
Abstract
This is a visual representation of the abstract.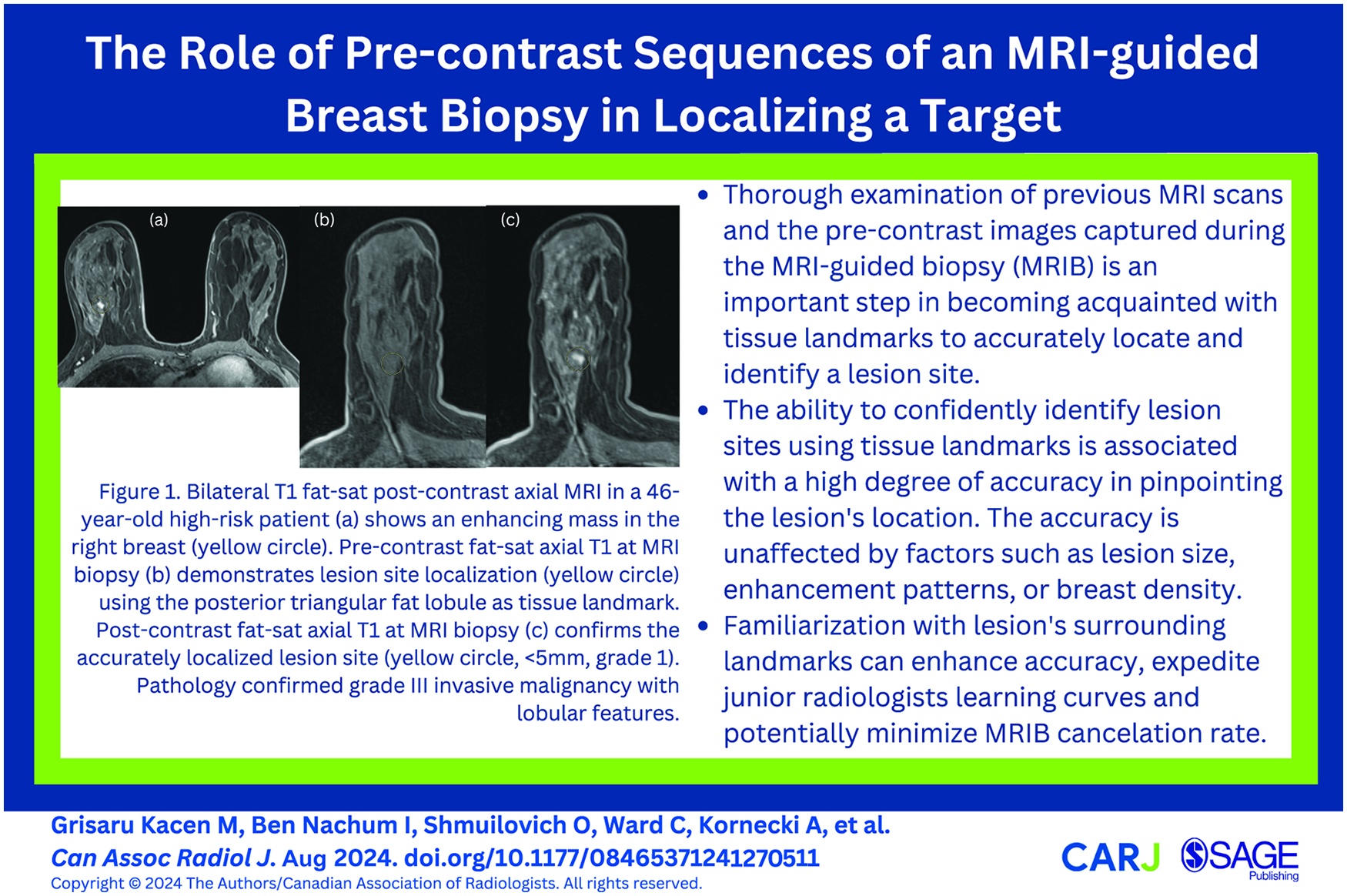
Introduction
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is the most sensitive imaging modality for the detection of breast cancer.1-3 Suspicious breast lesions detected only by DCE-MRI are usually biopsied under magnetic resonance imaging (MRI) guidance, and histopathology results yield a cancer diagnosis in approximately 25% to 61% of cases.4-6 While MRI-guided biopsy (MRIB) has been proven to be a safe and effective method, a significant challenge presents itself when a suspicious breast MRI finding is not well-visualized at the time of MRIB which may lead to biopsy cancellation. 7 In fact, the reported cancellation rate of MRIB ranges between 5% and 17%8-15 with the most common reason being lesion non-visualization at the time of biopsy. 10 About 28% of the lesions for which their biopsies were cancelled due to non-visualization have been reported to still be visible on follow-up MRI, and up to 10% of the lesions for which tissue sample was made available through surgery were found to be malignant.8-15 This highlights the fact that the absence of lesion visualization does not necessarily indicate that the lesion has resolved, nor does it exclude the presence of malignancy.
