
Abstract
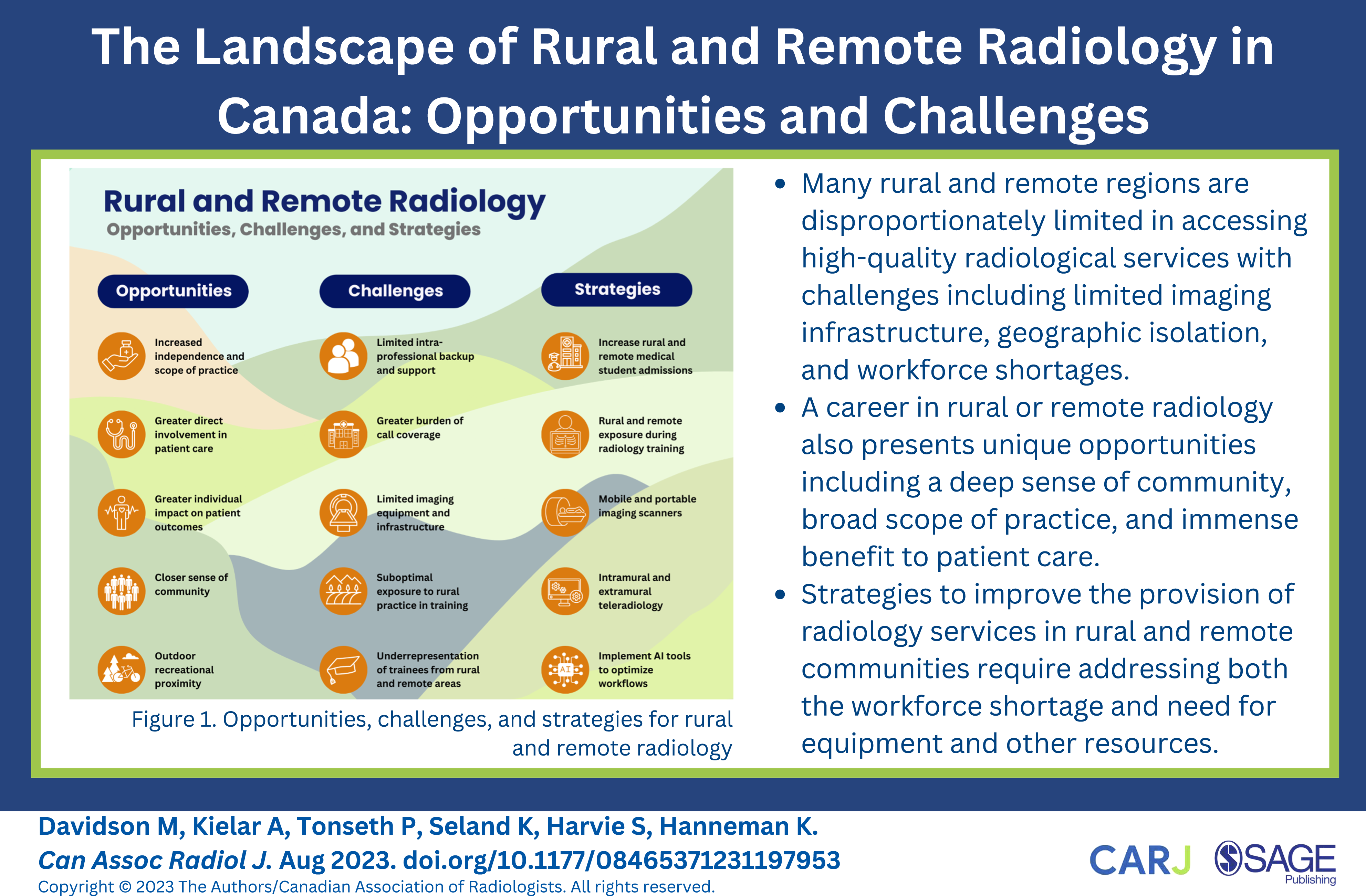
Diagnostic and interventional radiology play a crucial role in healthcare, facilitating diagnosis of disease, treatment planning, interventional therapies, and assessment for response to treatment. However, many rural and remote regions are disproportionately limited in accessing high-quality radiological services. Challenges include limited imaging infrastructure in these communities, geographic isolation, and workforce shortages impacting provision of interventional image-guided procedures and subspecialty imaging in particular. However, a career in rural or remote radiology also presents unique opportunities including a deep sense of community, broad scope of practice, and immense benefit to patient care. This review aims to explore the landscape of rural and remote radiology with a focus on Canada, including opportunities, challenges, and potential strategies. Some of the challenges are shared by both rural and remote communities while others are distinct. Factors that have contributed to challenges in recruitment and retention of rural and remote radiologists include workload burden, inadequate or suboptimal imaging and interventional equipment, and limited exposure during training. Additionally, strategies to improve the provision of radiology services in rural and remote communities are highlighted, addressing both the workforce shortage and the lack of essential equipment and other resources.
