
Abstract
In 2023, the Canadian Society of Abdominal Radiology (CSAR) and Canadian Emergency, Trauma, and Acute Care Radiology Society (CETARS) received Canadian Association of Radiologists (CAR) member feedback that there was an unmet educational need for guidance in the imaging investigation of right lower quadrant (RLQ) pain. Members requested specific guidance on how to handle controversial scenarios including which test to order when, specifics of imaging protocols, and managing pregnant patients who have RLQ pain—all from a Canadian perspective. After conducting an exhaustive literature review, the working group agreed that a Canadian-specific set of guidelines was warranted. The management recommendations presented in this guideline were discussed as a group to achieve expert consensus. As the workup for RLQ pain can vary considerably in the paediatric population, the scope of this paper was restricted to adults (18 years of age or older). Whenever possible, the best evidence was used to inform the clinical guidance, and where gaps existed, the guidelines reflect consensus among experts in the field. The result is a framework to aid in this process of managing patients with RLQ pain across various clinical scenarios while addressing current questions and controversies, particularly those most relevant to the Canadian healthcare system.
Introduction
In 2023, the Canadian Society of Abdominal Radiology (CSAR) and Canadian Emergency, Trauma, and Acute Care Radiology Society (CETARS) received Canadian Association of Radiologists (CAR) member feedback that there was an unmet educational need for guidance in the imaging investigation of right lower quadrant (RLQ) pain. There were specific requests to provide recommendations on how to handle controversial scenarios such as which test to order when, specifics of imaging protocols, and managing pregnant patients who have RLQ pain—all from a Canadian perspective. The CAR Right Lower Quadrant Pain Working Group was formed to address this request and consisted of members of the CSAR and the CETARS from a variety of practice settings across Canada. The group conducted an exhaustive literature review, including a review of the American College of Radiology Appropriateness Guidelines, and concluded that a Canadian-specific set of guidelines was warranted. 1 All management recommendations were discussed as a group to achieve expert consensus. As the workup for RLQ pain can vary considerably in the paediatric population, the scope of this paper was restricted to adults (18 years of age or older). 2
While the recommendations presented are based on the best available scientific evidence, there are some significant gaps in the literature, particularly pertaining to the Canadian experience and resource limitations. As a result, these guidelines reflect consensus recommendations rather than a fully evidence-based standard of care.
Scope of the Problem and Overview
Approximately 5% to 10% of emergency department (ED) patients present with abdominal pain, and almost half of those patients will have RLQ pain.3,4 Just under half of all patients with abdominal pain in the ED will undergo ultrasound (US) or computed tomography (CT), and the use of diagnostic imaging in this setting increased 6-fold from 1992 to 2007. 3 Due to the availability of diagnostic imaging, 8 out of 10 patients presenting to the ED with abdominal pain receive a specific diagnosis. 3
