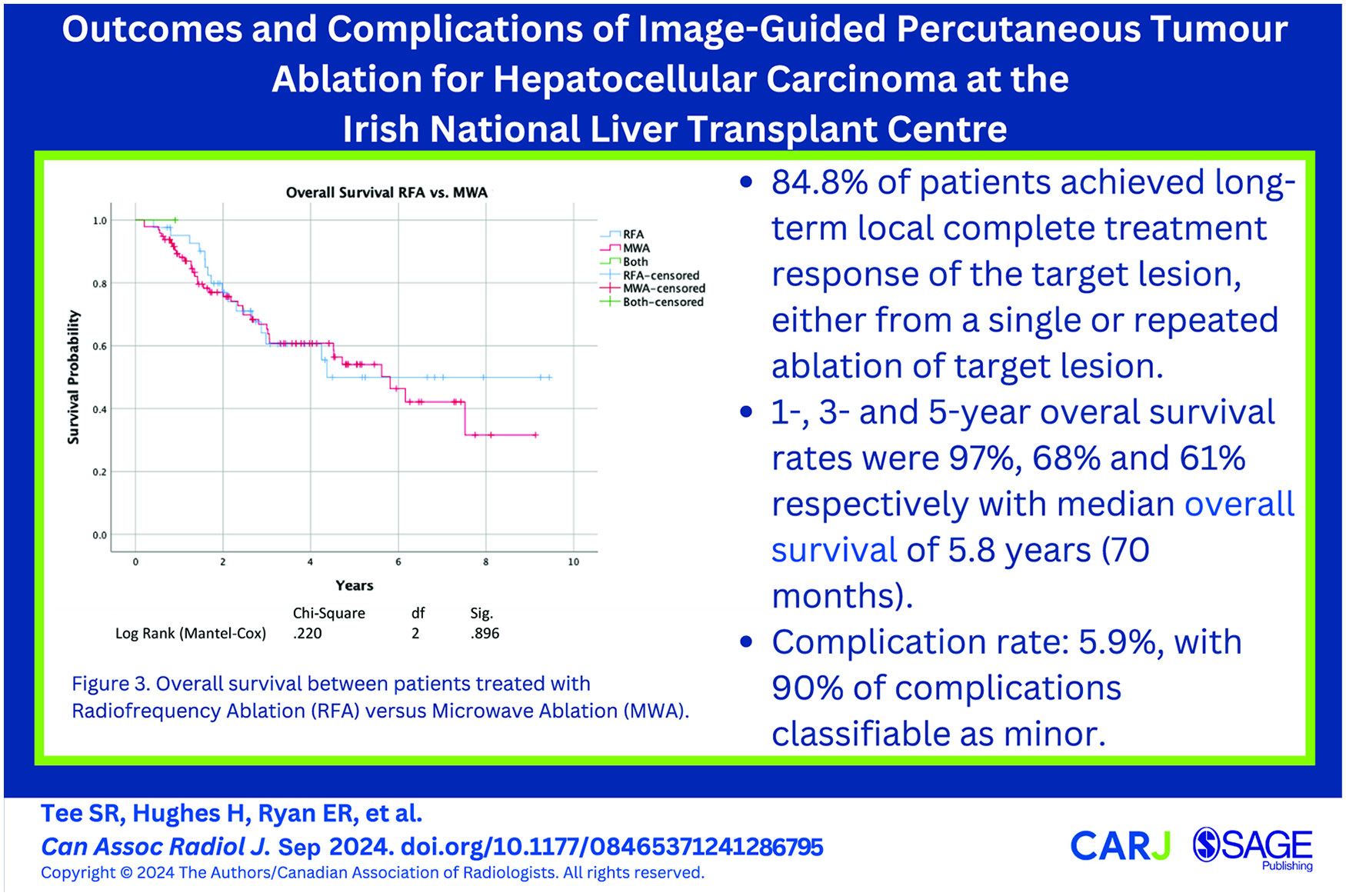
Background: Image-guided tumour ablation is a minimally invasive treatment for early stage hepatocellular carcinoma (HCC). Our study reviews the complications and long term outcomes in patients treated at a tertiary referral centre. Methods: Retrospective study. All patients with HCC who underwent microwave ablation (MWA) or radiofrequency ablation (RFA) from 1st January 2014 to 31st December 2022 were identified. Treatment response of target lesion, complications, and survival were recorded. Results: One hundred seventy ablations were performed in 118 patients; 70% MWA, 30% RFA. Median radiological follow-up 21 months (range 3-107). Follow-up imaging was reported using LI-RADS and mRECIST. At first follow-up imaging, 94 patients had complete response (primary efficacy rate 80.3%) while 19.7% (n = 23) had residual disease. Fifteen of these had repeat ablation; 10 had complete response (secondary efficacy rate 85.6%). By end of study duration, 70.5% (n = 79) achieved sustained local complete response from single ablation without documented recurrence. 14.3% (n = 16) required more than one ablation of target lesion. Overall, 84.8% (n = 95) demonstrated long term local complete response to ablation. Complication occurred in 5.9% (n = 10); 40.0% Grade I, 40.0% Grade II, 10.0% Grade III, 10.0% Grade IV as per the CIRSE Classification. 1-, 3-, and 5-year overall survival (OS) rate was 97%, 68%, and 61% respectively. Mean OS was 5.3 years (median 4.7). No difference in OS (P = .7) or local progression free survival (P = .5) between patients treated with MWA versus RFA. Conclusion: This study demonstrates excellent long-term response to TA, with acceptable complication profile. No difference in survival between RFA versus MWA.
Ahrens-IwersLJVJanssenMTeeSRMeissnerRH. ELECTRODE: an electrochemistry package for atomistic simulations. J Chem Phys. 2022;157(8):084801.
2.
RumgayHArnoldMFerlayJ, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598-1606.