Introduction
Radiology is an integral and rapidly evolving field within healthcare, playing a pivotal role in diagnosis of disease, treatment planning, interventional therapies, and assessment for response to treatment. However, rural and remote communities face unique challenges in accessing consistent and high-quality medical imaging. Consequently, a career in rural or remote radiology presents both appealing prospects and potential hurdles that warrant closer examination.
The definition of rural and remote communities differs across various sources. Rural communities are commonly defined by their population, while remote communities more often reflect geographic location and proximity to urban centres. 1 Many communities meet criteria for both remote and rural medicine. However, rural communities may have urban centers in accessible proximity, whereas remote communities may have a population that qualifies them as a small city.
Despite differences in population, location, and proximity to larger cities, rural and remote communities often share similar considerations in the health care setting. In Canada, 18% and 12% of the population reside in rural and remote areas, spread over 95% and 75% of the total land mass, respectively. 2 –4 According to the Canadian Institute of Health Information (CIHI), 8% of physicians work in a rural setting, 5 serving a proportionately larger patient population than their urban counterparts. The population of rural and remote Canada is also different; both settings have a higher prevalence of patients with lower socio-economic status with poorer health outcomes, with the increasing remoteness of a community predicting these two factors. 4 Among many attributable reasons for poorer health is limited access to health care services. Consequently, rural and remote physicians operating in these underserviced regions are crucial in supporting their community. While there is some overlap in challenges and opportunities for rural and remote radiology, other aspects are unique.
In this article, we will explore the unique appeal and challenges of a radiology career in rural and remote locations, and discuss strategies to address both the workforce and material shortage for radiological services in Canada, Figure 1. Opportunities, challenges, and strategies for rural and remote radiology.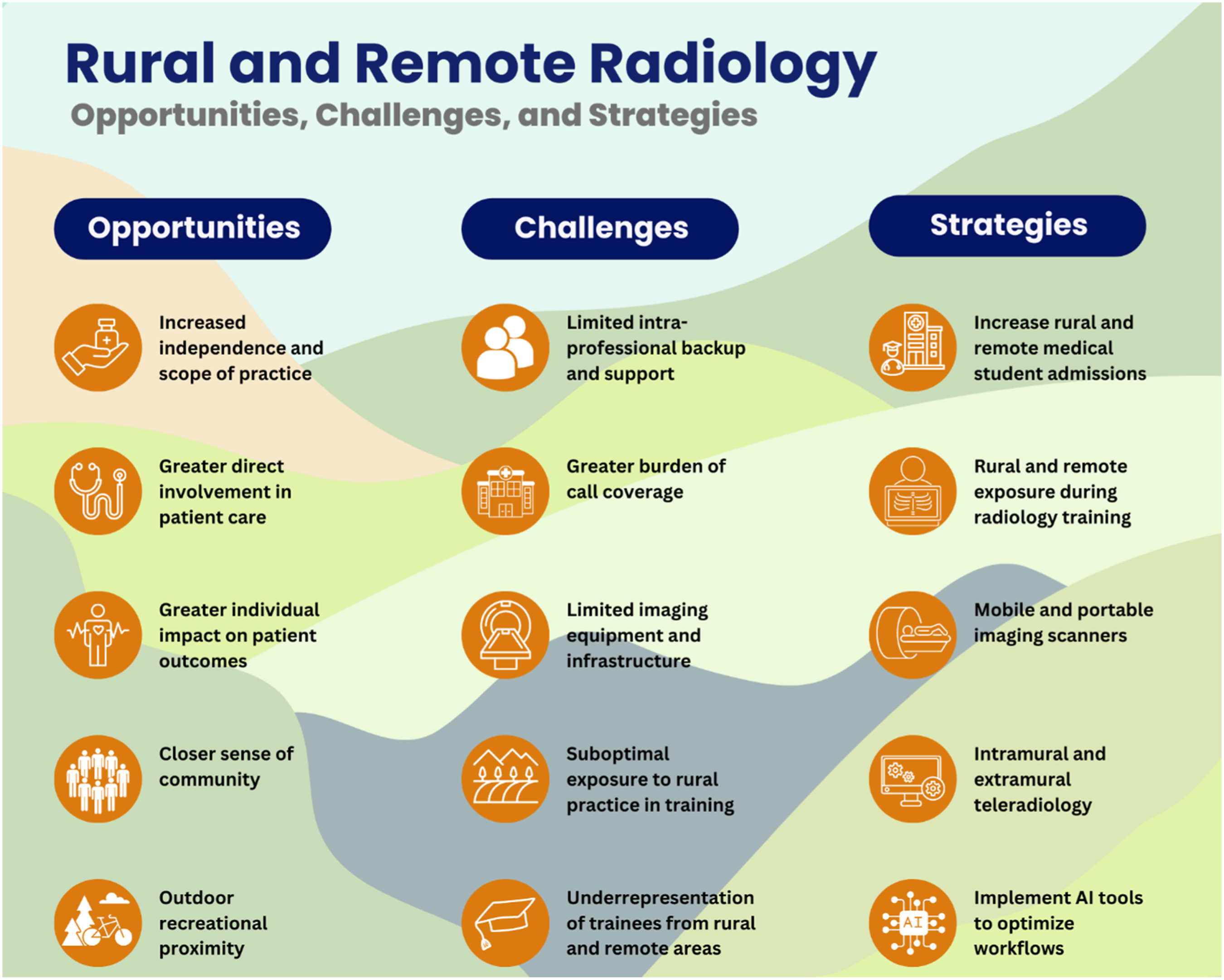
The Appeal of Rural and Remote Radiology
