
Abstract
The Canadian Association of Radiologists (CAR) Central Nervous System Expert Panel is made up of physicians from the disciplines of radiology, emergency medicine, neurosurgery, and neurology, a patient advisor, and an epidemiologist/guideline methodologist. After developing a list of 24 clinical/diagnostic scenarios, a rapid scoping review was undertaken to identify systematically produced referral guidelines that provide recommendations for one or more of these clinical/diagnostic scenarios. Recommendations from 55 guidelines and contextualization criteria in the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) for guidelines framework were used to develop 51 recommendation statements across the 24 scenarios. This guideline presents the methods of development and the referral recommendations for congenital disorders of the brain, cerebrovascular disease, multiple sclerosis and demyelinating disease, headache, concussion, pituitary and juxtasellar lesions, cranial neuropathy, brain stem symptoms, altered intracranial pressure (hypertension, hypotension, hydrocephalus suspected shunt malfunction, normal pressure hydrocephalus), vestibular and cochlear symptoms (hearing loss, vertigo), mental status change (acute, dementia/memory loss), visual loss, epilepsy and seizure, CNS infection, intracranial space-occupying lesions, suspected cerebral venous sinus thrombosis, vasculitis, movement disorders/Parkinsonism, metabolic and toxic encephalopathies, and aneurysm screening.
Introduction
Beginning in January 2024, an Expert Panel (EP) made up of physicians from the disciplines of radiology, emergency medicine, neurosurgery, neurology, and physiatry, a patient advisor, and an epidemiologist/guideline methodologist met to develop a new set of recommendations specific to referral pathways for central nervous system (CNS) conditions. Through discussion (via a virtual meeting) followed by offline communication, the EP developed a list of 24 clinical/diagnostic scenarios to be covered by this guideline. These recommendations are intended primarily for referring clinicians (eg, family physicians, specialty physicians, nurse practitioners); however, they may also be used by radiologists, individuals/patients, and patient representatives.