Brennan et al 14 reported that the cancellation rate of MRIB was the highest in the first year of radiologists’ practice at 14%, with a 50% rate reduction in subsequent years. We hypothesize that this drop likely reflects a learning curve for recognizing tissue landmarks in lesion localization. The lesion location, morphology, surrounding tissue configuration, presence of cysts, scars, surgical clips, or tissue markers, are all presumed to help identify a lesion site. The identification of these landmarks might help more experienced radiologists avoid biopsy cancellations, even when the lesion is sub-optimally visualized. Believing that the review of the pre-contrast images plays an important role in completion of an accurate biopsy, we designed this study to explore the rate at which radiologists feel confident in identifying the lesion site before contrast is administered. We then wanted to examine radiologist accuracy in identifying a lesion location when they were confident. In this article, we report on a retrospective study conducted to assess the ability of radiologists to accurately identify lesion site on the pre-contrast images of an MRIB exam while blinded to the post-contrast images.
Material and Methods
Ethical approval to conduct this single site study was obtained and informed consent was waived. A retrospective study was performed according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 16 The charts of 192 consecutive MRIB procedures obtained between January 2018 and December 2020 were reviewed. Inclusion criteria included availability of a prior bilateral MRI exam and at least one follow-up breast MRI at 6 months for benign or high-risk lesions, or surgical pathology results. Exclusion criteria included patients with a prior DCE-MRI exam performed at a different institution (due to differences in study protocols), patients who had MRIB following contrast-enhanced mammography without a baseline MRI, and those with cancelled MRIB.
Patient age, breast density category (ACR BI-RADS® Atlas Fifth Edition), 17 lesion enhancement morphology, biopsy positioning (unilateral vs simultaneous bilateral biopsy), histopathology, lesion size, and follow-up MRI descriptive data points were collected and entered into a computerized spreadsheet, Microsoft Excel 365.
Prior reference bilateral breast MRI exams were performed with the patients lying in the prone position, using a SIEMENS MAGNETOM Aera 1.5Т system and a 16-channel AI Breast Coil. Standard imaging protocol included a localizing sequence followed by axial and sagittal T2-weighted fat-suppressed, T1-weighted non–fat-suppressed, and bilateral T1-weighted axial fat-suppressed sequences before and at least 3 times after a rapid bolus intravenous injection of Gadovist® 1.0, 0.3 mmol/kg body weight, at 3 mL/s. The section thickness was 1 mm. The post-processing images were obtained using DynaCAD for Breast (DC; Invivo, Gainesville, FL).
The biopsies were performed by breast imaging radiologists with 1 to 13 years of experience utilizing a dedicated coil and an Invivo Sentinelle MR 1.5T Breast Imaging Table. Imaging was performed with all patients in prone position using a dedicated breast compression coil. The standard imaging protocol used for biopsy included a localizing sequence followed by at least one axial fat-suppressed T1-weighted sequence performed before and after contrast injection. The section thickness was 1 mm. Processed images and coordinates were calculated through DynaCAD for Breast (DC; Invivo, Gainesville, FL) and were only available at the time of the biopsy but were not saved on PACS. All MRI-guided biopsies were performed with a 9-gauge (standard or petite size needle) vacuum-assisted biopsy device (VAB-ATEC; Suros Division of Hologic, Indianapolis, IN). Minimum of 12 samples were obtained.
Reader Image Evaluations
Three radiologists (A, B, and C) with 10 to 13 years of experience in breast imaging and MRI-guided biopsies independently reviewed all patients’ exams retrospectively. The radiologists had access to the prior reference breast MRI exam including pre- and post-contrast images, and to the pre-contrast axial and sagittal images taken at the time of the biopsy. The reviewers were tasked with identifying the site of each lesion of interest on the pre-contrast axial MRIB images based on tissue landmarks, while being blind to the post-contrast MRIB images, biopsy results, patient medical records, and assessment of the other reviewers. The reviewers were asked to rate their level of confidence in identifying the lesion site by marking the images with different symbols; Level I was assigned when the site was identified with high confidence (marked with a circle; Figure 1), Level II when the site was identified with low confidence (marked with an arrow), and Level III when the site could not be identified (marked with a “?”). For level III confidence, the reviewers were asked to estimate the location of the lesion and place the symbol on the approximate expected lesion site. Marked-up images were saved as key images on PACS on the axial plane. The radiologists were asked to place the centre of the symbols at the centre of the expected lesion site. Symbol sizes were not specified.