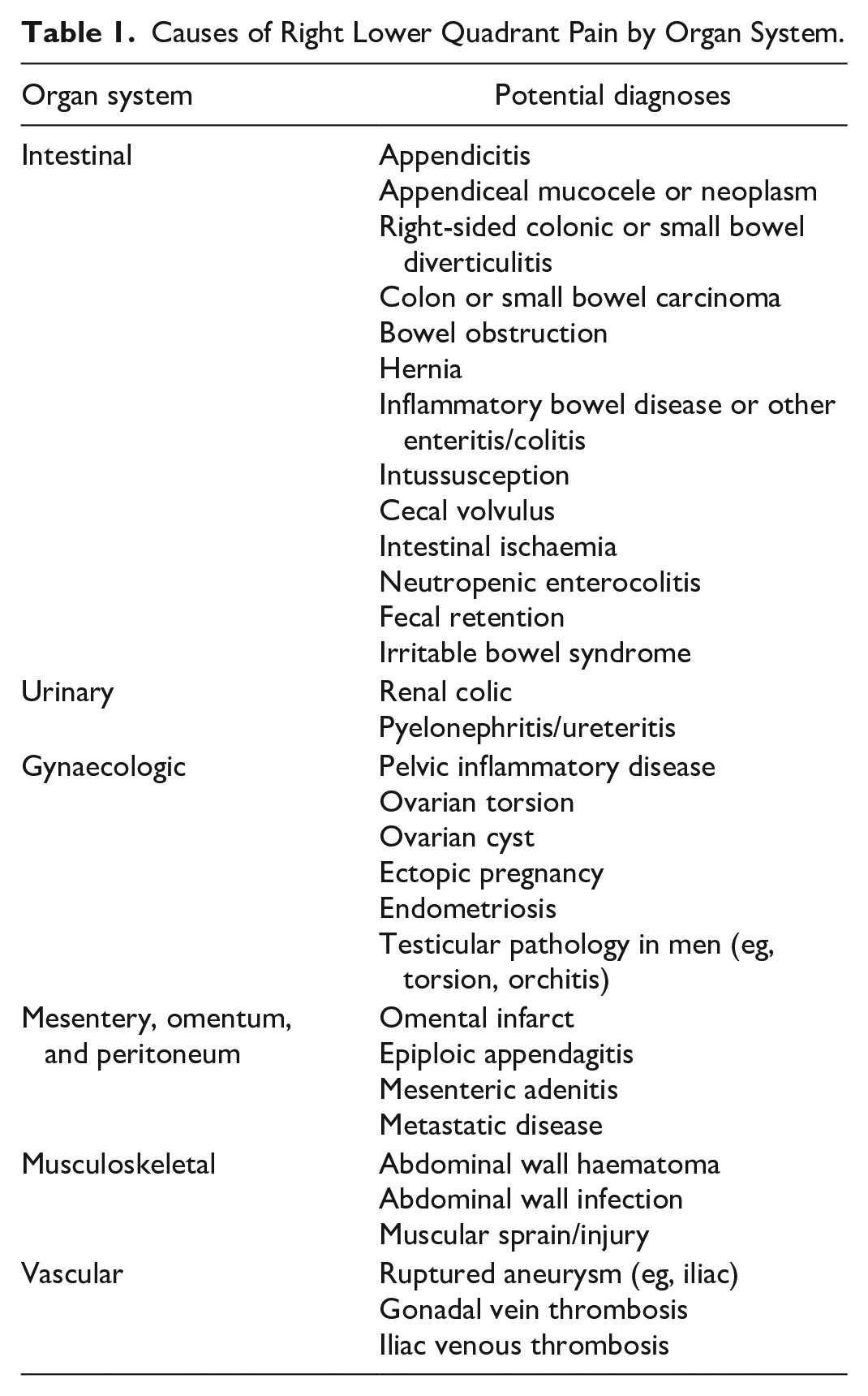
There are several potential causes of RLQ pain, and these can be categorized by organ system (Table 1).1,2,5-7 In female patients, it is vital for the ordering clinician to perform a comprehensive physical examination in order to differentiate pelvic from RLQ pain, as this will significantly impact the choice of investigations. Key clinical information should be readily available so that the consultant radiologist may triage patients and select the appropriate study and protocol. Requisitions should indicate the patient’s age, sex (and, if applicable, pregnancy status), the location of the pain (including if it has migrated), relevant past medical and surgical history, other ancillary findings such as fever, elevated white blood cell count, and urinalysis results.
Causes of Right Lower Quadrant Pain by Organ System.
The remainder of the paper will provide guidance on the following: (1) selecting the best imaging modality for specific clinical scenarios, (2) recommended imaging protocols, and (3) specific guidance for imaging pregnant patients.
The authors would like to express their acknowledgement and respect for all gender identities while clarifying the terminology used. In this article, the term “female” is employed to signify patients with internal gynaecologic organs for ease of reference, with no intent to disrespect or overlook individuals across the diverse spectrum of gender identities.
What to Order When
Imaging patients with RLQ pain should lead to a confident early and definitive diagnosis and help eliminate alternative diagnoses with high accuracy. There is an increased cost and ED length-of-stay when more than one imaging modality is used, 8 and it is thus ideal to perform the highest-yield test to make the correct diagnosis first, without further testing. A rapid and accurate diagnosis can prevent substantial morbidity and reduce overall health system costs. After-hours availability of skilled US technologists and radiologists may be dependent on local availability, and expertise but is pivotal when making a choice of modality.
Ultrasound
US is a widely available imaging modality at most institutions. It is a relatively inexpensive, non-invasive method of investigating RLQ pain, with the added advantage of avoiding ionizing radiation. As an operator-dependent test, variable sensitivities and specificities have been reported for the diagnosis of acute appendicitis (sensitivity of 76%-90% and specificity of 83%-100%).9,10 The rate of appendix visualization is also reported to be both sonographer and radiologist-dependent, 11 with inconclusive results in 15% to 84% of cases.12-14 Knowledge and awareness of local expertise is therefore necessary when considering US in the context of acute RLQ pain and suspected appendicitis. If local technologists and radiologists are less proficient in performing these studies and making the diagnosis, CT may be a more appropriate alternative.