Our methods describing the guideline development process, including the rapid scoping review to identify the evidence base, has been published in CMAJ Open 1 and an editorial to this series of guideline publications is available in CARJ. 2 The application of well-established scoping review and rapid review guidance (JBI, 3 Cochrane Handbook, 4 Cochrane Rapid Review Methods Group 5 ) and guideline methodology (ie, Grading of Recommendations Assessment, Development, and Evaluation or GRADE6,7) were used to identify the evidence-base and to guide the Expert Panel in determining the strength and direction of the recommendations for each clinical scenario (Table 1). The quality of conduct and reporting of the included guidelines identified in the scoping review were evaluated with the AGREE-II checklist, 8 using a modified scoring system. In instances where guidelines were lacking, expert consensus was used to develop the recommendation. Contextualization to the Canadian health care system was considered for each recommendation, with discussion around the factors found in the Evidence to Decision framework in GRADE for guidelines (eg, balance of desirable and undesirable outcomes, values and preferences, resources implications). 7
Recommendation Text, Symbol, and Interpretation.
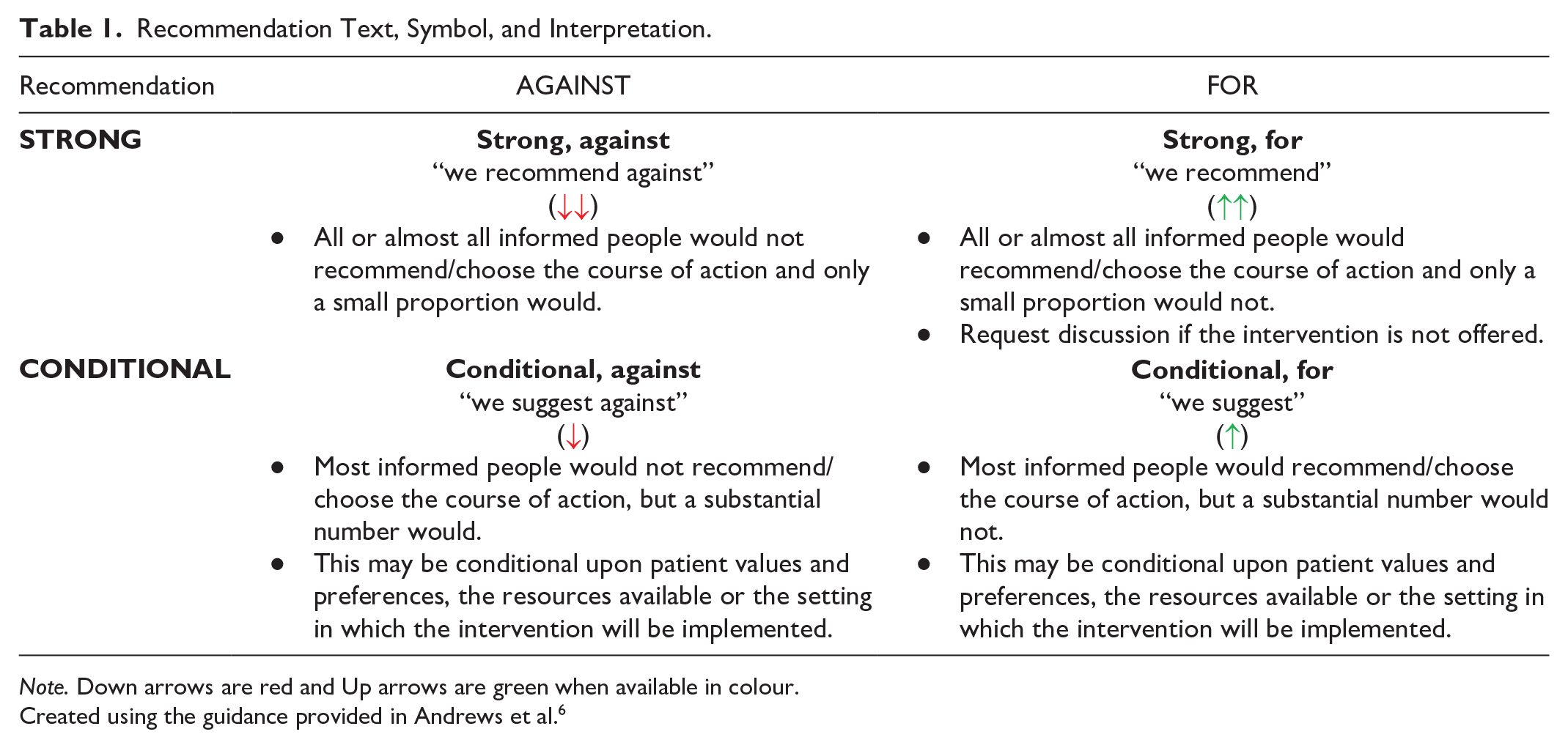
Note. Down arrows are red and Up arrows are green when available in colour.
Created using the guidance provided in Andrews et al. 6
A systematic search for guidelines (with an a priori defined inclusion criteria) was run in Medline and Embase on February 27, 2024. The search was limited to publications from 2019 onward (Supplemental Appendix 1). Supplemental searching included the following national radiology and/or guideline groups: the American College of Radiology, the National Institute for Health and Care Excellence, and the Royal College of Radiologists 8th Edition (2017). Recommendations for each clinical scenario were formulated over 2 virtual meetings on October 18 and 23, 2024. External review and feedback were obtained from radiologists, an emergency physician, and family physicians. The full guideline can be found on the CAR website (www.car.ca).
Results
Systematic Scoping Review
A total of 6737 records were identified through the electronic database and 17 additional records were added from the supplemental search. Fifty-five guidelines, plus 4 companion papers, were included (Figure 1). Potentially relevant guidelines published in languages other than English can be found in Supplemental Appendix 2. A list of excluded records with justifications for exclusion is available upon request. Most guidelines were rated as moderate or high quality, using the modified AGREE-II checklist 8 (Supplemental Appendix 3). The number of guidelines included per clinical/diagnostic scenario ranged from 0 to 16, with a median of 3 guidelines per clinical scenario.