Subsequently, a fourth radiologist with 3 years’ experience in breast imaging compared the key images with the post-contrast MRIB images and site of the actual biopsied lesions as well as post biopsy pathology report. The fourth radiologist then graded the accuracy of lesion site localization. Accurate localization was defined when the symbol centre was placed within ≤5 mm radius from the actual biopsy site (Grade 1; Figures 1 and 2). Inaccurate lesion localization was assigned if the symbol centre was placed between 5 and 10 mm radius (Grade 2) or a >10 mm radius (Grade 3) from the biopsied site (Figure 3). We determined 5 mm as a reasonable threshold to define accuracy as the standard of care is using vacuum-assisted biopsy, where large samples are taken with a 9-gauge needle with an inner diameter of 3.8 mm.
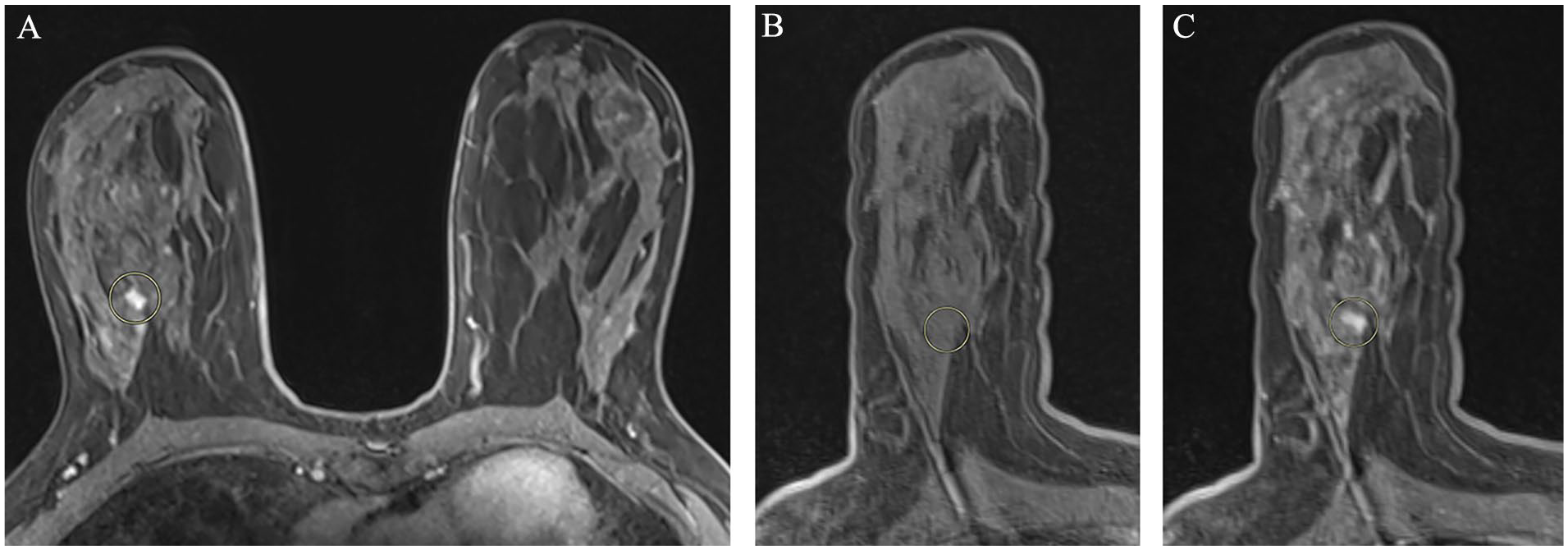
Bilateral T1 fat-sat post contrast axial MRI image (A) obtained for routine screening in a 46-year-old patient at high risk, demonstrates developing enhancing mass within the right upper outer quadrant (yellow circle). Pre-contrast fat-sat axial T1 sequence obtained at the time of MRI biopsy (B). Lesion site was localized with a high level of confidence. The reviewer used a triangular shaped fat lobule that was seen posterior the lesion as a landmark, in order to identify the lesion site (yellow circle). Post-contrast fat-sat axial T1 sequence obtained at the time of MRI biopsy (C), demonstrates the enhancing lesion corresponding to the site marked by the reviewer (yellow circle). Lesion site localization was accurate in this case (<5 mm, grade 1). Pathology results confirmed grade III invasive malignancy with lobular features.