A career in rural or remote radiology shares features common to rural and remote medicine in general. Commonly cited reasons to enter rural or remote practice amongst physicians are increased scope of practice, lower cost of living, and access to outdoor recreational activities. 6,7 Rural settings provide an environment that may be conducive for raising a family. 8,9 Overall, 76% of rural and remote physicians feel a sense of belonging to their community, compared to 52% of urban residents. 6,10 Many rural and remote areas in Canada offer financial incentives, which combined with a lower cost of living facilitates financial independence earlier in one’s career.
Rural or remote practice offers the opportunity for increased independence and a broad scope of practice, using the full skillset of a physician’s training. 6,11 Whereas in urban and academic settings, a radiologist may practice in a subspecialized area such as interventional neuroradiology or abdominal diagnostic radiology only, rural radiologists frequently contribute to patient care through a wide and diverse range of diagnostic and interventional work. 12 Patients presenting with various symptoms may end up with a full workup and follow-up in the rural or remote area, allowing radiologists the opportunity to follow through with the best options for the patient in a “one-stop shop”. Further, rural and remote practice allows radiologists greater interactions with the community they serve. Radiologists in these settings are more often involved in direct patient care and planning, leading to increased interprofessional collaboration and relationship building with patients and their families. 8,12,13
Rural and remote radiologists can have an immense impact on the accessibility of care. This is especially important in remote communities, often hundreds of kilometres away from the nearest urban centre. Through the provision of necessary procedures such as biopsies and drains, on-site radiologists negate the need for patients to travel or be transferred long distances. Further, specialized interventional radiology (IR) services are increasingly in demand due to their minimally invasive nature and their ability to provide targeted treatments for various medical conditions. In Canada, there are no interventional radiologists in the territories, and very few centres outside of urban cities offer such services in the country’s central provinces. 14 Although rural hospitals may have limitations in terms of patient volume and funding to offer interventional services, larger remote hospitals may be better equipped with the necessary resources to provide IR services.