3.
ReigMFornerARimolaJ, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681-693.
4.
MajumdarARoccarinaDThorburnDDavidsonBRTsochatzisEGurusamyKS. Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis. Cochrane Database Syst Rev. 2017;3(3):CD011650.
5.
WangYLuoQLiYDengSWeiSLiX. Radiofrequency ablation versus hepatic resection for small hepatocellular carcinomas: a meta-analysis of randomized and nonrandomized controlled trials. PLoS One. 2014;9(1):e84484.
6.
KimYSLimHKRhimH, et al. Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: analysis of prognostic factors. J Hepatol. 2013;58(1):89-97.
7.
ShiinaSTateishiRAranoT, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012;107(4):569-577; quiz 578.
8.
BertotLCSatoMTateishiRYoshidaHKoikeK. Mortality and complication rates of percutaneous ablative techniques for the treatment of liver tumors: a systematic review. Eur Radiol. 2011;21(12):2584-2596.
9.
TanWDengQLinSWangYXuG. Comparison of microwave ablation and radiofrequency ablation for hepatocellular carcinoma: a systematic review and meta-analysis. Int J Hyperthermia. 2019;36(1):264-272.
10.
FilippiadisDKBinkertCPellerinOHoffmannRTKrajinaAPereiraPL. Cirse quality assurance document and standards for classification of complications: the Cirse classification system. Cardiovasc Intervent Radiol. 2017;40(8):1141-1146.
11.
ChernyakVFowlerKJKamayaA, et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology. 2018;289(3):816-830.
MazzaferroVBattistonCPerroneS, et al. Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg. 2004;240(5):900-909.
14.
WangTLuXJChiJC, et al. Microwave ablation of hepatocellular carcinoma as first-line treatment: long term outcomes and prognostic factors in 221 patients. Sci Rep. 2016;6:32728.
15.
HanKKimJHKimGH, et al. Radiofrequency ablation of subcapsular versus nonsubcapsular hepatocellular carcinomas ≤ 3 cm: analysis of long-term outcomes from two large-volume liver centers. Eur Radiol. 2024;34(3):1578-1586.