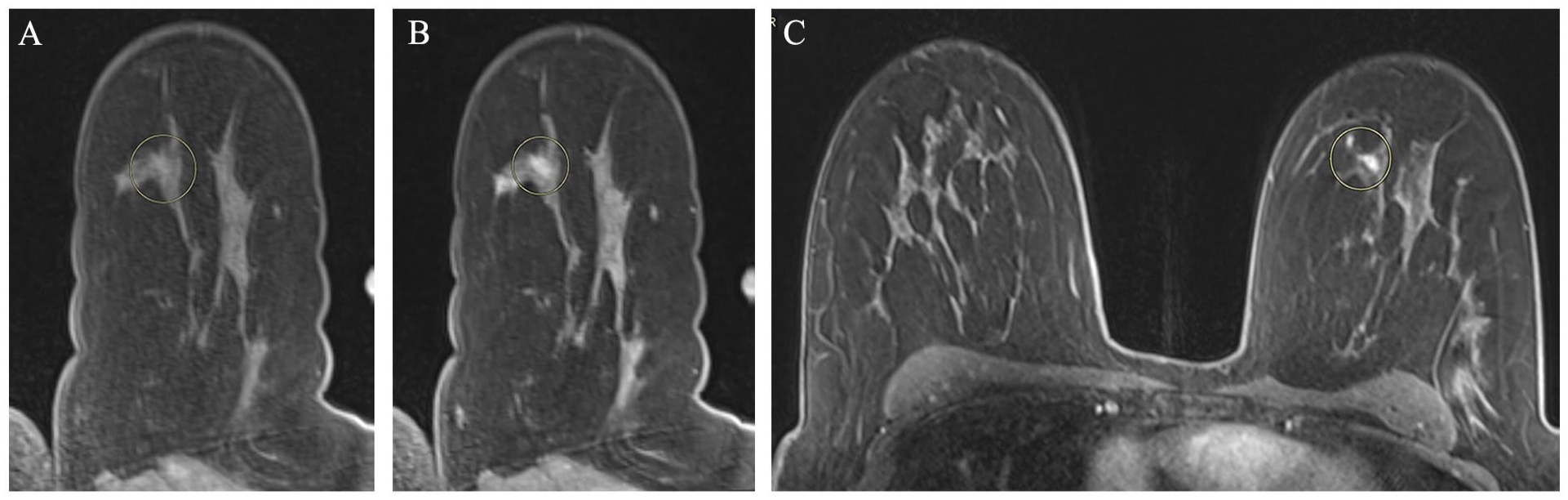
Pre- and post-contrast T1 fat-sat MRI images obtained at the time of biopsy (A and B respectively) in a 46-year-old patient at high risk. Image (A) demonstrates the reviewer’s marker (yellow circle) placed with a high level of confidence. The post-contrast image (B) was used by the fourth radiologists as reference to grade the accuracy. In this case the lesion site was detected with grade 1 accuracy (<5 mm). The reviewer used the configuration of fibroglandular tissue surrounded by fat as a landmark in order to identify the lesion site. The bilateral T1 fat-sat post contrast axial MRI image (C) used as reference, demonstrates the target lesion marked with a yellow circle. Pathology results confirmed grade III invasive malignancy.
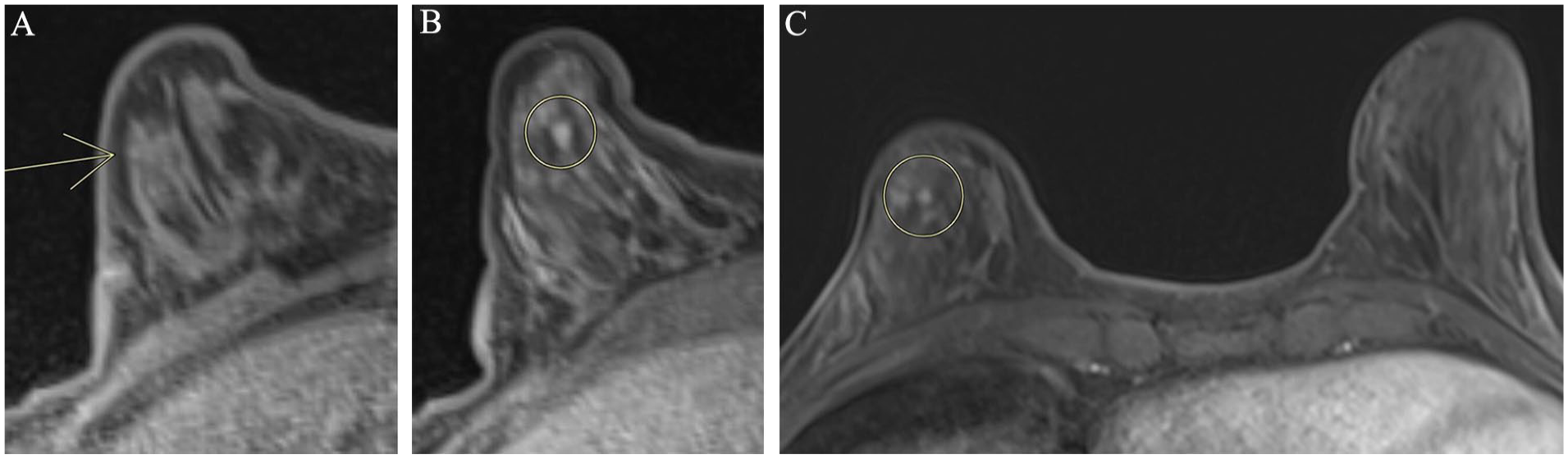
A 48-year-old patient at high risk who was positioned for bilateral MRI guided biopsy. Pre and post contrast T1 fat-sat MRI images ((A) and (B) respectively). Image (A) demonstrates the reviewer’s marker placed on the right breast with low level of confidence (yellow arrow). Post-contrast image (B) demonstrates the actual lesion site (yellow circle). The bilateral T1 fat-sat post contrast axial MRI image (C) obtained at time of routine screening was used as reference. The target lesion is seen within the right breast marked with a yellow circle. The lesion site detection graded as inaccurate in this case (>10 mm, grade 3). This example highlights the potential difficulty in identifying a lesion site when specific landmarks, such as fat lobes, cysts, or scars, are missing. Pathology results showed ductal carcinoma in situ (DCIS).