Challenges in Rural and Remote Radiology
While rural and remote radiology offers unique attractions to providers, these practice settings also confer challenges that necessitate innovative solutions. Increased independence and scope of practice are often a double-edged sword. Work can be isolating, without access to a team of colleagues for case deliberations, assistance, or shift coverage. Dissatisfaction can arise due to perceived lack of control over work hours, increased administrative duties, call burden, and high patient volumes due to large catchment areas. 8,11,15 In addition, the broad scope of practice can require additional training. All this can result in less control over one’s lifestyle, one of the initial main attractants of rural and remote practice. 6,7
Accessibility of Medical Imaging in Rural and Remote Centres
Rural and remote radiologists may be limited in their ability to provide timely care to underserviced communities due reliance on government funding for imaging and interventional equipment and reduced opportunities for donations through hospital foundations.
One of the foremost obstacles is the inadequate availability of radiological resources and expertise in rural and remote areas. Less than 20% of rural emergency departments (ED) in Canada have in-house access to CT, 16 necessitating patient transfers to other hospitals if CT imaging is needed. The exception to this is Quebec, which has CT scanners in over 70% of its rural EDs. This discrepancy with the rest of the country is likely multifactorial: structured government policy for rural EDs, fewer per-capita rural hospitals, and comparatively less infrastructure to facilitate inter-hospital transfers in Quebec. 16 Access to local imaging without the need for patient transfer can improve time to treatment and reduce costs, especially in Canada’s remote communities. In 2010, over 400 patients were transferred from Iqaluit to Ottawa for CT imaging. The average duration of patient stay was 13 days, with total incurred costs amounting to approximately $25,000 per patient per trip. 17 Currently, Canada’s Northern Health Travel Grant reimburses some of the travel and accommodation costs incurred for patients accessing medical services; however, the funding is woefully insufficient. For example, the fund reimburses a maximum of $550 total for accommodations for stays of 8 nights or longer. 18 Patients are then left to cover any remaining costs they may incur during the trip, including food, car rental, and outstanding costs for accommodation.
Not only are patients transfers costly, but they are also suboptimal in terms of access and quality of care. A study in Brazil investigated outcomes during transfers of ICU patients and found that 50% of transfers occurred for imaging purposes, and 20% of transfers had an adverse outcome with at least mild harm occurring to the patient. 19 Outcomes in Canada may be comparable, as inter-facility transfer services often only have basic life support training and frequently operate under limited conditions. 20 In rural or remote settings, transfers for diagnostic imaging are not limited to only the sickest patients. A study of rural EDs in the US found that 25% of interhospital transfers occurred due to a lack of radiology services, and 38% of these could have been avoided if there was a local CT scanner. 21 A pilot study of a hospital in Quebec without a CT scanner showed similar rates of transfer for CT imaging. 22
IR is a field recognized as a subspecialty of medicine in many counties. IR procedures are often beneficial to the healthcare system, offering decreased morbidity, improved patient safety, and overall cost savings compared to invasive and surgical options in some instances. Despite this, Canada performs the fewest IR procedures per capita amongst the G7 nations. 23 While there have been efforts to increase IR services, lack of funding and costs to develop infrastructure serve as barriers to advancement. Community radiologists in particular face greater challenges in this regard. 14 A survey in the US found that 29% of rural centres fell short in providing IR services. 24 In Canada, IR services are sparse to non-existent in Canada’s rural and remote regions, 25 paralleling the US landscape of poor provision of IR care outside of urban centers.
Through limited funding and availability of imaging and interventional equipment and support, radiologists can be constrained in their scope of practice and job opportunities in rural and remote communities.
Recruitment and Retention
The rural radiologist workforce faces poor recruitment and retention compared to its urban counterpart. Between 2010 to 2020, the number of radiologists practising in urban areas grew by 24%, whereas the number of radiologists practising in rural areas only grew by 5%. 5,15 Compared to a 26% increase in rural specialists practising in rural areas, 5 it becomes evident that there are reasons specific to radiology deterring the growth of the rural and remote workforce.