If RLQ US is available and rapidly accessible, it should be considered a first-line modality for patients <30 years old with a body mass index (BMI) <25. Using a cut-off of 30 years of age minimizes radiation exposure in younger individuals but may increase the number of patients requiring a second test. The Working Group reached a consensus that for the Canadian population, the relatively higher degree of intraperitoneal fat in most patients over the age of 30 favours the use of CT over US. A BMI less than or equal to 25 is specified to maximize the likelihood of obtaining a conclusive result. 15 If gynaecological pathology is a primary diagnostic consideration in a female patient, US is the test of choice regardless of age/BMI, as it can be tailored to include both RLQ and pelvic assessment, including endovaginal sonography. US may also be considered in patients who have had multiple prior CT studies in order to minimize the cumulative radiation dose. 16
The above scenario (BMI <25, age <30 years old) becomes less relevant when comorbidities are present. For example, if the patient has an oncological history or suspected complications from another known pathology (eg, inflammatory bowel disease), CT would be the preferred first-line modality.
Computed Tomography
In all other non-pregnant patients with undifferentiated RLQ pain or for those with an inconclusive US study, CT is the most appropriate imaging modality. Diagnostic yield with CT is excellent and it provides a survey of all relevant anatomy, assessing for the primary suspected pathology as well as any alternative diagnoses. 17 Intravenous (IV) iodinated contrast is usually recommended unless contraindicated (see next section).18,19 The sensitivity and specificity of CT for diagnosing acute appendicitis are high (sensitivity 95% (95% confidence interval [CI]: 0.93-0.96) and specificity 94% (95% CI: 0.92-0.95)). 18 The use of CT has been associated with a significant decrease in the negative appendectomy rate. 20