Statistical Analysis
All analyses were conducted using SPSS (V27; copyright IBM, 2020). When relations between dichotomous variables were being analyzed, cross-tabulation tables were constructed and analyzed using the Chi-square statistic. Dichotomous variables were tabulated and presented in table form when applicable, whereas continuous variables were reported using means, standard deviations, and standard error of the mean. All statistical analyses were considered significant when the probability of a Type 1 error was observed to be less than .05 (P < .05). Descriptive statistical analysis was used to calculate the percentage of confidence and accuracy category for each reviewer.
Results
Out of the 192 patients, 8 patients had MRIB following contrast-enhanced mammography without baseline MRI, 2 patients had their reference MRI in a different institution, 2 patients were lost to follow-up, and 6 patients in whom MRIB was cancelled were excluded from the trial. A total of 174 female patients with 181 biopsied breast lesions were eligible for the study. The ages of the participants ranged from 25 to 79 years (mean 55 years, median 51 years). Unilateral biopsy was performed in 164 out of the 174 patients. In 10/174 patients who were positioned for bilateral biopsy, biopsy was completed in 17/20 lesions (biopsies of 3 lesions were cancelled). Lesion sizes ranged between 3 and 43 mm (mean 18 mm, median 8 mm). Breast density category was fatty (A) in 6% (11/181) of patients, scattered (B) in 32% (59/181), heterogenous (C) in 49% (88/181), and extremely dense (D) in 13% (23/181) of patients. Most lesions (62% 113/181) presented as a non-mass enhancement (NME). The remaining lesions presented as masses (25%, 45/181) and enhancing foci (13%, 23/181). The majority (77%, 139/181) of patients had their prior MRI for routine surveillance, with 36% (65/181) having a lifetime risk of over 25% for developing breast malignancy and 41% (74/181) at intermediate risk with dense breasts. The remaining 23% (42/181) of patients underwent diagnostic MRI, typically for breast cancer staging.
