
Abstract
Introduction
Patients with pancreatic ductal adenocarcinoma (PDAC) have poor 5-year survival despite curative-intent resection. 1 Given the aggressiveness of PDAC, and the requirement for complete resection for cure, it seems intuitive that patients with PDAC with potentially resectable disease would benefit from proceeding to resection as soon as possible. However, prior research has not shown this, possibly due to limited sample size and exploration of wait time as a categorical variable.2-5 The purpose of this study was to determine if wait time from pre-operative computed tomography (CT) to pancreatectomy impacts overall survival using a provincial cohort of patients with PDAC.
Methods
All adult patients in Ontario, Canada who underwent pancreatectomy for PDAC between January 2011 and December 2022 were identified via linked provincial administrative datasets, using previously described inclusion and exclusion criteria. 6 These datasets were linked using unique encoded identifiers and analyzed at the Institute for Clinical Evaluative Sciences. All pancreatectomy types were eligible. The most recent pre-operative CT prior to pancreatectomy was used as this most likely informed surgical management, with wait time documented as number of days between CT and pancreatectomy, up to 90 days. Patients who died within 30 days following surgery were excluded due to the likelihood of post-surgical complication. Patients were followed until the first occurrence of all-cause mortality (primary outcome), 5 years following pancreatectomy, loss of provincial health insurance coverage, or March 31, 2023. We computed hazard ratios to quantify the relationship of wait time between pre-operative CT, surgery and all-cause mortality, while adjusting for age, time elapsed between PDAC diagnosis and surgery, Charlson comorbidity index, neighbourhood income quintile, distance between home and surgical centre, receipt of pre-operative abdominal MRI, cancer stage, pancreaticoduodenectomy versus other pancreatectomy type, and adjuvant chemotherapy in a Cox proportional hazards model with significance defined as P < .05. Covariates selected via backward elimination.
Results
A total of 3888 patients were identified (2078 men, 1810 women, age range 23-94 years), including 1071 patients who died within 1-year post-pancreatectomy and 2817 who survived. Median wait time from pre-operative CT to surgery was 29 days (range 0-90 days). The mortality rate per 1000 person-years differed between 427 patients who waited ≤7 days (313, 95%CI: 279-351), 1569 patients who waited 8 to 30 days (338, 95%CI: 318-358), and 1892 patients who waited 31 to 90 days (265, 95%CI: 250-281), P < .0001. With each 5-day increase in wait time between pre-operative CT and pancreatectomy, the rate of all-cause mortality decreased by 1.4% (HR 0.986 [95%CI: 0.976-0.996]), Table 1.
Patient Characteristics and Adjusted Hazard Ratios for All-Cause Mortality.
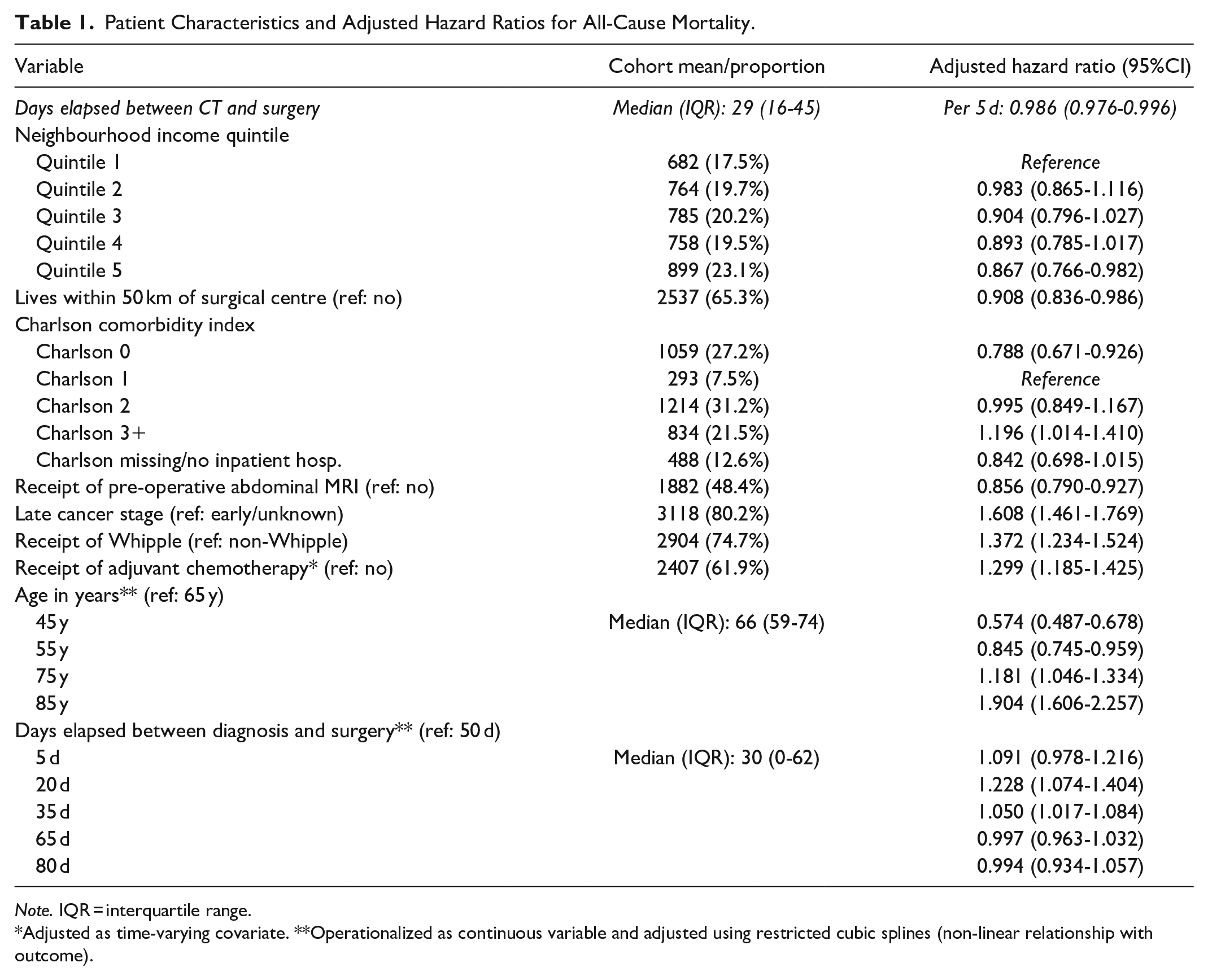
Note. IQR = interquartile range.
Adjusted as time-varying covariate. **Operationalized as continuous variable and adjusted using restricted cubic splines (non-linear relationship with outcome).
Discussion
Longer wait time between pre-operative CT and pancreatectomy for PDAC was associated with improved overall survival. This could be due to patients with relatively more aggressive PDAC or other comorbidities proceeding to the operating room sooner, triaging of patients with less aggressive PDAC to later operation dates, a combination of each, or other factors. Aspects of PDAC aggressiveness including tumour grade could not be determined, and cancer stage was unknown for many patients which may have limited our ability to adjust for disease aggressiveness. Future research would benefit from prospective data collection and a more detailed data source providing pre-operative imaging, clinical and surgical report content. It remains unclear if time from CT to pancreatectomy impacts survival for patients with PDAC.
Disclosures
Parts of this material is based on data and/or information compiled and provided by Ontario Health, Canadian Institute for Health Information, and the Ontario Ministry of Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Footnotes
Acknowledgements
This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care.