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is generally reserved for pregnant patients and will be addressed last in the guideline. MRI does not offer any significant improvement in sensitivity or specificity for the diagnosis of acute appendicitis over noncontrast CT, 21 and considering access challenges and exam length, there is little role for MRI in the initial diagnosis of RLQ pain. MRI should generally be reserved as a problem-solving modality, acknowledging that some centres with greater access to the modality may elect to perform MRI in carefully selected young patients after a nondiagnostic US.
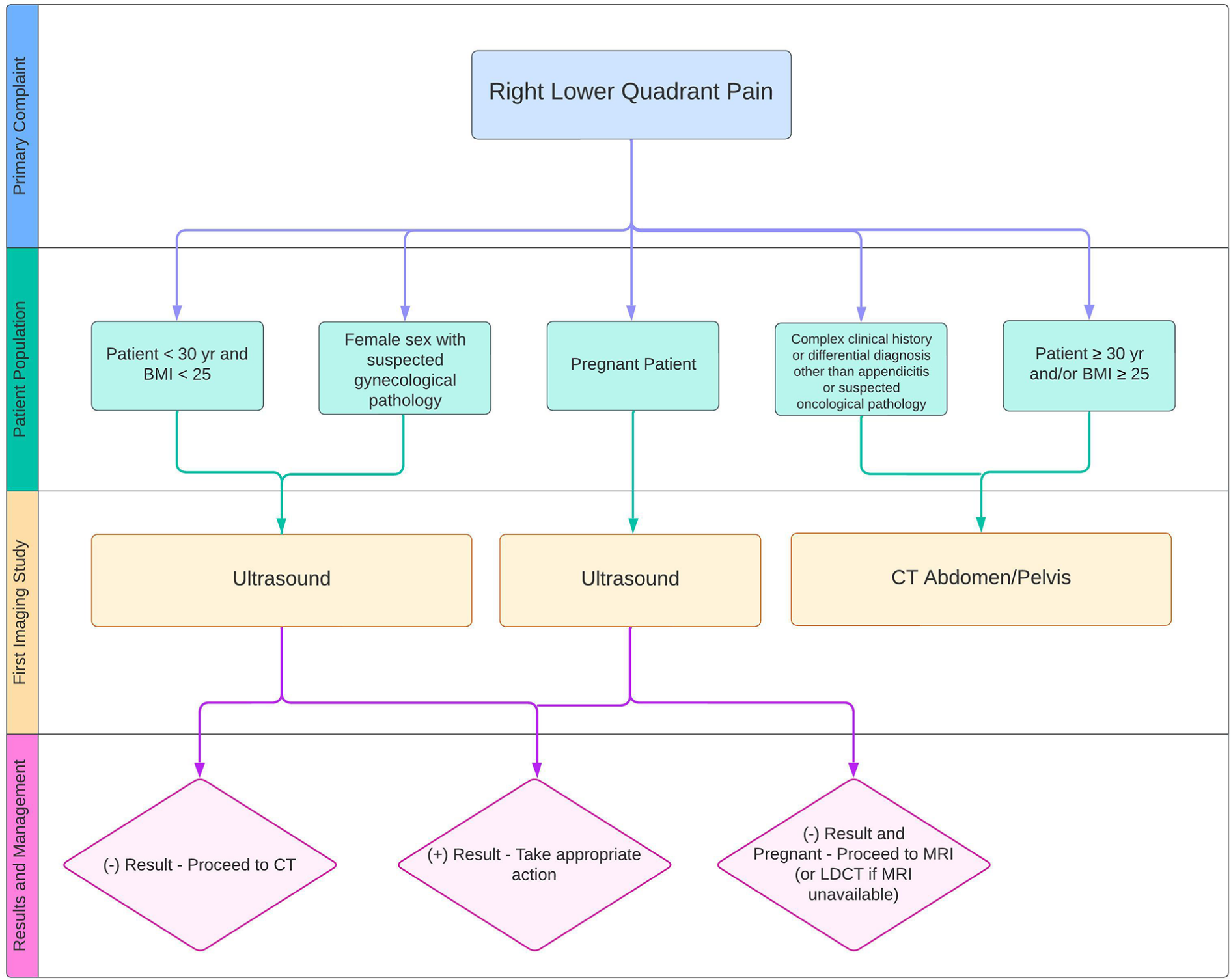
Right lower quadrant pain imaging modality algorithm.
Imaging Protocols
Ultrasound
In EDs, imaging may be used to triage patients prior to assessment by an emergency physician. Although a requisition may indicate a presumptive diagnosis of acute appendicitis, these clinical histories are often recorded before completing a physical examination and obtaining laboratory results. It cannot be assumed that other diagnoses have been adequately excluded. When US is used as a first line modality for assessment of RLQ pain, the expert panel therefore recommends that a comprehensive, rather than targeted, US be performed. This should include evaluation of the following abdominal and pelvic structures: liver, gallbladder, kidneys, pancreas, RLQ/appendix, bladder, ureterovesical junctions, gynaecologic organs in female patients, and hepatorenal recess/pelvis for free fluid assessment.
Pelvic US should be performed with a full bladder to optimize evaluation of the gynaecologic organs. A curved 3 to 5 mHz transducer is recommended for global assessment, followed by targeted assessment using a higher frequency linear transducer (10-12 mHz). Both transabdominal and transvaginal US should be performed in all eligible female patients of reproductive age.
Graded compression US is advised as part of the standard protocol for assessing RLQ pain, with detection of the appendix reported in 60% to 83% of patients. 22 The technique simulates deep abdominal palpation by using the transducer and operator’s hands to apply pressure, displacing organs during exhalation.