Reviewer Level of Confidence and Their Grades of Accuracy
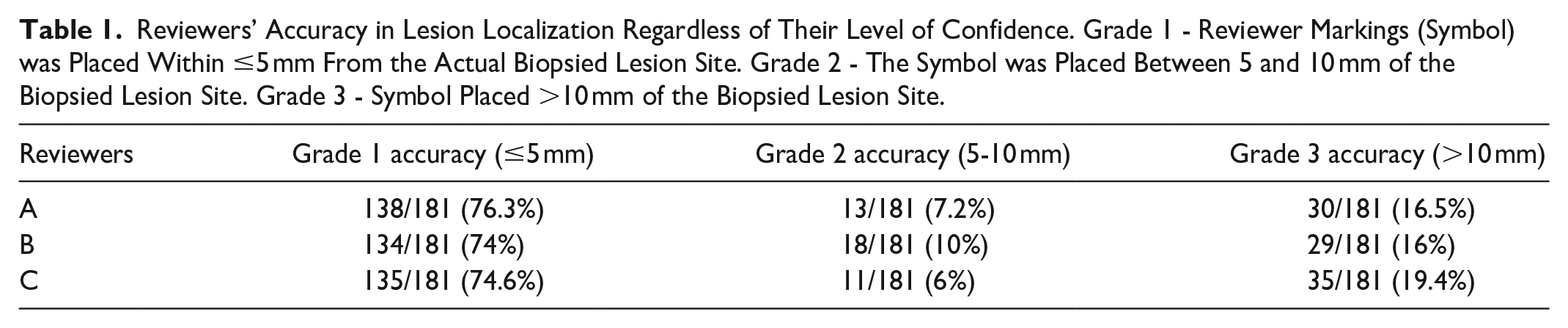
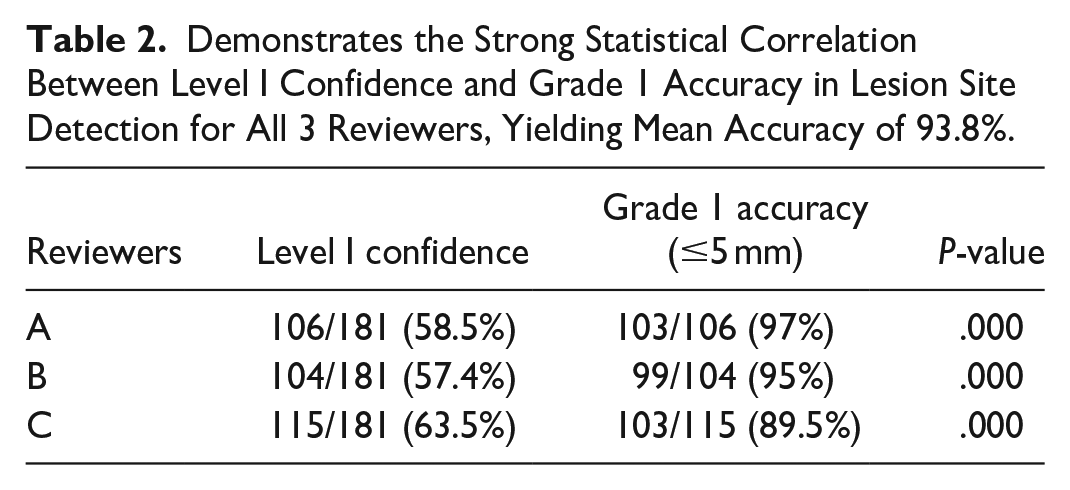
Grade 1 (≤5 mm) accuracy in identifying lesion site across all levels of confidence for all 3 radiologists ranged between 74% and 76.3% (134-138/181), mean = 75% (Table 1). Strong correlation (P < .001) was found between Grade 1 accuracy and Level I confidence. The confidence in identifying lesion site was rated as Level I in 106/181 (58.5%), 104/181 (57.4%), and 115/181 (63.5%) lesions and was associated with Grade 1 accuracy of 103/106 (97%), 99/104 (95%), and 103/115 (89.5%), for reviewers A, B, and C, respectively, yielding mean accuracy of 93.8% (Table 2). Out of all the cases where lesion sites were confidently identified, variations were seen between the 3 reviewers in 29 and 40/181 (16%-22%) of cases. The accuracy dropped significantly with Level II and III confidence. Level II confidence mean of 21.6% (39/181 of lesions, 23%, 18%, and 24% for reviewers A, B, and C, respectively) demonstrates mean accuracy of 55.3% (21/39 of lesions, 54.7%, 54.5%, 56.8% for reviewers A, B, and C, respectively). Level III confidence mean of 18.2% (33/181 of lesions, 18%, 24%, and 13.8% for reviewers A, B, and C, respectively) demonstrates mean accuracy of 34.2% (11/33, 36%, 38.6%, and 28% for reviewers A, B, and C, respectively; Table 3).
Reviewers’ Accuracy in Lesion Localization Regardless of Their Level of Confidence. Grade 1 - Reviewer Markings (Symbol) was Placed Within ≤5 mm From the Actual Biopsied Lesion Site. Grade 2 - The Symbol was Placed Between 5 and 10 mm of the Biopsied Lesion Site. Grade 3 - Symbol Placed >10 mm of the Biopsied Lesion Site.
Demonstrates the Strong Statistical Correlation Between Level I Confidence and Grade 1 Accuracy in Lesion Site Detection for All 3 Reviewers, Yielding Mean Accuracy of 93.8%.
Demonstrates the Decrease in Accuracy Grade in Lesion Site Detection as the Level of Confidence Decreases.


Note. Light gray and dark gray shadings indicate lesion site detection in Level II and Level III, respectively, along with their corresponding accuracy grades.