16.
LuDSYuNCRamanSS, et al. Radiofrequency ablation of hepatocellular carcinoma: treatment success as defined by histologic examination of the explanted liver. Radiology. 2005;234(3):954-960.
17.
Serbanescu-Kele Apor de ZalanCMCRuiterSJSvan den BergAPPenningsJPde JongKP. Outcomes after primary and repeat thermal ablation of hepatocellular carcinoma with or without liver transplantation. Eur Radiol. 2022;32(6):4168-4176.
18.
De MuzioFCutoloCDell’AversanaF, et al. Complications after thermal ablation of hepatocellular carcinoma and liver metastases: imaging findings. Diagnostics (Basel). 2022;12(5):1151.
19.
WeiQXiongSLuoWLiangMLuoB. Thermal ablation versus liver resection for hepatocellular carcinoma in patients with cirrhosis: a systematic review and meta-analysis of propensity-score matched studies. Clin Exp Med. 2024;24(1):32.
20.
BaiXMCuiMYangW, et al. The 10-year survival analysis of radiofrequency ablation for solitary hepatocellular carcinoma 5 cm or smaller: primary versus recurrent HCC. Radiology. 2021;300(2):458-469.
21.
ZhengHXuCWangX, et al. Microwave ablation shows similar survival outcomes compared with surgical resection for hepatocellular carcinoma between 3 and 5 cm. Int J Hyperthermia. 2020;37(1):1345-1353.
22.
HuoYREslickGD. Microwave ablation compared to radiofrequency ablation for hepatic lesions: a meta-analysis. J Vasc Interv Radiol. 2015;26(8):1139-1146.e2.
23.
YuJYuXLHanZY, et al. Percutaneous cooled-probe microwave versus radiofrequency ablation in early-stage hepatocellular carcinoma: a phase III randomised controlled trial. Gut. 2017;66(6):1172-1173.
24.
TanakaTTakataKMiyayamaT, et al. Long-term outcome and eligibility of radiofrequency ablation for hepatocellular carcinoma over 3.0 cm in diameter. Sci Rep. 2023;13(1):16286.
25.
ImamuraHMatsuyamaYTanakaE, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200-207.
26.
TabrizianPJibaraGShragerBSchwartzMRoayaieS. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947-955.
27.
JiaJBZhangDLudwigJMKimHS. Radiofrequency ablation versus resection for hepatocellular carcinoma in patients with Child-Pugh A liver cirrhosis: a meta-analysis. Clin Radiol. 2017;72(12):1066-1075.
28.
JooIMorrowKWRamanSSMcWilliamsJPSayreJWLuDS. CT-monitored minimal ablative margin control in single-session microwave ablation of liver tumors: an effective strategy for local tumor control. Eur Radiol. 2022;32(9):6327-6335.
29.
AnCLiXZhangM, et al. 3D visualization ablation planning system assisted microwave ablation for hepatocellular carcinoma (Diameter >3): a precise clinical application. BMC Cancer. 2020;20(1):44.
30.
RaiPAnsariMYWarfaM, et al. Efficacy of fusion imaging for immediate post-ablation assessment of malignant liver neoplasms: a systematic review. Cancer Med. 2023;12(13):14225-14251.
31.
SolbiatiMMugliaRGoldbergSN, et al. A novel software platform for volumetric assessment of ablation completeness. Int J Hyperthermia. 2019;36(1):337-343.
32.
ReinhardtMBrandmaierPSeiderD, et al. A prospective development study of software-guided radio-frequency ablation of primary and secondary liver tumors: clinical intervention modelling, planning and proof for ablation cancer treatment (ClinicIMPPACT). Contemp Clin Trials Commun. 2017;8:25-32.
33.
van AmerongenMJMariappanPVoglreiterP, et al. Software-based planning of ultrasound and CT-guided percutaneous radiofrequency ablation in hepatic tumors. Int J Comput Assist Radiol Surg. 2021;16(6):1051-1057.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.