Self-localization by the patient to the area of maximum tenderness can be very useful in the diagnosis of acute appendicitis and is also recommended as part of the focused technique. 23
Computed Tomography
IV contrast-enhanced CT of the abdomen and pelvis is recommended as the first-line study for the evaluation of RLQ pain in most patients. A systematic review including 64 studies and 10 280 patients showed improved sensitivity with IV contrast-enhanced CT imaging (96% [92%-98%]) over noncontrast CT (91% [87%-93%]) for the diagnosis of appendicitis. 18 In cases where there is an absolute contraindication to IV contrast, such as prior severe allergic reaction or high risk of contrast-induced nephropathy, noncontrast CT may be the only option, but the diagnostic performance is still reasonable, with a sensitivity of 86% to 95%, and specificity of 92% to 97.5%.24,25
Routine administration of oral contrast in CT evaluation of RLQ pain is not recommended. A systematic review including 23 studies and 3474 patients comparing CT performance with and without oral contrast showed similar sensitivities (92% vs 95%, respectively) and specificities (94% vs 97%, respectively) between both protocols. 26 Many prospective and retrospective studies have also shown that oral contrast does not increase diagnostic performance, and repeat CT with oral contrast was only necessary in 0.2% of cases.27-29 Foregoing the administration of oral contrast allows for a more timely diagnosis, avoids unnecessary delays in treatment, and discomfort in patients presenting with RLQ pain.27,30
The routine administration of rectal contrast in CT evaluation of RLQ pain is not indicated. A prospective multicentre study including 56 hospitals and 8089 patients undergoing nonelective appendectomy found similar radiology-pathology concordance rates between IV contrast-enhanced CT and IV contrast-enhanced CT with enteral (oral and/or rectal) contrast. 27 Furthermore, rectal contrast administration requires rectal catheterization, which is often an uncomfortable procedure for both patients and CT technologists. 31
In young patients for whom radiation exposure is of concern, low-dose CT (LDCT) with IV contrast may be performed to evaluate for RLQ pain. Single-centre and multicentre randomized-controlled trials including 891 and 3074 patients aged 15 to 44 years presenting with suspected appendicitis found that contrast-enhanced LDCT (2 mSv) was noninferior to contrast-enhanced standard-dose CT (3-8 mSv) and both modalities had similar negative appendectomy rates and diagnostic performance.32,33 However, it is worth noting that less than 5% of the studied patient population had a BMI over 30.32,33 Although image degradation due to noise can be of concern when scanning obese patients with a low-dose protocol, increased intra-abdominal fat may conversely help visualize the appendix in these patients. 33 LDCT can be obtained through various methods, such as by decreasing the tube current (mA), increasing the degree of iterative or deep-learning based reconstruction, or altering the noise index of the acquisition. However, before implementing LDCT in the clinical setting, consultation with local medical physicists and application specialists is recommended to build a low-dose protocol that best suits each institution’s CT scanner. It is more important to obtain a confident diagnosis of appendicitis than to obtain a small reduction in ionizing radiation at the expense of CT sensitivity and specificity.
Limited field-of-view (FOV) CT covering only the pelvis is not recommended as first-line imaging for the evaluation of RLQ pain. Retrospective studies evaluating pelvic CT below the iliac crests showed missed alternative diagnoses in 16% to 26% of patients presenting with suspected appendicitis.34,35 Sensitivity for limited FOV pelvic CT was found to be significantly lower than that of full-range CT (88% vs 99%, P < .05). 34 However, a limited FOV CT may be considered in young patients who have already undergone full abdominal-pelvic US imaging to exclude alternative diagnoses. Retrospective studies showed that reducing scan range to cover the superior vertebral endplate of L2 to the superior border of the pubic symphysis is adequate to fully visualize the appendix in patients who had previously undergone inconclusive US for suspected appendicitis.36-38 Limiting the scan range from the superior vertebral endplate of L1 to the inferior border of the pubic symphysis can also reduce total effective radiation dose by 39%. 36
Shielding of radiosensitive organs during CT examinations is no longer recommended.39,40 Proper placement of contact shields is difficult. They can often migrate or become misplaced, which leads to suboptimal dose reduction.39,40 Incorrect placement of shields can even lead to increased radiation exposure if obscured anatomy warrants repeat imaging, or when the shields are detected by automatic exposure control systems, which results in unwanted increases in radiation output.39,40 Contact shielding is also inefficient against radiation from internal scatter, a substantial source of radiation from CT imaging.39,40 Furthermore, other advancements in CT technology have allowed for significant dose reduction while maintaining image quality without the use of shields. 39
Multi-energy CT (MECT) is a CT technique that acquires images using photon spectra of different energy levels to allow for the characterization and differentiation of various tissues, including calcium and iodine. 41 The terms multi-energy CT, dual energy CT, and spectral CT are often used interchangeably. In abdominal imaging, MECT can be used to differentiate well-perfused bowel wall from necrotic bowel-wall by identifying iodine in the wall or by making it more visually conspicuous. 41 A retrospective study found that gangrenous appendicitis can be distinguished from uncomplicated appendicitis using beams at 80 to 100 kVp and 140 to 150 kVp.41,42 Potential drawbacks of MECT include difficulties in maintaining dose-neutral radiation exposure compared with standard single-energy CT, restrictions in pitch with certain manufacturers, increased number of images, storage requirements, more complex post-processing, and increased interpretation times. 43 Therefore, in institutions that have not already adopted MECT as the standard emergency abdominal CT acquisition technique for other reasons, MECT is not specifically recommended for the evaluation of RLQ pain.