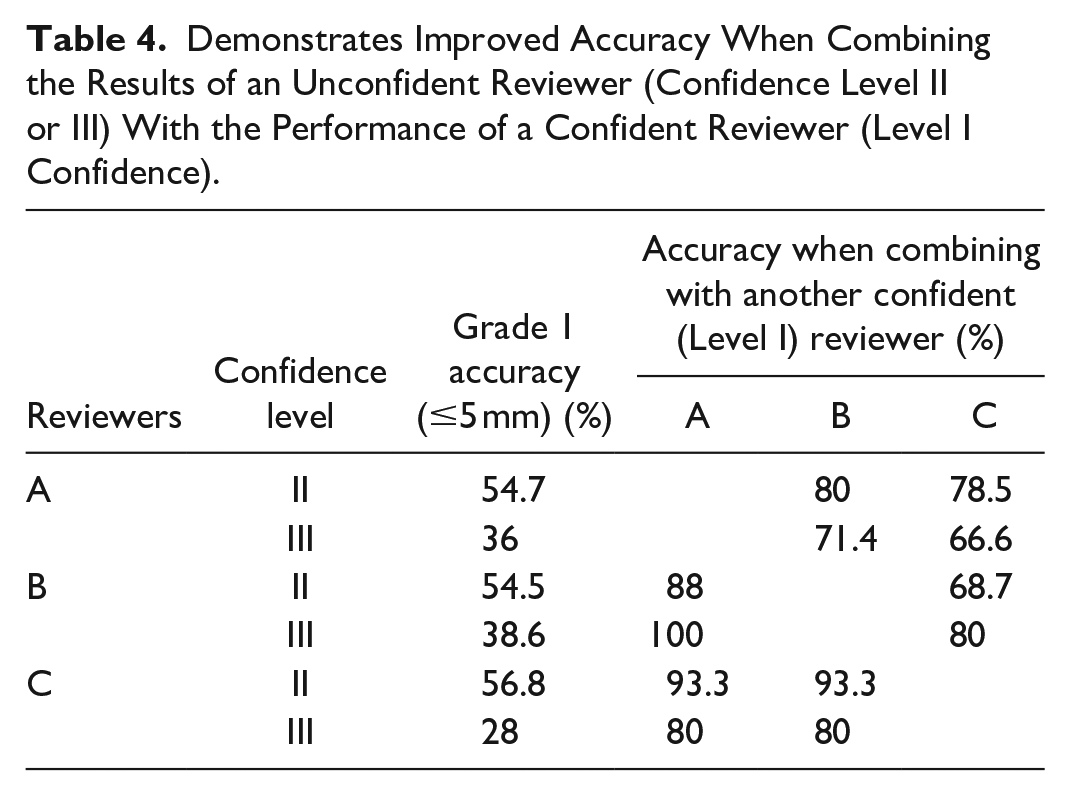
The accuracy in each unconfident lesion site localization (confidence level II or III) was combined with the accuracy of the other reviewers’ assessments when confident (Level I). Improved performance was seen with all combinations. For reviewer A combined with reviewers B and C, accuracy increased from 54.7% to 80% and 78.5% with Level II confidence, respectively, and from 36% to 71.4% and 66.6% with Level III confidence, respectively. For reviewer B, combined with reviewers A and C, the accuracy increased from 54.5% to 88% and 68.7%, with Level II confidence and from 38.6% to 100% and 80%, with Level III confidence. For reviewer C, the accuracy improved from 56.8% to 93.3% and from 28% to 80%, with reviewers A and B, respectively (Table 4). When 2 readers were confident (level I) about the lesion site, the combined accuracy was 96.5% (84/87), 94.1% (81/87), and 92.8% (78/84) for readers A and B, A and C, and B and C, respectively. All 3 readers were confident (level I) in a total of 75/181 cases (41.4%), and grade 1 accuracy was seen in 71/75 (94.6%) of these cases. A drop in confidence level was seen for all reviewers (21%-30%) in cases of BIRADS category D breast density although not statistically significant (P = .31). No correlation was found between breast density and accuracy (P = .5). The lesion morphology, size available with prior reference DCE-MRI, and unilateral versus bilateral positioning for biopsy were not found to have statistically significant correlation with either level of confidence or accuracy (P > .5).
Demonstrates Improved Accuracy When Combining the Results of an Unconfident Reviewer (Confidence Level II or III) With the Performance of a Confident Reviewer (Level I Confidence).
In 2/181 (1.1%) cases, all 3 reviewers agreed on the lesion site with high confidence. This site was different from the actual biopsied site and therefore deemed inaccurate. MRI follow-up in 6 months showed the post biopsy tissue marker in a completely different location than the enhancing lesion, indicating that the actual biopsy site was inaccurate. Among the 181 biopsied lesions, 27 (14.9%) were malignant; 14 (7.7%) invasive carcinomas, 13 (7.3%) ductal carcinoma in situ, and 35 (19.3%) were high-risk. Thirty-six lesions were excised.
Discussion
Our study revealed a high mean accuracy (93.8%) in lesion site localization on pre-contrast images when reviewers were confident. Despite NME lesions previously linked to higher MRIB cancellation rates, 14 we found no correlation between lesion morphology and reviewer performance. Although NME lesions may be hard to visualize due to background parenchymal enhancement (BPE) during biopsy compression, identifying NME lesions on pre-contrast images based on landmarks could improve accuracy and confidence in post-contrast identification. While the median lesion size was only 8 mm, lesion size did not affect radiologist performance, highlighting the importance of evaluating surrounding tissue for lesion identification. Confidence slightly dropped in patients with dense breasts, suggesting that distinguishing lesions becomes more challenging with increased density, though not statistically significant. The biopsy images are inferior to the non-contrast MRI images due to deformation from the biopsy grid and limited sequences. However, previous DCE-MRI references significantly aided in lesion localization by highlighting surrounding landmarks. Confidence and accuracy also remained steady in bilateral MRIB procedures despite decreased spatial resolution due to a wider field-of-view.