Reasons for limited recruitment in rural and remote areas is likely multifactorial. General deterrents to non-urban practice are decreased opportunities for culture and diversity in communities, potentially leading to social isolation or exclusion. 12,13 Greater call frequency and lack of professional backup to cover clinical practice are both frequent in rural and remote areas. 6 Specific to radiology is the increased workload seen year over year. Between 2003-2019, the use of CT and MRI in Canada has doubled and tripled, 26 respectively, greatly outpacing the 5% growth of radiologists in rural settings since 2010. 5
The option to work remotely including teleradiology services in recent years has likely impacted recruitment in rural and remote locations. Teleradiology can be differentiated into two models: intramural and extramural. Intramural refers to radiologists who are working for, or associated with the medical entity that is acquiring medical images. Extramural radiology is defined as an off-site imaging interpretation practice not associated with the health care entity acquiring the images. 27 Both models of teleradiology have become increasingly popular over the last two decades, 28 with many job opportunities evolving to include intramural teleradiology with reduced on-site requirements and the opportunity to cover more affiliated imaging facility locations. Rural and remote sites struggle to compete with similar hybrid structures as there is insufficient coverage for necessary on-site procedures and responsibilities. Further, the increased ability of radiologists to provide coverage through extramural work eliminates the need to move and integrate in smaller or less accessible communities. In combination with limited IR facilities and imaging technology, the result is less competitive job opportunities that can be offered for rural and remote locations.
Poor recruitment of rural and remote staff has been a consequence of both poor admission of medical students from these areas and limited exposure to rural and remote practice during training. Growing up in a non-urban setting is a strong predictor of the future decision to practice rurally, 29 –35 with one study showing up to 90% of graduates from rural areas remain in non-urban regions in future practice. 29 Retention is also improved, with another study demonstrating that 68% of family physicians from rural areas remain in rural practice after more than a decade, vs 46% of rural family physicians not originally from a rural background. 31 Unfortunately, students from rural and remote areas are underrepresented in medical school with a trend toward even lower representation in recent years. In 2002, 10.8% of students were from non-urban areas, compared to 22.4% of the total population at the time. 36 In the last 15 years, the US has seen a decline in the number of rural medical students, with racialized students from rural areas representing only .5% of new medical students, despite comprising more than 15% of rural residents.
Physicians are more likely to practise in underserved settings if they have exposure during their medical training. 37 –43 A survey of emergency medicine programs in the United States found 22% of graduates from schools with a required rural rotation entered rural practice, compared to 7% of graduates from schools with elective or no rural rotations. 41 This finding is especially important as it eliminates the selection bias of those with a pre-existing interest in rural medicine who choose to participate in a rural rotation. Unfortunately, the vast majority of radiology residency in Canada is conducted in urban settings. With limited exposure, residents are less likely to grow connections to non-urban communities and garner interest in practicing in these locations. Implementing rural and remote training programs requires a concerted effort among programs, as these communities often face challenges for trainees such as inadequate patient volumes for learners, limited educational resources, and insufficient support for faculty development and protected teaching time. 44
Proposed Strategies
The challenges of rural and remote radiology involve both a workforce and material shortage. Proposed strategies aim to address these two domains.
Increasing Admission for Medical Students From Rural and Remote Areas
Admitting students from rural and remote areas to better reflect the Canadian rural demographic can ultimately increase recruitment and retention of physicians in non-urban locations. The Northern Ontario School of Medicine (NOSM) trains students in communities such as Sudbury and Thunder Bay, Ontario, offering seats to 74 students each year, almost all of whom are from rural areas. 45 Similarly, the University of British Columbia (UBC) offers the Northern and Rural Pathway, with up to 44 seats annually. 46 Extending upon this infrastructure for medical education in rural and remote areas is important to not only raise recruitment of non-urban physicians, but to provide underrepresented groups equitable opportunity to service their communities.
Increasing Exposure to Rural and Remote Radiology During Radiology Residency
Increased exposure to rural and remote radiology during training is an important step to increase the future workforce in these locations. Numerous studies have demonstrated an association between exposure to rural practice during medical training and subsequent decision to practice in rural or remote locations. 37 –43 Access to rotations during training offer the opportunity to connect to local communities and develop a deeper understanding of the unique challenges and rewards associated with practicing within them.
Health systems have faced similar challenges recruiting surgeons to rural and remote areas and have launched several initiatives to address this. In 2002, Oregon Health and Science University provided the option of a year-long rotation for fourth-year surgical residents in a remote, rural community. Those that participated were more likely to practice in a community with a population less than 50 000. 42 Similarly, the University of Tennessee introduced a rotation in its residency program that provides skills relevant to rural or remote practice in a community of 14 000. Residents who completed this training found it highly beneficial and were more likely to consider rural practice in the future. 47 In Canada, there is an opportunity to expand training programs in non-urban areas by leveraging existing medical school infrastructure. While institutions like NOSM and UBC already provide medical students and residents with training experiences in rural and remote sites, the same opportunity is currently not available for radiology residents. Actively supporting the development of radiology training programs in locations with pre-existing training capabilities can increase recruitment of radiologists to these locations once they are done training.
