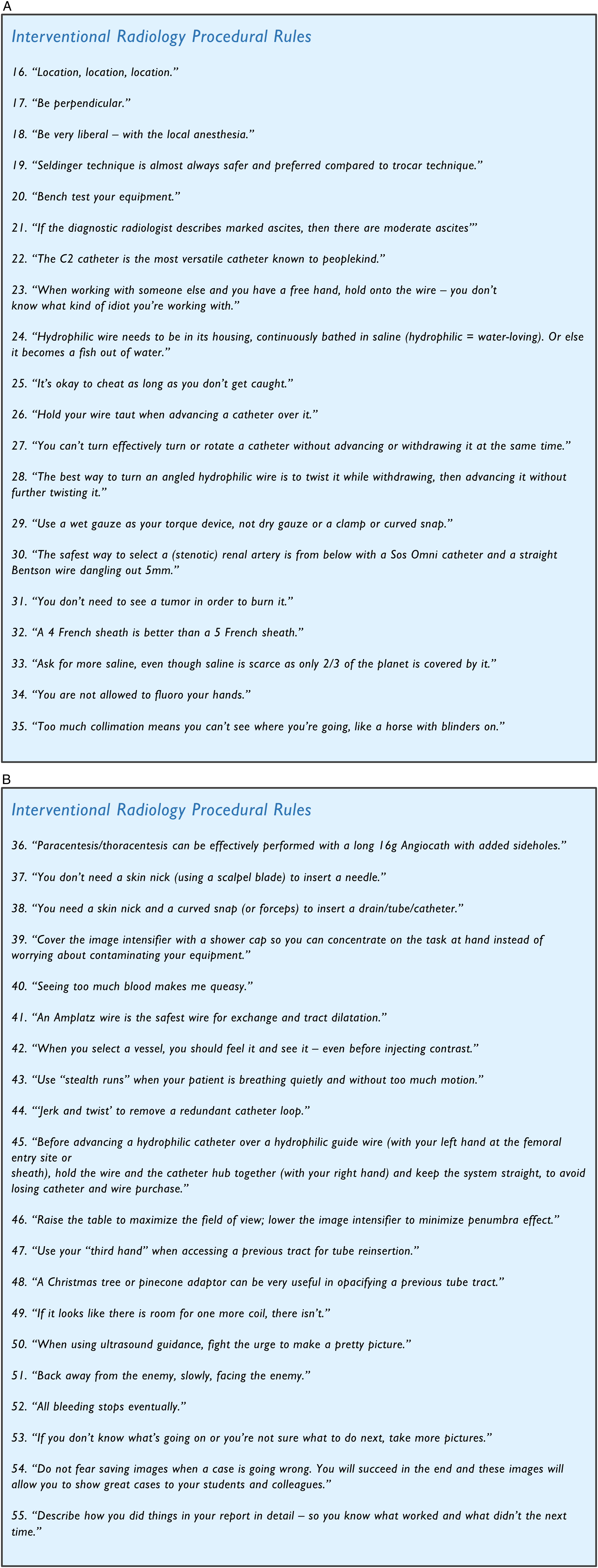
Interventional Radiology Procedural Rules
The 3 more important things in real estate are also the 3 most important considerations in starting many IR procedures. Time spent carefully selecting an entry site is often rewarded. A suboptimal catheter entry site, for instance, can make the procedure more difficult and prone to complications.
If one is not inserting a needle or tube perpendicular to the skin and tissue planes, one runs the risk of kinking a wire, buckling a wire and losing access.
Sven Ivar Seldinger, a Swedish radiologist, was the first to describe the technique that forms a major foundation of IR. 7 During an arteriographic intervention at Mount Sinai Hospital, an elective medical student who was shadowing me at the time asked me to explain to him the Seldinger technique. Instead, I instructed him to ‘look it up’ and explain it to me the next day. He came up with the best summary that I have heard for the technique in 5 simple steps: “Needle in, wire in, needle out, catheter in, wire out.” The student, Nicholas P. Plaskos, became a Radiologist.
It is safest to test and re-familiarize oneself with equipment on the procedure tray before entry into the patient’s body, for example, ensuring that the selected guiding cannula and coaxial biopsy needle are of appropriate and matching gauge and lengths.