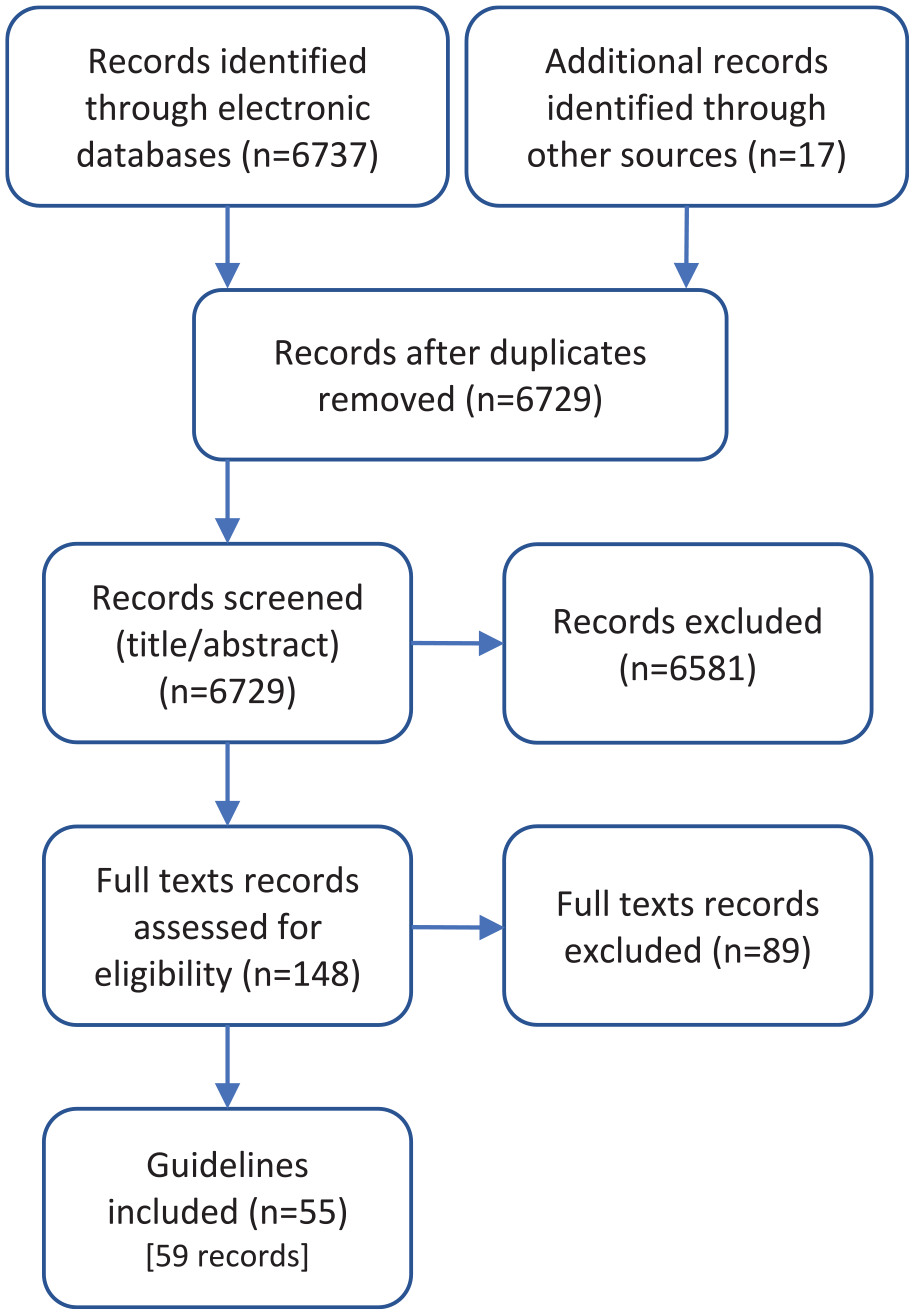
PRISMA flow diagram.
Recommendations
Additional details of the included guidelines, including which imaging modalities (eg, computed tomography [CT], magnetic resonance imaging [MRI], radiograph [XR], ultrasound [US]) that were discussed can be found in Supplemental Appendix 4.
A guideline is intended to guide and not be an absolute rule. Medical care is complex and should be based on evidence, a clinician’s expert judgment, the patient’s circumstances, values, preferences, and resource availability. Not all imaging modalities are available in all clinical environments, particularly in rural or remote areas of Canada. Decisions about patient transfer, use of alternative imaging or serial clinical examination and observation can be complex and difficult. Therefore, the expected benefits of recommended imaging, risks of travel, patient preference, and other factors must be considered. The guideline recommendations are designed to assist the choice of imaging modality in situations where it is deemed clinically necessary to obtain imaging.
Unless the panel agreed a specific protocol is required to optimize patient care/diagnosis, the recommendations do not specify when contrast should or should not be used, as this decision may vary based on clinical presentation, regional practice preferences, preference of the referring clinician, radiologist and/or the patient, and resource availability.