Magnetic Resonance Imaging
Recognizing the challenge of appendix non-visualization, a combined approach using different imaging modalities may be necessary for a confident diagnosis in some patients, predominantly pregnant patients. Vasileiou et al 44 found that in pregnancy, a combination of abdominal US and MRI was most commonly performed (41%), followed by MRI alone (29%), US alone (22%), CT (5%), and no imaging (2%).
When MRI is performed for RLQ pain, the expert panel recommends use of a phased-array body coil due to its superior signal-to-noise ratio (SNR) relative to the built-in body coil. Antiperistaltic medication such as hyoscine (20 mg IM or IV) has been used in eligible patients to reduce artifacts arising from bowel peristalsis. As there is limited data on the use of hyoscine and other antiperistaltic agents during pregnancy and lactation, it is preferable to avoid its use as a precautionary measure. A 1.5T field strength is preferred, as lower field strengths are less susceptible to artifacts from enteric gas, motion, and peristalsis compared to 3T.
The expert panel MRI protocol recommendations are listed in Table 2.
Recommended MRI Sequences for Assessment of RLQ Pain in Adult Patients.
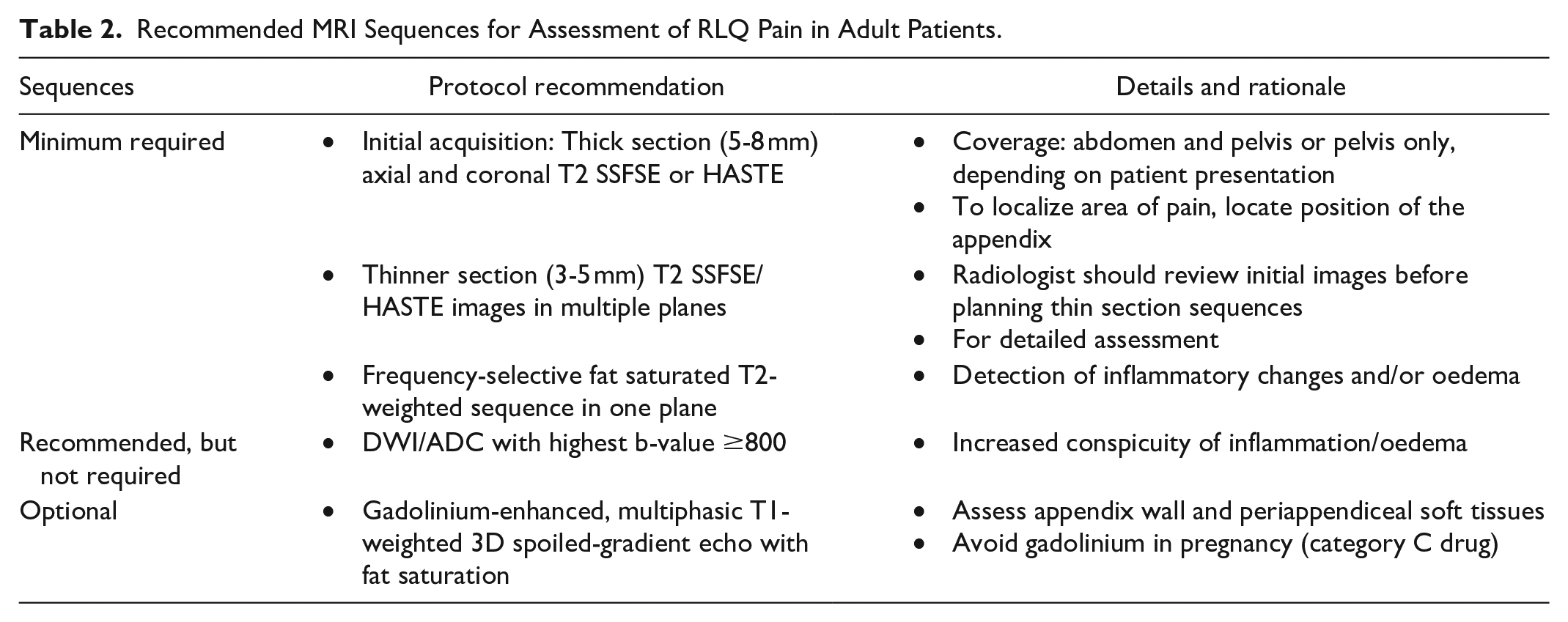
The use of abbreviated MRI protocols is becoming more common in abdominal imaging to reduce imaging and interpretation time. In a prospective study of 67 patients with clinical suspicion of acute appendicitis, Islam et al 45 used an abbreviated protocol consisting of axial and coronal T2WI SSFSE/HASTE (3 mm slice thickness) and axial DWI, and found a sensitivity of 93.3%, specificity of 86.4%, and diagnostic accuracy of 91.0%. Mian et al 46 also found that abbreviated protocols consisting of HASTE and DWI images reduce imaging and interpretation times in the diagnosis of acute appendicitis, with similar accuracy to a full protocol.