Teleradiology
Teleradiology is a crucial tool in providing diagnostic imaging interpretation coverage across the country. In particular, Canada’s most remote communities often rely solely on teleradiology for interpretation. 5
Teleradiology offers the opportunity to augment the diagnostic imaging services available to both rural and remote Canadians. Extramural services enable after-hours coverage, helping to alleviate the increasing workload of local radiologists. 48,49 Further, teleradiology has the ability to facilitate increased consultation and collaboration through allowing local physicians, including radiologists, to access off-site specialists for enhanced patient care and provider support.
Despite the significant benefits of remote radiologic interpretation, there are important limitations associated with teleradiology. Interventional and procedural services require an on-site presence and cannot be outsourced. Extramural teleradiologists may have little to no input in developing protocols for imaging acquisition and quality control. 50 Further, identifying technologist quality issues is more difficult, as extramural teleradiologists may review fewer cases from an individual technologist. A survey conducted among European radiologists revealed that teleradiology was associated with poor participation in multidisciplinary meetings, inadequate quality reports, and difficulties in communicating with off-site radiologists. 48 While teleradiology services have the potential to increase communication amongst rural and remote healthcare teams, in practice this capability is often not met.
Local radiologists play a pivotal role as advocates for radiology services within their communities. Often faced with limited resources, local radiologists advocate for expanded diagnostic services and timely access to scans for patients. This may involve extra training to provide broader procedural services or communicating with local government for increased funding. Extramural teleradiologists with limited connection to these communities are far less likely to fulfill the same advocacy role.
While extramural teleradiology offers the advantage of timely imaging interpretation and provider call coverage, intramural and on-site radiologists remain indispensable for the comprehensive provision of radiological services in rural and remote communities.
Pooling of Rural and Remote Call Groups
A survey of Canadian rural and remote physicians demonstrated that leading reasons for leaving a rural setting to pursue urban practice are long work hours, lack of professional backup and inability to secure locum coverage. 6 Pooling rural groups can alleviate work and call burden through allowing fewer radiologists to provide coverage across multiple centers during off-hours. Further, it can facilitate centres to have 24-hour access to imaging interpretation, which can be critical in informing treatment decisions. Consolidating regional radiology groups and implementing intramural teleradiology presents the opportunity to enhance the provision of local radiology services while improving on the limitations of extramural models.
In comparison to extramural teleradiology, a pooled rural radiology group comprises individuals practicing in a more similar setting, faced with similar considerations. As a result, these groups share needs and can consolidate their advocacy efforts, leveraging their collective strength to secure regional funding and drive improvements in services. Pooled groups maintain a greater level of connection to the communities they serve when compared to extramural teleradiology. This has the potential to lead to greater involvement and input to optimize the imaging process for each patient. While providing IR and procedural services to Canada’s most remote and rural locations will remain challenging due to geographic isolation, this model offers significant benefits for diagnostic interpretation services in these communities. However, successful implementation of group models necessitates initial government investment to establish the appropriate infrastructure for collaboration and data sharing.