We reviewed relevant recommendations related to the 24 clinical/diagnostic scenarios previously published by radiology and specialty societies, including: the Canadian Association of Radiologists, 9 the American Association of Neurological Surgeons and the Congress of Neurological Surgeons, 10 the American College of Radiology,11-20 the American Headache Society, 21 the American Heart Association/American Stroke Association,22,23 British Society of Rheumatology,24,25 the British Society for Haematology, 26 the Canadian Consensus Conference guideline, 27 the Canadian Parkinson’s Disease guideline, 28 the Canadian Stroke Consortium, 29 the Canadian Stroke Best Practice, 30 the Chinese Hepatic Encephalopathy guideline, 31 the Chinese Neurosurgical Society of the Chinese Medical Association/Society of Hematological Malignancies of the Chinese Anti-Cancer Association, 32 the Chinese Stroke Association,33-35 the European Academy of Neurology,36,37 the European Academy of Neurology/Peripheral Nerve Society,38,39 the European Alliance of Associations for Rheumatology, 40 the European Association of Neuro-Oncology,41-43 the European Association of Neuro-Oncology and the European Society for Medical Oncology, 44 European Association for the Study of the Liver, 45 the European Society of Clinical Microbiology and Infectious Diseases, 46 the European Stroke Organization,47,48 the Italian Society of Neurosurgery, Italian Association of Neuro-Oncology, and Italian Association of Neurology, 49 the Japanese Society of Normal Pressure Hydrocephalus, 50 the Japan Stroke Society, 51 the Japanese National Research Committee, 52 the Meniere’s disease guideline,53,54 the Multidisciplinary Specialists Interest Group, 55 the National Institute for Health and Care Excellence,56-63 the Society of NeuroInterventional Surgery, 64 the Sudden Hearing Loss guideline,65,66 and the Swedish Society of Rheumatology. 67
Recommendations are presented in Table 2.
Central Nervous System Recommendations.
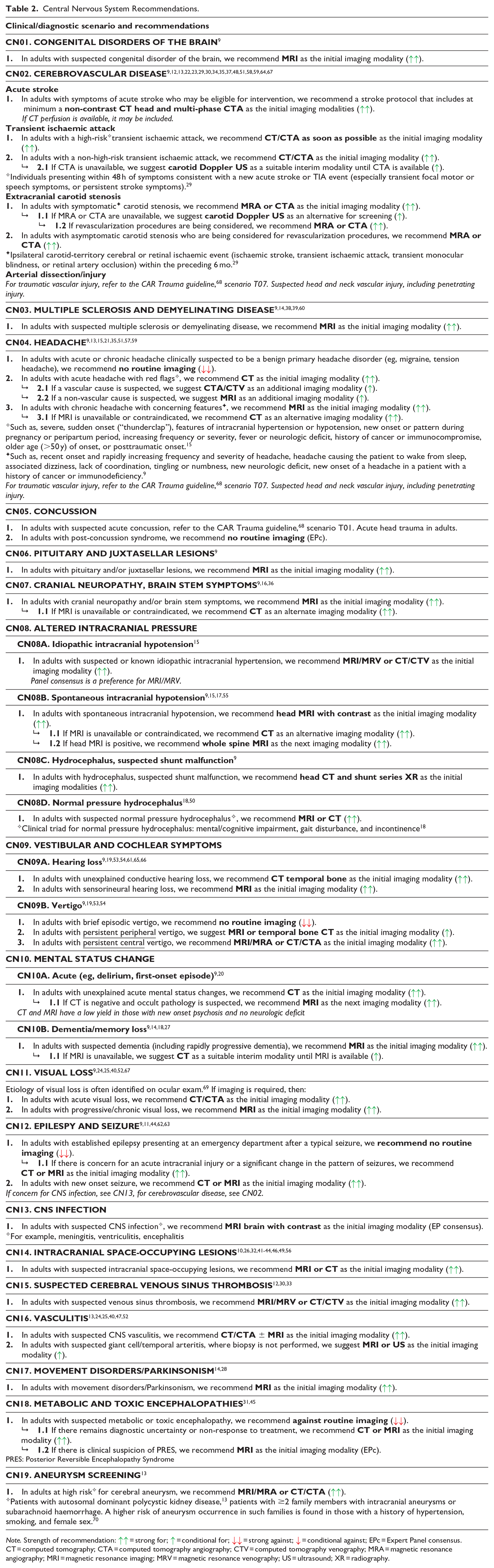
Note. Strength of recommendation:
Supplemental Material
sj-pdf-1-caj-10.1177_08465371241311247 – Supplemental material for Canadian Association of Radiologists Central Nervous System Diagnostic Imaging Referral Guideline
Supplemental material, sj-pdf-1-caj-10.1177_08465371241311247 for Canadian Association of Radiologists Central Nervous System Diagnostic Imaging Referral Guideline by Candyce Hamel, Barb Avard, Nicolas Dea, Ryan Margau, Andrew Mattar, Alan Michaud, Matthias Schmidt, David Volders, Christopher Witiw, James Worrall and Amanda Murphy in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
We would like to thank: Becky Skidmore for creating the search strategies for the systematic scoping review, and the following individuals on the Diagnostic Imaging Referral Guidelines Working Group and external stakeholders for providing feedback on the guideline (listed alphabetically): Noel Corser, Cathy MacLean, Paul Pageau, and Kaitlin Zaki-Metias.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Medical Association.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.