Similarly, moderate ascites = mild ascites, and mild ascites = trace ascites.
A rule stated in jest to remind one to use all measures available to avoid losing access or purchase already gained.
And a fish out of water flops around and then can easily be lost.
This rule only refers to changing catheters, of course! Sometimes during catheter exchanges, the guide wire is slightly too short. Instead of switching to a longer wire, which would be the safest option but more time-consuming, one may be tempted to take a short cut and proceed with catheter exchange over the shorter wire. This can work without complication such as wire embolization or loss of access, but one should always keep in mind the corollary to this rule: ‘The problem with cheating is that eventually you will get caught.’
A dry gauze may be difficult to remove from an hyrdrophilic wire once a torque device is no longer needed. Use of a clamp does not transmit tactile information very well.
As one crosses the origin, the wire tip not infrequently flicks into the vessel. Knowledge gleaned from the teachings of renowned Interventional Radiologists Thomas A. Sos and Kenneth W. Sniderman.
In percutaneous ablation procedures such as radiofrequency or microwave ablation of liver or kidney tumours, one can use sonographic and/or CT landmarks to help guide needle electrode insertion, without clearly delineating the edges of the targeted lesion.
If an arterial intervention can be performed with a lower profile device, then potentially a complication such as puncture site haematoma or pseudoaneurysm may be less likely.
A sarcastic response in dealing with a pet peeve of mine (that the amount of saline provided on a procedural tray is often less than ideal). Corollary: ‘There are only 1.3 billion cubic kilometers of saline on planet Earth.’ 8
Although following this rule can make a procedure longer and more complicated, sufficient practice of this rule, including the generous use of last-image hold (LIH), can virtually eliminate the extra time spent avoiding self-radiation.
The most resistance to catheter insertion can be at the skin.
This rule serves as reminder to keep one’s work area (and patient) clean and tidy, and to keep stopcocks closed at the ends of catheters and tubes not currently being used for injection.
For some digital subtraction angiographic runs, a breath hold by the patient may not be required, for example, in pelvic arteriography.
During gastrojejunostomy tube insertion or change, for example, sometimes your exchange wire forms a loop, with the wire directed towards the fundus, first deflected against the lesser curvature and then coursing along the greater curvature, despite maintaining access to the duodenum/jejunum. This redundant loop in the stomach can be removed by exchanging for a 100cm-long 5–7 French catheter such as a multipurpose catheter, removing the wire and then jerking the catheter slightly outwards whilst twisting the catheter. In this manner, the redundant catheter loop can often be successfully removed while maintaining small bowel access.
When accessing a previous tube tract using a 4 or 5 French curved/directional catheter and an hydrophilic wire, backing out of the catheter tip is a common problem. Your left hand can also function as your third hand, in maintaining catheter access: squeeze the catheter at the skin exit site between the hypothenar eminence and the fourth and fifth fingers of your left hand, while holding the hub of the catheter between the thumb and index finger of your left hand (the catheter is looped externally), as your right hand directs the wire.
When a long-term indwelling catheter such as a nephrostomy or gastrostomy tube has fallen out completely, one often attempts to opacify the old tract with contrast as the initial step in tube replacement by probing the old exit site with a 4 or 5 French short directional catheter or dilator. This method may not necessarily reveal the pathway to the collecting system or gastric lumen, respectively, as injected contrast easily leaks out onto the skin. A Christmas-tree adaptor firmly lodged into the exit site can provide a better seal so that injected contrast may more easily reach its intended destination.
Towards the end of an embolization procedure, estimating that there is sufficient space for an additional embolic device such as an embolization coil is a common miscalculation leading to misembolization and necessitating an attempt at retrieval of the misplaced device.
The purpose of sonography during IR procedures is to guide it, and thus, it is different that for diagnostic imaging.
When performing embolization, to treat bleeding, for example, perform sequential angiograms as your catheter is withdrawn step-wise to less (super-)selective positions, to ensure that you do not miss another contributing branch.
Hopefully in conjunction with favourable patient outcome.
Footnotes
Acknowledgments
Dedicated to the many Interventional Radiology residents and fellows I have had the honour and pleasure of teaching.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.