Collaborations With Urban Centres
Collaborations between urban and non-urban centres present the opportunity to address labour shortages and offer subspecialty diagnostic services that are otherwise limited. Partnerships between these centres entail radiologists who practice in urban – and often academic centers – to travel to remote locations on a rotating basis to provide diagnostic and potentially procedural services. While similar to extramural teleradiology models, these relationships are formed with the additional intention of providing subspecialty consultation and specialty imaging service provision. For example, the radiology groups at the University of Ottawa Heart Institute and The Ottawa Hospital have established a collaboration with Qikiqtani General Hospital (QHS) in Iqaluit, providing subspecialty access to one of Canada’s most remote regions. Through the partnership, QHS now offers cardiac CT, and is the northernmost community in the country to do so. 51 This relationship saves patients the need to travel long-distances for this type of specialized imaging. Similarly, Sudbury’s Health Sciences North and Toronto’s Joint Department of Medical Imaging have a collaboration to decrease wait times and access to subspecialty radiology services for this Northern Ontario population. Since the partnership began, diagnostic interpretation wait times have significantly decreased from fifteen to two hours, alleviating a significant workforce shortage in this community. 52
Not only do these inter-hospital relationships benefit patients directly, but also indirectly through increased physician collaboration. Collaborations between urban and rural sites increases access to subspecialists, facilitating opportunities such as multidisciplinary case conferences between physicians practicing across multiple locations. In addition to supporting patient care, increased availability of professional support is one of the primary factors that influences rural and remote physicians to remain in non-urban practice. 6
Mobile Imaging
To bring complete diagnostic radiology services to a community, imaging equipment including scanners must be available along with required expertise to acquire the images (technologists) and interpret them (radiologists). Mobile imaging provides an opportunity to address the shortage of CT and MRI scanners that Canada faces. A mobile imaging unit consists of an enclosure of imaging equipment in a trailer that can be deployed to multiple sites. As of 2020, there were 2 mobile CT scanners and 7 MRI units in use in Canada, 5 of which serviced rural areas. While the CT scanners remain fixed in one site at present, the MRI units service 20 sites nationally. 53 Mobile imaging units offer significant benefits to rural communities through sharing of initial investment costs, increased patient volumes through larger catchment areas, and decreased transportation costs to patients. 54 However, challenges include substantial cost and associated energy required for transport. 55
Remote communities often are too far apart in geography for mobile units to feasibly be deployed. Recently, portable MRI scanners have been approved for use in Canada. 56,57 Portable scanners have the potential to greatly improve the accessibility of advanced imaging in underserviced communities across Canada, as they are both more transportable and significantly less costly than traditional MRI machines. 58 Further, these scanners are equipped with deep learning sequences, allowing them to automatically make adjustments during the image reconstruction process, thereby improving the quality of the images and significantly reducing scanning time. 57 Currently, these portable scanners’ imaging capacity is limited to the head, with hopes to extend their capability to other structures. Future data derived from the use of these units in rural and remote communities will inform their efficacy in improving the accessibility of care.
AI Initiatives
Artificial intelligence (AI) offers the opportunity to improve the speed, accuracy, and quality of imaging acquisition and interpretation. 59 One potential implementation for AI is the ability to triage images into those that are high-risk for emergent findings and bring them to the attention of reporting radiologists. Recently, an initiative has been funded with this purpose, to implement in remote Northern Canadian communities. 60 A group has recently demonstrated the potential of AI by creating a deep learning algorithm that can identify cerebral hemorrhage, mass effect, or hydrocephalus with high accuracy. 61 Further opportunity for AI exists to route images to the most appropriate radiologist in a group. This way, a given study would be directed to the radiologist with the most experience, improving quality of care. If implemented, deep learning algorithms have the potential to optimize workflow and facilitate timely care to the most acutely ill, maximizing the efficiency of a strained service in rural and remote communities.
Professional Organizations and Opportunities for Rural and Remote Radiologists
Professional organizations, such as the Canadian Association of Radiology (CAR), provide an opportunity for rural and remote radiologists to participate in continuing medical education (CME) and network in person with colleagues. Continuing medical education (CME) is mandatory for all physicians in Canada. Opportunities such as in-person conferences offer rural and remote physicians the chance to learn relevant technical skills and expand their professional networks. Large society meetings such as the annual meeting of the Radiological Society of North America offers hands-on technical workshops that can empower rural and remote radiologists to learn new skills (for example, musculoskeletal ultrasound), to potentially expand imaging services not currently offered in their region. In addition, CAR has a large repository of on-line CME offerings for its members, which can be of immense value to radiologists living and working remotely. 62 A specific rural and radiology interest or affiliate group could be explored within CAR as another avenue to support radiologists practicing in rural and remote locations.
Conclusions
Rural and remote radiology offers a multitude of advantages, including improved patient-centred care, community integration, and lifestyle benefits. Simultaneously, there are unique challenges to rural and remote radiology that have restricted recruitment and retention in recent years. Among chief factors are limited exposure during training, workforce shortages and poor infrastructure for image acquisition and procedures. Mobile imaging initiatives, teleradiology, and AI technologies have emerged to bridge the imaging divide and enhance radiological services in these areas. However, none of these strategies are without their flaws. Local radiologists remain indispensable for procedural work, quality control of image acquisition, and patient advocacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.