Right Lower Quadrant Pain in Pregnancy
Clinical Context
The overall prevalence of appendicitis during pregnancy is 0.001% to 0.004%. 47 Widespread use of imaging has reduced the rate of negative laparotomy to 1% to 3% versus 25% to 30% historically. 19 Unfortunately, more than 15% to 30% of patients who undergo an appendectomy, specifically in the second and third trimester, still have a normal appendix.48,49 This is not inconsequential, as laparotomy increases the risk of pre-term delivery and is associated with surgical complications. Conversely, the risk of appendiceal perforation is increased to 66% in the setting of a delayed diagnosis which can result in an increased risk of fetal loss and maternal mortality if left untreated for >24 hours. 50 The rate of fetal loss increases from 2% when appendicitis is unruptured to >30% when the appendix has ruptured.51-53
Imaging Issues Specific to Pregnancy
There is an anatomical alteration in the location of the appendix during pregnancy arising from anterior and superior peritoneal displacement. Presenting symptoms may be vague and non-specific. When coupled with a limited physical examination and an atypical location of pain, the diagnosis may be delayed or confounded. Moreover, physiological elevation of the white blood cell count and C-reactive protein during pregnancy can further lead to misinterpretation. 54 US can be sensitive when performed by experienced sonographers, but is operator dependent (sensitivity 56% and a specificity of 88%). 55 As the appendix displaces cranially during the third trimester and bowel loops are compressed against each other, locating the appendix becomes increasingly difficult as the pregnancy progresses. US remains the first line test as it has reasonable performance characteristics, is free of ionizing radiation and can offer alternate diagnoses in the setting of acute pain. Several studies have shown that MRI in pregnancy has a sensitivity and specificity for detecting appendicitis of up to 100% and 94% to 100%, respectively53,56-58 A systematic review and meta-analysis of 19 studies reinforced these findings by demonstrating a sensitivity and specificity of 91.8% and 97.9%, respectively. 59 This accuracy was also replicated by readers with variable experience who achieved an accuracy of 99.8% and positive predictive value of 100% for the presence of acute appendicitis. 60
Consent
Guidelines vary with regards to consent and may vary between jurisdiction and regulatory bodies. The Working Group agrees with the ACR that consent may be either verbal or written but should be documented. The latter should be uploaded either as an attachment to PACS or within the electronic patient medical record. An example of wording that could be used in a consent form is given in Appendix A.
Technique
The MRI technique in pregnancy has been previously described, but several key points should be reinforced. In the pregnant population, the use of gadolinium is not recommended unless absolutely necessary for acquiring information that cannot be otherwise obtained and if its use would meaningfully alter management (which is typically unlikely). Although there are no documented adverse outcomes associated with MRI in any trimester of pregnancy at 1.5 or 3T, most recommend using 1.5T in the first trimester if both field strengths are available. Given this, and owing to increased susceptibility artifacts at 3T, the Working Group recommends that all pregnant patients be scanned at 1.5T if possible. There is insufficient evidence at this point to recommend scanning at a field strength of <1.5T. Specific absorption rate (SAR) and energy deposition are a theoretical concern, but sequence parameters and radiofrequency pulse design will automatically adjust to lower SAR on modern scanners. 61 DWI can increase the sensitivity of MRI in the detection of the appendix and specifically has increased potential to improve performance in the novice or less sub-specialty trained reader, at the expense of increased SAR.60,62
Which Modality and in Which Order?