To our knowledge, this study is the first to emphasize the significance of pre-contrast images in MRIB study. Early localization of the lesion site ensures that the biopsy grid properly encompasses the area of interest, minimizing the need for patient repositioning. Identifying tissue landmarks can aid in intra-procedural verifications, such as adjusting the position of the obturator. Quite often, this is where fine adjustments are required, ensuring the lesion is not displaced from the target sampling area. However, it is not uncommon for the lesion to become less visible at this stage, often due to contrast dispersion or persistent BPE.
In the 2 instances mentioned previously, where the initial biopsy was deemed inaccurate on the 6-month follow-up MRI, it shows that sampling error might occur even with available post-contrast images. This underscores the importance of identifying tissue landmarks on the pre-contrast images to enhance the accuracy of sampling, rather than relying solely on post-contrast images. Tissue migration is reported in 14% of MRIB cases. 18 In such cases where surgical excision is necessary, localization may need to rely on tissue landmarks as well. 19 In addition, recognition of tissue landmarks may enhance more junior radiologists’ confidence with MRIB. The authors acknowledge that this technique may require more expertise and experience from the operator and may vary among different operators. As previously mentioned, the cancellation rate of MRIB procedures has been reported to decline with operator experience. 14 While identifying landmarks may be done intuitively by more experienced radiologists, this may not be the case for less experienced ones. Our results show that when combining the results of 2 radiologists, the accuracy is dramatically improved for Level II confidence and, to a greater degree, for Level III confidence. The overall accuracy remained high when 2 or 3 reviewers were confident, simulating clinical scenario when 2 radiologists discuss a challenging case and come to an agreement about the lesion site. Our study may encourage radiologists, particularly less experienced ones, to consult colleagues about challenging MRIB procedures before cancelling them.
Similar to our results, many of the patients in whom MRIB will be required reported to be at higher risk of developing breast malignancy and undergo routine screening or surveillance MRI (26.76% and 19.26%, respectively 20 ). Breast MRIs are also commonly used for breast cancer staging (28.05% of breast MRIs according to Özcan et al 20 ). Therefore, in some clinical scenarios where a lesion is not visible, the authors argue that it might be worthwhile to discuss with the patient the option of proceeding with the biopsy—provided that landmarks can be confidently identified—instead of opting for short-term follow-up after cancelling the biopsy. Given that our study indicates over 90% accuracy in lesion localization when the radiologist is confident, we suggest informing the patient of these 2 management options before obtaining consent. We hypothesize that most patients would opt to proceed with the biopsy, trusting the radiologist’s confidence in lesion localization, particularly since the issue of lesion non-visualization typically arises only after the patient has been positioned for the procedure and after contrast injection.
In the case that biopsy is completed based on landmarks, we recommend that more samples be taken around the centre of the estimated site to compensate for potential errors. If a 9-gauge (3.8 mm) vacuum needle is being used, additional samples in different directions will likely achieve coverage of at least 5 mm radius, which will be within the range of our threshold for grade 1 and 2 accuracy of <5 and <10 mm, respectively. For sub-optimally visualized lesions for which biopsy was completed and yielded benign concordant results, the authors feel that 6-month follow-up MRI is appropriate, similar to what has been recommended for MRIB with benign results.14,15,21
Our study’s limitations include its retrospective nature and as such it is prone to bias, and the absence of a junior radiologist reviewer. We tried to overcome the bias factor by blinding the 3 reviewers to the actual biopsied site. Our findings indicate that consulting with colleagues can increase accuracy, which may be relevant especially for less experienced radiologists. This approach could accelerate the learning curve for junior radiologists. One cannot ignore that radiologist confidence varies with character, which is not always linearly related to their experience. This diversity is notable even with our study, showing differences in level of confidence despite similar clinical experiences.
In conclusion, our study has demonstrated that careful review of pre-contrast MRIB images yields a high accuracy in identifying lesion sites when the radiologist is confident. When the radiologist’s confidence is low, performance can be significantly improved by consulting with a colleague and potentially minimizing cancellation rate. We therefore suggest that careful review of the MRIB pre-contrast images be embedded and taught to be an integral part of MRIB procedure.
Footnotes
Acknowledgements
The authors would like to thank research coordinator Kalan Lynn for the help provided with this study’s ethics submissions and manuscript preparation.
Author Contributions
Maya Grisaru Kacen: data collection, radiology case reviewer, data analysis, statistics, manuscript preparation, and main author. Ilanit Ben Nachum: Radiology case reviewer, data collection. Olga Shmuilovich: Radiology case reviewer, data collection. Caitlin Ward: Data collection. Anat Kornecki: Primary investigator, ethics submissions, research design, data collection, radiology case reviewer, manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.