Data on the modality and ideal order of investigations remains anecdotal, but outside the confines of academic institutions and larger communities, the availability of MRI to image pregnant patients urgently is limited in Canada. US is widely used as the first line of imaging in pregnant patients with an acute abdomen as it is inexpensive, portable, free of ionizing radiation, reasonably sensitive, and specific in experienced hands. 63 As previously stated, the sensitivity of US is adversely affected by bowel gas, body habitus, pain, and displacement of normal anatomy by the gravid uterus—all of which become more problematic as a pregnancy advances. Higher rates of inconclusive results (up to 63%-97%) have been reported after 24 weeks of gestation64,65 compared to the first trimester (26%). 64 This finding has led some institutions to advocate for noncontrast MRI of the abdomen as an initial modality of investigation in pregnant patients with suspected acute appendicitis. 66 This approach remains limited to centres with streamlined access to MRI and radiologist expertise to interpret the studies. However, the current reality in Canada is that few centres can provide this option. Despite demonstrating mediocre accuracy in later trimesters, it is the opinion of the Working Group that US should always be performed prior to MRI given the ease of access and relative complexity of arranging MRI in most emergent settings.63,67 In most Canadian institutions, even if an MRI is requested, an US could be performed in the time it takes for the scan to be arranged.
Given the ionizing radiation involved with CT, this should be an option of last resort except in cases of a trauma-related RLQ pain in pregnant patients,63,68,69 as supported by the European Society of Urogenital Radiology (ESUR) and ACR. There is a role for low-dose CT if MRI is unavailable or inaccessible (also supported in this setting by ESUR recommendations), but there is no consensus on the specific LDCT protocol. Low-dose CT is non-inferior to conventional dose CT in the imaging of both gravid and non-gravid patients.32,68 In one study, low-dose CT was able to confirm or rule out the diagnosis of appendicitis, or provide an alternate explanation for RLQ pain in 83% of the patients scanned. 68 That said, the Working Group feels it is more important to establish a definitive diagnosis than obtain a technically suboptimal scan which could be both non-diagnostic and delay care for further downstream testing. We recommend that departments work collaboratively with their medical physicist and CT vendors (and respective application specialists) to use as much iterative or deep-learning reconstruction as possible to minimize dose while maintaining study quality. If a CT is performed, iodinated IV contrast should be considered (unlike gadolinium-based contrast agents, iodinated contrast agents are not contraindicated in pregnancy).
The Role of Specialist Consultation: When and Whom?
There is no clear consensus on when to include a specialist consultation in the management of pregnant patients presenting with RLQ pain. The European Association for Endoscopic Surgery rapid guideline recommends operative treatment over conservative management in pregnant patients with complicated appendicitis or appendicoliths on imaging studies (strong recommendation) and suggests operative treatment over conservative management in pregnant patients with uncomplicated appendicitis and no appendicolith on imaging studies (weak recommendation). 70 Extrapolating from these guidelines and based on consensus opinion, we suggest early involvement of a surgical consultant in the pregnant patient presenting with RLQ pain. The specific surgical specialty needed can be guided by first- or second-line imaging findings and early emergency medical workup. Consultation could be obtained as early as after first-line US evaluation, even if equivocal, and either MRI (preferred) or CT (last resort) are required to navigate decision-making with the management plan in mind well in advance. This can also assist in the best approach to patient counselling and guidance in informed decision-making.
Conclusion
The evaluation of patients with RLQ pain should be geared towards timely diagnosis with minimal testing to reduce patient morbidity and healthcare costs. The Working Group has provided a framework to aid in this process for various clinical scenarios and has addressed current questions and controversies, particularly those relevant to the Canadian healthcare system.
Footnotes
Appendix A
Acknowledgements
The authors would like to thank the members of the Canadian Association of Radiologists who took the time to provide their feedback and peer review during the drafting of these guidelines.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Tanya Chawla published the following relevant article related to this work: CT following US for possible appendicitis: anatomic coverage. O’Malley ME, Alharbi F, Chawla TP, Moshonov H. Eur Radiol. 2016 Feb;26(2):532-8. doi: 10.1007/s00330-015-3778-0. Epub 2015 Oct 31. Dr. Angus Hartery is a faculty member of Memorial University of Newfoundland. Dr. Zahra Kassam reported receiving a research grant and speaker honorarium from Bayer Pharmaceuticals. Dr. Kassam is also Division Head, Body Imaging at Western University. Dr. Iain Kirkpatrick reported receiving an honorarium for recording an educational podcast on contrast conservation for Bayer. Dr. Kirkpatrick has written relevant articles in the Canadian Association of Radiologists Journal in his capacity on the Incidental Findings Standing Committee and has presented on this topic at the Canadian Association of Radiologists Annual Scientific Meeting in his capacity on the Incidental Findings Standing Committee. No other authors declared potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.